
Abstract
Background:
Whether endovascular treatment (EVT) is safe and effective for vertebrobasilar artery occlusion (VBAO) is yet incompletely understood. Two RCTs, the endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST) trail and the Basilar Artery International Cooperation Study (BASICS), concentrating on this field were recently reported.
Objective:
We use real-world registry data of VBAO to compare the outcome of EVT inside and outside the inclusion and exclusion criteria of the BEST and BASICS study to testify the feasibility of the selection paradigms of VBAO in these trials.
Methods:
Consecutive patients with VBAO receiving EVT involving 21 stroke centers were retrospectively included. The safety outcomes [3-month mortality, symptomatic intracranial hemorrhage (sICH), and effectiveness outcomes (the proportion of 3-month functional independence (mRS of 0–2) and favorable outcome (mRS of 0–3)] were compared between VBAO patients who meet or failed to meet the BEST/BASICS selection criteria for EVT.
Results:
Our study cohort consisted of 577 VBAO patients who underwent EVT. Of them, 446 patients had pc-ASPECTS ≧8. Successful reperfusion (mTICI 2b or 3) was achieved in 85.4% (n = 493). There were 418 patients fulfilling the BEST criterion for EVT and 194 fulfilling the BASICS criterion. Regression analysis indicated that adherence to BEST or BASICS criterion for EVT was not independently related to most of the safety and effectiveness outcome except that adherence to BEST was significantly associated with the 3-month favorable outcome (ORBEST: 1.742, 95% CI: 1.087–2.790). However, when we put pc-ASPECTS into both criteria with a cut-off value of 8, meeting both BEST criterion plus pc-ASPECTS and BASICS criterion plus pc-ASPECTS was independently related to 3-month functional independence (ORBEST: 1.687, 95% CI: 1.077–2.644; ORBASIC: 1.653, 95% CI: 1.038–2.631) and favorable outcome (ORBEST: 2.280, 95% CI: 1.484–3.502; ORBASIC: 2.153, 95% CI: 1.372–3.378).
Conclusion:
Our study indicated that, based on real-world data of EVT, adherence to BEST or BASICS criterion for EVT was not independently associated with the safety and effectiveness outcome except that adherence to BEST was significantly related to the 3-month favorable outcome. However, the BEST or BASICS selection criterion and pc-ASPECTS ≧8 might be better paradigms for EVT patient selection.
Introduction
Acute vertebrobasilar artery occlusion (VBAO), accounting for about 1% of all ischemic strokes, is associated with high mortality and disability of up to 70%, which represents the most devastating type of ischemic stroke.1–4
Previous large trials had indicated an overwhelming benefit of endovascular treatment (EVT) for treating acute anterior circulation ischemic stroke due to emergent large vessel occlusion.5–8 However, whether EVT is safe and effective for patients with acute VBAO is yet incompletely understood.9–11
Recently, two multicenter, randomized controlled trials (RCTs), the endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion trial (BEST) and the Basilar Artery International Cooperation Study (BASICS), failed to indicate the superiority of EVT over standard medical treatment.12,13 Despite that, it is still believed in clinical practice that EVT might be helpful for VBAO in case of proper patient selection. We hypothesized that the inclusion and exclusion protocols for EVT in BEST and BASICS are suboptimal for selecting the real patients who need EVT, which might partly explain the negative results of both studies. We therefore use a real-world multicenter database to compare the safety and effectiveness of EVT for patients with VBAO according to the current BEST/BASICS selection criteria for EVT.
Furthermore, the Acute Stroke Prognosis Early Computed Tomography Score (ASPECTS) is a standardized semi-quantitative computed tomographic (CT) grading system used to assess early ischemic changes and predict functional outcomes and ischemic core volumes in patients with acute anterior circulation ischemic stroke. 14 Low ASPECTS has been reported to be associated with poor functional outcome after reperfusion and was adopted as one of the exclusion criteria in several trails in acute anterior circulation ischemic stroke.6,15–17 The posterior circulation ASPECTS (pc-ASPECTS), first proposed by Puetz et al., was considered as one of the factors associated with functional outcome and mortality in patients with acute VBAO. 18 Several studies have shown that pc-ASPECTS <8 could also identify patients unlikely to achieve favorable outcomes despite successful reperfusion of the basilar artery.18,19 However, neither the BEST nor the BASICS trial investigators included pc-ASPECTS evaluation in the inclusion criteria. Therefore, we further tried to consider pc-ASPECTS ≧8 as an additional selection criterion and analyzed the safety and effectiveness of EVT divided by the new selection criterion.
