
Abstract
The past decades have yielded major therapeutic advances in many autoimmune conditions – such as multiple sclerosis (MS) – and thus ushered in a new era of more targeted and increasingly potent immunotherapies. Yet this growing arsenal of therapeutic immune interventions has also rendered therapy much more challenging for the attending physician, especially when treating patients with more than one autoimmune condition. Importantly, some therapeutic strategies are either approved for several autoimmune disorders or may be repurposed for other conditions, therefore opening new curative possibilities in related fields. In this article, we especially focus on frequent and therapeutically relevant concomitant autoimmune conditions faced by neurologists when treating patients with MS, namely psoriasis, rheumatoid arthritis and inflammatory bowel diseases. We provide an overview of the available disease-modifying therapies, highlight possible contraindications, show pathophysiological overlaps and finally present which therapeutics can be utilized as a combinatory treatment, in order to ‘kill two birds with one stone’.
Introduction
In the past decades, treatment of autoimmune conditions such as multiple sclerosis (MS) has experienced significant changes, resulting from major advances in disease-modifying therapies (DMTs). However, considering the growing armamentarium of immunomodulatory drugs, selecting the right therapeutic agent for an individual patient has become more challenging. Genome-wide association studies have identified hundreds of shared susceptibility loci for autoimmune diseases, 1 and it is not uncommon for patients to have more than one autoimmune disorder. While some of these patients may present therapeutic challenges, it also creates the opportunity to utilize elegantly specific immunosuppressants targeting two autoimmune conditions simultaneously and consequently ‘kill two birds with one stone’. MS is associated with several other auto-inflammatory conditions, which share not only certain susceptibility genes, but also general pathophysiological principles. For example, psoriasis (PsO) – like MS – is a largely T-cell driven disease with the interleukin (IL)23/T helper (Th)17-axis being critically involved in the pathology of both conditions.2,3 These immunological interfaces can be used to repurpose DMTs that were initially developed for other inflammatory disorders and tailor crossover therapies for the individual patient, as shown for the anti-IL17 antibody secukinumab 4 or sphingosine-1-phosphate receptor (S1PR) modulators such as ozanimod. 5 In contrast, other DMTs may exacerbate pre-existing autoimmune diseases or even trigger their onset. For instance, tumor necrosis factor alpha (TNFα) blockers are known potentially to induce or worsen demyelinating conditions.6–8 Thus, it is important to shed a light on the ever-growing jungle of immunosuppressants and the possibilities to repurpose these substances for the treatment of other inflammatory comorbidities, such as MS.
Of note, systemic cortisone is the common therapeutic denominator for almost all inflammatory conditions, yet due to its long-term unwanted side effects, cortisone is generally used to induce a state of remission quickly and not as a continuously administered DMT. In fact, many DMTs are used to taper cortisone intake to low levels. Thus, we excluded cortisone from this review and instead exclusively focused on long-term DMTs. Furthermore, we specifically focus on the most common concomitant autoimmune diseases that provide specific challenges for clinicians treating patients with MS, namely PsO, rheumatoid arthritis (RA), and inflammatory bowel diseases [IBDs: ulcerative colitis (UC) and Crohn’s disease (CD)]. Thus, the aim of this review is to offer an overview of the available therapeutic tools across those diseases and to propose pragmatic treatment approaches for the selection of potential disease-overlapping substances, when facing patients with MS and coexisting autoimmune disorders.
Common immunosuppressants
Azathioprine (AZA)
Azathioprine (AZA) and its active metabolite 6-mercaptopurine (6-MP) are antimetabolites, which block the de novo synthesis of nucleobases and thus affect rapidly dividing lymphocytes. AZA is approved by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) for many inflammatory conditions, including RA 9 (Table 1). In IBD, AZA can be utilized in combination with other therapeutics (like TNFα blockers) to induce and maintain remission; however, its effect commences with a delay of several months. While AZA is no longer routinely used in MS (despite being approved in some countries, including Germany), it is an established therapeutic option in other demyelinating conditions, such as low-active neuromyelitis optica spectrum disorder (NMOSD).10,11 In clinical studies, AZA has proved non-inferiority 12 or even superiority 13 to interferon-beta (IFNβ), although the investigated cohorts were relatively small and the number of adverse events (e.g. nausea, vomiting, and lymphopenia) was generally higher, while AZA additionally increases the long-term risk of malignancies. 14 Thus, despite its very limited use in MS now, it is a reasonable option in patients with, among other things, comorbid IBD.
FDA approval status of presented disease-modifying therapies in regards to specific autoimmune disorders.

, FDA approved; (+), used off-label; −, not generally used.
