
Abstract
Background:
Whether epilepsy surgery, such as corpus callosotomy is effective in patients with pediatric intractable epilepsy with mitochondrial dysfunction is controversial, and there is a paucity of literature on this issue.
Objective:
This study aimed to assess and describe the effective application of corpus callosotomy for treating pediatric patients with intractable epilepsy with mitochondrial dysfunction in a single institution in Korea.
Methods:
This was a retrospective study of pediatric patients with intractable epilepsy and mitochondrial dysfunction who underwent corpus callosotomy in a single tertiary care center. Ten patients with intractable epilepsy with mitochondrial dysfunction were included, and 10 patients with intractable epilepsy with non-mitochondrial dysfunctions were included as a control group. The outcomes of corpus callosotomy in the two groups were evaluated and compared.
Results:
Corpus callosotomy was safely performed and was efficacious in reducing seizure frequency in both groups. The group with non-mitochondrial dysfunction showed slightly better treatment outcomes, with greater reductions in overall seizures, traumatic falling seizures, and electroencephalography improvements, but the differences in treatment effects were not statistically significant.
Conclusions:
Our study is meaningful as it identified the use of corpus callosotomy as a means to save lives and improve quality of life by reducing the frequency of seizures and those associated with traumatic falling in pediatric patients with intractable epilepsy with mitochondrial dysfunction. Larger multicenter studies are necessary to confirm the efficacy of the procedure.
Introduction
Corpus callosotomy is effectively used as a palliative neurosurgical treatment in patients with intractable generalized epilepsy. In particular, corpus callosotomy is known to dramatically reduce traumatic focal/generalized tonic or atonic seizure.1–4
Mitochondria play an important role in generating adenosine triphosphate (ATP) through the electron transport chain and the oxidative phosphorylation (OXPHOS) system. 5 Therefore, mitochondrial dysfunction causes various adverse effects, including placing excessive acute energy demand on the brain; it can be an important etiology of some types of intractable epilepsy, such as status epilepticus.6–9
The treatment of intractable epilepsy with mitochondrial dysfunction is challenging and somewhat different from the treatment of intractable epilepsy with non-mitochondrial dysfunction, and there are additional considerations in anti-seizure medications (ASMs) use.8,10 Although several active trials for treatment of primary mitochondrial dysfunction have been attempted, medications that can reliably treat mitochondrial dysfunction have not yet been generalized.11–14 As a result, pediatric neurologists have attempted diet therapies (DTs) to treat intractable epilepsy with mitochondrial dysfunction, as well as surgical treatments, such as vagus nerve stimulation (VNS) and hemispherectomy. However, whether epilepsy surgery is effective in patients with intractable epilepsy with metabolic causes, such as mitochondrial dysfunction, is controversial, and there is insufficient literature on this issue.15–17
This study aimed to assess and describe the effective application of corpus callosotomy in pediatric patients with intractable epilepsy with mitochondrial dysfunction in a single institution in Korea. This study could help expand the list of possible options for the treatment of intractable epilepsy with mitochondrial dysfunction.
Materials and methods
Inclusion of patients and data collection
This was a retrospective study of pediatric patients with intractable epilepsy with mitochondrial dysfunction who underwent corpus callosotomy between 2007 and 2015 in a single tertiary care center, Severance Hospital, Seoul, Korea. Altogether, 20 patients with intractable epilepsy who underwent corpus callosotomy were included in the study. Etiological work-ups for intractable epilepsies were performed before the patients underwent surgery. Mitochondrial dysfunction was identified as a metabolic etiology of intractable epilepsy in 10 patients; mitochondrial dysfunction was not found in the remaining 10 patients, who were included as a control group for comparisons, later.
