
Abstract
Drug-resistant epilepsy occurs in 25–30% of patients. Furthermore, treatment with a first-generation antiseizure drug (ASD) fails in 30–40% of individuals because of their intolerable adverse effects. Over the past three decades, 20 newer- (second- and third-)generation ASDs with unique mechanisms of action and pharmacokinetic profiles have been introduced into clinical practice. This advent has expanded the therapeutic armamentarium of epilepsy and broadens the choices of ASDs to match the individual patient’s characteristics. In recent years, research has been focused on defining the ASD of choice for different seizure types. In 2017, the International League Against Epilepsy published a new classification for seizure types and epilepsy syndrome. This classification has been of paramount importance to accurately classify the patient’s seizure type(s) and prescribe the ASD that is appropriate. A year later, the American Academy of Neurology published a new guideline for ASD selection in adult and pediatric patients with new-onset and treatment-resistant epilepsy. The guideline primarily relied on studies that compare the first-generation and second-generation ASDs, with limited data for the efficacy of third-generation drugs. While researchers have been called for investigating those drugs in future research, epilepsy specialists may wish to share their personal experiences to support the treatment guidelines. Given the rapid advances in the development of ASDs in recent years and the continuous updates in definitions, classifications, and treatment guidelines for seizure types and epilepsy syndromes, this review aims to present a complete overview of the current state of the literature about the efficacy and tolerability of ASDs and provide guidance to clinicians about selecting appropriate ASDs for initial treatment of epilepsy according to different seizure types and epilepsy syndromes based on the current literature and recent US and UK practical guidelines.
Introduction
Epilepsy is a chronic disorder of brain function characterized by recurrent seizures. 1 At any one time, about 1% of the population requires medication to treat epilepsy. 2 Research shows that in 30–40% of patients with new-onset epilepsy, treatment with an older- (first-)generation antiseizure drug (ASD) (e.g. carbamazepine and valproate) will fail because of adverse effects. 3 Moreover, 30% of patients will continue to experience seizures despite trying different ASDs, alone and in combinations, and these patients are described as having ‘drug-resistant epilepsy’. 4 These outcomes spurred a continuing search for newer ASDs with novel molecular targets that could provide optimal care for epilepsy patients.5,6 The past three decades have seen the licensing of about 20 newer- (second- and third-)generation ASDs with unique mechanisms of action and pharmacokinetics following a period of relative paucity. 7 This advent has expanded the epilepsy therapeutic armamentarium and allowed the drugs to match the individual patient’s characteristics. 7 The American Academy of Neurology (AAN) subcommittee reports in 2004 and 2018, however, observed that newer ASDs were not different in controlling seizures, but some have better tolerability, particularly fewer neurotoxic adverse effects.8–11
In 2017, the International League Against Epilepsy (ILAE) published a new classification for seizure types and epilepsy syndrome to improve our understanding of epilepsies and include missing seizure types.12–15 This classification replaced the previous versions published in 1981 16 and 1989, 17 and extended in 2010, 18 and has been of paramount importance to accurately classify the patient’s seizure type(s). In 2018, the AAN and the American Epilepsy Society (AES) subcommittee published updated guidelines for ASD selection in adult and pediatric patients with new-onset and treatment-resistant epilepsy.10,11 The subcommittee reports observed that data for the efficacy of some second-generation and most third-generation ASDs were limited and sometimes unavailable. One explanation is that physicians and researchers are still not confident trying the new drugs in monotherapy or giving a placebo in randomized controlled trials (RCTs). This practice limits the research on newer ASDs from advancing as it could be and warrants the future need for head-to-head comparative studies of these drugs (particularly brivaracetam, eslicarbazepine, lacosamide, and perampanel) for efficacy in focal and generalized epilepsy compared with the established drugs.
Given the rapid advances in the development of ASDs in recent years and the continuous updates in definitions, classifications, and treatment guidelines for seizure types and epilepsy syndromes, this article aims to present a complete overview of the current state of the literature about the efficacy and tolerability of currently available ASDs for the specific seizure type(s), according to the new ILAE classification of seizure types and epilepsy syndromes. To ensure the inclusions of robust data, only the best available evidence of efficacy from the randomized clinical trials and meta-analyses were considered. 19 The review also provides guidance for ASD selection in adult and pediatric patients with new-onset and drug-resistant epilepsy. The guidance is supplemented herein based on a comprehensive assessment of the current literature and recently published US and UK treatment guidelines.8,9,10,11,20–26 The drug mechanisms of action, adverse effects, and pharmacokinetics are also briefly reviewed here, as these represent the most relevant considerations when making an ASD selection. Data related to adverse effects and clinical pharmacology of the drugs were accessed at the US Food and Drug Administration (FDA) drug labeling database (FDALabel) 27 and recent experts review articles. It is hoped that this review becomes a succinct and practical guide to assist clinicians in everyday patient care decisions.
Epilepsy: definition and epidemiology
Epilepsy is a neurological disorder that is characterized by an enduring predisposition to generate epileptic seizures and the associated cognitive, psychological, and social consequences. 1 Epilepsy is the third most common neurologic disorder; almost 10% of people will experience a seizure during their lives. 2 The prevalence of epilepsy is 6.4 cases per 1000 persons, and the annual incidence is 67.8/100,000 person-years. 28
Classification of seizures and epilepsy
The ILAE classification framework, which was revised in 2017, is the key tool for the diagnosis of individuals presenting with seizures.12–15 According to that classification, epileptic seizures are classified into ‘focal’, ‘generalized’, and ‘unknown’ seizures, while epilepsy is classified into ‘focal’, ‘generalized’, ‘combined generalized and focal’, and ‘unknown’ epilepsy. Focal-onset seizures can be further described as focal aware (previously called simple partial), impaired awareness (complex partial), or focal to bilateral (secondarily generalized) tonic–clonic seizures. Generalized seizures are classified into generalized tonic–clonic (formerly idiopathic) seizures, motor (myoclonic and other motor) seizures, and nonmotor (absence) seizures. Etiologies of seizures and epilepsy syndromes have been reintroduced in the 2017 ILAE classification of seizure types and epilepsy syndromes, to include ‘genetic’, ‘structural’, ‘metabolic’, ‘infectious’, ‘immune’, and ‘unknown’.
