
Abstract
Background:
Serum neurofilament light chain (sNfL) is a promising biomarker to complement the decision-making process in multiple sclerosis (MS) patients. However, although sNfL levels are able to detect disease activity and to predict future disability, the growing evidence has not yet been translated into practicable recommendations for an implementation into clinical routine.
Methods:
The observation of a patient with extensive inflammatory activity in magnetic resonance imaging (MRI) along with an extremely high sNfL level in the absence of any clinical symptoms prompted us to investigate common characteristics of our MS patients with the highest sNfL levels in a retrospective cohort study. The 97.5th percentile was chosen as a cut-off value because the mean sNfL level of the resulting extreme neurofilament light chain (NfL) cohort corresponded well to the sNfL level of the presented case. Patient characterization included clinical and MRI assessment with a focus on disease activity markers. sNfL levels were determined by single molecule array.
Results:
The 97.5th percentile of our MS cohort (958 sNfL measurements in 455 patients) corresponded to a threshold value of 46.1 pg/ml. The mean sNfL level of the extreme sNfL cohort (n = 24) was 95.6 pg/ml (standard deviation 68.4). Interestingly, only 15 patients suffered from a relapse at the time point of sample collection, whereas nine patients showed no signs of clinical disease activity. sNfL levels of patients with and without relapse did not differ [median 81.3 pg/ml (interquartile range [IQR] 48.0–128) versus 80.2 pg/ml (IQR 46.4–97.6), p = 0.815]. The proportion of patients with contrast-enhancing lesions was high and also did not differ between patients with and without relapse (92.9% versus 87.5%, p = 0.538); 78.9% of the patients not receiving a high-efficacious therapy had ongoing disease activity during a 2-year follow-up.
Conclusion:
Extremely high sNfL levels are indicative of subclinical disease activity and might complement treatment decisions in ambiguous cases.
Keywords
Introduction
Recent advances in multiple sclerosis (MS) immunotherapies provide the tools to attempt optimal disease control along with personalized therapy on the basis of individualized treatment decisions. 1 Monitoring of disease activity usually consists of clinical assessment and magnetic resonance imaging (MRI) with recommended monitoring intervals depending on the applied disease-modifying treatment (DMT). However, current standard procedures bear the risk that subclinical disease activity in between MRI control time points will go unnoticed, leading to delayed treatment adaptations. Furthermore, deciding on an adequate DMT can be challenging in some situations.
Neurofilament light chain (NfL) is currently one of the most studied biomarkers in MS and other neurological diseases that might be able to close this prognostic and diagnostic gap in the future.2,3 Following axonal damage, NfL, along with other structural proteins, is released into the cerebrospinal fluid (CSF) and to a lesser extent into the serum. 4 Ultrasensitive antibody-based analytical techniques including single molecule array (SiMoA) technology enable the detection of low concentrations of NfL in serum neurofilament light chain (sNfL) and its alterations. 5
In MS, increasing sNfL levels are associated with clinical relapses2,6 and disability. 6 Furthermore, it has been shown by our group and others that active MRI contrast-enhancing lesions (CELs) are substantially associated with sNfL levels,3,5,7–9 indicating the potential of sNfL to detect subclinical disease activity. sNfL might also be used as a prognostic marker because sNfL levels at disease onset can predict future relapses 3 and longer-term outcome, 10 whereas the initiation of immunotherapy is associated with decreasing sNfL levels.2,3,5,6,11 Interestingly, changes in sNfL levels reflect escalation/de-escalation decisions as well. 3 However, due to a lack of practicable recommendations concerning test intervals and cut-off values that require treatment interventions, this increasing knowledge on sNfL as a biomarker in MS has not yet been integrated into clinical patient care.
Here, we report a patient who presented with extending MRI activity and extremely high sNfL levels in the absence of any clinical signs of disease activity, which made therapy consultation challenging. This observation prompted us to analyze common characteristics of our MS patients with the highest sNfL levels in a large retrospective cohort study (n = 958). Notably, about one-third of these extremely high sNfL values were also detected during clinically stable disease phases, and the majority of these patients required high-efficacious immunotherapy during a 2-year follow-up. Therefore, our study might serve as an instructive example on how sNfL assessments could contribute to disease activity monitoring and personalized treatment recommendations for MS patients in the future clinical routine.