Evaluation of epilepsy
Measures of epilepsy characteristics included seizure onset, seizure types, type of epilepsy syndrome, seizure frequency, history of ketogenic diet, number of ASMs, electroencephalography (EEG) findings, and developmental status immediately before corpus callosotomy. The criterion for intractable epilepsy refers to the condition in which seizures recur despite the use of two or more appropriately chosen ASMs; all enrolled patients in this study met this criterion.18,19
Evaluation of mitochondrial dysfunction
Mitochondrial dysfunction was defined as satisfying one or more of the following clinical diagnostic criteria: (a) evidence of mitochondrial dysfunction based on muscle biopsy and (b) mitochondrial respiratory chain (MRC) defects found in biochemical evaluations. Muscle biopsy samples were processed using routine morphological and histochemical staining, including periodic acid-Schiff, modified Gomori trichrome, ATPase pH 9.4, nicotinamide adenine dinucleotide tetrazolium reductase, and succinate dehydrogenase stains. Based on light microscopic findings, ragged red fibers (RRFs) were included as an indicator of mitochondrial dysfunction, but non-specific findings, such as type I or type II atrophy were excluded. Moreover, all samples were examined for electron microscopic changes, such as mitochondrial pleoconia and megaconia. Finally, MRC enzyme complex activities were evaluated by standard spectrophotometric assays to assess the activities of NADH–coenzyme Q (CoQ) reductase (complex I), succinate–CoQ reductase (complex II), succinate–cytochrome c reductase (complex II–III), cytochrome c reductase (complex III), cytochrome c oxidase (complex IV), and citrate synthase enzymes in isolated mitochondria from freshly prepared muscle tissues.20–22 We defined MRC defects as a reduction of residual enzyme activity to below 10% of that of controls. 23 Of the total of 20 patients, 10 patients for whom consent to genetic testing was obtained were subjected to targeted exome sequencing testing. Among them, consent to genetic testing was obtained for three patients in the mitochondrial dysfunction group. The results of targeted exome sequencing were negative in all 10 patients.
Neuroimaging
All patients underwent brain magnetic resonance imaging (MRI) at the time of diagnosis, and some patients were also examined using brain magnetic resonance spectroscopy (MRS). 20 Through this neuroimaging, we tried to evaluate the structural and metabolic status of each patient’s brain.
Corpus callosotomy
All 20 patients underwent a total corpus callosotomy. The surgeries were performed by the same surgical team at a single institution. As brain surgery may result in a serious neuronal energy depletion crisis, we confirmed that each patient was in good general health before surgery, and we focused on providing general supportive care and close observation in a neurological intensive care unit for several days.
Outcomes of corpus callosotomy
The outcomes following corpus callosotomy for intractable epilepsy were evaluated as follows: (a) whether lateralization was secured based on EEGs after surgery, and improvements were evaluated by follow-up EEGs 3 and 12 months after corpus callosotomy. The EEG findings were graded as follows: Grade 1: normalization; Grade 2: slow and disorganized background rhythm without focal or unilateral sharp wave discharges; Grade 3: slow and disorganized background rhythm with focal or unilateral sharp wave discharges; and Grade 4: slow and disorganized background rhythm with multifocal sharp wave discharges and with/without generalized spike and slow wave discharges (GSSWs) or generalized paroxysmal fast activities (GPFAs).15,21 To assess reductions in seizure frequency after corpus callosotomy on a percentage scale, the baseline seizure frequency of each patient was set as ‘0’, and patients were followed up every 3 months until 12 months after corpus callosotomy. The higher the number, the greater the effect, with ‘100’ indicating a seizure-free state. 15
In addition, as existing studies have shown that corpus callosotomy is a palliative neurosurgical treatment that has the greatest effect on the frequency of traumatic tonic or atonic seizures,2,4 the reduction in traumatic tonic or atonic seizures experienced by each patient was assessed at 12 months after corpus callosotomy, evaluated as a percent change. The higher the number, the greater the effect, with ‘100’ indicating freedom from traumatic tonic or atonic seizures.
Developmental status before and 12 months after corpus callosotomy was also compared. Developmental progress was categorized as either ‘improved’ or ‘static’ compared with baseline levels based on the results of interviews and a simple questionnaire, with careful examination of patients by more than two pediatric neurologists who were directly treating them. 15 Patient subgroup analysis was also performed. Patients were divided into subgroups with and without histological pathology identified by muscle biopsy to compare the outcomes of corpus callosotomy.
Data analysis and statistical methods
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software version 20.0, for Windows (IBM Corp., Armonk, NY, USA). Descriptive statistics, including median and range, were used to describe the patient characteristics. Nonparametric comparisons of the characteristics of the mitochondrial dysfunction and non-mitochondrial dysfunction groups were performed using the Mann–Whitney U test. The comparison of treatment outcomes between the two groups was conducted using Fisher’s exact test. Statistical significance was set at p < 0.05.