Treatment of epilepsy
Epilepsy can persist for years and often for the patient’s lifetime. ASDs are the mainstay of treatment for seizures, although the choice of ASDs varies with different seizure types and epileptic syndromes. 29 The appropriately chosen ASD provides adequate seizure control in 60–70% of patients. 30 There is no general agreement on when treatment should start after a ‘first seizure’, but RCTs in adult and pediatric patients have shown that early treatment reduces the recurrence for at least 2 years from the first seizure. 31 ASDs are often administered orally for a long period of time to prevent seizure recurrence. The choice of medications depends on the type of seizures that the patient exhibits or on the patient’s syndromic classification. In designing a therapeutic strategy, the use of a single drug (monotherapy) is preferred because of fewer adverse effects. However, 30% of the patients will continue to have uncontrolled seizures, and multiple drugs are often used simultaneously. 30 Monotherapy trials of two ASDs that are appropriate first-line treatment for the patient’s seizure type usually be initiated before combinations are tried.
Patients who do not achieve seizure control following adequate trials with two or more appropriate drugs are considered drug resistant. 4 The ILAE, in 2010, has proposed the definition of drug-resistant (often used interchangeably with ‘medically refractory’, ‘intractable’, ‘pharmaco-resistant’, or ‘treatment-resistant’) epilepsy as ‘failure of adequate trials of two tolerated, appropriately chosen and used ASD schedules (whether as monotherapies or in combination) to achieve sustained seizure freedom’. 32 The mechanisms of drug resistance are likely to be variable and multifactorial according to the underlying cause. 33 Patients with drug-resistant epilepsy may require multiple drugs, resective surgery, neuromodulation, or dietary therapies. Treatment failure in such patients spurred a continuing search for new ASDs with novel molecular targets that could provide optimal care for patients with epilepsy.5,6 Over the past three decades, 20 newer-generation ASDs have been approved for clinical use, 34 and it was hoped that these drugs would have better efficacy in controlling seizures than that of the older-generation drugs, but as yet, there is little evidence.8,9
Classifications of ASDs
ASDs are classified as ‘older (first-)generation’ or ‘newer (second- and third-)generation’ agents. The ‘older generation’ ASDs introduced into clinical practice more than four decades ago include phenobarbital, phenytoin, primidone, ethosuximide, valproate, carbamazepine, clonazepam, and clobazam. The ‘second-generation’ ASDs, which have been approved for the treatment of epilepsy since the late 1980s, include, in chronological order, vigabatrin, oxcarbazepine, lamotrigine, gabapentin, felbamate, topiramate, tiagabine, levetiracetam, and zonisamide. The third-generation ASDs include pregabalin, fosphenytoin, lacosamide, rufinamide, eslicarbazepine, retigabine (also known as ezogabine), perampanel, brivaracetam, cannabidiol, stiripentol, cenobamate, and fenfluramine.8,34–36 The newer ASDs differ substantially in their mechanisms of action, spectra of activity, pharmacokinetics, and adverse-effect profiles. Current information on the other drugs in the pipeline can be found on the Epilepsy Foundation website. 37
Mechanisms of actions of ASDs
ASDs have many different pharmacologic profiles that are relevant when selecting and prescribing these agents in patients with epilepsy. Mechanism of action is a consideration in rationalizing ASD selection when switching or combining ASDs. To some degree, the cellular effects of ASDs are linked with the types of seizures against which they are most effective. An improved understanding of the molecular effects of existing ASDs, as well as the development of new drugs that act against novel targets, may allow for more “rational polytherapy” in the future. A propensity for seizure generation occurs when there is an imbalance favoring excitation of neurons over inhibition. ASD actions can generally be viewed in the context of inhibition of excitation or strengthening of inhibition, or both. Inhibition of excitation can be produced by effects on intrinsic excitability mechanisms in excitatory neurons (e.g. inhibition of sodium channel (carbamazepine, lacosamide, lamotrigine, phenytoin, and zonisamide) and calcium channel (ethosuximide, gabapentin, pregabalin, and valproate)) or on excitatory synaptic transmission (e.g. glutamate α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) and N-methyl-D-aspartate (NMDA) receptor antagonists (perampanel and felbamate) and synaptic vesicle protein 2A modulators (levetiracetam and brivaracetam)). Enhancement of inhibition is produced by the increased availability of GABA (e.g. valproate, tiagabine, and vigabatrin), increased activation of GABAA receptors; the mediators of inhibition in cortical areas relevant to seizures (e.g. benzodiazepines and phenobarbital), and modulation of voltage-gated potassium channel of the Kv7 type (e.g. retigabine). For some drugs, the precise mechanism of action is not known (e.g. valproate, zonisamide, and rufinamide), and some have multiple targets (e.g. topiramate and felbamate). 38 The ASD mechanisms of action are summarized in Table 1.
Mechanistic categorization of current antiseizure drugs based on foremost targets at therapeutic concentrations. 38

Fenfluramine’s mechanism of action for the treatment of seizures associated with Dravet syndrome is unknown.
