
Abstract
The terms autoimmune dementia and autoimmune encephalopathy may be used interchangeably; autoimmune dementia is used here to emphasize its consideration in young-onset dementia, dementia with a subacute onset, and rapidly progressive dementia. Given their potential for reversibility, it is important to distinguish the rare autoimmune dementias from the much more common neurodegenerative dementias. The presence of certain clinical features [e.g. facio-brachial dystonic seizures that accompany anti-leucine-rich-glioma-inactivated-1 (LGI1) encephalitis that can mimic myoclonus] can be a major clue to the diagnosis. When possible, objective assessment of cognition with bedside testing or neuropsychological testing is useful to determine the degree of abnormality and serve as a baseline from which immunotherapy response can be judged. Magnetic resonance imaging (MRI) head and cerebrospinal fluid (CSF) analysis are useful to assess for inflammation that can support an autoimmune etiology. Assessing for neural autoantibody diagnostic biomarkers in serum and CSF in those with suggestive features can help confirm the diagnosis and guide cancer search in paraneoplastic autoimmune dementia. However, broad screening for neural antibodies in elderly patients with an insidious dementia is not recommended. Moreover, there are pitfalls to antibody testing that should be recognized and the high frequency of some antibodies in the general population limit their diagnostic utility [e.g., anti-thyroid peroxidase (TPO) antibodies]. Once the diagnosis is confirmed, both acute and maintenance immunotherapy can be utilized and treatment choice varies depending on the accompanying neural antibody present and the presence or absence of cancer. The target of the neural antibody biomarker may help predict treatment response and prognosis, with antibodies to cell-surface or synaptic antigens more responsive to immunotherapy and yielding a better overall prognosis than those with antibodies to intracellular targets. Neurologists should be aware that autoimmune dementias and encephalopathies are increasingly recognized in novel settings, including post herpes virus encephalitis and following immune-checkpoint inhibitor use.
Keywords
Rationale
Autoimmunity is a cause of cognitive decline that is potentially reversible, and, in the case of paraneoplastic syndromes, can lead to discovery of an underlying cancer. It is important for neurologists recognize these syndromes and know when testing is appropriate as early treatment typically results in better outcomes.
Introduction
When evaluating a patient with a cognitive disorder, one of the most important aspects is to distinguish reversible from irreversible causes. The presentation of immune-mediated brain dysfunction can range from acute encephalitis and status epilepticus to an insidious cognitive disorder. Therefore, given the potential for good response to immunotherapy, it is essential that neurologists evaluating a patient with new onset dementia consider autoimmune causes. Major advances in antibody biomarker discovery have allowed us to better identify these immune-mediated cognitive disorders. These disorders were initially recognized to occur as an idiopathic autoimmune phenomenon or as a cancer-related immune response (paraneoplastic disorder). It is now recognized that autoimmune dementias can occur in other novel settings, such as post-herpes virus encephalitis, 1 post-transplant, 2 or after cancer treatment with immune checkpoint inhibitors (ICI). 3 The expanding range of clinical scenarios in which autoimmune dementia can arise emphasizes the need for all neurologists to recognize and understand these disorders. In this article, we will highlight the current understanding of autoimmune dementia, its clinical presentation, diagnostic biomarkers, and treatments.
The overlap and differences between autoimmune dementia and encephalopathy
Dementia has been defined by the World Health Organization (WHO) as a syndrome, usually chronic and progressive, with deteriorating cognitive function beyond what is expected with normal aging. 4 The syndrome can affect memory, thinking, orientation, comprehension, calculation, learning, capacity, language and judgment, emotional control, social behavior, and motivation, and is without impairment in consciousness. 4 A recent updated Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) criteria uses the terminology major neurocognitive disorder to describe this syndrome. 5 The term encephalopathy, strictly speaking, is defined as a disease process that affects brain function. The term encephalitis is used when an inflammatory cause, which can be autoimmune or infectious, is at play. 6 While grave alterations in consciousness have historically been associated with encephalopathy/encephalitis, and do occur with many of these patients [e.g. new onset refractory status epilepticus (NORSE) or florid limbic encephalitis], it is also recognized that many patients with autoimmune encephalitis/encephalopathy will not have alteration in consciousness and have a subacute/rapidly progressive dementia syndrome in which they present for evaluation to an outpatient clinic rather than acutely to a hospital. Moreover, some characteristic dementia syndromes, such as Lewy Body Disease, are recognized to have prominent fluctuations in arousal, which makes distinction between neurodegenerative and autoimmune etiologies of dementia more difficult. 7 This article will focus on patients who present with more of a subacute dementia syndrome, realizing that patients with the same disease [e.g., anti-leucine-rich-glioma-inactivated-1 (LGI1) encephalitis/dementia] may present as a rapidly progressive dementia without altered consciousness or acutely to the hospital with severe encephalopathy and impaired consciousness. The difficulties in distinguishing these syndromes is highlighted by up to a third of patients with autoimmune etiologies of dementia initially given a diagnosis of an irreversible neurodegenerative dementia or prion disorder. 8
Nomenclature
Autoimmune dementia is a term that describes cognitive decline of an autoimmune basis.