Methods
Study design and participants
The study was conducted based on the PostErior ciRculation iSchemIc Stroke regisTry (PERSIST), a multicenter EVT registry program of VBAO patients treated with EVT in China (registration: URL: http://www.chictr.org.cn/; unique identifier: ChiCTR2000033211). The study was approved by the ethics committee of First Affiliated Hospital of University of Science and Technology of China (2020KY-40). Due to its retrospective nature, the need for patient consent was waived. The details of the registry have been published elsewhere. 20 In brief, it is a multicenter retrospective registry program of consecutive posterior circulation ischemic stroke patients with acute, symptomatic, radiologically confirmed VBAO (basilar artery occlusion or vertebral artery occlusion resulting in no flow to the basilar artery) who were treated with EVT. The inclusion and exclusion criteria of the registry along with the BEST and BASICS selection criteria are listed in Table s1.
In this study, all cases of the real-world registry were coded as either meeting or not meeting BEST/BASICS criteria for EVT. The safety and effectiveness outcomes were compared, respectively.
Baseline characteristics
Patients’ baseline and clinical characteristics [e.g. demographic data, National Institutes of Health Stroke Scale (NIHSS) score, laboratory test results, neurovascular images, operative information, and perioperative management] were retrospectively obtained by reviewing medical records. Details of the data are available in Table 2.
The pc-ASPECTS was graded according to the previous description. 18 And each region was scored 0 if abnormal or 1 if normal. A higher pc-ASPECTS represents a smaller infarct. Two neuroradiologists, who were blind to clinical outcomes and treatment assignment, retrospectively evaluated the neuroimaging parameters to include pc-ASPECTS on non-contrast computed tomography (NCCT) and occlusion site on digital subtraction angiography (DSA). If there was a dispute, the final result was reached through consultation. The intraclass correlation coefficient for pc-ASPECTS was 0.493. However, we use the pc-ASPECTS ≧8 points as the cut-off for dichotomy; the interrater variability (κ) was 0.744 for the identification of the pc-ASPECTS ≧8. The occlusion site of ‘basilar artery + vertebral artery’ was defined as an occlusion of the vertebral artery resulting in no flow to the basilar artery, and the occlusion site of ‘basilar artery’ was limited to only basilar artery occlusion. If there is any disagreement, the final assessment was confirmed on the basis of consensus.
Outcome measurement
All patients had a CT or magnetic resonance imaging (MRI) scan within 48 h after EVT to assess hemorrhagic complications. The functional outcome of all patients was assessed by modified Rankin scale (mRS) at 3 months after stroke onset.
The primary effectiveness endpoint is 3-month functional independence, defined as an mRS score of ≦2. Favorable outcome is defined as a 3-month mRS score ≦3. Successful reperfusion is defined as a modified Thrombolysis in Cerebral Infarction (mTICI) scale score of 2b to 3.
The primary safety outcomes of this study include symptomatic intracranial hemorrhage (sICH) and mortality at 90 days after EVT. sICH was defined, based on Heidelberg Bleeding Classification, as a newly observed ICH on imaging that was related to any of the following conditions: (1) an NIHSS score that increased more than 4 points; (2) an NIHSS score that increased more than 2 points in a category; and (3) deterioration that led to hemicraniectomy, external ventricular drain placement, intubation, or other major medical interventions. There were no other explanations for symptom deteriorations. 21 After enrolling all patients, two neuroradiologists, who were unaware of the clinical data, the intervention, and outcomes, retrospectively evaluated the occlusion site and the presence of sICH and mTICI.
Statistical analyses
Differences between the two groups were tested using the Pearson’s Chi-square tests for categorical values and the t test or Mann–Whitney U test for continuous variables, as appropriate.