Production of the drug retigabine (ezogabine) has been discontinued by the manufacturer, and it is no longer available.
Principles of ASD selection
Treatment should be considered in patients reporting more than one unprovoked seizure or after a single seizure if the risk of recurrence is high. 1 The initial ASD should be individualized on the basis of the epilepsy syndrome and seizure type and slowly titrated up to a target dosage. Other important selection criteria include patient characteristics, drug efficacy, adverse-effect profile, potential drug-drug interactions, and cost. 39 Combination therapy should be considered after the failure of two monotherapies. 40 However, Kwan and Brodie observed that few patients who have failed to achieve seizure freedom with two monotherapies achieved it with the trial of a subsequent drug. 30 The profile of activity against different seizure types varies among the ASDs. The therapeutic spectrum of these medications can be categorized into (1) broad-spectrum drugs used to treat a broad range of seizure types (both focal and generalized onset), including, in alphabetical order, brivaracetam, clobazam, felbamate, lamotrigine, levetiracetam, perampanel, rufinamide, topiramate, valproate, and zonisamide. However, lamotrigine may worsen or precipitate myoclonic seizures. (2) Narrow-spectrum drugs used primarily for focal-onset seizures, including focal evolving to bilateral tonic–clonic seizures including carbamazepine, cenobamate, eslicarbazepine, gabapentin, lacosamide, oxcarbazepine, phenobarbital, phenytoin, pregabalin, primidone, stiripentol, tiagabine, and vigabatrin; and (3) a narrow-spectrum drug used primarily for absence seizures which is ethosuximide. Carbamazepine, phenobarbital, phenytoin, and primidone have evidence of efficacy for generalized-onset tonic–clonic seizures but may also worsen certain generalized seizure types. Eslicarbazepine, gabapentin, oxcarbazepine, tiagabine, and vigabatrin also have the potential to worsen certain generalized seizure types.
For many years, carbamazepine was considered the first-line treatment for focal-onset seizures, and the standard treatment for focal epilepsy in clinical trials, whereas valproate, with its broad-spectrum efficacy, was, and still, recommended first-line treatment for generalized-onset and unclassified seizures.8,9,41–43 These recommendations were based largely on the results of RCTs comparing carbamazepine and/or valproate with other older drugs.44–51 A large meta-analysis by Marson and colleagues 52 emphasizes that carbamazepine and valproate are broadly similar in terms of clinical outcomes of efficacy, tolerability, and drug retention after randomization. A large multicenter, double-blind RCT by Mattson and colleagues 48 in 206 patients with impaired-awareness focal seizures and 274 patients with focal to bilateral tonic–clonic seizures showed no difference between carbamazepine and valproate for controlling focal to bilateral seizures, but carbamazepine was superior for controlling impaired-awareness focal seizures and for the outcomes of time to first seizure and time to 12-month remission. However, the literature has shown that 30–40% of people treated with an older ASD as monotherapy (including carbamazepine and valproate) experience adverse effects that contribute to treatment failure. 53
Ever since, there has been a great deal of research into formulating better ASDs, primarily spurred by the fact that the older-generation ASDs do not provide optimal safety, tolerability, or seizure control for many patients with epilepsy. The past two decades have seen the licensing and introduction of many “newer-generation” ASDs following a period of relative inactivity. 7 This advent has expanded the epilepsy therapeutic armamentarium and warranted the future need for more evidence and guidelines for prescribing the newer-generation drugs in terms of efficacy, tolerability, and safety profiles. The AAN subcommittee reports in 2004 and 2018, however, observed that the newer-generation ASDs were “not different” in controlling seizures, but better tolerated than the older drugs.8–11 Drug retention (or time to treatment failure) is an increasingly popular pragmatic measure of the effectiveness of epilepsy treatment, as it is dependent on both efficacy and tolerability. 54 The previous RCTs in patients with new-onset focal epilepsy have shown that lamotrigine,41,55–60 vigabatrin,61–63 topiramate, 64 and gabapentin,41,59,65 were better than carbamazepine for time to treatment failure outcomes. Other trials have found that lamotrigine, 41 topiramate,41,64 tiagabine, 66 levetiracetam,67–69 oxcarbazepine,41,70 zonisamide,71,72 and lacosamide 73 have equivalent efficacy to that of carbamazepine and/or valproate.
Furthermore, a number of RCTs showed that some newer medications could be more effective than others. For time to treatment failure, the SANAD study (2007), a pragmatic randomized clinical trial, has shown that lamotrigine is significantly better than carbamazepine, gabapentin, and topiramate for the treatment of new-onset focal seizures in adults. 41 The SANAD II (2021) has shown that lamotrigine was superior to levetiracetam and zonisamide for time to 12-month remission and should remain the first-line treatment in patients with new-onset focal epilepsy and should be the standard treatment in future trials as an alternative to carbamazepine. 74 Kwan and Brodie also found that pregabalin has similar tolerability but seems to have inferior efficacy to lamotrigine for the treatment of new-onset focal epilepsy. 75 In patients with new-onset generalized and unclassified epilepsy, the SANAD (2007) has shown that valproate is better tolerated than topiramate and more effective than lamotrigine, 42 whereas the SANAD II (2021) has suggested that levetiracetam is inferior to valproate for time to 12-month remission. 43 The two studies confirm valproate as the most effective drug for the treatment of generalized or unclassified epilepsy.