8
Neurologists are most familiar with dementia occurring with an insidious onset of cognitive decline in older patients – a situation in which the vast majority of causes are degenerative (e.g., Alzheimer’s disease). However, the likelihood of encountering a cognitive decline of immune-mediated origin is higher in specific clinical settings. For instance, autoimmune etiologies of dementia represent a higher proportion of cases in young onset (<45 years) and early onset (<65 years) dementia (see below).9,10 Also, rapidly progressive dementia that has a subacute onset, with worsening over weeks to months, is a category in which autoimmune etiologies are over-represented.11–13 However, it should be noted that autoimmune etiologies can also occur in the elderly, and up to one-third of these can be misdiagnosed with an irreversible neurodegenerative disorder.
8
When the autoimmune dementia occurs in the setting of an immune-mediated response to an underlying cancer, the term paraneoplastic dementia/encephalitis may be used. A number of autoantibody biomarkers of immune-mediated cognitive disorders have been discovered, and, thus, these disorders may be named by the antibody they associate with [anti-N-methyl-
Demographic and clinical characteristics of the main CNS autoantibodies targeting cell-surface antigens associated with cognitive impairment/encephalopathy according to the largest series reported.

AMPAR, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; ANA, anti-nuclear antibody; CASPR2, contactin associated protein 2; CNS, central nervous system; DPPX, dipeptidyl aminopeptidase-like protein 6; FBDS, facio-brachial dystonic seizures; GABAAR, γ-aminobutyric acid type-A receptor; GABABR, γ-aminobutyric acid type-B receptor; GI, gastrointestinal; GlyRα1, glycine receptor subunit alpha-1; IgLON5, immunoglobulin-like cell adhesion molecule IgLON family member 5; LE, limbic encephalitis; LGI1, leucine-rich glioma inactivated 1; mGluR5, metabotropic glutamate receptor 5; NMDAR, N-methyl-D-aspartate receptor; ON, optic neuritis; PERM, progressive encephalopathy with rigidity and myoclonus; SPS, stiff-person syndrome. (Modified with permission from Table 1 in ref. 75 ).
Pathophysiology
Antibodies can be stratified into two categories based on their antigenic target location within the cell 14 :
Antibodies that bind to cell-surface/synaptic antigens (Table 1). In patients with these antibodies (e.g. anti-NMDAR encephalitis), it is suspected or has been confirmed that the antibody is directly pathogenic.15,16,17 The binding of the antibody may result in dysfunction of the receptor, internalization, antibody mediated cytotoxicity, or activation of complement. The frequency of cancer is less (~ 50%) and these disorders tend to respond well to immunotherapy, particularly antibody depleting therapy [e.g., plasma exchange (PLEX), 18 rituximab]. 19
Antibodies that bind intracellular antigens (Table 2). These encompass what were traditionally referred to as the classical paraneoplastic disorders, where antigens within the cytoplasm or nucleus are targets of the antibody. The exact pathophysiologic mechanisms for autoantibodies targeting intracellular antigens is unknown. In vitro studies suggest that the antibody is not directly pathogenic but rather a biomarker of a cytotoxic CD8-T-cell mediated process [e.g., anti-neuronal nuclear antibodies type-1 (ANNA-1)/anti-HU associated limbic encephalitis],20,21 although these findings have not yet been reproduced in animal models. Postmortem findings may also support a cytotoxic damage in these patients. 22 These disorders tend to be associated more frequently with an accompanying cancer (>80%) and respond less to immunotherapy.
Demographic and clinical characteristics of the main CNS autoantibodies targeting intracellular antigens associated with cognitive impairment/encephalopathy according to the largest series reported.

AK5, adenylate kinase 5; ANNA-1/2, anti-neuronal nuclear antibodies type-1/2; CNS, central nervous system; CRMP5, collapsin response-mediator protein-5; GAD-65, glutamic acid decarboxylase-65; GFAP, glial fibrillary acidic protein; GI, gastrointestinal; LE, limbic encephalitis; NfL, neurofilament light chain; PCA-2/MAP1B, Purkinje cells antigens-2/microtubule-associated protein 1B; SPS, stiff-person syndrome. (Modified with permission from Table 2 in in ref. 75 ).