Methods
Standard protocol approvals, registrations, and patient consent
The study was approved by the Ethics Committee of the Rhineland-Palatinate Chamber of Physicians (number 837.019.10). Written informed consent was obtained from all patients included in the Mainz NfL cohort. The patient of the included exemplary case presentation also gave written informed consent to publish her clinical data, radiological findings, and laboratory test results in this scientific case report.
Study design
NfL levels were determined in 958 serum samples of 455 patients with a diagnosis of clinically isolated syndrome (CIS) or relapsing–remitting multiple sclerosis (RRMS) (according to the 2017 revision of the McDonald criteria) 12 from the MS outpatient clinic of the Department of Neurology at the University Medical Center Mainz (Mainz, Germany). Patients with extremely high sNfL levels defined as values above the 97.5th percentile (subsequently referred to as the ‘extreme NfL cohort’) were retrospectively characterized with regard to clinical and MRI findings (Figure 1). This cut-off value was chosen because the mean sNfL value of the resulting cohort corresponded well to the sNfL level of our presented case. Furthermore, two previous studies were able to demonstrate that sNfL levels above the 97.5th percentile are associated with an increased risk of relapses and Expanded Disability Status Scale (EDSS) worsening within 12 months 6 as well as brain and spinal cord volume loss over 5 years. 8

Study design.
Assessment of clinical data
The clinical assessment included the determination of signs of clinical disease activity (relapse defined as new neurological symptoms lasting >24 h along with the exclusion of Uthoff’s phenomenon) within 90 days prior to sample collection and the rating of EDSS scores at the time point of sample collection. Furthermore, the application of steroids within 30 days prior to sample collection, history of relapses, DMTs within 2 years after sample collection, and comorbidities were documented.
In patients with a follow-up time of at least 2 years after sample collection, physicians’ recommendations to switch to a higher efficacy DMT (i.e. treatment escalation) due to continued relapses or new MRI lesions were recorded. However, some patients decided not to follow these recommendations due to individual preferences. Therefore, we chose treatment escalation recommendation instead of actual treatment escalation as an outcome parameter.
MRI analysis
The presence and number of contrast-enhancing, ring-enhancing and tumefactive lesions (defined as demyelinating lesions with a diameter >2 cm and associated mass effect and/or edema) 13 were assessed in a cerebral MRI that was performed within 3 months prior to or following serum collection. In addition, quantitative maps were analyzed in the regions of interest, namely hyperintense lesions. Lesion delineation was performed manually on the spatially normalized fluid-attenuated inversion recovery (FLAIR) images slice by slice using the freely available software MRIcron (http://people.cas.sc.edu/rorden/mricron/index.html). In patients who also received a spinal MRI, the numbers of T2 lesions and CELs were determined. An experienced rater blinded to sNfL levels and clinical data assessed all images.
Processing and NfL single molecule array of serum samples
Serum samples were collected following standard procedures. After 30–45 min at room temperature, separation of serum was achieved by differential centrifugation at 2000
Statistical analysis
Continuous variables were tested for normal distribution using the Shapiro–Wilk test. Comparisons of the mean between two groups were tested by Student’s t test in the case of normal distribution and by the Mann–Whitney U-test in non-normally distributed variables. Categorical variables were compared with the chi 2 test and Fisher’s exact test if appropriate. p Values of less than 0.05 were considered significant.
Data availability
The raw data used in preparation of the figures and tables will be shared in anonymized format upon request of a qualified investigator to the corresponding author for purposes of replicating procedures and results.
Results
Case presentation
A 39-year-old Caucasian female patient from Cyprus was diagnosed with CIS in April 2016 according to the 2010 McDonald criteria 14 after presenting at the local outpatient clinic in Cyprus with hypoesthesia of the lower body due to active myelitis at thoracic level 5/6. MRI revealed an additional non-contrast-enhancing cerebral lesion in the right parietal lobe. In CSF analysis, leukocyte count [0 white blood cells (WBCs)/mm2] and protein levels (29.9 mg/dl) were within normal ranges; the oligoclonal bands (OCBs) were negative. A 5-day steroid pulse resulted in partial improvement with mild residual symptoms corresponding to an EDSS score of 1.5. As the clinical and radiological follow-up examinations did not reveal any signs of ongoing disease activity, it was decided to monitor the patient’s disease course carefully without immediately starting a DMT.