The first AAN/AES evidence-based practice guidelines for prescribing ASDs in patients with new-onset and treatment-resistant epilepsy were published in 2004.8,9 The guidelines included seven second-generation ASDs (gabapentin, oxcarbazepine, lamotrigine, topiramate, tiagabine, levetiracetam, and zonisamide). These guidelines were updated in 201520 and then in 201810,11 with clobazam, vigabatrin, the previous seven second-generation ASDs (plus felbamate), and six third-generation ASDs (eslicarbazepine, lacosamide, perampanel, pregabalin, retigabine, and rufinamide). Please refer to the complete guidelines at AAN.com/guidelines (Practice Guideline Update: Efficacy and Tolerability of the New Antiseizure drugs I: Treatment of New-onset Epilepsy 10 & II: Treatment-resistant Epilepsy). 11 A possible limitation of those guidelines was that the recommendations primarily relied on studies that compare the first- and second-generation ASDs. Evidence for the efficacy of third-generation drugs was found insufficient.
Table 2 in this article presents the efficacy of ASDs against common seizure types and epilepsy syndrome. Data in Table 2 are based largely on the results of RCTs comparing the newer versus older drugs including the SANAD studies,41,42,43,74 and others.57,59–62,64,67,69,71,73,75–88 Table 3 and the remainder sections of this articles present guidance for ASD selection for different seizure types and epilepsy syndromes according to the 2017 ILAE classification.12–15 The guidance is based on the current state of the literature on the efficacy and tolerability of ASDs and the recently published practical guidelines. The most popular treatment guidelines applied herein are the guidelines published by the AAN/AES in 2004, 2015, and 2018,8–11,20 the ILAE in 2006 and 2013,21,22 the UK National Institute for Health and Care Excellence in 2012,23,24 and the Scottish Intercollegiate Guidelines Network in 2018.25,26
Efficacy of antiseizure drugs against common seizure types and epilepsy syndromes.

ASD: antiseizure drug; GTCS: generalized tonic clonic seizure.
+ Effective; ?+ possibly effective; – worsen seizure. Note that although there is evidence to support the use of these drugs for these seizure types, the drugs may not be indicated for this use by the US Food and Drug Administration.
Especially when associated with tuberous sclerosis complex.
None of these is very effective in Dravet’s syndrome.
Can cause aplastic anemia and severe hepatitis, used only for patients who respond poorly to other agents.
Possibly effective but may worsen myoclonic seizures in some cases.
Has been discontinued by the manufacturer, and it is no longer available.
In combination with clobazam and valproate.
Preferred in patients with concomitant GTCS or myoclonic seizures (myoclonic absence seizure).
Recommendations for add-on and monotherapy in adults and pediatric patients >four years of age according to seizure typea and based on assessment of current literature and published guidelines.

Other selection criteria include patient characteristics, adverse-effect profile, potential drug–drug interaction, availability, and cost (see text).
Lamotrigine was superior to levetiracetam and zonisamide for time to 12-month remission and should remain a first-line treatment for new-onset focal epilepsy.
Evidence is insufficient to consider gabapentin, oxcarbazepine, or topiramate instead of lamotrigine in patients with new-onset focal epilepsy. Gabapentin may be considered first-line monotherapy in patients aged ⩾60 years.
Phenobarbital is often regarded as second-line treatment in adults because of sedation and behavioral problems.
Received FDA approval for extrapolation of efficacy as monotherapy across individuals with focal seizures. 11
Evidence is insufficient to consider the use of clobazam, felbamate, tiagabine, vigabatrin, or third-generation antiseizure drugs as monotherapies in treating new-onset focal epilepsy.
Valproate should be avoided, if possible, in women of childbearing potential.
Evidence is insufficient to support efficacy of third-generation antiseizure drugs in unclassified generalized tonic–clonic seizures.
Drugs effective for focal-onset seizures
Focal-onset seizures account for 60% of all epilepsies. The RCTs and meta-analyses have demonstrated comparable efficacy of the different ASDs in controlling this type of seizure.10,22,41,89 The drug of the first choice for focal and focal to bilateral tonic–clonic seizures is lamotrigine.10,41,55,60,74,90 Phenytoin is the drug of choice for the urgent treatment of new-onset or recurrent focal epilepsy.10,90–92 The other most widely used first-line drugs for focal seizures include levetiracetam and zonisamide.10,67,69,71,72,74,89 However, findings from the SANAD II have suggested that levetiracetam and zonisamide are inferior to lamotrigine for time to 12-month remission. 74 Carbamazepine may now be considered a second-line treatment for new-onset focal epilepsy owing to its unfavorable efficacy-to-tolerability profile.10,41 Oxcarbazepine,70,83,86,93 topiramate,42,64,87,94,95 and valproate42,91 can be used, but they may not be as effective as lamotrigine and carbamazepine. 10 Phenobarbital (and its derivative primidone) is often regarded as a second-line treatment in adults because of sedation and behavioral problems.10,46,47 However, it is a primary drug for neonatal seizures.