Results
General characteristics of patients before corpus callosotomy
Of the 20 patients, 10 were diagnosed with intractable epilepsy with mitochondrial dysfunction (Table 1). The total male-to-female ratio was 15:5; this ratio did not differ between the mitochondrial dysfunction and non-mitochondrial dysfunction group. The age of diagnosis of epilepsy ranged from 0.2–9.4 years, with a median of 0.7 years. The time interval from diagnosis of epilepsy to evaluation of mitochondrial dysfunction ranged from 0.4 to 9.0 years, with a median of 2.4 years. In addition, the median time interval from evaluation of mitochondrial dysfunction to corpus callosotomy was 1 year. Therefore, the median time interval from diagnosis of epilepsy to corpus callosotomy in all patients was 4.4 years, with a statistically significant difference between the two groups.
General characteristics of patients before corpus callosotomy.
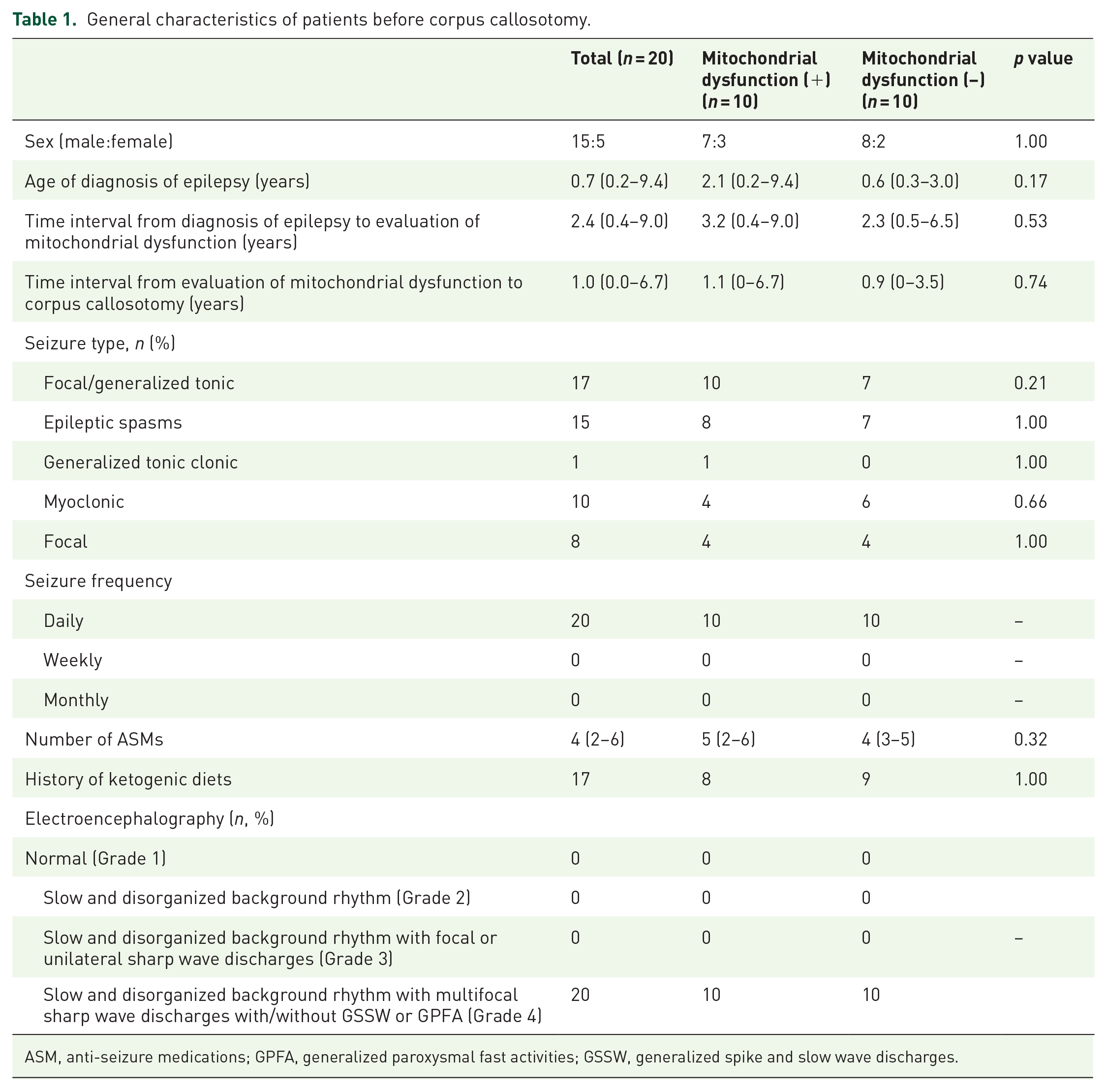
ASM, anti-seizure medications; GPFA, generalized paroxysmal fast activities; GSSW, generalized spike and slow wave discharges.