5-ASA, 5-aminosalicylic acid; ALEM, alemtuzumab; Anti-CD20, CD20 antibodies; Anti-TNFα, TNFα antibodies; AZA, azathioprine; BD, Behcet’s disease; CORT, cortisone; CYA/TAC, cyclosporine/tacrolimus; DMF, dimethylfumarate; EGPA, eosinophilic granulomatosis with polyangiitis; FDA, US Food and Drug Administration; GCA, giant cell arteritis; GPA, granulomatosis with polyangiitis; HCQ, hydroxchloroquine; IBD, inflammatory bowel disease; IFN, interferon; JAK, Janus kinase inhibitor; MMF, mycophenolate mofetil; MPA, microscopic polyangiitis; MS, multiple sclerosis; MTX, methotrexate; NATA, natalizumab; PAN, polyarteritis nodosa; PsO, psoriasis; PSS, primary systemic sclerosis; RA, rheumatoid arthritis; S1PR, sphingosin-1-phosphate receptor modulator; SARC, sarcoidosis; SEC, secukinumab; SLE, systemic lupus erythematosus; SpA, spondylo arthritis; SS, Sjögren’s syndrome; TA, Takayasu arteritis; TER/LEF, teriflunomide/leflunomide; TOC, tocilizumab; USTE, ustekinumab.
Cyclosporine A and tacrolimus
Cyclosporine A (CYA) and tacrolimus (TAC) are inhibitors of calcineurin, an enzyme involved in the transcription of IL-2 and thus T-cell activation and proliferation. Both substances have a broad operational field, including RA, 15 IBD16,17 and PsO15,18 (Table 1). Especially in diseases with cutaneous manifestations, CYA and TAC can also be applied topically. CYA has been shown to reduce the relapse rate in relapsing–remitting multiple sclerosis (RRMS),19,20 and there are also promising case reports and small trials for TAC in MS. 21 However, with more potent and targeted DMTs in hand, both substances are not first line treatment options for IBD/RA/PsO patients with comorbid MS.
(Hydroxy-)chloroquine (HCQ)
The anti-malarial agent hydroxychloroquine (HCQ) blocks lysosomal enzymes by raising the intra-lysosomal pH, thus hampering the presentation of antigens to CD4+ T cells via major histocompatibility complex (MHC) II. HCQ is in clinical use for several autoimmune conditions including systemic lupus erythematosus (SLE) and RA (Table 1), yet has proved to be less efficient than other disease-modifying antirheumatic drugs (DMARDs). 22 So far, there is only experimental evidence [in experimental autoimmune encephalomyelitis (EAE) and cuprizone models] for the efficacy of HCQ in neuroinflammatory conditions.23–25 However, there are two ongoing clinical trials for the application of HCQ in progressive MS (NCT02913157 and NCT03109288); publication of the final results is still pending. Thus, data are currently too limited to recommend HCQ as a treatment option in patients with MS and coexisting autoimmune disorders.
Methotrexate (MTX)
Methotrexate (MTX) is an antimetabolite and competitive inhibitor of folate-dependent enzymes, such as dihydrofolate reductase (DHFR), thereby blocking purine and pyrimidine base biosynthesis necessary for fast (T-) cell proliferation. MTX is generally used for the treatment of RA, IBD, and PsO,15,18 is well tolerated and is thus in rampant use for many autoimmune conditions including vasculitis and SLE (Table 1). Despite some favorable effects on relapse rates and disease progression in early trials,26,27 more potent and targeted DMTs were developed as first line treatment options in MS. However, MTX may serve as a therapy for MS patients with comorbid RA, IBD or PsO.
Mycophenolate mofetil (MMF)
Mycophenolate mofetil (MMF) inhibits the enzyme inosine monophosphate dehydrogenase, which is crucially involved in de novo biosynthesis of purine nucleobases. MMF is relatively specific to lymphocytes, because these cells lack salvage pathways for purine biosynthesis compensating for this deficiency. MMF has been widely used for immunosuppression after organ transplantation and has proved to be effective in various autoimmune conditions including IBD, 28 PsO 29 and RA. 30 In a retrospective analysis conducted by Michel et al., 31 MMF failed to influence positively MS-related disability progression as assessed using the Expanded Disability Status Scale (EDSS), yet significantly reduced relapse rates in MS patients. This was further corroborated in a more recent study on patients with progressive MS. 32 Due to limited data on MS and its lack of approval for use in MS, PsO, RA or IBD, MMF might not be among the first choices for a cross-over therapy.
5-Aminosalicylate (5-ASA)
Sulfasalazine consists of sulfapyridine and 5-aminosalicylic acid (5-ASA), which is either absorbed intact or as sulfapyridine. While 5-ASA affects arachidonic acid metabolism and thereby inflammation in IBD, intact sulfasalazine or sulfapyridine – like MTX – have been shown to inhibit folate-dependent enzymes and both appear to be active in RA. 22 Thus, 5-ASA is approved for the treatment of IBD and RA33,34 (Table 1). Regarding MS, sulfasalazine has promoted remyelination and suppressed EAE in several animal models of MS,35,36 yet aggravated EAE or completely failed to show beneficial effects in rat EAE models.37,38 In clinical studies, 5-ASA did not reduce EDSS progression 39 and there is also a case report of a patient developing MS under a long treatment with sulfasalazine. 40 Thus, sulfasalazine may not be considered a suitable therapeutic option for MS, but oral or topical sulfasalazine may serve as an add-on DMT for RA and IBD.