Epidemiology
Autoimmune dementia and encephalopathy is less common than other causes of cognitive decline, such as neurodegenerative diseases. A study evaluating the causes of dementia in young patients (ages 17–45 years) found that neurodegenerative dementia was the most common cause (31.1%), followed by autoimmune or inflammatory etiologies (21.3%). 10 A more recent study found immune-mediated diseases accounted for 46% of rapidly progressive dementia in Brazil, 12 while it was lower at 18% in India, where infectious diseases predominated. 11 In a separate study from Spain, autoimmune/paraneoplastic causes accounted for only 4%. 13 The frequency of autoimmune dementia as a proportion of all dementia is lower at an older age as neurodegenerative etiologies become more common, but certain antibodies do have a preponderance for older individuals (e.g., anti-LGI1 autoantibodies). In patients with rapidly progressive dementia that was not secondary to prion disease, autoimmunity was a cause of 9–13% of cases in tertiary referral centers.23,24 Therefore, although it is critical to recognize autoimmunity as a cause of dementia, it is important to know it is not as common as other etiologies, and the diagnosis should be made carefully. However, some epidemiologic studies are based on older data and autoimmune dementias may be underdiagnosed in these cohorts. Gender differences in autoimmune dementia are recognized and vary depending on the accompanying autoantibody. For instance, anti-NMDAR encephalitis predominate in females, while anti-LGI1 encephalitis is more common in males.
Clinical features
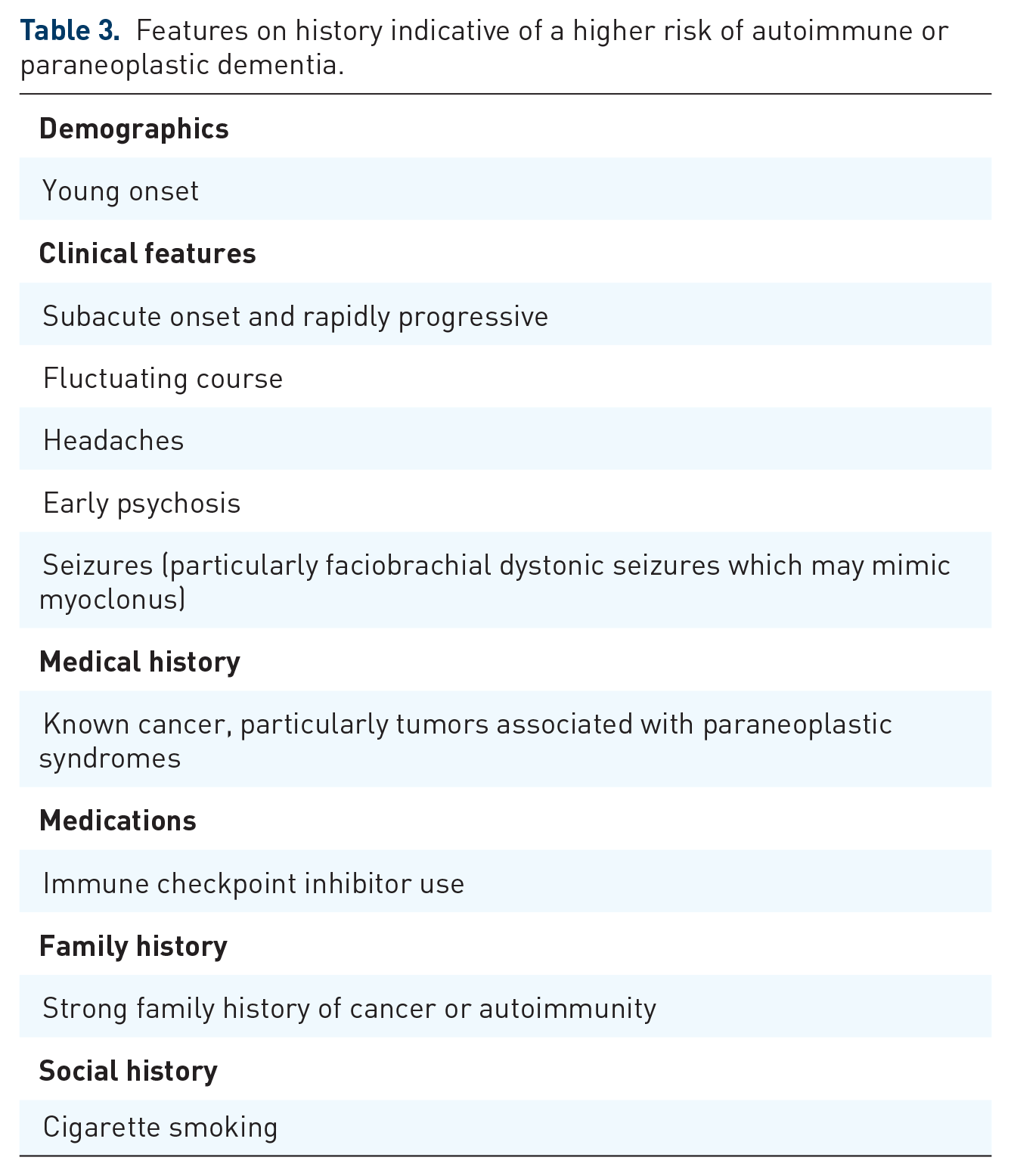
Certain clinical features that accompany cognitive decline may be a clue to an autoimmune dementia, and these are summarized in Tables 1 and 2. In addition, clinical features that give a clue to autoimmune dementia are summarized in Table 3. The early prodromal phase in autoimmune dementia may consist of non-specific or non-neurologic symptoms. Episodes of severe weight loss (median of 10–20 kg), with or without diarrhea, may precede encephalopathy/dementia, and have been reported with dipeptidyl aminopeptidase-like protein 6 (DPPX) and occassionally with glial fibrillary acidic protein (GFAP) autoantibodies, the latter often preceded by a viral prodrome or vaccination.25,26 The onset of cognitive decline in autoimmune cases is typically acute to subacute, and worsens rapidly with the memory domain impacted disproportionately. 8 A prior study comparing patients with autoimmune dementia to those with other causes of dementia, a subacute onset, fluctuating course, tremor, and headache were symptoms that were more likely to suggest an autoimmune cause. 8 Short-term memory loss developing subacutely without severe loss of consciousness can occur with limbic encephalitis. 27 Following the onset of the cognitive/behavioral symptoms, the development of seizures early in the course is a clue to an autoimmune etiology and is rare with neurodegenerative dementia, usually occurring at the end-stage.8,27 Facio-brachial dystonic seizures are a unique and characteristic manifestation of anti-LGI1 encephalitis and can be mistaken for myoclonus or non-epileptic phenomenon, and, hence, up to half of patients with these episodes are initially diagnosed as having Creutzfeldt Jakob Disease (CJD) or psychiatric disease. 