Multiple types of seizure patterns were observed in patients, and all patients had at least one traumatic seizure type characterized as a focal/generalized tonic seizure, or epileptic spasms. In particular, all patients with intractable epilepsy and mitochondrial dysfunction experienced a previous generalized tonic seizure. Eighteen patients were diagnosed with Lennox–Gastaut syndrome, the most common epilepsy diagnosis in patients before corpus callosotomy. All the patients experienced daily seizures. The median number of ASMs taken by patients before corpus callosotomy was four, and ketogenic diets had been previously attempted in 17 patients, but all were insufficient for effective seizure control. The preoperative EEG of all patients showed multifocal sharp wave discharges and generalized patterns.
Intractable epilepsy patients with mitochondrial dysfunction
Ten patients had mitochondrial dysfunction (Table 2). The median period between diagnosis of epilepsy and diagnosis of mitochondrial dysfunction was 3.94 years, ranging from 0.38 to 6.97 years. Measures of serum lactic acidosis ranged from 0.7 to 3.2 mmol/L, with a median concentration of 1.3 mmol/L. In muscle biopsies, RRFs were detected by light microscopy in two patients. Changes associated with megaconia were observed by electron microscopy in seven patients, and mitochondrial pleoconia was observed in three patients. MRC I defects were observed using MRC complex enzyme assays in seven patients.
Mitochondrial dysfunction profiles of patients (n = 10).
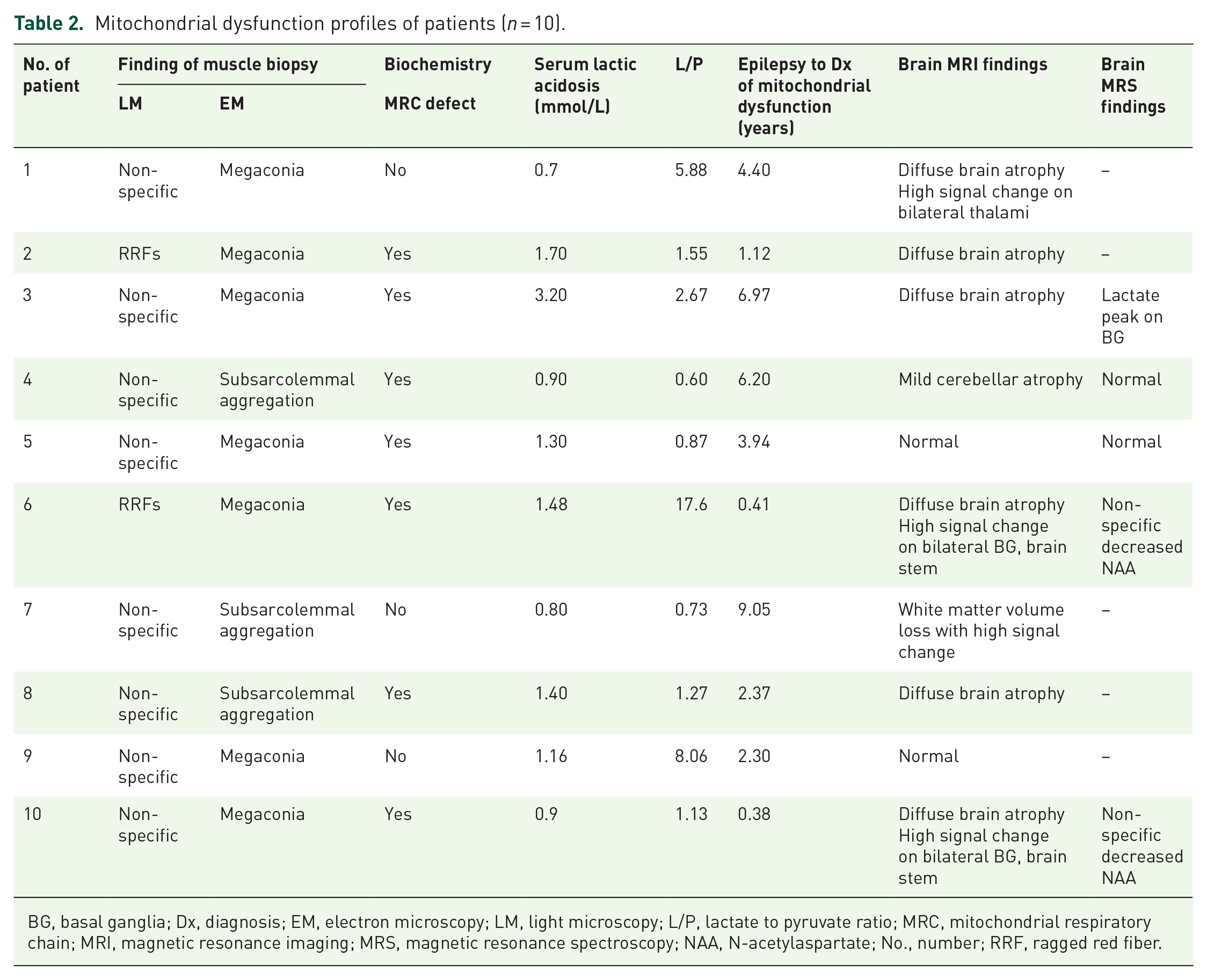
BG, basal ganglia; Dx, diagnosis; EM, electron microscopy; LM, light microscopy; L/P, lactate to pyruvate ratio; MRC, mitochondrial respiratory chain; MRI, magnetic resonance imaging; MRS, magnetic resonance spectroscopy; NAA, N-acetylaspartate; No., number; RRF, ragged red fiber.