Monoclonal antibodies
Alemtuzumab
Alemtuzumab is a humanized monoclonal antibody targeting and thus depleting CD52-expressing B and T cells. Because of its safety profile, the use of alemtuzumab is reserved for highly active RRMS patients who have not sufficiently responded to other therapies. 41 Initially, the efficacy of alemtuzumab was assessed for the treatment of therapy-refractory RA. 42 However, because of the induction of profound lymphopenia with a concomitant slow immune reconstitution, the trials were eventually cut short. 43 So far, there is only one case report showing a beneficial effect of alemtuzumab in a patient with both chronic plaque PsO and MS; 44 there is only limited experimental evidence for the benefit of an anti-CD52 therapy in IBD. 45 Thus, a certain subgroup of patients with highly active RRMS plus PsO/RA may profit from a treatment with alemtuzumab.
Anti-CD20 antibodies (rituximab, ocrelizumab, ofatumumab)
Anti-CD20 antibodies target and deplete CD20-expressing B cells. Rituximab has been in clinical use for moderate to severe RA since 2006, but has also been utilized for other autoimmune conditions, including demyelinating disorders and certain types of leukaemia.46,47 There is increasing evidence that T and B cells both play equally important roles in the pathogenesis of MS. 48 Moreover, there are several studies and case reports showing the efficacy of rituximab in MS. However, the antibody has not been formally approved for the treatment of RRMS and is thus used off-label to a varying degree with considerable variations across different countries.49,50 Recently, the humanized anti-CD20 antibody ocrelizumab has been shown to reduce disease activity of RRMS and primary progressive multiple sclerosis (PPMS) patients and is the first approved substance for the treatment of PPMS.51,52 Ocrelizumab has also been tested in RA patients, showing a promising safety profile and therapeutic efficacy. 53 In IBD and PsO, the reports for CD20 antibodies have not been as promising: an Icelandic study recently reported a six-fold increased risk of developing an IBD in patients treated with rituximab, 54 and there are several case reports of patients who developed colitis or PsO during an anti-CD20 treatment with rituximab or ocrelizumab.55–58 Immunity critically relies on the homeostasis of pro and anti-inflammatory stimuli and CD20+ cells have an important regulatory and protective role in the gastrointestinal system59,60 as well as the skin; 61 thus B cell depletion may trigger an abnormal B cell-mediated T cell regulation and, as a consequence, PsO or IBD. Thus, CD20 antibodies may be the ideal therapeutic for patients with highly active MS and RA, yet should be carefully considered in MS plus IBD/PsO patients.
Natalizumab
Natalizumab is a humanized IgG4 monoclonal antibody that specifically targets the α4 integrin and thus hampers the invasion of (autoreactive) lymphocytes into the central nervous system (CNS) via α4β1 integrin and into the gut via α4β7 integrin. Natalizumab is approved for the treatment of highly active RRMS, but has also been used in IBD trials, in which the antibody has proved efficient in the induction and maintenance of clinical remission in CD.62,63 However, due to the risk of progressive multifocal leukoencephalopathy (PML) (as a consequence of a reactivation of JC virus), natalizumab is not used in IBD patients. 64 Instead, the humanized monoclonal antibody vedolizumab, which only targets the α4β7 integrin–MAdCAM-1 interaction in the intestinal mucosa thereby avoiding the risk of developing PML, 65 has proved to be the safer therapeutic option for patients with IBD. As the effect of vedolizumab is limited to the intestine, it is not an option for patients with RRMS. 66 Moreover, there have been several cases of MS patients who developed RA or experienced an onset or exacerbation of PsO on treatment with natalizumab.67–70 Natalizumab has been shown to alter the composition of lymphocyte subpopulations in the peripheral blood, with especially CD8+ T and CD19+ B cells being increased. 71 These changes – in addition to the hampered migration of leukocytes across the blood–brain or blood–gut barrier – could shift the inflammatory response from the CNS towards other tissues (e.g. the skin or joints), thus triggering the onset of PsO or RA. Thus, natalizumab may be an elegant option for patients with highly active MS and CD, but should be used with caution in patients with comorbid PsO or RA.
TNFα blockers (adalimumab, infliximab, etanercept, golimumab, certolizumab-pegol)
TNFα is a key pro-inflammatory cytokine that induces the production of C-reactive protein, regulates the ability of antigen-presenting cells to activate T cells and induces the production of various pro-inflammatory cytokines, chemokines and cell-adhesion molecules. 72 Hence, blocking TNFα with monoclonal antibodies (adalimumab, infliximab, golimumab and certolizumab-pegol) or the soluble TNFα receptor–IgG fusion protein etanercept, has proved to be a very effective therapeutic strategy for several autoimmune conditions, including PsO, RA and IBD73,74 (Table 1). Moreover, TNFα has an even broader range of effects, as tumor necrosis factor alpha receptors (TNFRs) are expressed in almost every cell type. 75 However, there are multiple case reports of TNFα blockers promoting or exacerbating demyelinating diseases.6–8 The potential underlying mechanism was unravelled by the discovery of a MS-associated Δ6-TNFR1 genetic variant. 76 This gene encodes a soluble protein comprising the extracellular TNFR1 domain (TNF receptor 1), and acts as a decoy receptor for TNFα (similar to etanercept), thus preventing potentially neuroprotective signalling through membrane-bound TNFR1. Furthermore, MS is positively associated with many other TNFα gene variants. 77 Therefore, an ongoing anti-TNFα therapy (for PsO, RA or IBD) should be discontinued in patients with coexisting MS.