Although the patient did not perceive any new symptoms, a scheduled MRI in November 2018 revealed numerous new lesions and CELs in the periventricular and juxtacortical white matter, as well as a new spinal lesion at the level of C3. One lesion in the right parietal lobe had a diameter of 2.5 cm and showed signs of a mass effect, and was therefore classified as tumefactive. In total, there were now 27 lesions to be distinguished, of which 23 were contrast-enhancing (Figure 2A). Due to the unexpected MRI findings, CSF analysis was repeated and showed that OCBs were now positive. As the presence of a tumefactive lesion in the absence of correlating clinical symptoms was considered atypical, a brain biopsy was performed in November 2018. Histopathological findings were consistent with an active MS lesion and revealed no evidence of malignancy. According to the 2017 revised diagnostic criteria, the patient was then diagnosed with RRMS. 12 In the light of the extending focal inflammatory activity in MRI, a 3-day steroid pulse was administered.

Case presentation. A. Magnetic resonance imaging (MRI) findings over time: The first row shows axial and sagittal images of fluid-attenuated inversion recovery (FLAIR) sequences and T1 sequences after gadolinium (Gd) administration before treatment initiation. The arrow indicates the tumefactive lesion. The second row shows remission of lesions after treatment initiation with ocrelizumab. B. Serum neurofilament light chain (sNfL) levels over time in temporal relationship to treatment.
When the patient was referred to the outpatient clinic of the Department of Neurology at the University Medical Center Mainz in January 2019, the assessment of sNfL revealed a remarkably high value of 90.5 pg/ml. Initiation of a high-efficacy DMT was recommended to prevent further disease progression and disability. Recent concerns regarding the safety profile of alemtuzumab 15 and the increased risk of developing progressive multifocal leukoencephalopathy on natalizumab therapy in a patient with a high anti-JC virus antibody index, 16 argued against the use of these two monoclonal antibodies. Based on careful risk–benefit considerations, it was therefore decided to start therapy with ocrelizumab. The first cycle was administered in two subsequent doses in January 2019 and was well tolerated. Treatment initiation was associated with a dramatic reduction in radiological disease activity in the MRI in February 2019 (Figure 2A). The second cycle of ocrelizumab was administered in July 2019. Regular follow-up examinations revealed a stable clinical and radiological disease course. In December 2019, the sNfL level had dropped to 11.9 pg/ml (Figure 2B). With regard to this remarkable amelioration of disease course, a de-escalation of the immunotherapy is now being considered.
Characteristics of patients of the extreme NfL cohort
The mean sNfL level in our cohort (958 sNfL measurements in 455 patients) was 11.5 pg/ml [standard deviation (SD) 19.3] and the median was 7.2 pg/ml [interquartile range (IQR) 4.7–11.6; Figure 3A]. All sNfL values above the 97.5th percentile, corresponding to a threshold value of 46.1 pg/ml, were considered ‘extreme’ and were thus included in further analyses. The resulting extreme NfL cohort (n = 24) had sNfL levels ranging from 46.1 pg/ml to 364.0 pg/ml (mean 95.6 pg/ml, SD 68.4, median 80.7, IQR 49.3–108.3).

Cohort overview. A. Overview of all serum neurofilament light chain (sNfL) measurements (n = 958). The horizontal line denotes the median, boxes indicate the interquartile range (IQR), and whiskers represent the 2.5th and the 97.5th percentile. The Y-axis is shown in logarithmic scale. B. As in A, boxes represent the IQR and whiskers denote the 2.5th and the 97.5th percentile of all sNfL measurements. sNfL values of the extreme neurofilament light chain (NfL) cohort are shown as individual circles. Red color indicates relapse at the time of sample collection, blue color indicates clinically stable disease. The patient of the case presentation is shown as a triangle.