Neuroimaging findings
Brain MRI findings of mitochondrial dysfunction group showed diffuse brain atrophy in six patients and high signal changes in the thalamus, basal ganglia, brain stem, or other white matter structures in four patients. Brain MRS was performed in five patients, and a lactate peak was observed in the basal ganglia in one patient. In contrast, brain MRI findings of the non-mitochondrial dysfunction group showed diffuse brain atrophy in six patients, periventricular leukomalacia in two patients, and normal findings in two patients.
Outcomes of corpus callosotomy
The median age of patients undergoing corpus callosotomy was 8.7 years and ranged from 1 to 17 years (Tables 3 and 4). All patients underwent total corpus callosotomy, and no serious complications were noted before or after surgery. All patients were followed at 3-month intervals from 3 to 12 months after surgery to assess the outcomes of corpus callosotomy.
Outcomes of corpus callosotomy of each patient (n = 20).
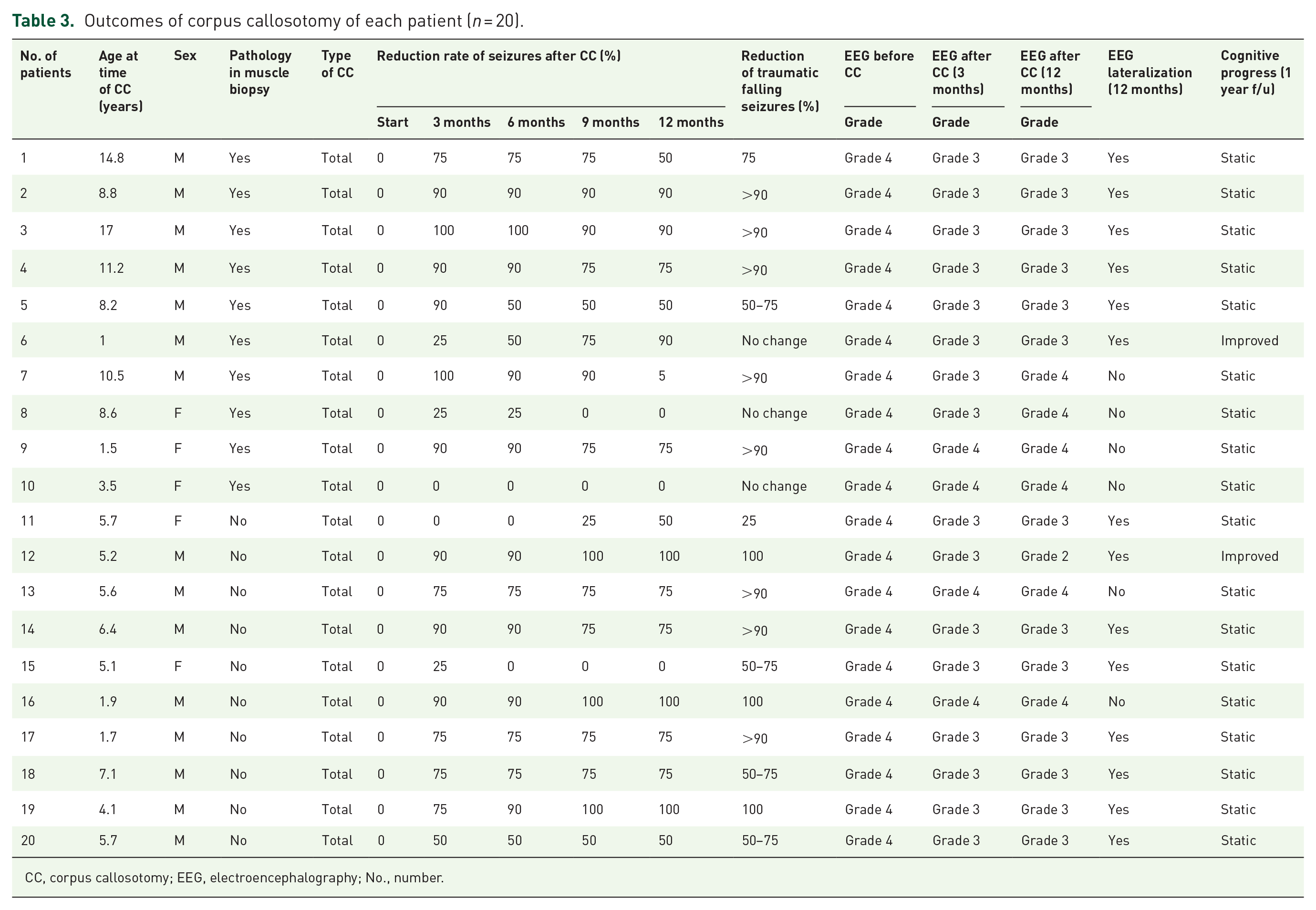
CC, corpus callosotomy; EEG, electroencephalography; No., number.
Comparison of number of improved patients after corpus callosotomy of the two groups.
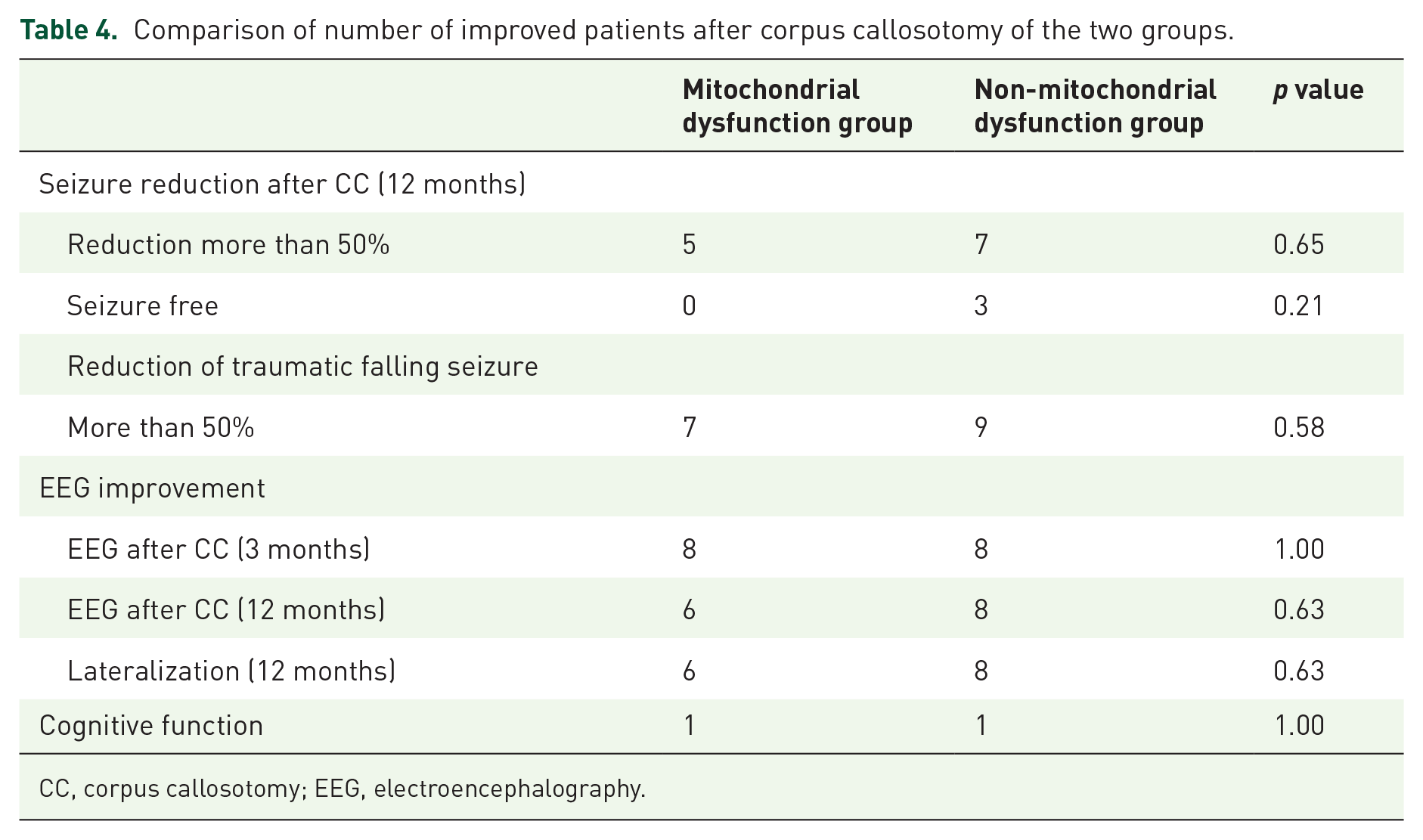
CC, corpus callosotomy; EEG, electroencephalography.
In most patients, a reduction in the seizure frequency was observed. In the non-mitochondrial dysfunction group, three patients became seizure-free 12 months after surgery. However, a reduction in seizure frequency was not observed in three patients, two of whom were from the mitochondrial dysfunction group and one from the non-mitochondrial dysfunction group. In addition, the frequency of traumatic falling seizures was reduced in 17 patients; three patients from the non-mitochondrial dysfunction group experienced none, but there were no changes in the frequency of traumatic falling seizures in three patients in the mitochondrial dysfunction group.