28 The hallmark feature consists of short-lived episodes of dystonic posturing of the face, arm, or both, with the leg also sometimes impacted.28-30 Patients often retain awareness and may complain of dropping items from their hand. The episodes occur frequently (multiple per hour is typical) and can alternate from side to side. Paroxysmal dizzy spells are also recognized in association with anti-LGI1 encephalitis. 31 Psychosis is another common feature of autoimmune encephalitis, particularly with anti-NMDAR antibodies. 16 Other presentations have been reported including a case mimicking fronto-temporal dementia 32 ; the subacute onset, rapid progression, and absence of a family history would help distinguish an autoimmune etiology from a neurodegenerative cause. Sleep disorders are increasingly recognized; parasomnias and sleep-disordered breathing is a major feature of immunoglobulin-like cell adhesion molecule IgLON family member (IgLON5) antibodies, which has a chronic presentation and may be accompanied by a bulbar disorder and gait dysfunction sometimes mimicking progressive supranuclear palsy.33,34 A rapidly progressive dementia with insomnia, hyperhidrosis, and peripheral nerve hyper-excitability (painful cramps and fasciculations) should raise suspicion for Morvan’s syndrome, which is associated with contactin-associated protein 2 (CASPR2) antibodies. 35 While isolated Parkinsonism is uncommon, a clinical syndrome of progressive encephalomyelitis, rigidity, and myoclonus (PERM) is recognized (often with accompanying hyperekplexia) and occurs in association with GAD65 or glycine receptor antibodies.36,37 Other movement disorders that can be encountered include autoimmune/paraneoplastic chorea [e.g. collapsin response mediator protein 5 (CRMP5)/anti-CV2], 38 jaw dystonia [anti-neuronal nuclear antibody type-2 (ANNA-2)/anti-Ri], 39 and oro-facial dyskinesias (anti-NMDAR encephalitis). 16 Episodic ataxia has been reported with CASPR2 antibodies, 40 while many other antibodies can associate with a progressive ataxia combined with an autoimmune dementia (Table 1). Opsoclonus-myoclonus, jaw dystonia, and laryngospasm may associate with ANNA-2/anti-Ri antibodies. 41 Visual dysfunction can occur in autoimmune dementia with optic disc edema (GFAP-IgG), 42 or retinopathy (CRMP5-IgG/anti-CV2). 43
Features on history indicative of a higher risk of autoimmune or paraneoplastic dementia.
Diagnostic testing
Cognitive assessment
Bedside cognitive testing, involving tests such as the Short Test of Mental Status (Kokmen) or Mini Mental Status Exam are useful when possible to determine the severity of dementia and to monitor the progression over time. 8 Formal neuropsychological testing can be useful to better identify abnormalities and provide a baseline from which immunotherapy response can be judged (see below). On both assessments, short-term memory loss appears to be the most severely impacted cognitive domain. 8 However, some patients may be too unwell to participate acutely, depending on the severity of the cognitive disorder.