Tocilizumab and satralizumab
Tocilizumab and satralizumab are monoclonal humanized IL-6 receptor antibodies, which have become a valuable therapeutic asset in several inflammatory conditions, including RA, 78 giant cell arteritis (GCA) and aquaropin-4-positive NMOSD. 79 Although there are a few case reports describing a presumably secondary CNS autoimmunity on tocilizumab treatment, it has to be taken into account that one of these patients was treated with TNFα blockers prior to tocilizumab and two patients had an already established MS and relapsed during the treatment.80–82 On the other hand, there are also reports of a successful MS therapy with tocilizumab;81,83 there is further experimental evidence showing that blockage of IL-6R can be protective of EAE. 84 However, considering the lack of clinical data, we cannot recommend the general use of tocilizumab in patients with MS and RA.
Secukinumab
Secukinumab is a fully human monoclonal IgG1κ IL-17A antibody, which has demonstrated efficacy in phase II and III trials of PsO, psoriasis arthritis and RA.85–87 The IL23/Th17 axis plays a major pathophysiological role in many autoimmune disorders and has particularly been linked to disease severity in PsO and MS.2,3 In fact, Th17 cells were initially described in the EAE model.88,89 Secukinumab has demonstrated promising trends in a phase II trial with RRMS patients; 4 although the study’s primary endpoint was not reached. Moreover, there are several case reports that describe a successful treatment of comorbid PsO/MS with secukinumab.90–94 All patients described had a relapsing–remitting disease course and remained clinically and radiologically stable during their respective follow-up periods. Thus, more advanced monoclonal IL-17 antibodies with improved pharmacodynamics, such as brodalumab (anti-17A) or ixekizumab (anti-17A) may also be considered for application in MS. Hence, secukinumab may be one of the best therapeutic options for patients with PsO and coexisting RRMS.
Ustekinumab
Ustekinumab is a fully human monoclonal antibody, targeting the p40 epitope of IL-12 and IL-23. Therefore, ustekinumab blocks the differentiation of naive CD4+ lymphocytes into Th1 and Th17 cells and has shown clinical efficacy in phase III studies for PsO and IBD.95–97 In MS animal models, ustekinumab has proved effective 98 and IL-23R−/− mice are even protected from EAE.99,100 Yet ustekinumab failed to transfer those results to a clinical phase II trial. 101 This was further corroborated in an EAE model with mice lacking the p40-ustekinumab target epitope. 102 However, the patients included in the ustekinumab study had a chronic disease course with long disease durations with low relapse activity. Furthermore, it is not clear whether the antibody can cross the blood–brain barrier effectively. Nevertheless, there are two case reports of patients with MS and comorbid PsO successfully treated with ustekinumab. 103 Interestingly, these patients also had a chronic disease course, but did not experience disease progression over a follow-up period of 3–4 years. Taken together, ustekinumab and potentially also other IL-23 antibodies (risakinzumab, tildrakizumab and guselkumab) may have beneficial effects in early MS, but further research needs to be conducted.
Oral/injectable MS therapeutics
Fumaric acid esters
The anti-inflammatory effect of fumarates on psoriatic lesions was initially discovered in the late 1950s 104 and it took almost half a century until dimethyl fumarate (DMF) was finally introduced as a potent MS therapeutic. 105 DMF exerts its anti-inflammatory effects through activation of the nuclear factor erythroid 2-related factor 2 (Nrf2) transcriptional pathway and the interaction with hydroxycarboxylic acid receptor 2 (HCAR2),106,107 which fosters the upregulation of antioxidant and cytoprotective response genes 108 and shifts T cells from a Th1/Th17 profile towards a Th2 phenotype. This was further corroborated by experimental results in murine PsO and EAE models as well as in humans. 109 Fumarates are approved for the treatment of mild to moderate RRMS, moderate to severe PsO110–112 (although both being approved in distinct disease-specific drug formulations) and have shown promising results in a model of experimental colitis. 113 Furthermore, DMF is in phase II clinical testing for the treatment of RA. 114 As DMF is approved for both RRMS and PsO, it is the obvious choice for patients with this particular comorbidity, as exemplified by case reports of patients who experienced remission of PsO flares and additionally remained MS relapse-free on a treatment with DMF.115,116 However, especially older patients may be at risk of developing PML.