Given the unique mechanistic and pharmacokinetic profiles of the third-generation ASDs, a recent FDA strategy allowed extrapolation of these drugs as add-on or monotherapy in persons ⩾ four years old.10,96 The FDA approved eslicarbazepine and lacosamide (oral only for pediatric use) as add-on or monotherapy and brivaracetam and perampanel as monotherapy. 10 Accordingly, brivaracetam,84,97 eslicarbazepine,82,88,89,98 lacosamide,73,89,99–101 and perampanel 77 can also be used in focal epilepsy as second-line monotherapy. 10 However, future trials should consider these medications in head–head comparison with the standard drug, lamotrigine. Vigabatrin appears to be less efficacious, although better tolerated, than immediate-release carbamazepine61–63,81 and may not be offered; furthermore, toxicity profile precludes vigabatrin use as first-line therapy. 10 The drugs used as add-on (adjunctive) therapy in focal seizures include gabapentin,41,59,102 pregabalin,75,78,102 felbamate, 103 rufinamide,79,104 cenobamate, 105 retigabine,80,85 and tiagabine. 66 However, the AAN/AES guidelines state that gabapentin is possibly as effective and better tolerated than immediate-release carbamazepine and may be considered, with lamotrigine, first-line monotherapy in patients aged ⩾60 years with new-onset focal epilepsy.10,59 The FDA determined that the efficacy of ASDs for focal-onset seizures in adults can be extrapolated downward to children four years of age and above.10,96
For drug-resistant focal epilepsy in adults, eslicarbazepine can be used as monotherapy 106 while the immediate-release pregabalin, perampanel, lacosamide, eslicarbazepine, extended-release topiramate, rufinamide, clobazam, felbamate, and vigabatrin should be considered as add-on therapy. 11 However, vigabatrin, felbamate, and rufinamide are not first-line treatments because of the retinopathy risk with vigabatrin,62,107,108 the modest benefit with rufinamide,79,104 and the hepatotoxicity and hematotoxicity risk with felbamate. 103 In pediatric patients, levetiracetam, oxcarbazepine, and zonisamide should be considered as add-on therapy. 11
Drugs effective for generalized tonic–clonic seizures
There has been a limited number of ASDs that can be used as first-line treatment for generalized tonic–clonic seizure (GTCS). Valproate remains the first-line drug for many patients with generalized and unclassified epilepsies.10,22,42,43 while phenobarbital (or primidone) is a primary drug in infants (for neonatal seizures) and an alternative in adults.46,47 However, valproate should not be prescribed for women of childbearing potential because of its dose-dependent teratogenic profile; 109 unless other ASDs cannot control the seizures, in which case, the dose should be kept as low as possible. Indeed, some patients with idiopathic generalized epilepsy can control their seizures only with valproate. 43 The other most widely used monotherapies for GTCS include lamotrigine,42,110 levetiracetam, 43 brivaracetam,97,111 topiramate,42,94,95 clobazam, and zonisamide. 10 Evidence is insufficient to compare the efficacy of lamotrigine and topiramate with that of valproate in GTCS. 10 However, the SANAD study found that valproate is better tolerated than topiramate and more efficacious than lamotrigine for many patients with generalized and unclassified epilepsies. 42 Moreover, the SANAD II study has suggested that levetiracetam is inferior to valproate for time to 12-month remission. 43
Phenytoin and carbamazepine are effective but may worsen certain seizure types in generalized epilepsies, including absence epilepsy, juvenile myoclonic epilepsy, and Dravet’s syndrome.91,92,112 Vigabatrin, tiagabine, oxcarbazepine, and possibly gabapentin are other drugs that may worsen these seizure types. 113 Seizures of most patients with generalized epilepsy are easily controlled with appropriate medication. Immediate-release and extended-release lamotrigine use, however, should be considered add-on therapy to decrease seizure frequency in drug-resistant GTCS in adults. 11 Levetiracetam and brivaracetam 111 should also be effective in both drug-resistant GTCS and drug-resistant juvenile myoclonic seizures. 11 Other drugs used as add-on therapy in primary GTCS include perampanel 77 and lacosamide. 114 The combination of lamotrigine and valproate is believed to be particularly efficacious. However, valproate causes a two-fold increase in the half-life of lamotrigine and can increase its blood levels correspondingly, leading to adverse effects such as skin rash. In patients receiving valproate, the initial dose of lamotrigine must be reduced. 113
Drugs effective for focal seizures and certain generalized-onset seizure types
A variety of drugs are primarily used to treat focal seizures; these drugs have also been effective in certain generalized-onset seizure types. These drugs are lamotrigine,42,74,76 levetiracetam,43,69,74 zonisamide,72,74 brivaracetam,97,111 perampanel,10,77 phenobarbital,46,47 primidone, and felbamate.103,113
Drugs effective for myoclonic seizures
Valproate is widely used for myoclonic seizures, such as in juvenile myoclonic epilepsy.42,115 Other drugs effective in treating this seizure type are levetiracetam, brivaracetam, zonisamide, topiramate, clonazepam, and piracetam.111,115 There is also increasing evidence for the efficacy of perampanel in progressive myoclonic epilepsies. 116 Myoclonic seizures can be precipitated or aggravated by some drugs, including carbamazepine, phenytoin, oxcarbazepine, eslicarbazepine, gabapentin, pregabalin, tiagabine, and vigabatrin. 112 Substituting those drugs can result in the improvement or resolution of myoclonus.
Drugs effective for absence seizures
Ethosuximide is the first-line drug. It is often used in uncomplicated absence seizures if patients can tolerate its adverse gastrointestinal effects.10,76,117 Despite the long half-life (~ 40 h), ethosuximide is generally administered in two or even three divided doses to minimize the adverse gastrointestinal effects. Valproate is preferred in patients with concomitant GTCS or myoclonic seizures (myoclonic absence seizure). Clonazepam is effective as an alternative drug but has the disadvantages of causing sedation and tolerance. Lamotrigine, levetiracetam, and zonisamide are also used in absence seizures but not as effective as ethosuximide or valproate. Unless there are compelling adverse effect–related concerns, ethosuximide or valproate use should be considered before lamotrigine in treating absence seizures in childhood absence epilepsy.76,117 Lamotrigine should be considered in women of childbearing age because of its better tolerability and fewer fetal risks compared with valproate.