Interestingly, only 15 (62.5%) of the extremely high sNfL values were detected in patients with a relapse within 90 days prior to sample collection, whereas nine (37.5%) were collected during clinically stable disease phases (Figure 3B). There was no difference between sNfL levels of patients with and without relapse [median 81.3 pg/ml (IQR 48.0–128) versus 80.2 pg/ml (IQR 46.4–97.6), p = 0.815; Figure 4A]. Furthermore, there was no difference in EDSS scores between patients with and without relapse [1.4 (SD 1.2) versus 0.9 (SD 1.3), p = 0.347]. However, patients with a relapse at the time point of sample collection had significantly shorter disease duration than patients without relapse [median 1.5 months (IQR 1.0–2.0) versus 17.5 months (5.5–36.0)]. In fact, most of them (93.3%) were first diagnosed with RRMS at this time. In total, 45.8% of the patients received steroids prior to sample collection (60.0% of patients with relapse versus 22.2% without relapse, p = 0.105). sNfL levels did not differ in patients with prior steroid treatment (median 95.2 pg/ml, IQR 52.7–128) compared to patients without prior steroid treatment (median 66.7 pg/ml, IQR 48.0–95.4; p = 0.134).
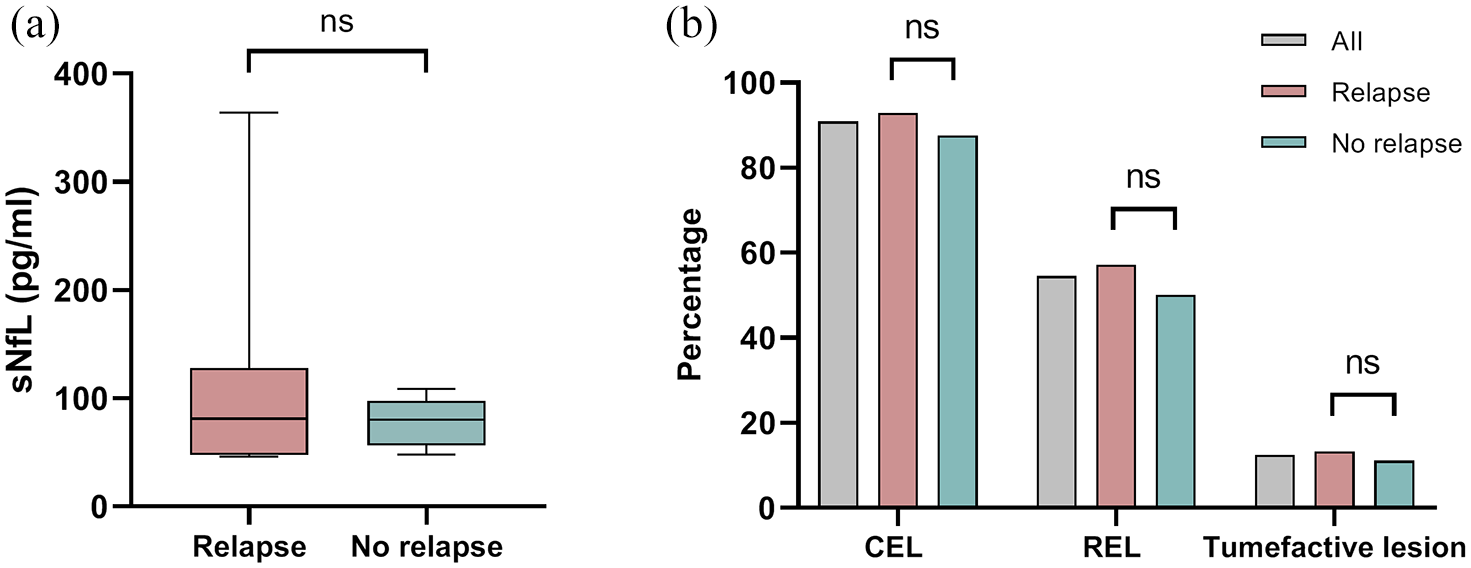
sNfL levels and disease activity markers. A. We observed no differences in serum neurofilament light chain (sNfL) levels between patients with (n = 15) and without (n = 9) relapse in the extreme NfL cohort. B. Comparison of magnetic resonance imaging (MRI) activity markers between patients with and without relapse revealed no differences between the proportion of patients with contrast-enhancing lesions (CELs), ring-enhancing lesions (RELs) and tumefactive lesions.
In addition to the patient presented above (who received ocrelizumab), one other patient was also treated with a high-efficacious DMT (alemtuzumab) as a first-line therapy. Eight patients were initially treated with dimethyl fumarate or fingolimod, and 11 with interferon beta or glatiramer acetate. Three patients chose not to start an immunotherapy. Twenty-one of the 24 extreme NfL cohort patients presented to our outpatient clinic for annual clinical and MRI examinations for at least 2 years after sample collection. Of the 19 patients that started with no, low or moderate DMT, 15 experienced disease activity during the 2-year follow-up and were thus recommended to escalate treatment (Table 1).