The reduced number of seizures and improvements in EEG and cognitive function measures between the mitochondrial dysfunction and non-mitochondrial dysfunction groups were compared. The non-mitochondrial dysfunction group showed a trend of better treatment outcomes in all aspects, including in the number of patients who achieved more than a 50% reduction in the total number of seizures, the number of those who remained seizure-free, and the number of those who achieved a 50% reduction in traumatic falling seizures; however, these differences were not statistically significant (p = 0.65, p = 0.21, p = 0.58, respectively).
In terms of EEG changes, 14 patients achieved lateralization at 12 months of follow-up. The ratio of this lateralization of EEG was 6:8 for the mitochondrial dysfunction and non-mitochondrial dysfunction groups. In the follow-up EEGs conducted 3 months and 12 months after surgery, after lateralization, the therapeutic performance of the non-mitochondrial dysfunction group was superior to that of the mitochondrial dysfunction group, but no statistical significance was observed. In addition, cognitive improvements were observed in both the groups.
Only one patient developed a subcutaneous abscess after surgery and recovered after additional surgery. All other patients were discharged within 2 weeks of active postoperative intensive care.
Discussion
This study, conducted in a single tertiary medical center, compared the effects of corpus callosotomy on intractable epilepsy patients with and without mitochondrial dysfunction. In general, pediatric patients with intractable epilepsy with metabolic causes, such as mitochondrial dysfunction, do not meet the indications for epileptic surgery, and few studies related to this subject have been conducted to date. We performed corpus callosotomy in patients with intractable epilepsy with mitochondrial dysfunction and observed that those patients acquired partial seizure control without serious complications.
