
Abstract
Background:
Peginterferon beta-1a administered every 2 weeks via subcutaneous (SC) injection is approved to treat adult patients with relapsing-remitting multiple sclerosis (RRMS) and relapsing forms of multiple sclerosis (RMS). However, associated injection site reactions (ISRs) can lead to treatment discontinuation. Prior studies with interferon beta-1a reported a lower frequency of ISRs with intramuscular (IM) administration than with SC administration. IM administration of peginterferon beta-1a may therefore represent a useful alternative treatment option.
Methods:
A phase I, open-label, two-period crossover study randomized healthy volunteers to receive a single dose of peginterferon beta-1a 125 mcg administered IM followed by a single 125 mcg dose administered SC after a 28-day washout or vice versa. Blood samples were collected up to 504 h post dose to determine pharmacokinetic (PK) and pharmacodynamic (PD) profiles. The primary endpoint was assessment of bioequivalence based on maximum serum concentration (Cmax) and area under the curve from time zero extrapolated to infinity (AUCinf). Other PK parameters, as well as PD (serum neopterin) and safety profiles, were also evaluated.
Results:
The study enrolled 136 participants. Bioequivalence of IM and SC peginterferon beta-1a was established for both Cmax ([least squares (LS)] mean IM/SC ratio: 1.083 [90% confidence interval (CI), 0.975–1.203]) and AUCinf (LS mean IM/SC ratio: 1.089 [90% CI, 1.020–1.162]). Other PK and PD parameters were similar between administration routes, although moderate to high inter-subject variability was observed for IM and SC. Safety profiles were generally balanced between IM and SC administration. ISRs occurred at a lower frequency with IM [14.4% (95% CI, 8.89–21.56%)] than with SC [32.1% (95% CI, 24.29–40.70%)] administration (p = 0.0005).
Conclusions:
These results demonstrate bioequivalence between peginterferon beta-1a IM and SC and support the consideration of IM injection of peginterferon beta-1a as a viable treatment option in patients with RRMS and RMS.
Keywords
Introduction
Disease-modifying therapies (DMTs) such as interferon beta play an important role in the treatment of multiple sclerosis (MS). Most interferon beta therapies require administration via injection 1–3 times per week and are associated with adverse events (AEs) such as injection site reactions (ISRs; including swelling, erythema, and pain) and flu-like symptoms (FLS).1,2 The occurrence of such AEs and need for frequent injections are common reasons for poor medication adherence or discontinuation of long-term treatment with interferon beta agents. 2 Poor adherence and treatment discontinuation lead to treatment failure, which may be correlated with disease progression and worse patient outcomes. 3
A pegylated form of interferon beta-1a (peginterferon beta-1a; Plegridy®, Biogen, Cambridge, MA, USA) provides a mean half-life (t½) of 78 h in patients with MS, which is approximately two-fold longer than that of other interferon beta-1a agents. 4 The prolonged t½ of peginterferon beta-1a allows for subcutaneous (SC) administration every 2 weeks. Peginterferon beta-1a was approved in the United States (US) and the European Union in 2014 to treat adults with relapsing forms of MS (RMS) and relapsing-remitting MS (RRMS), respectively.5,6 As of 31 March 2020, approximately 57,369 patients have been prescribed SC peginterferon beta-1a, representing 107,764 patient-years of exposure. 7
SC peginterferon beta-1a was formulated to allow a lower dosing frequency than other interferon beta products and to facilitate increased treatment adherence, but many patients receiving the drug experience AEs, such as ISRs and FLS, and may discontinue treatment for these reasons.8–10 Previous studies of interferon beta therapies have reported lower incidence rates of ISRs with intramuscular (IM) administration than with SC administration.10–17 An IM formulation of peginterferon beta-1a may, therefore, offer patients an additional treatment option. Results from a single-dose phase I study in a small group of subjects demonstrated similar pharmacokinetic (PK) and pharmacodynamic (PD) (serum neopterin, induced by interferon beta-1a) profiles for IM and SC formulations of peginterferon beta-1a, but the study was not designed to assess bioequivalence. 18 The current study assessed bioequivalence of IM- and SC-administered peginterferon beta-1a in healthy volunteers.
Methods
Study design
In this open-label, multicenter, two-period crossover study, healthy volunteers who met all eligibility criteria after a 28-day screening period were randomized 1:1 to receive a single dose of IM peginterferon beta-1a 125 mcg followed by a single dose of SC peginterferon beta-1a 125 mcg (IM to SC), or a single dose of SC peginterferon beta-1a 125 mcg followed by a single dose of IM peginterferon beta-1a 125 mcg (SC to IM). In each treatment period, participants checked into the study site on day −1, received a single dose of study treatment on day 1, were discharged from the study site on day 15, and completed outpatient visits on days 17, 19, and 22. A 28-day washout period was incorporated between treatments, and participants received a follow-up phone call 28 (±3) days after receiving their last dose of study treatment. In addition to receiving study treatment, all participants also received naproxen sodium or acetaminophen ⩽1 h pre-dose and ⩽24 h post dose as prophylactic treatment of FLS.