Interferons
Interferons (IFNs) are long established DMTs for the treatment of mild to moderately active MS. Similar to results in EAE models, IFNs have shown efficacy in murine models of experimental arthritis,117,118 yet – unlike in MS – these results were either not replicated in RA patients 119 or showed conflicting results.120–122 The same holds true for IBDs and PsO.123–128 Exacerbations of autoimmune conditions during an IFN treatment are actually not uncommon and have also been shown for NMOSD.129,130 In PsO, this may be due to a direct involvement of IFNs in PsO pathophysiology: type 1 interferons (IFNα and IFNβ) are key cytokines induced during skin damage; psoriatic lesions can be triggered by skin injury, also known as ‘Köbners phenomenon’. 131 Furthermore, the type 1 IFN pathway is necessary for the development of psoriasis-like inflammatory diseases in mice.132,133 Ultraviolet (UV) light therapy, on the other hand, ameliorates PsO flares, as it triggers ubiquitination and downregulation of the type 1 interferon receptor IFNAR1 and thus IFN signalling. 134 Yet despite these negative associations, an established IFN therapy in MS patients should not necessarily be discontinued when a second autoimmune condition is diagnosed.
S1PR modulators (fingolimod, siponimod, ozanimod)
S1PR modulators cause an internalization and degradation of S1PRs, thus trapping lymphocytes in secondary lymphoid organs (e.g. lymph nodes). 135 This reduces the number of circulating lymphocytes and ultimately precludes their invasion into the CNS. In 2010, the non-selective S1PR modulator fingolimod was the first orally administered drug approved for the treatment of highly active RRMS. 136 Since then, siponimod and now also ozanimod have been approved as DMTs for patients with secondary progressive multiple sclerosis (SPMS) and RRMS, respectively. While S1PR modulators have shown promising results in MS, they also have the potential to be useful DMTs in IBD, RA or PsO, as recently demonstrated in various animal models.137–142 While there are no clinical data on S1PR modulators in RA, and two studies regarding PsO,143,144 the TOUCHSTONE (NCT01647516) and STEPSTONE (NCT02531113), as well as the ‘True North’ trials demonstrated that ozanimod is safe, well tolerated and effective in patients with moderate to severe UC.5,145 Taken together, especially ozanimod could be an elegant monotherapy option for patients with highly active MS and moderate to severe IBD.
Teriflunomide and leflunomide
Teriflunomide and leflunomide reversibly inhibit the mitochondrial enzyme dihydroorotate dehydrogenase (DHODH), causing a decreased de novo pyrimidine synthesis, thus diminishing T- and B cell activation and proliferation. 146 Teriflunomide is approved for the treatment of mild to moderate RRMS, whereas its pro-drug leflunomide is in clinical use for the treatment of RA and psoriatic arthritis.147,148 Gastrointestinal symptoms are among the most common unwanted side effects of teriflunomide, but these events are usually mild and self-limiting. However, there are a few cases of severe (lymphocytic) colitis with teriflunomide treatment in patients with RRMS,149,150 and teriflunomide has also been associated with the onset of PsO.151,152 However, as these are single case reports, a discontinuation of teriflunomide in patients with comorbid PsO and IBD should be carefully considered, while in patients with mild to moderate RRMS and coexisting RA, teriflunomide remains a valid therapeutic option.
Discussion