Drugs effective for other epilepsy syndromes
In combination with lamotrigine and a benzodiazepine (such as clobazam), valproate is the most widely used treatment for atonic seizures (for example, drop attacks in the Lennox–Gastaut syndrome). Other drugs used for the atonic seizures in Lennox–Gastaut syndrome include topiramate, felbamate, and rufinamide. 113 Because felbamate can cause aplastic anemia and severe hepatitis, it is used as an add-on therapy in patients who respond poorly to other medications. Felbamate decreases the clearance of valproate (and phenytoin) and increases their blood levels; dose reductions of these drugs may be necessary when felbamate is initiated.
For infantile spasms (west’s syndrome), valproate, topiramate, zonisamide, or a benzodiazepine (such as clonazepam or nitrazepam) are effective. 113 Vigabatrin and everolimus are used if associated with tuberous sclerosis complex (a rare genetic disease that causes noncancerous (benign) tumors to grow in the brain and other parts of the body like the eyes, heart, kidneys, lungs, and skin). 118 However, infantile spasms are primarily treated with intramuscular adrenocorticotropic hormone (ACTH) or oral corticosteroids, such as prednisone or hydrocortisone (unknown mechanism). For Dravet’s syndrome (the severe myoclonic epilepsy of infancy), valproate, topiramate, and clobazam can be used, although none of these is very effective.113,119 Stiripentol, a modulator of GABAA receptors, is often used in conjunction with clobazam or valproate. 119 Cannabidiol was approved in 2018 to treat Dravet’s syndromes in addition to Lennox–Gastaut syndrome and infantile spasms associated with tuberous sclerosis complex. 120 Fenfluramine is another new drug approved in 2020 for Dravet’s syndrome. 121 The drug is available only through a restricted drug distribution program, under a risk evaluation and mitigation strategy (REMS) because of the risk of valvular heart disease and pulmonary arterial hypertension.
Adverse effects of ASDs
The first-generation ASDs have acute dose-related effects, primarily neurological effects such as sedation, dizziness, unsteadiness, blurred vision, diplopia, and tremor, in addition to neurocognitive and psychiatric symptoms.39,122,123 These effects are found across the different ASDs68,123 and often mild and reversible. However, some drugs are better tolerated than others; for example, lamotrigine and levetiracetam are better tolerated than carbamazepine in elderly patients. 124 Psychiatric adverse effects include depression, anxiety, irritability, impaired concentration, mood changes, hyperactivity, and, in rare cases, psychosis. Although the newer ASDs are touted as better tolerated than older drugs, 8 psychiatric adverse effects are common with levetiracetam, topiramate, zonisamide, vigabatrin, and perampanel. Lamotrigine, carbamazepine, valproate, gabapentin, and pregabalin, in contrast, have mood-stabilizing effects in some patients and less frequently cause behavioral or psychiatric effects. 125 The adverse effects of older- and newer-generation ASDs are listed in Tables 4 and 5, respectively.
Common and serious adverse effects of older antiseizure drugs.

ASD: antiseizure drug.
Common and serious adverse effects of commonly used newer antiseizure drugs.
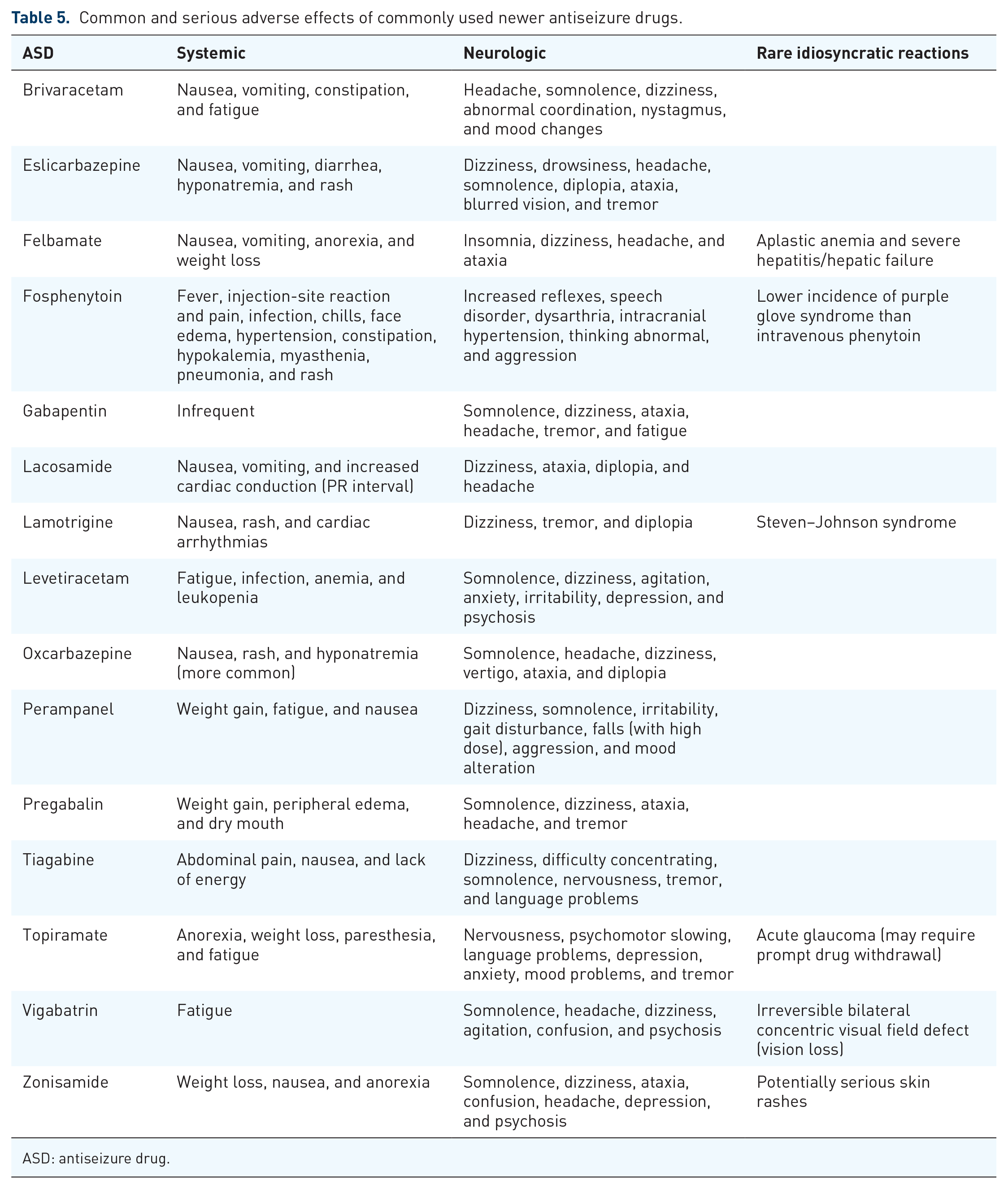
ASD: antiseizure drug.