In this study, we emphasize that even in intractable epilepsy with mitochondrial dysfunction, major brain surgery, such as corpus callosotomy, can be safely and effectively performed, and it should be considered a treatment option for patients with epilepsy with mitochondrial dysfunction. The treatment performance of total corpus callosotomy is slightly superior to that of anterior corpus callosotomy. 4 To date, it has been known that administration of general anesthesia in patients with diseases associated with mitochondrial dysfunction must be performed extremely carefully, as it can inhibit MRC complex I and promote catabolism, which can lead to increased systemic energy demands.10,24 In addition, since mitochondrial dysfunction is not a condition in which surgery can remove epileptogenic focal lesions in the brain, surgery is rarely indicated in the standard treatment protocol of epilepsy with mitochondrial dysfunction, and studies related to surgical intervention in such cases are very rare.8,10 Arthur et al. 17 have reported the application of vagus nerve stimulation, a relatively short surgical treatment, in intractable epilepsy with mitochondrial dysfunction, but no significant effect was observed. 17 However, in the present study, reductions in the frequency of overall seizures and traumatic focal/generalized tonic seizures in the non-mitochondrial dysfunction group were slightly superior to, but not statistically different from, those of the mitochondrial dysfunction group, and the mitochondrial dysfunction group also showed good treatment performance after corpus callosotomy.