Imaging
Magnetic resonance imaging (MRI) is helpful to diagnose autoimmune etiologies of dementia and encephalopathy and exclude other causes of cognitive impairment. Unilateral or bilateral fluid attenuated inversion recovery (FLAIR) or T2-hyperintensity of mesial temporal lobes with or without gadolinium enhancement is characteristic of limbic encephalitis (Figure 1a,c) but can also be seen with epilepsy and herpes simplex virus (HSV) encephalitis. 44 Basal ganglia T1 and T2 hyperintensities can be seen in some patients with facio-brachial dystonic seizures and anti-LGI1 encephalitis 28 ; basal ganglia T2-hyperintensities may be seen in association with multiple other antibodies including anti-NMDAR, anti-Ma2, or anti-CRMP5.45-47 Anti-Ma2 antibodies may also have diencephalic involvement, particularly around the surface of the third ventricle. 45 Signal abnormalities within the basal ganglia and thalamus, particularly when accompanied by restricted diffusion, are recognized with non-autoimmune dementia/encephalopathy such as CJD or Wernicke encephalopathy.48-50 γ-Aminobutyric acid type-A receptor (GABAAR) antibodies may have multiple cortical and subcortical T2-hyperintensities. 51 Radial perivascular enhancement is typical of GFAP-IgG (Figure 1b). 42 Susac syndrome is an immune mediated vascular disorder that may reveal “snow-ball” and “spoke” type lesions in the center of the corpus callosum, or punctate restricted diffusion that may form a “string of pearls” sign along the internal capsule. 52 Restricted diffusion and micro-hemorrhages illustrated by darkening on gradient echo or susceptibility weighted imaging often accompanied by leptomeningeal enhancement may be encountered in central nervous system (CNS) vasculitis or amyloid beta related angiitis, and should be considered in the appropriate setting. 53 CNS vasculitis is recognized to occur in a paraneoplastic context in association with lymphoma. 54 Most neurodegenerative disorders have accompanying atrophy; moderate-to-severe atrophy without signal abnormality should raise suspicion for a non-autoimmune dementia.

MRI examples of autoimmune dementia. (a) Bilateral T2-hyperintensities in the mesial temporal lobe are shown in a patient with autoimmune limbic encephalitis associated with GAD65 autoantibodies. (b) Radial perivascular enhancement is shown in a patient with GFAP autoantibodies. (c) Bilateral mesial temporal T2-hyperintensities consistent with limbic encephalitis and occurring after immune checkpoint inhibitor use with an accompanying unclassified neural autoantibody detected with follow-up MRI 1 month later revealing bilateral temporal lobe atrophy (d).
Electroencephalogram
Electroencephalogram (EEG) may assist in the diagnosis of patients with suspected autoimmune dementia. In anti-NMDAR encephalitis, 30% of patients have a pattern of extreme delta brush with rhythmic delta (1–3 Hz) activity with bursts of beta (20–30 Hz) superimposed on the delta waves. 55 Occasionally, this pattern may also be seen in patients with other conditions including: non-autoimmune mesial temporal lobe epilepsy, hypoxic ischemic encephalopathy, and brain tumors. Other findings on EEG in autoimmune dementia are non-specific, including diffuse or focal slowing and epileptiform activity, 56 the latter favoring an autoimmune over most neurodegenerative etiologies. 57 Of note, facio-brachial-dystonic seizures rarely have any ictal EEG correlate. 28 EEG can also provide clues to alternative etiologies, with periodic sharp waves suggestive of CJD, 58 and periodic slow wave complexes suggestive of subacute sclerosing pan-encephalitis post-measles infection. 59
Laboratory testing
Laboratory evaluation, including serum and cerebrospinal fluid (CSF) testing are important to evaluate patients with suspected autoimmune dementia. An optimal panel of routine serum tests include a complete blood count; sedimentation rate; C-reactive protein; markers of liver, renal, and thyroid function; electrolytes; vitamins (especially group B-vitamins like B1 and B12) 60 ; and, as appropriate, markers or toxic/metabolic encephalopathies (e.g., benzodiazepines, opioids); and cancer CSF assessment (cytology, flow cytometry). Neurologic involvement of a rheumatologic disorder can occasionally, initially or during its course, manifest with a subacute dementia syndrome.61,62 Thus, serum testing for non-neural antibodies such as antinuclear antibody, double-stranded DNA antibodies, antibodies to the extractable nuclear antigen, anti-neutrophilic cytoplasmic antibodies (ANCA), rheumatoid factor, phospholipid antibodies, beta 2 glycoprotein-1 antibodies, lupus anticoagulant, and IgG4 can be considered when clinical features are suggestive to assess for neurologic involvement of rheumatologic disorders. 63
CSF analysis may show evidence of inflammation, including pleocytosis, elevated oligoclonal bands, and elevated IgG index, in up to 50% of patients. 8 It is very rare for CSF pleocytosis and elevated oligoclonal bands to be encountered in neurodegenerative disorders.64,65 It is important to note that an inflammatory CSF does not confirm the diagnosis of autoimmune dementia nor does a normal CSF exclude it; anti-LGI1 encephalitis and other autoantibody-associated encephalitides may have a normal CSF profile, and, in those situations, detection of the antibody is particularly useful. 66 Other CSF testing for alternative causes of dementia can be helpful, including levels and ratio of phospho-tau and amyloid-β-42 to evaluate for Alzheimer’s dementia, 67 and real-time quaking-induced conversion (RT-QuIC) to evaluate for prion disorders. 68
Extensive screening for viral, bacterial, and fungal/parasitic infections is recommended in both serum and CSF, especially in immunocompromised patients or patients with recent history of travel to a region where infectious encephalitis is endemic.