In the following, we suggest three pragmatic treatment approaches for patients with MS and coexisting autoimmune disorders (Figures 1–3). After exclusion of contraindicated drugs, the therapeutics should be chosen according to the individual patient’s disease activity. Table 2 shows the safety rating. Table 1 shows the FDA approval status of the respective immunosuppressants. Overall, TNFα blockers are effectively utilized in PsO, RA and IBD, yet have doubtlessly been shown to exacerbate or induce demyelination. Thus, TNFα blockers are the only real absolute contraindication for all patients with coexisting MS (Figures 1–3; Table 2).

Flow chart showing the decision-making process for patients with MS and PsO. Descriptions are given in the main text.
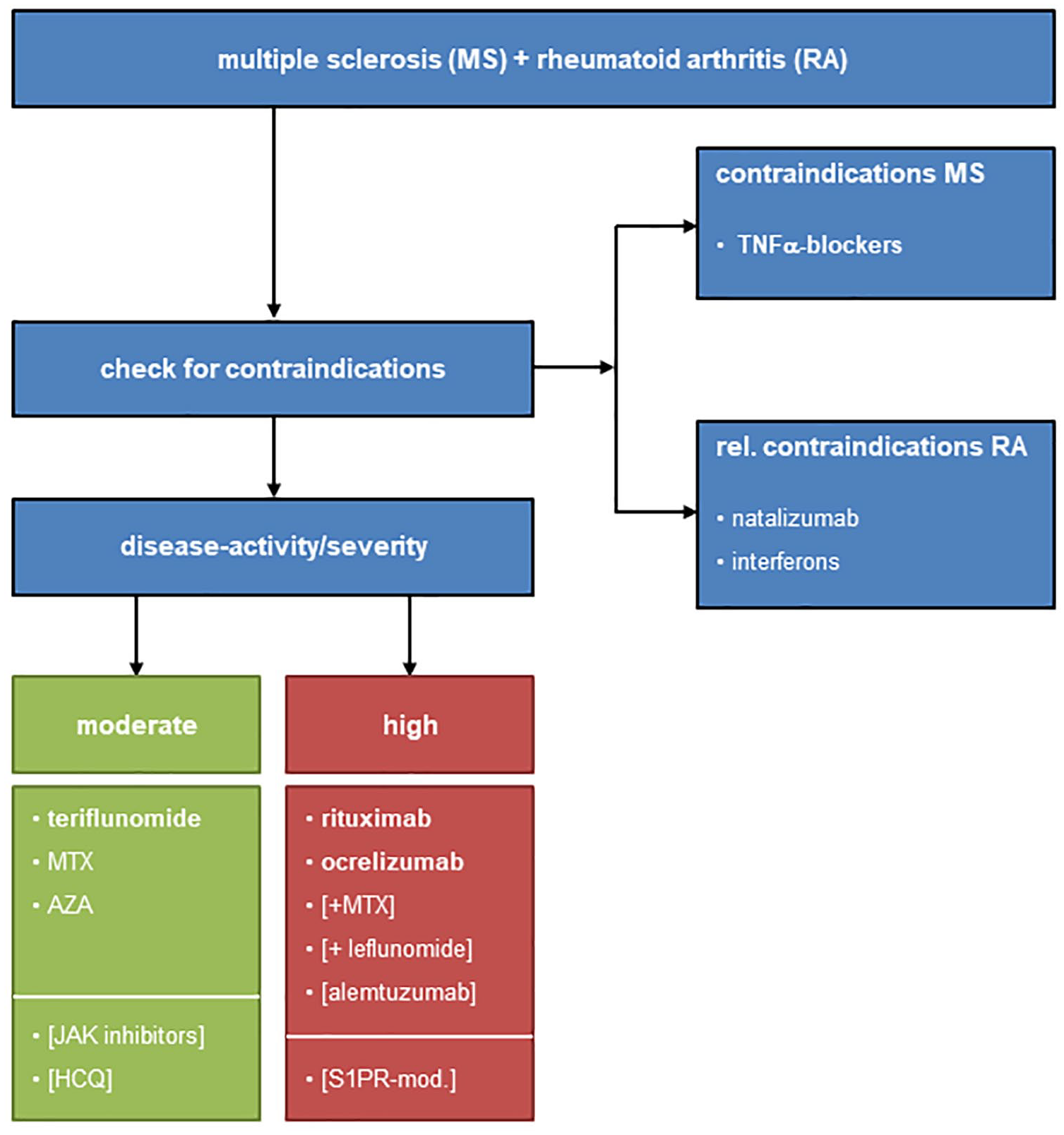
Flow chart showing the decision-making process for patients with MS and RA. Descriptions are given in the main text.

Flow chart showing the decision-making process for patients with MS and IBD. Descriptions are given in the main text.
Efficacy and safety rating for each disease-modifying therapy with regard to use in the main autoimmune disorders discussed here.

Color gradient ranges from absolutely contraindicated (dark red) to highly effective (dark green). – – –, absolutely contraindicated; (−), possibly harmful; (+), possibly effective; (+/−), mixed reports; (+++), highly effective; but restricted label due to safety concerns; –, harmful; +, effective; ++, very effective; +++, highly effective; 0, not effective.
5-ASA, 5-aminosalicylic acid; ALEM, alemtuzumab; Anti-CD20, CD20-antibodies; Anti-TNFα, TNFα antibodies; AZA, azathioprine; CYA/TAC, cyclosporine/tacrolimus; DMF, dimethylfumarate; HCQ, hydroxchloroquine; IBD, inflammatory bowel disease; IFN, interferon; JAK, Janus kinase inhibitor; MMF, mycophenolate mofetil; MS, multiple sclerosis; MTX, methotrexate; NATA, natalizumab; PsO, psoriasis; RA, rheumatoid arthritis; S1PR, sphingosin-1-phosphate receptor modulator; SEC, secukinumab; TER/LEF, teriflunomide/leflunomide; TOC, tocilizumab; USTE, ustekinumab; x, no data.
MS plus PsO (Figure 1)
As a chronic inflammatory skin condition, PsO can be treated not only systemically, but depending on disease severity and the existence of extracutaneous manifestations (e.g. psoriasis–arthritis), topical DMTs are also available. Those therapeutics can be combined with every DMT approved for MS.
Fumarates have proved effective in both RRMS and PsO, thus patients with a moderate disease course could be set on a monotherapy with DMF or alternatively a combination of DMF and MTX or CYA. Patients with highly active RRMS and more severe psoriasis could benefit from a monotherapy with secukinumab or a combination of secukinumab and DMF or MTX. As secukinumab has already been tested in a clinical phase II trial and there are several case reports of its successful application in RRMS patients,90–94 the anti-IL17 antibody has – in comparison with other DMTs – the highest level of clinical evidence. However, it needs to be taken into account that the trial by Havrdova et al. 4 failed to reach its primary endpoint [the cumulative number of combined unique active lesions (CUALs) observed in magnetic resonance imaging (MRI) scans within 2 years], while still showing a significant reduction in cumulative new gadolinium-enhancing T1 lesions (secondary endpoint). Hence, larger, better powered trials are still needed to evaluate further the benefit of IL-17 targeting in RRMS patients (e.g. brodalumab, ixekizumab).