Multivariable logistic regression models were used to evaluate the associations between EVT performed in accordance with or against BEST, BEST + pc-ASPECTS ≧8, or BASICS criterion, BASICS + pc-ASPECTS ≧8 with mRS (0–2 and 0–3) at 3 months, 3-month mortality, and sICH after adjusting for potential confounders with p < 0.20 on univariate analysis. Associations are presented as odds ratios (ORs) and 95% confidence intervals (CIs). All tests were two-tailed and statistical significance was determined at p < 0.05. All statistical analyses were performed using the SPSS software package (version 24.0).
Result
Registry characteristics
A total of 577 VBAO patients across 21 stroke centers undergoing EVT were included in the analysis; the average age was 63.51 ± 12.89 years. The median NIHSS score of included patients at admission was 23 [interquartile range (IQR), 14–29]. In our cohort, 446 patients had pc-ASPECTS ≧8. Successful reperfusion (mTICI 2b and 3) was achieved in 85.4% (n = 493) of patients. Three-month functional independence (mRS 0–2) was found in 176 (30.5%), favorable outcome (mRS 0–3) at 3 months in 222 (38.5%), and death within 3 months in 216 patients (37.4%). A total of 38 patients (6.6%) experienced sICH.
Outcomes of EVT according to the BEST criterion
The most common reason for non-adherence to BEST criterion was the delayed treatment time window in our registry. Of the 577 VBAO patients, 418 patients fulfilled the BEST criterion for EVT (As shown in Flow Chart). Compared with the 159 patients against BEST, significant differences were found in atrial fibrillation (AF) (p = 0.011), baseline NIHSS score (p = 0.039), intravenous tissue plasminogen activator (IV tPA) treatment (p < 0.001), estimated occlusion to groin