Other diagnostic investigations
Evaluation for infectious, neoplastic, and toxic or metabolic etiologies should be undertaken prior to initiating immunotherapy. Brain fludeoxy-glucose-positron-emission-tomography (FDG-PET) in patients with autoimmune encephalitis can show focal or diffuse areas of hypo- or hyper-metabolic activity. 69 In anti-NMDAR encephalitis, medial occipital hypometabolism is recognized. 70 In patients who do not respond to immunotherapy, or if the diagnosis remains unclear, brain biopsy may be considered, and the presence of inflammatory infiltrates may support the diagnosis of autoimmune encephalitis, but is not diagnostic. Typically brain biopsy is most helpful in ruling out other causes of cognitive impairment such as a primary brain tumor or lymphoma.
Neural autoantibody testing
Utility
Testing of neural antibodies in patients with appropriate clinical history can confirm the diagnosis of autoimmune dementia. It is important to test for antibodies prior to initiating treatment as testing after starting therapy may lead to false positive (e.g. IVIg), 71 or false negative results [e.g., PLEX (unpublished observations from E.P.F)]. The sample with optimal sensitivity for autoantibody detection varies; CSF is preferable for anti-NMDAR and anti-GFAP antibodies, while serum is preferable for anti-LGI1. 6 In many cases where an autoimmune etiology is suspected, testing both serum and CSF is preferred. 72 In most cases it is best to test a panel of antibodies as most clinical syndromes may be caused by a wide variety of autoantibodies (Table 1), and, in rare patients with multiple positive results, the profile of antibodies may help refine the cancer search. The range of antibodies that associate with autoimmune dementia are summarized and referenced in Tables 1 and 2.
Antibody testing methodology
Older generation techniques using immunoprecipitation have an increased risk of false positivity, where up to 5% of normal or disease controls can be positive.73, 74 Newer generation techniques using cell-based assays have reduced the risk of false positivity to approximately 0.2%. 74 It is also recognized that tissue immunofluorescence/immunohistochemistry in combination with western blot (mostly used for antibodies targeting intracellular antigens), or in combination with cell-based assays (generally used only for antibodies directed against cell-surface antigens), is optimal, and caution is advised when using western blot alone where there is a high risk of false positivity. 75 An initial screening with tissue immunofluorescence/immunohistochemistry in specialized laboratories is generally recommended as it may reveal unexpected, or as yet not classified, antibodies.
Pitfalls
Given the relative rarity of autoimmune dementias in the population, it is important to first exclude other more common etiologies (e.g., neurodegenerative or metabolic disorders). 76 Testing for antibodies in very low probability situations (e.g., classical dementia due to Alzheimer’s disease) increases the risk of false positives, particularly with antibodies detected by older generation techniques such as immunoprecipitation. 74 Refinement of the antibody targets has also led to improved categorization of some antibody-associated cognitive disorders. For example, voltage-gated-potassium-channel-complex antibodies were initially identified as the antibody target in some patients with autoimmune dementia/encephalitis, but it was later shown that only antibodies bound to certain proteins that associate with the channel (LGI1, CASPR2) were clinically relevant, and antibodies that bind to the channel but not LGI1 or CASPR2 were of no clinical significance.77,78 With some autoantibodies, the titer may be useful; for example, glutamic acid decarboxylase 65 (GAD-65) antibodies may be found at low titer in up to 8% of the general population, 80 while high titers can be associated with PERM, 81 limbic encephalitis, and can occasionally mimic CJD. 82 Further, clinically significant antibodies are typically of the IgG isotype. Anti-thyroid peroxidase (TPO) antibodies are not specific and are seen in anywhere from 10% to 25% of the normal population.83,84 These antibodies have been associated with a disorder termed Hashimoto’s encephalopathy, and this syndrome has been reported to occasionally manifest with a rapidly progressive dementia mimicking CJD. 85 However, caution is advised as the high frequency of these antibodies in the general population precludes their diagnostic utility, and many patients can be assigned with this diagnosis when an alternative etiology for their cognitive impairment is present. 86
Cancer investigations
Cancer investigation should be directed to particular antibody positivity status, as outlined in Table 1. 87 Age- and sex-appropriate cancer screening should be up to date, including colonoscopies and mammograms. Cancer screening typically starts with a computed tomography (CT) chest, abdomen, and pelvis. Whole body FDG-PET has increased sensitivity for cancer in paraneoplastic disorders, and should be considered if the initial cancer screen is unrevealing, particularly when antibodies with high positive predictive value for cancer are detected. 88 Ovarian or testicular ultrasounds and skin evaluation for melanoma should also be considered as applicable. In patients with antibodies that have a strong association with cancer such as ANNA-1/anti-Hu antibodies if the initial cancer evaluation is negative, cancer screening should be repeated at 6 months and 1 year as occult cancers may occasionally emerge in follow-up imaging.