S1PR modulators have shown promising results in various PsO mouse models, demonstrating strong anti-proliferative and anti-inflammatory effects, significantly reducing the animals’ disease burden.137,138 This has been further corroborated in clinical studies with PsO patients, which demonstrated a significant reduction of PsO plaque burden on treatment with the S1PR modulator ponesimod;143,144 interestingly, ponesimod is about to be approved for its application in RRMS. 153 Thus, in addition to anti-IL17 antibodies, S1PR modulators may be another good alternative for patients with highly active RRMS and coexisting PsO. Patients with concomitant active SPMS and PsO may be treated with siponimod, yet there are no clinical data to support this assertion. Certain subgroups of RRMS patients with comorbid PsO may also profit from a therapy with alemtuzumab, yet there is only one single case report to support this approach. 44
There have been several case studies describing an onset or exacerbation of PsO in MS patients treated with CD20 antibodies, teriflunomide, natalizumab and IFNs. However, these studies are mostly based on single case reports, whereas the vast majority of patients did not exhibit comparable unwanted side effects. Thus, the application of those DMTs should be carefully evaluated in patients with MS and coexisting PsO, yet they should not be generally excluded from the therapeutic arsenal, especially when patients have remained relapse free with these substances.
RA plus MS (Figure 2)
The DHODH inhibitors teriflunomide and leflunomide are approved for moderate RRMS and RA, respectively. Even though leflunomide is the pro-drug of teriflunomide and there is vast clinical experience with both DMTs, slight differences between the two substances or the respective patient populations (RA/MS) cannot be completely excluded. However, as DHODH inhibitors are already in clinical application for both conditions, teriflunomide is the obvious choice for patients with moderate RRMS and comorbid RA. Although MTX is not commonly used in patients with RRMS, the DHFR inhibitor has a rather favorable therapeutic profile and is the most frequently used DMT in RA. Thus, MTX could also be utilized as a second line crossover DMT. The same holds true for AZA.
Patients with highly active RRMS and RA have both shown responsiveness to anti-CD20 antibodies (rituximab/ocrelizumab). In RA, rituximab is readily combined with other DMARDs (leflunomide or MTX), 15 which could additionally prohibit MS progression, but may also be a source of unwanted side effects and should therefore be carefully evaluated.
Patients with PPMS and RA could profit from ocrelizumab therapy, yet ocrelizumab is only approved for the application in MS. HCQ, which is now only rarely used in RA therapy, may potentially become another option for PPMS in the future, but so far there are only experimental data available. The same is true for S1PR modulators, which have shown promising results in experimental arthritis models, but have not yet been tested for their clinical application in RA. In the early to mid-1990s, alemtuzumab was successfully applied in certain cohorts of therapy-refractory RA patients, 42 yet its use has not prevailed due to its unfavorable safety profile and prolonged lymphopenia. However, as mentioned for PsO, certain subgroups of RRMS patients with comorbid RA might profit from a therapy with alemtuzumab.
The CTLA4 fusion protein abatacept and the recombinant IL-1 receptor antagonist anakinra are both approved for RA and have also been tested in patients with RRMS, yet have either failed to show beneficial effects on disease progression, 154 or the trials are still ongoing (anakinra: NCT04025554).
There are several case reports describing an onset or exacerbation of RA in MS patients treated with natalizumab and interferons.70,120–122 However, as discussed for PsO, these are single case reports and a general discontinuation of an already established MS therapy – after RA onset – should be carefully evaluated.
IBDs plus MS (Figure 3)
While mild cases of IBD can be treated with local (rectal) glucocorticoids (e.g. budesonide) and/or salicylates (5-ASA), severe, refractory cases may need surgical attention. As mentioned for PsO, these topically administered substances should be continued throughout the MS therapy. However, the standard relapse prophylactic for IBDs – oral 5-ASA – did not show a significant effect on MS disease progression and is thus not suitable for a combinatory treatment.
While AZA is no longer commonly used as a DMT in MS, the thiopurine is readily utilized as a monotherapy to maintain remission in IBD and is therefore the evident option for a combinatory therapy. If AZA is not well tolerated, MTX remains a possible secondary option. 155 The calcineurine inhibitor CYA is approved as a remission-inducing agent in severe, steroid refractory UC.16,17 Yet, because of the side effects of CYA, it is not generally used as a long-term therapeutic; remission maintenance is usually achieved instead with thiopurines or vedolizumab. Hence, CYA is not an optimal DMT for patients with coexisting MS and IBD, but may be carefully considered in certain cases.
Natalizumab has proved effective in the induction and maintenance of remission in IBDs. Hence, a natalizumab monotherapy is a valid therapeutic option for patients with highly active RRMS and IBD. Alternatively, ozanimod has recently been approved for both RRMS and moderate to severe IBD, thus especially patients with high documented JC virus titers could benefit from a treatment with the S1PR modulator.
Due to frequently reported gastrointestinal side effects and recent reports of refractory lymphocytic colitis under teriflunomide,149,150 the DHOD inhibitor may not be the best therapeutic choice for patients with RRMS and comorbid IBD. The same is true for CD20 antibodies, which have also been associated with the onset of colitis. This is further corroborated by several animal models, demonstrating that B-cell depletion can deregulate the gastrointestinal immune system by increasing inflammatory cytokines in both blood serum and intestinal tissue.156,157 Nevertheless, those cases are also reports of rare instances and should not be over-interpreted.