Most women with epilepsy who become pregnant require continued ASD therapy for seizure control. The established ASDs have all been shown to increase the likelihood of fetal malformations. If possible, valproate, carbamazepine, phenytoin, phenobarbital, and topiramate should be avoided in women of childbearing potentials. 109 Recent analysis from several large-scale international pregnancy registers suggests that in utero exposure to valproate during the first trimester is associated with a three-fold increased risk of congenital malformations, commonly neural tube defects (spina bifida) and cardiovascular, orofacial, and digital abnormalities. 126 The use of valproate during the first trimester is also associated with cognitive impairments. 127 Official guidelines issued by the Medicines and Healthcare Products Regulatory Agency (MHRA) warn against the use of valproate in female patients unless all other appropriate treatments have failed. 128 Carbamazepine may cause neural tube defects and craniofacial anomalies. Fetal hydantoin syndrome is related to the use of phenytoin. Treatment with topiramate during the first trimester of pregnancy is associated with a 10-fold increase in oral clefts risk. Phenobarbital can cause congenital malformations, most often cardiac defects. No ASD is known to be entirely safe for the developing fetus.129,130 However, lamotrigine, levetiracetam, and oxcarbazepine have the lowest risks of major congenital malformations and may be safer, particularly for cognition compared with valproate.109,113,131 Combining low-dose valproate with lamotrigine or levetiracetam in patients with idiopathic generalized epilepsy has less risk of teratogenicity than high-dose valproate monotherapy. Overdose toxicity with benzodiazepines and barbiturates may cause respiratory depression. Management is primarily supportive (airway management and mechanical ventilation) and flumazenil in benzodiazepine overdose.
Subacute idiosyncratic adverse effects, usually occur weeks or months after starting ASDs, are more common with some drugs and are mostly immune-mediated. The most common effect is an erythematous maculopapular rash, which occurs in 5–10% of patients commenced on carbamazepine, but can also occur with phenytoin, oxcarbazepine, phenobarbital, and lamotrigine. 39 Most ASD-induced rashes are self-limiting if the ASD is stopped but some can be severe, such as life-threatening Steven–Johnson syndrome and toxic epidermal necrolysis, which are strongly associated with the HLA-B*1502 allele. Asians, who have a 10-fold increased risk of the drug-induced Stevens–Johnson syndrome compared to other ethnic groups, should be tested before carbamazepine is prescribed.132,133 The use of zonisamide is also associated with severe skin reactions. Valproate causes hepatotoxicity in children less than 2 years of age. Aplastic anemia and acute hepatic failure have limited the use of felbamate to severe and drug-resistant epilepsy. Withdrawal from ASDs should be accomplished gradually (over a 1- to 3-month period or longer) to avoid the occurrence of severe seizures or status epilepticus. Physical dependence occurs with barbiturates and benzodiazepines, and there is a well-recognized risk of rebound seizures with abrupt withdrawal. However, withdrawal is less likely to be a problem with ethosuximide. Withdrawal is believed to be successful in patients with generalized epilepsies who exhibit a single seizure type, whereas the longer duration of epilepsy, an abnormal neurologic examination, an abnormal EEG, and certain epilepsy syndromes, including juvenile myoclonic epilepsy, are associated with increased risk of recurrence. 113 Clinical studies suggest a possible association of lamotrigine, levetiracetam, and topiramate with suicidality. In 2008, the FDA issued an alert that ASDs, as a class, may be associated with an increased risk of suicidality based on an analysis of data from placebo-controlled add-on clinical trials of ASDs in patients with drug-resistant epilepsy, although this is still highly controversial.134,135
Patients treated with ASDs have a two-fold to three-fold increased risk of bone fractures, which likely reflects a combined effect of the ASDs, both enzyme inducing and nonenzyme inducing, on bone health and fragility and balance rather than a direct effect of seizures.39,136,137 In addition, increased body weight and fat are common in patients using valproate, carbamazepine, gabapentin, pregabalin, vigabatrin, and perampanel and can lead to serious health consequences associated with obesity and increased cardiovascular disease risk. 138 In March 2021, the FDA issued an alert that lamotrigine may be associated with an increased risk of cardiac arrhythmias in people with underlying cardiac disease. 139 This warning stems from in vitro data by Harmer and colleagues 140 indicating that lamotrigine can weakly inhibit cardiac sodium channels, showing class IB antiarrhythmic activity. However, there is not an apparent arrhythmia risk of lamotrigine therapy in healthy individuals. 141
Pharmacokinetics and drug–drug interactions of ASDs
ASDs are commonly used for long periods of time and consideration of their pharmacokinetic properties is essential for avoiding toxicity and drug interactions.142,143 An ideal ASD should demonstrate complete absorption, linear kinetics, a long elimination half-life, and allowing once or twice-daily dosing. Other favorable properties include low protein binding, lack of active metabolites, and clearance by kidneys. In general, the ASD should be started at a low dose, with increments over several weeks to establish an effective and tolerable regimen. Some medications do not require titration, such as gabapentin and levetiracetam. Clinicians should be aware of certain factors that affect dosing. These factors include nonlinear relationships between dose and drug exposure and the influence of hepatic or renal impairment on clearance. For optimum therapy, therapeutic drug concentration should be monitored in individual patients for some drugs.144,145 Examples include carbamazepine, phenytoin, and valproate. Drug levels can be helpful (1) to guide dose adjustments, (2) when breakthrough seizures occur, (3) when an interacting medication is added, (4) during pregnancy, (5) to assess compliance, and (6) to determine whether adverse effects are related to drug levels.