Comparison of clinical characteristics between patients with and without relapse.

Patients in the extreme sNfL cohort with and without relapse did not differ in age, sex distribution, disability levels, pretreatment or presence of comorbidities (including diabetes mellitus type 1, Hashimoto thyroiditis and anemia). However, patients with a clinical relapse within 90 days prior to sample collection had a shorter disease duration than patients with sample collection during a clinically stable disease phase. One patient of each group received a high-efficacious first line treatment (defined as natalizumab, alemtuzumab or ocrelizumab). Of the remaining patients with a follow-up period of at least 2 years, treatment escalation (switch to a more efficacious therapy) was recommended to 15 patients due to ongoing disease activity. Comorbidities in the patient group with relapse included one case of diabetes mellitus type 1 and one case of anemia. In the clinically stable patient group, there was one case of Hashimoto thyroiditis and one case of diabetes mellitus type 1. Bold font indicates statistical significance.
CIS, clinically isolated syndrome; DMT, disease-modifying treatment; EDSS, Expanded Disability Status Scale; IQR, interquartile range; n, number; N/A, not applicable; RRMS, relapsing–remitting multiple sclerosis; SD, standard deviation.
A cranial MRI was available for all patients and a spinal MRI was performed in 16 patients (66.7%). However, two patients did not receive gadolinium. We observed no difference in the cerebral and spinal lesion load between patients with and without relapse [cerebral T2 lesion volume: mean 11.9 ml (SD 12.4) versus 13.2 ml (SD 17.0), p = 0.726; number of spinal lesions: 2.9 (2.7) versus 2.0 (1.9), p = 0.594]. The proportion of patients with CELs was high (90.9% of patients who received gadolinium had cerebral CELs and 46.7% had spinal CELs). The mean number of cerebral CELs was 4.9 (SD 6.9) and did not differ between patients with and without relapse (p = 0.926). Approximately half of the patients had ring-enhancing lesions (54.5%) and three had a tumefactive lesion (12.5%) (Figure 4B, Table 2).
Comparison of MRI characteristics between patients with and without relapse.
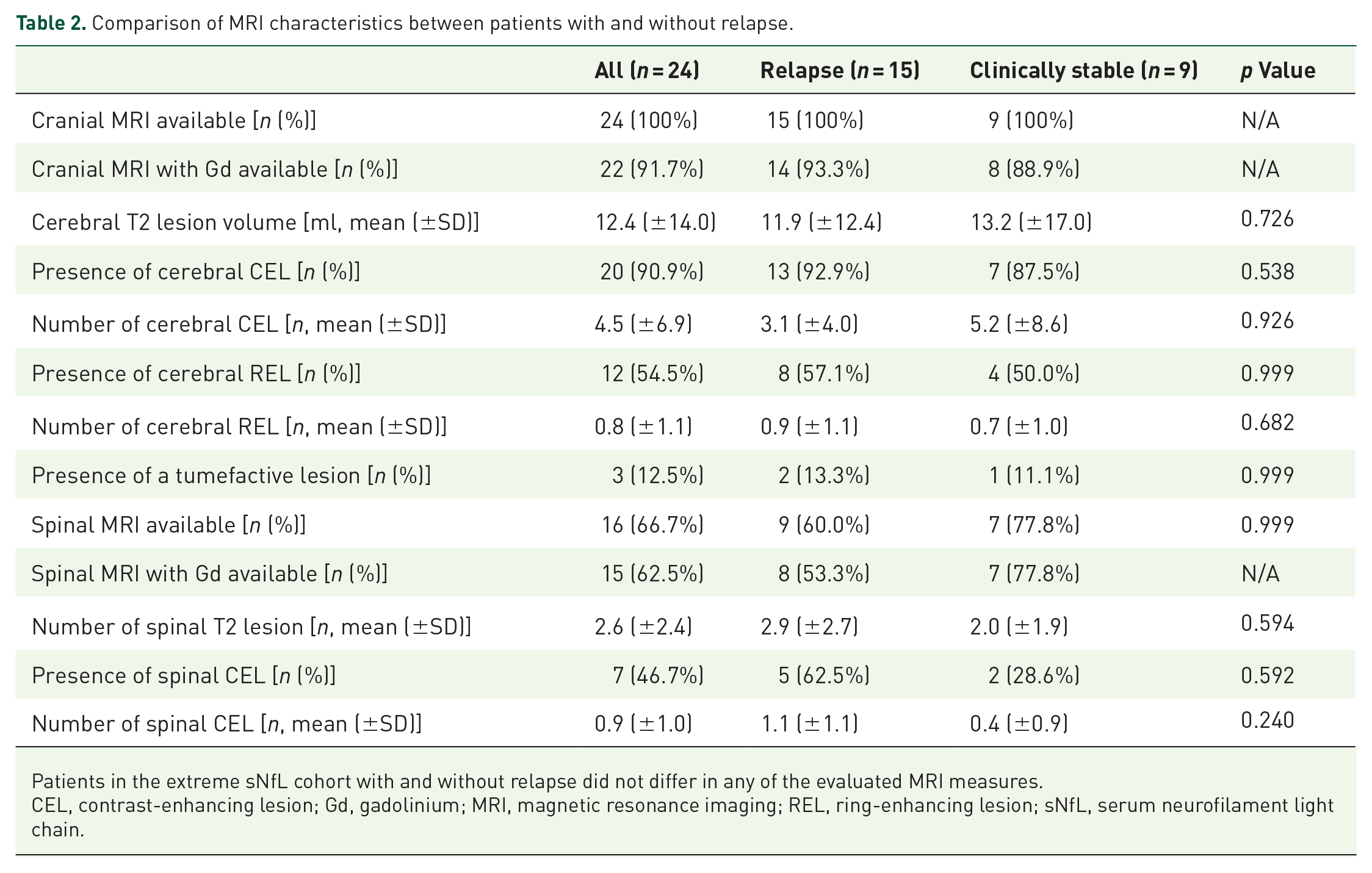
Patients in the extreme sNfL cohort with and without relapse did not differ in any of the evaluated MRI measures.
CEL, contrast-enhancing lesion; Gd, gadolinium; MRI, magnetic resonance imaging; REL, ring-enhancing lesion; sNfL, serum neurofilament light chain.
Discussion
In the here reported patient with a discrepancy between extensive MRI activity and absence of clinical disease activity, we observed an extremely high sNfL value above the 97.5th percentile of our CIS and RRMS cohort. We therefore retrospectively characterized other patients with comparably high sNfL levels with regard to clinical and MRI activity. Interestingly, about one-third of the patients in this extreme NfL cohort also exhibited MRI activity without any accompanying clinical symptoms.