Emerging clinical settings
Besides the traditional idiopathic and paraneoplastic forms, novel clinical scenarios are increasingly recognized to be at higher risk for development of autoimmune dementia and encephalopathies:
In patients with HSV encephalitis, about one-third of patients develop a subsequent autoimmune encephalitis in the following 4–6 weeks, likely triggered by neural epitopes released during the viral infection. Neural autoantibody testing is highly recommended after HSV encephalitis in patients who relapse or worsen after an initial improvement, as the probability of an autoimmune etiology is high. Anti-NMDAR antibodies are the most common accompaniment. 1
Post-transplant patients may paradoxically develop autoimmunity despite being on maintenance anti-rejection immunosuppressive medications and manifestations can include autoimmune dementia/encephalopathy. This is thought to be due to an imbalance between T and B cell immunosuppression that may result in systemic or neurological autoimmunity. 2
ICI are increasingly recognized as an effective treatment for many types of cancer. However, the augmented immune system activation induced by ICI may result in autoimmunity directed against any organ, including the central and peripheral nervous systems. 3 In patients with CNS involvement, encephalopathy represents the most common manifestation, variably including brainstem/limbic encephalitis, slowly progressive cognitive impairment mimicking a neurodegenerative disorder, 89 and posterior reversible encephalopathy syndrome (PRES). 90 Clinical and MRI features may be indistinguishable from their idiopathic counterparts (Figure 1c,d). 3 Encephalopathy secondary to tumefactive demyelination, 91 granulomatosis, or cerebral vasculitis has also been described. 92 Specific neural autoantibodies can be detected in the serum and/or CSF in about 50% of cases, although the frequency of novel or yet unidentified antibodies detectable only in highly specialized laboratories seems higher compared with idiopathic cases. 3 Neurological symptoms typically manifest within the first 3 months of ICI treatment but can be observed up to 1 year after treatment discontinuation. 3 Symptoms should carefully be differentiated from other more common causes of encephalopathy seen in cancer patients (e.g., brain metastases, metabolic/medication-related). Care is also needed in patients with a pre-existing paraneoplastic encephalitis/dementia as use of immune-checkpoint inhibitors in such patients may accelerate the autoimmune neurologic disease leading to severe morbidity or death. 3
Treatment
Treatment and management of autoimmune dementias is multifaceted and requires treatment of the underlying autoimmune disease, management of symptoms and sequelae, and treatment of associated cancers when present. If there is underlying cancer, treatment of the malignancy may result in improvement in the neurologic syndrome; however, adjuvant immunotherapy is often necessary. The general principle guiding therapy is to utilize antibody or B-cell depleting agents for antibodies to cell-surface antigens and T-cell depleting agents for antibodies to intracellular antigens (see section Pathophysiology). Randomized controlled clinical trials in acute and maintenance treatment of autoimmune dementia are generally lacking, and therefore treatment recommendations are typically based on results from retrospective analyses and expert opinion. While specific studies on autoimmune dementia alone do not exist, studies of autoimmune or paraneoplastic syndromes that include antibodies that can result in autoimmune dementia have been undertaken. An open label trial compared the efficacy of plasmapheresis plus conventional cancer chemotherapy versus plasmapheresis plus oral cyclophosphamide in 20 patients with new-onset paraneoplastic neurological syndromes, and showed improvement or stabilization in 40% and 60% of cases, respectively. 93 Recently, a small randomized trial on 17 patients with anti-LGI1 or anti-CASPR2 encephalitis associated showed superiority of intravenous immunoglobulins over placebo for 50% reduction in seizure frequency from baseline, but did not assess cognitive outcomes. 94 A randomized, double-blind, placebo controlled trial on the efficacy of ocrelizumab (anti-CD20 monoclonal antibody) in patients with autoimmune encephalitis is ongoing. 95
Acute treatment
Acute immunotherapy typically includes steroids, intravenous immunoglobulin (IVIg), and PLEX. Methylprednisolone may be given intravenously at 1 g daily for 5 days, and sometimes continued with 1 g intravenously once weekly for 6–12 weeks. IVIg and PLEX may be considered as an alternative, or as an adjunct to, therapy in severe cases. IVIg is dosed at 0.4 g/kg/day for 5 days and then 0.4 g/kg once weekly for 6–12 weeks, and PLEX can be done every other day for 5–7 sessions.
