
Abstract
Prolonged-release fampridine (PR-FAM), a potassium channel blocker, is approved for improving walking ability in patients with multiple sclerosis (MS). Beyond this, positive effects on other MS symptoms like fatigue, cognition, and tremor have been described. To our knowledge, a positive effect of PR-FAM on spinal myoclonus has not been described so far. Here, we report a 32-year-old female with myoclonus after cervical myelitis affecting both hands which markedly improved after administration of PR-FAM. Treatments used before such as carbamazepine or levetiracetam had to be withdrawn because of intolerable side effects or lack of efficacy. The positive effect of PR-FAM could be confirmed by transient suspension. PR-FAM may be considered as a treatment option in refractory spinal myoclonus after myelitis in selected cases.
Introduction
Myoclonus of spinal origin is a rare clinical manifestation of structural lesions of the central nervous system arising from various etiologies, for example, myelitis. 1 Pathophysiologically, the loss of inhibition of spinal interneurons results in hyperexcitation of anterior horn cells. 2 Given the limited data on symptomatic treatment of spinal myoclonus and lacking evidence from controlled clinical trials, current treatment strategies are based on case reports or series only. 3 We report a female patient suffering from myoclonus after cervical myelitis in whom prolonged-release fampridine (PR-FAM) had a very favourable effect, previously not reported in the literature.
Methods
We describe patient’s history, clinical, laboratory, electromyography (EMG) and imaging data. The effect of PR-FAM was documented by video recording. Written informed consent for patient information and videos to be published was provided by the patient.
Case description
A 32-year-old, left-handed, otherwise healthy female presented with progressive sensory symptoms of both legs and left arm. She had received a tick-borne encephalitis (TBE) booster vaccination 4 weeks before admission. Neurologic examination revealed hypoesthesia and paresthesia in both legs below the knees and in the left forearm and hand, furthermore a weakness of the left hand with fine motor impairment. Spinal magnetic resonance imaging (MRI) showed myelitis at level C4/C5; cerebrospinal fluid (CSF) analysis revealed lymphocytic pleocytosis (10 leucocytes/µl) with 6 oligoclonal bands only in CSF. Cranial MRI was normal. Further diagnostic workup revealed negative results for infectious origins, aquaporin-4 and MOG antibodies and vasculitis parameters. The patient was diagnosed with autoimmune myelitis, possibly triggered by the previous TBE booster vaccination; diagnostic criteria for multiple sclerosis (MS) were not fulfilled. Repeat administration of high-dose glucocorticosteroids resulted in incomplete remission, suspension was followed by symptoms worsening. Intravenous immunoglobulins (2 g/kg body weight) resulted in stabilization with residual mild sensorimotor deficits of the left hand.
Approximately 5 months after clinical onset of myelitis, the patient complained about irregular jerky movements of both hands, particularly affecting the left hand. Clinical examination revealed irregular myoclonus affecting all fingers of both hands sparing the thumbs (Supplemental Video 1 and 2). Myoclonus was confirmed by EMG of the left abductor digiti minimi muscle (Figure 1(a)), also differentiating it from tremor. Patient’s daily as well as professional activities were markedly impaired hereby. Treatment with primidone up to 31.25 mg, propranolol up to 30 mg and levetiracetam up to 1000 mg daily were ineffective (Figure 2). Carbamazepine prolonged release up to 600 mg daily markedly reduced myoclonus but was not tolerated because of marked fatigue. Treatment with PR-FAM 10 mg b.i.d., approved for improving walking ability in adult MS patients, was considered based on published positive effects on various MS symptoms. 4 PR-FAM resulted in a rapid and marked reduction of myoclonus of both hands within 1 day (Supplemental Video 3 and 4), improving fine motor skills and daily as well as professional activities. EMG confirmed the clinical findings (Figure 1(b)). No immunotherapy was given at that time. After pausing PR-FAM for 2 days by the patient due to leg cramps, myoclonus of both hands increased to the former intensity, again rapidly improving after PR-FAM intake. Leg cramps could not be attributed to PR-FAM intake, as they persisted in the PR-FAM free interval. PR-FAM was well tolerated without any side effects.