Previous studies have demonstrated that the presence of CELs is associated with an increase in sNfL levels, which peaks in a 3-month window around the occurrence of contrast enhancement,17,18 some have even suggested that sNfL will only be elevated in relapses that are associated with a CEL. 18 In the current study, nearly all of the patients in our extreme NfL cohort demonstrated contrast enhancement, whereas only about two-thirds had corresponding symptoms, which further underlines the contribution of focal inflammatory activity to acutely elevated sNfL levels.
Currently, it is typically recommended to perform clinical examinations every 3–6 months along with yearly MRI of the brain in order to monitor disease activity. The use of spinal cord MRI in addition to brain MRI is not recommended for routine monitoring.19,20 Regular sNfL assessments could complement this established monitoring regimen in order to detect subclinical disease activity in the interval between two MRI examinations. This is also supported by a recent study which demonstrated that regular sNfL level assessments were able to detect disease activity more reliably than routine clinical and MRI examinations in a cohort of alemtuzumab-treated patients with high inflammatory activity. 21
In addition to its potential to increase the sensitivity of disease activity monitoring, our finding that nearly all of the patients with extremely high sNfL levels had CELs further suggests that the simultaneous assessment of sNfL and MRI might be a suitable substitute for gadolinium administration in the future. This is of interest because the recent observation of intracranial gadolinium deposition after contrast-enhanced MRI 22 has led to a restricted administration of gadolinium in routine monitoring, although its clinical significance is still unclear. The use of sNfL as a monitoring tool is also supported by a recent report that found sNfL levels below the 30th percentile to be associated with a low probability of new lesions or CELs on MRI at a 12-month follow-up. 23
Furthermore, our current observations suggest that sNfL levels could especially complement the evaluation of treatment decisions in ambiguous cases such as described for our presented case, who was subsequently treated with the high-efficacious DMT ocrelizumab as a first-line therapy based on individualized risk–benefit stratification. Along with the vast reduction in the focal inflammatory activity in MRI follow-up, the substantial drop in the sNfL concentration to a level comparable to an average RRMS patient was an additional indicator of the excellent treatment response in this patient.