In a prior Mayo Clinic study focused specifically on autoimmune dementia, most patients (64%) had improvement with first-line therapy, mostly within the first week of therapy. 8 Individual antibody types respond differently to therapy. Patients with anti-LGI1 encephalitis often respond well to initial corticosteroid therapy with resolution of cognitive impairment in the first few weeks. 30 Patients with anti-NMDAR encephalitis were shown to improve with first-line therapy in the first 4 weeks in half of cases, but returning to baseline function typically takes months to years. In this same study, half of the patients that did not improve received a second-line immunotherapy with subsequent improvement in final outcome. Therefore, patients with anti-NMDAR encephalitis are frequently initiated on second-line therapies such as rituximab or cyclophosphamide. 96
In patients with autoimmune dementia triggered by ICI, the recommended treatment consists of discontinuation of the causative drug, plus administration of high-dose intravenous corticosteroids, IVIg, and/or PLEX, and generally results in a favorable outcome. 3 However, a more aggressive approach with addition of rituximab or cyclophosphamide could be necessary in specific subsets of patients with worse prognosis (e.g., patients with neurological autoimmunity pre-existing to ICI treatment). 3 The decision to withdraw ICI should be evaluated carefully for each patient based on cancer response to treatment and severity of the neurological manifestations. Improvement has been reported in some cases with ICI-related neurological manifestations of moderate severity treated with immunotherapy only (without ICI discontinuation). 3 Depending on available cancer treatment options, ICI re-challenge may be considered, and seems safer in those with mild/moderate acute manifestations. 97 Further discussion on ICI-related toxicity is beyond the scope of this manuscript, but specific recommendations have been published. 98
Maintenance therapy
In patients that respond to acute immunotherapy a variety of maintenance steroid-sparing immunosuppressants may be considered in an attempt to try prevent relapses. Such treatments include azathioprine, methotrexate, mycophenolate, and rituximab. The decision for which maintenance immunotherapy to use depends on the antibody type, immunosuppressant medication availability, cost, and speed of onset (rituximab begins working within a few weeks, while mycophenolate and azathioprine may take 3–6 months to take effect). Patients should be regularly monitored (every 6–8 months) for disease-relapses and opportunistic infections that can occur in case of immunosuppression. Often, maintenance immunosuppressants are utilized for 2–5 years and, at that stage, weaning off of immunotherapy with observation may be considered.
Clinical course and prognosis
The prognosis for patients with autoimmune dementia varies based on antibody and associated cancers. In a large case series of autoimmune dementia, a mean of 9 point improvement on the 38 point Kokmen Short Test of Mental Status was noted. 8 Improvements were most notable in learning and memory. The clinical improvements are generally followed by resolution of MRI, EEG, and CSF abnormalities. The type of antibody accompanying the dementia syndrome can help predict prognosis with antibodies to cell surface targets having a much better prognosis than those with antibodies to intracellular antigens.
Among patients with autoantibodies targeting cell-surface antigens, a study of 38 patients with anti-LGI1 encephalitis showed a 2-year fatality rate of 19%, but 80% of patients had substantial response to immunotherapy, with seizures responding quickly and cognitive function improving more gradually. Approximately one-third of patients experienced relapse. 79 A study evaluating 577 patients with anti-NMDAR encephalitis found that 30 patients died in the first year, but about half of patients had improvement with first line treatment or tumor removal in the first 4 weeks, and those that did not respond well to first-line treatment did better if they received a second-line therapy. 96 In a study of 38 patients with anti-NMDAR encephalitis, predictors of poor outcomes were abnormal findings on MRI, sensorimotor deficits, and treatment delayed by more than 4 weeks. 99 Scoring systems have been developed to assist in predicting clinical outcomes. The antibody prevalence in epilepsy and encephalopathy (APE) score has high sensitivity (99%) and specificity (93%) for predicting neural specific antibodies, while the Response-to-immunotherapy-in-epilepsy-and-Encephalopathy (RITE) score has high sensitivity (96%) and specificity of 86% for predicting favorable response to initial immunotherapy for patients with any autoimmune encephalitis. 100 The anti-NMDAR Encephalitis 1-Year Functional Status (NEOS) Score has a strong association for poor functional status at 1 year. 101
Conclusion
Clinicians should have an understanding of, and recognize the potential for, autoimmune causes of cognitive decline as these syndromes are potentially reversible, and early recognition and treatment can dramatically improve patient outcomes. Novel antibody biomarkers of autoimmune cognitive decline assist with diagnosis and prognosis. Current acute and treatment strategies are based mostly on retrospective studies and expert opinion. Future prospective randomized controlled trials are needed to help guide treatment decisions.