puncture time (p < 0.001), groin puncture to reperfusion time (p = 0.002), and reduction in NIHSS score at discharge (p < 0.001). In terms of the sICH, 3-month mortality, 3-month functional independence, and favorable outcome, no significant differences were observed between groups according to the BEST criterion (Table 1).
Baseline characteristics and outcomes (effectiveness and safety) of the study population stratified according to the BEST/BASICS criterion.
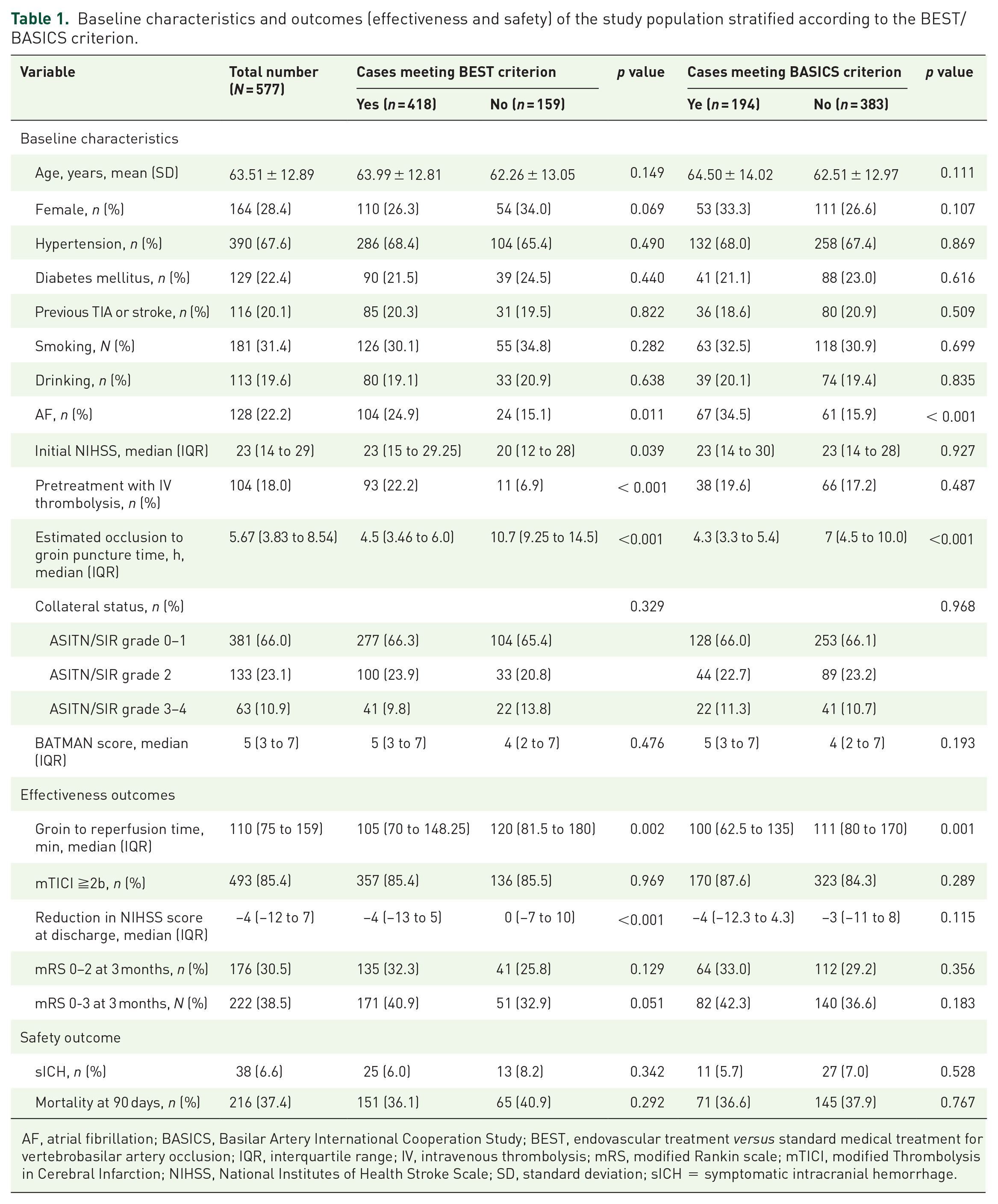
AF, atrial fibrillation; BASICS, Basilar Artery International Cooperation Study; BEST, endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion; IQR, interquartile range; IV, intravenous thrombolysis; mRS, modified Rankin scale; mTICI, modified Thrombolysis in Cerebral Infarction; NIHSS, National Institutes of Health Stroke Scale; SD, standard deviation; sICH = symptomatic intracranial hemorrhage.
Table 2 summarizes compliance with BEST criterion in relationship to sICH, 3-month mortality, and 3-month functional independence and favorable outcome using multivariable logistic regression models adjusting for potential confounders. Adherence to BEST criterion for EVT was not independently related to the 3-month functional independence (OR: 1.375, 95% CI: 0.841–2.249), sICH (OR: 1.040, 95% CI: 0.336–3.217), and 3-month mortality (OR: 0.733, 95% CI: 0.478–1.123) after EVT, while adherence to BEST was significantly associated with the 3-month favorable outcome (BEST: OR: 1.742, 95% CI: 1.087–2.790).
Association of compliance with BEST criterion with or without pc-ASPECTS ≧8 with outcomes on multivariable logistic regression models adjusting for potential confounders.
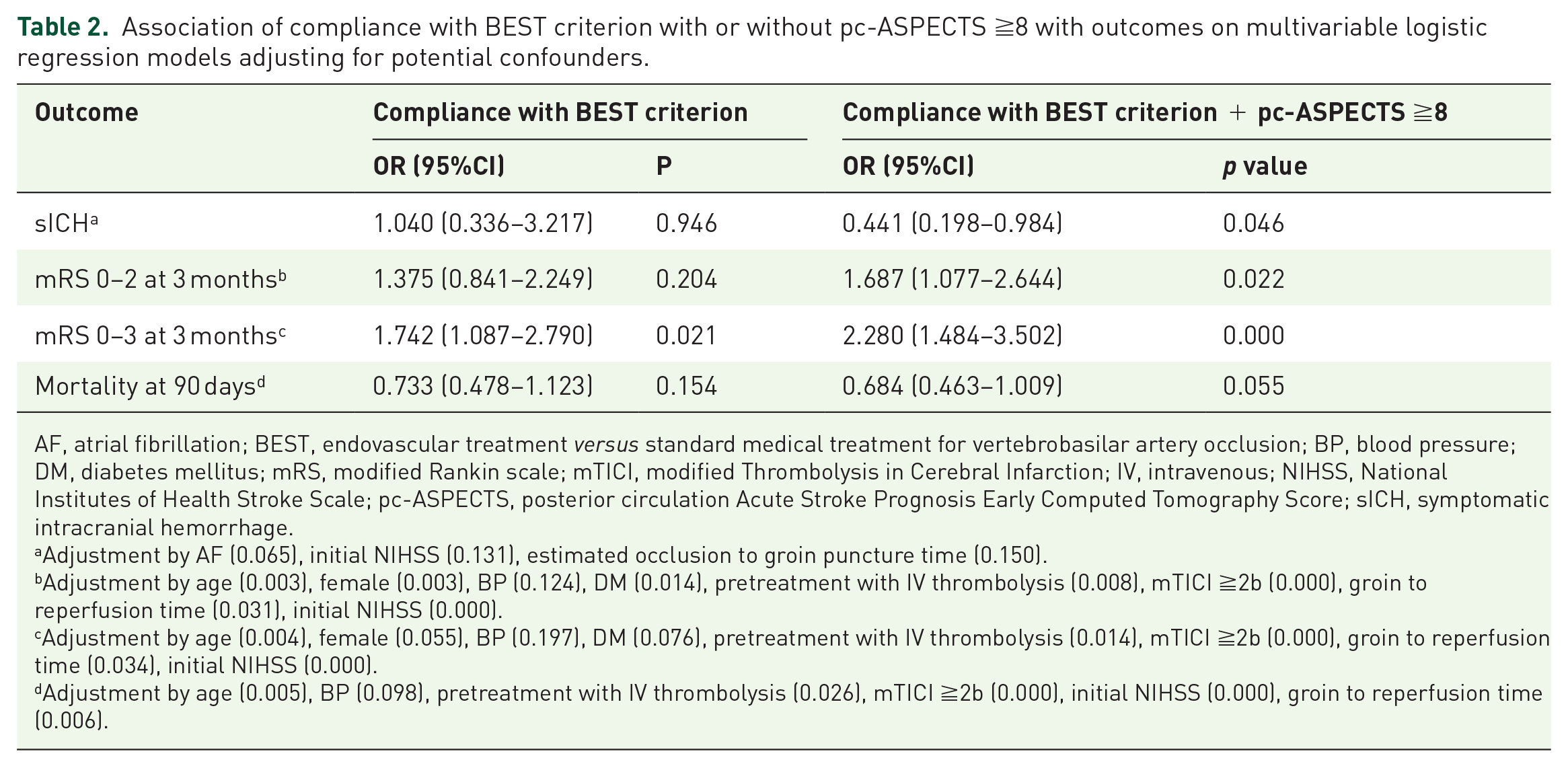