Corpus callosotomy could be effective as a palliative treatment for intractable epilepsy with mitochondrial dysfunction, as in the case of intractable epilepsy with non-mitochondrial dysfunction, because corpus callosotomy is a disconnective surgery that is short in duration and does not place the same excessive energy demands on patients that procedures, such as resective epilepsy surgery do. In addition, since all patients in this study underwent total corpus callosotomy, it is possible that the effect was similar to that observed when anterior corpus callosotomy was performed, where patients also displayed reductions in the frequency of overall seizures, traumatic focal/generalized tonic seizure, and EEG lateralization.1,4
In addition, the EEG findings improved 12 months after corpus callosotomy as a result of seizure reduction, with the mitochondrial dysfunction group obtaining lateralization in 60%. Also, although it was observed only in a small number of patients, improvement in cognitive function was observed in one patient in each of the two groups. There is controversy over changes in cognitive performance after corpus callosotomy in intractable epilepsy patients, with some reporting that corpus callosotomy may not negatively affect cognitive performance when preoperative baselines are already below average. 25 All of the patients in our study exhibited moderate to severe intellectual disability, and changes in cognitive function are difficult to accurately measure. Therefore, in such a case, EEG improvements rather than as additional loss of function due to corpus callosotomy are considered to be important surgical outcomes to be considered.
It is also noteworthy that all patients with pediatric intractable epilepsy with mitochondrial dysfunction recovered without significant complications after corpus callosotomy. Graham et al. 4 assessed 377 patients in a systematic review of corpus callosotomy in pediatric patients, assessing the side effects of corpus callosotomy that were classified as either neurological complications or surgical complications.4,26 According to this review, transient disconnection syndrome is the most common neurological complication of total corpus callosotomy in pediatric patients, accounting for approximately 12.5% of all complications. However, surgical complications are relatively rare and mostly minor, such as hematoma, subdural cerebrospinal fluid (CSF) accumulation, venous embolism, and infections, such as meningitis and osteomyelitis, and the mortality rate was very low (0.26%). 4 Thus, corpus callosotomy is considered a neurologically and surgically safe operation. In our patients, however, neurological complications were not effectively evaluated because patients had very low levels of basic functions; a minor complication was observed in one of the 10 patients, although this was also effectively controlled. Even if there is a metabolic problem, such as mitochondrial dysfunction, it is thought that corpus callosotomy could be safely and effectively attempted.
Our study is meaningful as it could lead to improved life-saving options and quality of life improvements in patients by reducing the frequency of overall seizures and traumatic falling seizures by performing a corpus callosotomy in patients with pediatric intractable epilepsy with mitochondrial dysfunction. Moreover, corpus callosotomy has not been indicated for epileptic patients with metabolic causes; thus, this study has implications for pediatric neurologists and epileptologists. However, since the number of patients is currently too low to draw a strong conclusion, additional studies with larger sample sizes or multicenter studies are necessary to confirm the positive effects of corpus callosotomy in pediatric intractable epilepsy with mitochondrial dysfunction. In addition, a study reporting the experience of epilepsy surgery for gene-confirmed primary mitochondrial disorder may be necessary, so that, further follow-up studies are needed.
Key points
Corpus callosotomy could reduce the frequency of overall seizures and traumatic falling seizures in patients with pediatric intractable epilepsy and mitochondrial dysfunction.
Corpus callosotomy has not been indicated for epileptic patients with metabolic causes; therefore, this study has implications for pediatric neurologists and epileptologists.
Corpus callosotomy could lead to improved life-saving options and quality of life improvements in patients with few options.
Footnotes
Acknowledgements
The authors are grateful to the patients, families, and all staff involved in this study, particularly the surgical team, pediatric neurologists, and statistical consultants. This project was performed without any financial support.
Ethics statement
We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines. This study was carried out in accordance with the tenets of the Declaration of Helsinki and the recommendations of the Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine, which approved the protocol (approval number 3-2017-0168). Written informed consent was obtained from patients or guardians of all patients.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.