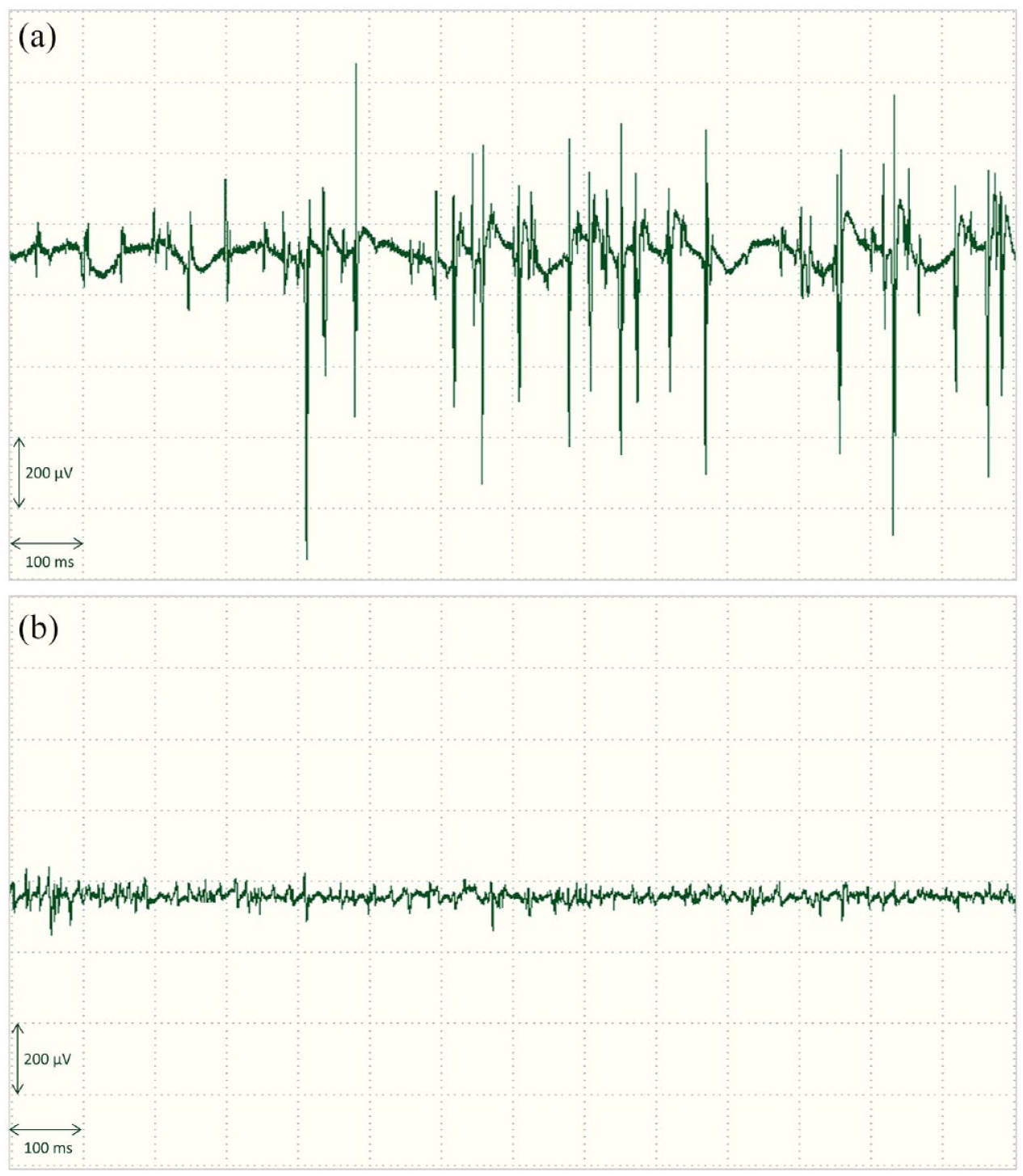
Needle electromyography of left abductor digiti minimi muscle; (a) myoclonus before PR-FAM (January 2021) and (b) marked reduction after PR-FAM initiation (March 2021).

Myoclonus responding to treatments applied (colour intensity of grey bar indicates symptom severity; the darker, the higher myoclonus intensity).
Discussion
We report a female patient markedly responding to PR-FAM for myoclonus after cervical myelitis. The deterioration of myoclonus during transient suspension of PR-FAM and improvement after continuation, clearly proves the therapeutic effect and argues against a spontaneous recovery. A beneficial effect of PR-FAM on myoclonus, especially of spinal origin, has not yet been described to our knowledge.
Spinal myoclonus after myelitis is a rare event and the pathophysiology is poorly understood. Proposed mechanisms of spinal myoclonus include the loss of inhibitory interneurons, the loss of inhibition from descending pathways, hyperactivity of local anterior horn cells, and changes in the distribution or activity of voltage-gated channels in the membrane (Figure 3). Ultimately, this results in a hyperexcitability of anterior horn cells leading to spontaneous discharges, which clinically manifests as myoclonus.5,6 Spinal myoclonus can be subclassified into segmental spinal myoclonus (SSM) and proprioceptive spinal myoclonus (PSM). In SSM, myoclonus originates from a few segments of the spinal cord and results in rhythmic or semi-rhythmic jerks that are unaffected by state of consciousness, motor activity, or stimulus. PSM is caused by an involvement of the propriospinal tracts connecting different spinal segments leading to multisegmental contractions, predominantly in the trunk muscles that may be stimulus-sensitive. 7 Since myoclonus was restricted to the arms not affecting the trunk or lower extremities, we assume SSM in the case reported. However, not typical for SSM in our report is the relatively short duration of the myoclonic bursts, which are usually up to 1000 ms, 7 and the finding that the affected myotomes (C7-8) are located below the myelitis detected in MRI (C4-5). Nevertheless, given the absence of brain lesions in MRI, the temporal relationship between the cervical myelitis and myoclonus onset, and the manifestation of myoclonus in cervical myotomes, we assume a spinal origin in our patient. No other underlying cause for myoclonus, like co-morbidity or co-medication could be found.