AF, atrial fibrillation; BEST, endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion; BP, blood pressure; DM, diabetes mellitus; mRS, modified Rankin scale; mTICI, modified Thrombolysis in Cerebral Infarction; IV, intravenous; NIHSS, National Institutes of Health Stroke Scale; pc-ASPECTS, posterior circulation Acute Stroke Prognosis Early Computed Tomography Score; sICH, symptomatic intracranial hemorrhage.
Adjustment by AF (0.065), initial NIHSS (0.131), estimated occlusion to groin puncture time (0.150).
Adjustment by age (0.003), female (0.003), BP (0.124), DM (0.014), pretreatment with IV thrombolysis (0.008), mTICI ≧2b (0.000), groin to reperfusion time (0.031), initial NIHSS (0.000).
Adjustment by age (0.004), female (0.055), BP (0.197), DM (0.076), pretreatment with IV thrombolysis (0.014), mTICI ≧2b (0.000), groin to reperfusion time (0.034), initial NIHSS (0.000).
Adjustment by age (0.005), BP (0.098), pretreatment with IV thrombolysis (0.026), mTICI ≧2b (0.000), initial NIHSS (0.000), groin to reperfusion time (0.006).
In our registry, 446 patients had pc-ASPECTS ≧8. Univariate analysis suggested that patients fulfilling BEST inclusive criteria + pc-ASPECTS ≧8 had a higher prevalence of functional independence (p < 0.001) and favorable outcome (p < 0.001) and a lower prevalence of sICH (p = 0.012) and 3-month mortality (p = 0.013) compared with those who do not (Table s2). After adjusting for potential confounders, meeting both the BEST criterion and pc-ASPECTS ≧8 was independently related to sICH (OR: 0.441, 95% CI: 0.198–0.984) and 3-month functional independence (OR: 1.687, 95% CI: 1.077–2.644) and favorable outcome (OR: 2.280, 95% CI: 1.484–3.502), but not independently related to 3-month mortality (OR: 0.684, 95% CI: 0.463–1.009) (Table 2).