High-efficacious DMTs including natalizumab, alemtuzumab, and ocrelizumab can be applied in patients with highly active RRMS (HAMS) as a first-line therapy, or as an escalation therapy in cases of persisting disease activity upon other DMTs. 24 However, as the definition of HAMS varies and is a matter of ongoing debate, 25 the initiation of a high efficacy DMT like ocrelizumab as a first-line treatment is currently often based on the individual evaluation of the treating physician. Common definitions of HAMS usually demand clinical signs of disease activity (e.g. at least two relapses within the past year, a relapse with incomplete remission associated with new or enlarging MRI lesions, or an EDSS increase of 4 points within 5 years after disease onset).25,26 High MRI activity is usually characterized by a high number of T2 lesions and CELs at disease onset.25,27 The presence of a tumefactive lesion is another indicator of high MRI activity. 9 In our case, as the patient fulfilled all criteria for high MRI activity, it was decided to start a first-line high-efficacy therapy, even in the absence of any new clinical symptoms.
Interestingly, nearly all of the patients in our extreme NfL cohort showed signs of clinical or subclinical disease activity within the 2-year follow-up period and were thus recommended to escalate therapy. Therefore, extremely high sNfL levels could be considered an additional factor for the definition of HAMS. This is supported by the observation that extremely high sNfL levels are associated with an unfavorable disease course indicated by an increased risk of future relapses and EDSS worsening 6 as well as brain and spinal cord atrophy in MRI. 8
However, so far, the implementation of sNfL level assessment has been hampered by the lack of international consensus on clear-cut thresholds leading to distinct clinical decisions. One important step towards a broad application into clinical routine is the recent publication of normative values from a population-based longitudinal study, which demonstrated that sNfL levels were relatively stable in patients under 60 years of age, but considerably increased in a non-linear manner thereafter. Furthermore, the authors observed a marked increase in the variability of sNfL levels with higher age, particularly above 60 years of age. 28 Other studies underline the significance of age-related changes in peripheral NfL levels.6,29 Furthermore, there is increasing evidence for the impact of comorbidities, such as small vessel disease, 30 on sNfL levels, which need to be taken into consideration when interpreting individual NfL levels. To date, it is still difficult to compare NfL values obtained from different laboratories accurately, although international multi-site analytical validation activities of sNfL measurements using SiMoA are currently underway. 31 When compared to our recently published healthy control group of comparable age, 7 sNfL levels in our extreme cohort were about nine times higher. However, the here reported data do not allow the recommendation of a general sNfL cut-off value for ongoing disease activity or poor prognosis.
Of note, the aim of the current study was to illuminate an interesting clinical observation and to illustrate the potential clinical implications of NfL. Due to its retrospective character and the small sample size of the extreme NfL cohort, general conclusions for clinical management cannot be drawn based solely on the data provided here. Unfortunately, spinal MRI was not available for all patients and some patients did not receive gadolinium. Furthermore, three patients were lost to follow-up, which must be considered when interpreting our data.
However, our current observations suggest that sNfL levels above the 97.5th percentile are highly indicative of ongoing disease activity even in patients without a relapse, and should therefore prompt a timely MRI in order to detect subclinical disease activity. Furthermore, sNfL might be able to guide treatment decisions in ambiguous cases.
Footnotes
Acknowledgements
The authors thank Cheryl Ernest for proofreading the manuscript.
Conflict of interest statement
SE, MP, FS, VP, CN, and MP report no conflicts of interest.
FZ has recently received research grants and/or consultation funds from DFG, BMBF, PMSA, MPG, Genzyme, Merck Serono, Roche, Novartis, Sanofi-Aventis, Celgene, ONO, and Octapharma.
SB has received honoraria and compensation for travel from Biogen Idec, Merck Serono, Novartis, Sanofi-Genzyme, and Roche.
FL received consultancy fees from Roche and support with travel cost from Teva Pharma.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Research Council (DFG, CRC-TR-128 to FZ), and the Hertie Foundation (MyLab to SB).