Potential effects of PR-FAM (orange), carbamazepine (blue) and levetiracetam (green) on spinal segmental myoclonus.
Treatment options for spinal myoclonus are limited, based on few case reports and series only.3,8 Positive effects have been reported for anticonvulsants (e.g. levetiracetam, clonazepam), (intrathecal) baclofen or botulinum toxin. 8 However, benefit is often limited and the pharmacological effect and pathophysiological mechanisms are not fully understood. Due to intolerable side effects including fatigue (carbamazepine) or insufficient response (primidone, propanolol, levetiracetam) in our patient, treatment of disabling myoclonus with PR-FAM was initiated with a marked reduction of myoclonus of both hands.
PR-FAM is a lipid-soluble, selective potassium channel blocker and is approved to improve walking ability in patients with MS. Positive effects of PR-FAM on inflammatory central nervous system disorders outside its approval have been reported for tremor, 9 central eye movement disorders, 10 vision, 11 cognition,12 –14 and verbal fluency, 15 among others.
A major role for ion channel dysfunction in the development of MS symptoms and in the processes underlying axonal degeneration is known. 16 During regeneration, redistribution of ion channels along the axon has been observed. 17 Increased expression of potassium channels due to demyelination contributes to conduction failure in MS by accelerating membrane repolarization. 16 In addition, demyelinated and possibly hyperexcitable axons may emit spontaneous discharges, which may present clinically as myoclonus. 18 PR-FAM affects demyelinated nerve fibres by enhancing their conduction velocity through blockade of voltage-gated potassium channels. 19 Based on the important function of potassium channels in modulating axonal excitability, the positive effect of PR-FAM on myoclonus may be explained. Potential effects of PR-FAM and other drugs on spinal myoclonus are displayed in Figure 3.
Our report has several limitations. Based on the single case presented, no general conclusions regarding the effect of PR-FAM in spinal myoclonus or myoclonus after myelitis, respectively, can be drawn. The patient reported suffered from autoimmune myelitis after TBE booster vaccination, not fulfilling diagnostic criteria for MS. However, the existing literature on PR-FAM and spinal myoclonus after myelitis predominantly refers to patients with MS. Therefore, discussing the pathophysiology of myoclonus and treatment effects in our report against the backdrop of findings in MS, even though also an autoimmune disorder frequently manifesting with myelitis, may have limitations. In addition, some therapeutic agents, such as primidone, propranolol and levetiracetam, were administered only for a short period of time or at a low dose before being discontinued due to a lack of efficacy or side effects, and some of them were given in an overlapping regimen. Due to these limitations, the effectiveness of these agents cannot be estimated finally in our patient.
Conclusion
Owing to only few available and not approved treatment options, treatment of spinal myoclonus is challenging regarding efficacy as well as tolerability. In our patient with myoclonus and a spinal cord lesion, PR-FAM resulted in a sustained and marked reduction of myoclonus, allowing the patient to return to her former daily activities with excellent tolerability. This positive effect has not been reported so far and PR-FAM may be considered as a treatment option for myoclonus in selected cases.
Supplemental Material
sj-docx-1-tan-10.1177_17562864221083608 – Supplemental material for Prolonged-release fampridine for the treatment of myoclonus after cervical myelitis: a case report
Supplemental material, sj-docx-1-tan-10.1177_17562864221083608 for Prolonged-release fampridine for the treatment of myoclonus after cervical myelitis: a case report by Mona Klara Ros Müller, Monika Christ, Markus Naumann and Antonios Bayas in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-2-tan-10.1177_17562864221083608 – Supplemental material for Prolonged-release fampridine for the treatment of myoclonus after cervical myelitis: a case report
Supplemental material, sj-docx-2-tan-10.1177_17562864221083608 for Prolonged-release fampridine for the treatment of myoclonus after cervical myelitis: a case report by Mona Klara Ros Müller, Monika Christ, Markus Naumann and Antonios Bayas in Therapeutic Advances in Neurological Disorders
Footnotes
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Antonios Bayas received personal compensation from Merck Serono, Biogen, Novartis, TEVA, Roche, Sanofi-Aventis/Genzyme, Celgene/Bristol-Myers Squibb and Janssen; he received grants for congress travel and participation from Biogen, TEVA, Novartis, Sanofi/Genzyme, Merck Serono and Celgene. None related to this report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.