The distribution of mRS scores in VBAO patients treated with EVT at 3 months according to the BEST criterion and BEST criterion + pc-ASPECTS ≧8 is displayed in Figure 1. There was no significant difference in the distribution of mRS scores between patients with EVT meeting the BEST criterion and those outside the selection criteria (p = 0.207). However, the distribution of mRS scores between patients with EVT meeting the BEST criterion + pc-ASPECTS ≧8 and those outside the selection criteria was significantly different (p < 0.001).

Distribution of 3-month modified Rankin scale (mRS) scores according to adherence to the BEST criterion.
Outcomes of EVT according to the BASICS criterion
A total of 194 patients underwent EVT fulfilling the BASICS criterion (only the final version of the BASICS selection criterion was applied as shown in Flow Chart). The most two common reasons for non-adherence to BASICS selection criteria were occlusion location and delayed treatment window. Patients meeting BASICS criterion for EVT tended to have a higher prevalence of AF (p < 0.001). The estimated occlusion to groin puncture time (p < 0.001) and groin puncture to reperfusion time (p = 0.001) were significantly shorter in patients with EVT fulfilling BASICS inclusive criteria (Table 1). After adjusting for potential confounders, adherence to BASICS criterion for EVT was not independently related to 3-month mRS functional independence (OR: 1.074, 95% CI: 0.683–1.688), 3-month favorable outcome (OR: 1.205, 95%CI: 0.784–1.852), sICH (OR: 0.833, 95%CI: 0.373–1.861), and 3-month mortality (OR: 1.031, 95% CI: 0.687–1.547) (Table 3). Besides, we also get similar outcome when we compare the effectiveness and safety outcomes in subgroups stratified on the basis of the BASICS inclusive criteria for the occlusion location and time from onset to groin puncture. The results are listed in Table s3 and s4.
Association of compliance with BASICS criterion with or without pc-ASPECTS ≧8 with outcomes on multivariable logistic regression models adjusting for potential confounders.

AF, atrial fibrillation; BASICS, Basilar Artery International Cooperation Study; mRS, modified Rankin Scale; BP, blood pressure; DM, diabetes mellitus; mRS, modified Rankin scale; mTICI, modified Thrombolysis in Cerebral Infarction; IV, intravenous; NIHSS, National Institutes of Health Stroke Scale; pc-ASPECTS, posterior circulation Acute Stroke Prognosis Early Computed Tomography Score; sICH, symptomatic intracranial hemorrhage.
Adjustment by AF (0.065), initial NIHSS (0.131), estimated occlusion to groin puncture time (0.150).
Adjustment by age (0.003), female (0.003), BP (0.124), DM (0.014), pretreatment with IV thrombolysis (0.008), mTICI ≧2b (0.000), groin to reperfusion time (0.031), initial NIHSS (0.000).
Adjustment by age (0.004), female (0.055), BP (0.197), DM (0.076), pretreatment with IV thrombolysis (0.014), mTICI ≧2b (0.000), groin to reperfusion time (0.034), initial NIHSS (0.000).
Adjustment by age (0.005), BP (0.098), pretreatment with IV thrombolysis (0.026), mTICI ≧2b (0.000), initial NIHSS (0.000), groin to reperfusion time (0.006).
In our registry, 158 patients fulfilling BASICS criterion had a pc-ASPECTS ≧8. Univariate analysis showed that patients fulfilling both BASICS criterion and pc-ASPECTS ≧8 had a higher prevalence of functional independence (p < 0.001) and favorable outcome (p < 0.001) and a lower prevalence of sICH (p = 0.032) (Table s2). Logistic regression analysis suggested that fulfilling both BASICS criterion and pc-ASPECTS ≧8 was independently related to 3-month mRS functional independence (OR: 1.653, 95% CI: 1.038–2.631) and favorable outcome (OE: 2.153, 95% CI: 1.372–3.378) (Table 3).