Generally, ASDs are well absorbed after oral administration, have good bioavailability, and readily cross the blood–brain barrier. Many ASDs are medium- to long-acting drugs (have half-lives of >12 h) and can be administered twice or three times a day because plasma clearance is relatively slow. Phenobarbital, phenytoin, zonisamide, eslicarbazepine, and perampanel can often be administered once daily. Extended-release preparations of drugs that have short half-lives (e.g. carbamazepine, valproate, levetiracetam, and lamotrigine) may decrease the incidence of adverse effects and allow once-daily dosing. 146 Most ASDs are metabolized by hepatic enzymes. Carbamazepine, oxcarbazepine, eslicarbazepine, phenobarbital, phenytoin, and primidone are inducers of hepatic cytochrome P450 enzyme and may decrease the effects of other drugs administered concomitantly (e.g. valproate). 147 Valproate and clobazam are inhibitors of hepatic enzymes and most likely to elevate the plasma concentration of other drugs administered concomitantly (e.g. carbamazepine, ethosuximide, phenytoin, phenobarbital, and lamotrigine). Drug–drug interactions with ASDs are complex since the drugs are often used in combination. These interactions may lead to either inadequate seizure control or drug toxicity. Of the newer drugs, levetiracetam, gabapentin, pregabalin, and vigabatrin are unique. These drugs are eliminated unchanged by the kidney and have no drug–drug interactions. Lamotrigine, perampanel, tiagabine, topiramate, and zonisamide undergo hepatic drug metabolism and have potential drug interactions. Oxcarbazepine, felbamate, and topiramate selectively induce the hepatic metabolism of the oral contraceptive pill, failing birth control. 148 Clinically relevant pharmacokinetic profiles of ASDs are summarized in Table 6.
Pharmacokinetic profiles of antiseizure drugs.

ASD: antiseizure drug; NE, not established.
++++ Extensive hepatic metabolism and active metabolite(s).
+++ Extensive hepatic metabolism but no active metabolite(s).
++ Hepatic metabolism (with or without active metabolites) and renal excretion.
+ Variable (or moderate) hepatic metabolism (with or without active metabolites).
– Renal excretion (unchanged). No hepatic metabolism.
ng/mL.
Saturable drug metabolism.
Conclusion
This article reviewed the latest evidence for ASD efficacy and tolerability. There have been rapid advances in the development of ASDs in recent years, and hence 20 second- and third-generation drugs with different pharmacological profiles have been introduced. The broader choice of ASD’s now available allows the drugs to match the individual patient’s characteristics. Furthermore, some second-generation drugs have shown advantages in tolerability and safety, particularly in the treatment of older patients and women of childbearing potential. Disappointingly, none of these medications appear to be more efficacious than first-generation drugs, highlighting the need for novel strategies in epilepsy drug development. The recommendations on ASD selection in new-onset and treatment-resistant epilepsy in this review were supplemented based on a comprehensive assessment of the current literature and published US and UK treatment guidelines. The recent treatment guidelines, however, emphasized moderate-certainty evidence for the second-generation drugs and limited information for the third-generation drugs.
The SANAD trials and few others offer a methodology to address some questions about choosing a more efficacious drug treatment for epilepsy. The studies identified lamotrigine, among other newer drugs, as a cost-effective alternative to carbamazepine for the treatment of focal epilepsy and confirmed valproate as the most effective drug for treating generalized or unclassified epilepsy, although concerns remain regarding teratogenicity. Importantly, the recent practice guidelines recommended the use of the third-generation drugs eslicarbazepine, lacosamide brivaracetam, and perampanel as monotherapy, and this warrants the urgent need for head-to-head studies of these drugs compared with the standard drugs lamotrigine and valproate for efficacy in focal and generalized epilepsy, respectively. It is, therefore, anticipated that Table 3 in this review (recommendations for ASD selection) would require updating as future studies yield more detailed results. It is hoped that this review remains a succinct and practical guide to assist clinicians in patient care decisions. Epilepsy experts may also wish to share their personal experience in supporting the practical guidelines for the proper ASD selections through reviews, short communications, and commentaries.
Supplemental Material
sj-docx-1-tan-10.1177_17562864211037430 – Supplemental material for Efficacy and tolerability of antiseizure drugs
Supplemental material, sj-docx-1-tan-10.1177_17562864211037430 for Efficacy and tolerability of antiseizure drugs by Tahir Hakami in Therapeutic Advances in Neurological Disorders
Footnotes
Author contributions
The author has made substantial contributions to the conception and design of the work, and acquisition, analysis, and interpretation of data for the work; drafting the work and revising it critically for important intellectual content; final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of interest statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.