The immunomodulatory drug glatiramer acetate (GLAT), is commonly used in patients with moderate RRMS, but has – from a pathophysiology perspective – no clear application in other autoimmune disorders. Nevertheless, there are a few studies in IBD animal models that demonstrate a therapeutic effect of GLAT158,159 via the induction of regulatory T cells. 160 Thus, GLAT may potentially have a broader application outside of MS, but so far there are only experimental data available.
Future perspectives
As therapeutic strategies for cancer and autoimmune diseases of different organs target similar pathways and thus show some parallels, novel approaches in one of these fields often emerge from neighboring disciplines and benefit from experiences made there. The latter, together with distinct contrasting effects of treatments in different diseases, provides valuable insight for overlapping clinical conditions with more than one disease. Targeting specific intracellular signalling cascades or tyrosine kinases with small molecule inhibitors has become a general therapeutic strategy in medical oncology. Thus, as shown for former chemotherapeutics – such as MTX or AZA – this trend has now also spread to autoimmune disorders, as demonstrated by Janus kinase inhibitors.
Janus kinases (JAKs) are cytoplasmic protein tyrosine kinases that mediate the induction of STAT proteins, which then activate the transcription of various pro-inflammatory cytokines (e.g. INFγ or TNFα). JAK inhibitors, such as tofacitinib, ruxolitinib or baricitinib, have shown efficacy in the treatment of several inflammatory conditions and are approved for the treatment of PsO, RA and UC.161–163 In general, these small molecule inhibitors are less effective than biologicals, yet have proved to be advantageous because of their oral/topical administration and overall cost-effectiveness. 164 Although there have been conflicting results for JAK inhibitors in EAE models and MS patients,165,166 the JAK/STAT pathway is critically involved in MS pathophysiology, 167 thus JAK inhibitors may also become available for MS in the future.
In the past decades, immunotherapy has become more and more precise, targeting specific cytokines (e.g. IL-17) or cell types (e.g. B cells). According to numerous experimental animal models, MS was primarily considered a T-cell-mediated disease. However, there is an increasing amount of evidence for the importance of B cells and humoral immunity in the genesis of demyelinating lesions, making especially the BAFF/APRIL system a possible therapeutic target. 168 B cell-activating factor (BAFF) and a proliferation-inducing ligand (APRIL) are inflammatory cytokines, which are primarily involved in B cell survival, maturation and activity. 169 Yet, thus far targeting BAFF and/or APRIL with monoclonal antibodies or a soluble decoy TACI-Fc fusion protein did not bring the desired results in MS patients.170,171 One possible explanation is that the soluble decoy TACI-Fc fusion protein atacicept only has a B cell subset-specific effect and might have disturbed the fine-tuned balance of conventional and regulatory B cells, resulting in excessive T cell responses. Furthermore, the BAFF antibody tabalumab, as well as atacicept, spares memory B cells, thus T cell activation may still be preserved. 170 Similar results and conclusions have been obtained for the application of atacicept and tabalumab in RA. 172 Nevertheless, in spite of these negative results, CD20 antibodies have demonstrated the efficacy of B cell targeting therapies, thus we may see the emergence of new B cell-associated therapeutics for MS and RA in the future. In this regard, the Burton tyrosine kinase (BTK) is critically involved in B cell signalling and small molecule BTK inhibitors (e.g. tolebrutinib, evobrutinib) have shown promising results in preclinical MS and also RA models 173 as well as in clinical trials. 174 Moreover, there are several ongoing phase III trials on BTK inhibitors in MS. Thus, BTK inhibitors may soon become readily used substances in MS, RA and potentially also other inflammatory conditions.
Although it is not uncommon for MS patients to present with comorbid autoimmune disorders such as PsO, RA, and IBD, the likelihood of recruiting sufficient numbers of these patients for large-scale clinical trials in the foreseeable future is low. This emphasizes the importance of case reports and review articles, until the growing arsenal of new immunosuppressants is able to provide more straightforward treatment approaches for patients with MS and coexisting autoimmune disorders.
Footnotes
Acknowledgements
The authors thank Cheryl Ernest for proofreading and editing the manuscript.
Conflict of interest statement
TB has no competing interests to declare. TR received travel grants and financial research support from Genzyme and Novartis and received honoraria for lecturing from Roche, Merck, Genzyme, Biogen and Teva. SGM received honoraria for lecturing and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and by Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, Merck Serono, Novartis, ONO Pharma, Roche and Teva. FZ has recently received research grants and/or consultation funds from DFG, BMBF, PMSA, MPG, Genzyme, Merck Serono, Roche, Novartis, Sanofi-Aventis, Celgene, ONO and Octapharma. SB has received honoraria and compensation for travel from Biogen Idec, Merck Serono, Novartis, Sanofi-Genzyme and Roche.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Research Council (DFG, CRC-TR-128 to FZ, SGM and SB) and Hertie-Stiftung (SB).