The distribution of mRS scores in VBAO with EVT at 3 months according to meeting the BASICS criterion and BASICS criterion + pc-ASPECTS ≧8 is displayed in Figure 2. No significant difference in the distribution of mRS scores was found between groups (p = 0.421). But the distribution of mRS scores between patients with EVT meeting the BEST criterion + pc-ASPECTS ≧8 and those outside the selection criteria was significantly different (p = 0.001).

Distribution of 3-month modified Rankin scale (mRS) scores according to adherence to BASICS criterion.
Discussion
Our study indicated that, based on the real-world data of EVT, adherence to BEST or BASICS criterion for EVT was not independently associated with safety outcomes (sICH and 3-month mortality) and effectiveness outcome (3-month functional independence and favorable outcome) except that adherence to BEST was significantly related to 3-month favorable outcome. However, we put pc-ASPECTS ≧8 as an additional inclusion criterion for both BEST and BASICS selection criteria; most of the safety and effectiveness outcome turned to be statistically significant.
In our retrospective registry, the most common reason for not meeting BEST/BASICS inclusive criteria for EVT was the delayed treatment window. The adjusted analysis of our data demonstrated that EVT can be performed outside the recommended time window with equal effectiveness and without increased proportion of sICH and mortality when compared with the group treated within the recommended time window. It consisted of some previous published data.12,13,22 The results suggested that the time window for patients with VBAO seemed less important than that in anterior circulation. We believed that the diversity in clinical courses and feature interferes with the time selection for EVT in patients with VBAO.18,22,23
The second reason for not meeting the BASICS criterion for EVT was the location of occlusion. In our registry, isolated basilar artery occlusion was found in 303 patients. Compared with the other occlusion site, the safety and effectiveness of EVT were similar. The reason may be attributed to the fact that damage caused by the harassment of perforating artery in the procedure of recanalization of isolated basilar artery might be balanced by the damage caused by the absence of compensatory capacity of collaterals such as posterior inferior cerebellar artery in vertebral artery occlusion.
Pc-ASPECTS is a semi-quantitative method for grading irreversible ischemia in the vertebrobasilar system. Previous studies have highlighted the importance of pc-ASPECTS on outcomes of BAO.18,19 However, studies have yielded inconsistent results on whether patients with low pc-ASPECTS should receive EVT. Several studies have shown that pc-ASPECTS <8 could identify patients unlikely to get good outcomes despite successful reperfusion.18,19,24,25 Another study from the Endovascular Treatment in Ischemic Stroke (ETIS) registry suggested that rapid endovascular reperfusion for patients with BAO is helpful despite pc-ASPECTS being <8. 26 In our study, we found that fulfilling the BEST or BASICS selection criteria plus pc-ASPECTS ≧8 might be better options compared with the original selection criteria. According to the recent announcement of the endovascular treatment for acute basilar artery occlusion (ATTENTION) trial and the basilar artery occlusion: Chinese endovascular (BAOCHE) trial in the European Stroke Organisation Conference 2022, both trials support our hypothesis with the inclusion criterion containing pc-ASPECTS and indicate significant advantage of EVT over standard medical treatment. We look forward for the detailed information after sufficient peer review.
In this study which contained 577 patients, the median pc-ASPECTS was 9 (IQR, 8–10). The bar diagram could be found in the supplementary materials. As we all know, patients with lower pc-ASPECTS are often in danger of life-threatening symptoms, such as irregularity of heart and respiratory rhythm. Their family members are more likely to choose standard pharmaceutical treatment in these cases, compared with the RCT studies. Moreover, unlike both RCTs, the pc-ASPECTS in our study was evaluated based on merely the NCCT. Compared with magnetic resonance angiography, the lesion of CT was hard to locate in early stage patients with acute cerebral infarction. For these reasons, the score is skewed to higher scores.
The strength of our study was the relative intact data of multiple centers and relatively large samples regarding the VBAO patients. However, several limitations should also be mentioned. First, due to the retrospective observational and non-randomized design, we urge a cautious interpretation of the results as it probably involves a high risk of selection bias. Second, it is known that the criterion applied in the BASICS trials had been modified once during the recruiting process. We only analyzed the final form of the selection criterion instead of both forms to keep the article friendly to readers. Third, our registry data were obtained during the period between December 2015 and December 2018; whether the new devices on embolectomy procedural would make difference on the selection criterion remains unknown.
In conclusion, our study found that most clinical outcomes did not reach statistical significance between patients meeting BEST/BASICS criteria for EVT and those outside the selection criteria based on the real-world data. Therefore, continued study of the efficacy and safety of EVT with more serious consideration of inclusion criteria should be performed. The ongoing multicenter controlled trails (NCT04751708) have considered the pc-ASPECTS as one of the inclusion criteria to explore the usefulness of endovascular treatment in basilar artery occlusion. We hope it will shed additional light on this crucial issue and be helpful in selecting VBAO patients suitable for EVT.

Supplemental Material
sj-docx-1-tan-10.1177_17562864221114627 – Supplemental material for The safety and effectiveness of endovascular treatment for patients with vertebrobasilar artery occlusions: according to the BEST and BASICS criteria
Supplemental material, sj-docx-1-tan-10.1177_17562864221114627 for The safety and effectiveness of endovascular treatment for patients with vertebrobasilar artery occlusions: according to the BEST and BASICS criteria by Wen Sun, Zuowei Duan, Pengfei Xu, Lulu Xiao, Jinjing Wang, Wei Gui, Genpei Luo, Zhongyi Wu, Zhongkui Han, Wei Li, Guoqiang Xu, Fengchang Liu, Jilong Yi, Chaolai Liu, Yan Zhang and Haiyan Liu in Therapeutic Advances in Neurological Disorders
Footnotes
Acknowledgements
PERSIST Investigators are as follows:
Wen Sun, Wei Hu, Pengfei Xu, Stroke Center & Department of Neurology, The First Affiliated Hospital of University of Science and Technology of China (USTC), Hefei, China; Xinfeng Liu, Wusheng Zhu, Lulu Xiao, Jinjing Wang, Yuanlu Liu, Kang Yuan, Department of Neurology, Jinling Hospital, Medical School of Nanjing University, Southern Medical University, Nanjing, China; Junshan Zhou, Mengmeng Gu, Department of Neurology, Nanjing First Hospital, Nanjing Medical University, Nanjing, China; Hongbin Chen, Department of Neurology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China; Yijiu Lu, Department of Neurology, The First People’s Hospital of Yulin, Yulin, China; Guoqiang Xu, Department of Neurology, The First People’s Hospital of Yongkang, Jinhua, China; Xinchun Ye, Department of Neurology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, China; Fengchang Liu, Department of Neurology, Xi’an North Hospital, Xi’an, China; Qizhang Wang, Department of Neurology, Shenzhen Hospital of Integrated Traditional Chinese and Western Medicine, Shenzhen, China; Shuanggen Zhu, Department of Neurology, Shenzhen Longhua People’s Hospital, Shenzhen, China; Dezhi Liu, Department of Neurology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, China; Min Li, Department of Neurology, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, China; Wenya Lan, Department of Cerebrovascular Disease Treatment Center, Nanjing Brain Hospital Affiliated to Nanjing Medical University, Nanjing, China; Jin Fan, Department of Neurology, The General Hospital of Western Theater Command, Chengdu, China; Yong Huang, Department of Neurosurgery, Jiangsu Provincial Corps Hospital of Chinese People’s Armed Police Forces, Yangzhou, China; Chaolai Liu, Department of Neurology, The First People’s Hospital of Jining, Jining, China; Jilong Yi, Department of Neurology, Jingmen No.1 People’s Hospital, Jingmen, China; Wei Li, Department of Neurology, The First Affiliated Hospital of Hainan Medical University, Haikou, China; Zhongkui Han, Department of Neurology, Fuyang Cancer Hospital, Fuyang, China; Lichao Ye, Qiankun Cai, Department of Neurology, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, China; Yongkun Li, Department of Neurology, Fujian Provincial Hospital, Fuzhou, China; Genpei Luo, Department of Neurology, Dongguan People’s Hospital, Dongguan, China
Declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of First Affiliated Hospital of University of Science and Technology of China local (2020KY-40); due to the retrospective nature of the study, the need for patient consent was waived.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Key Research and Development Plan Projects of Anhui Province (No. 202104j07020049), Fundamental Research Funds for the Central Universities (WK9110000056), and High-level Talents Innovation and Entrepreneurship Project of Quanzhou Science and Technology Bureau (No. 2018C049R).
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.