During each treatment period, blood samples for PK and PD assessments were collected ⩽2 h pre-dose and 3, 6, 12, 24, 32, 40, 48, 72, 96, 120, 144, 168, 192, 216, 240, 264, 288, 312, 336, 384, 432, and 504 h post dose. Treatment safety was assessed during days 1–15 and at all subsequent study visits by noting the occurrence of AEs and serious AEs (SAEs), clinically significant changes to laboratory values, and vital signs. Injection sites were monitored for ISRs immediately after dosing (±5 min) and at 0.5, 2, and 4 h (±15 min) post dose. ISRs were defined as injection site pain (tenderness to digital pressure), local temperature, itching, redness, edema, and induration/infiltration.
Participants
Men and nonpregnant women were eligible for inclusion if they were 18–55 years old and had a body mass index of 18.0–30.0 kg/m2, a body weight ⩾45.0 kg, and a systolic blood pressure ⩽150 mmHg and ⩾90 mmHg at screening and study site check-in. All participants were determined to be in good health by the investigator based on medical history and screening evaluations. Individuals were ineligible for the study if they had a history of clinically significant major disease; tested positive for bacterial, fungal, or viral infections; or had a history of serious infection (e.g. human immunodeficiency virus). Participants were not permitted to use any prescription drug or nutraceutical ⩽14 days prior to check-in or to consume alcohol or caffeine or exercise vigorously ⩽48 h prior to check-in. The Midlands Independent Review Board at each study site approved the study protocol, and the study was conducted in accordance with the International Council for Harmonisation Guidelines on Good Clinical Practice and the World Medical Association Declaration of Helsinki. All participants signed and dated informed consent forms prior to any evaluations for study eligibility.
Study objectives and endpoints
The primary study objective was assessment of the bioequivalence of SC and IM administration of peginterferon beta-1a in healthy volunteers. To evaluate this, the primary endpoints were set as maximum serum concentration (Cmax) and area under the curve (AUC) from time zero to infinity (AUCinf). Secondary objectives were to estimate other PK parameters and the safety and tolerability of peginterferon beta-1a administered via SC or IM injection. The key secondary endpoint was AUC from time zero to the last measurable concentration (AUC0–last). Other secondary endpoints included AUC from time zero to 336 h post dose (AUC0–336), AUC from time zero to 504 h post dose (AUC0–504), AUCinf, time to maximum observed plasma concentration, t½, apparent total body clearance, and apparent volume of distribution. Safety endpoints included the incidence of AEs and SAEs. As an exploratory study objective and endpoint, PD parameters based on serum neopterin levels were assessed, including baseline concentration, EAUC0–336, EAUC0–504, maximum effect (Epeak), and time to reach Epeak (ETmax). All PK and PD parameters were obtained from noncompartmental analysis using Phoenix WinNonlin (Version 8.1; Certara USA, Inc., Princeton, NJ, USA).
Statistical analysis
The sample size was calculated using Shuirmann’s two one-sided t tests of equivalence between the SC and IM routes of peginterferon beta-1a administration for a crossover design using the natural log-transformed Cmax data. The square root of the mean square error for within volunteer variability for log(Cmax) was assumed to be 0.5 based on data from previous studies of peginterferon beta-1a. 19 The 54 evaluable volunteers per treatment sequence provided 80% power to establish the bioequivalence of the two routes within the range of 80%–125% for Cmax, with a significance level of 0.05 and an expected ratio of 1.05 for the Cmax values between the two routes. Under the assumption that the estimated SD of the difference between paired measurements was smaller for log(AUCinf) than for log(Cmax), the sample size provided >80% power for the AUCinf endpoint.
Bioequivalence was evaluated in the PK population, which included all randomized participants who received both doses of study treatment and had sufficient PK measurements to allow calculation of PK parameters. Bioequivalence was established if the 90% confidence intervals (CIs) of the least squares (LS) mean ratio of the IM and SC treatment routes were within 80–125% for both Cmax and AUCinf. A two-treatment, two-period crossover analysis of variance (ANOVA) model was used to estimate LS mean ratios and their CIs. Descriptive statistics were used to analyze all other PK, PD, and safety outcomes. McNemar’s test was used to assess the difference in ISR and FLS incidence between the two administration routes. The PD population included all randomized participants who received at least one dose of study treatment and had at least one PD measurement after baseline. The safety population included all randomized participants who received at least one dose of study treatment. All analyses were conducted using SAS software (version 9.4; SAS Institute Cary, NC, USA).
Results
Participants
The study was conducted between December 2018 and May 2019 at two US sites. Healthy volunteers (N = 136) were randomized to receive peginterferon beta-1a 125 mcg administered as a single SC dose followed by a single IM dose (n = 68) or vice versa (n = 68) (Figure 1). All randomized participants received treatment during treatment period 1, but six discontinued prior to receiving treatment in treatment period 2 and were excluded from the PK population (n = 130). Reasons for discontinuation included AEs (n = 3; anemia, tachycardia, and increased blood creatine phosphokinase), physician decision (n = 1), and noncompliance (n = 2). An additional five participants discontinued the study (i.e. did not complete all follow-up visits) after receiving treatment in treatment period 2, which was attributed to loss to follow up (n = 1) and withdrawal of consent (n = 4). Nearly all participants received naproxen sodium for prophylactic treatment of FLS. Only three participants received acetaminophen for prophylactic treatment of FLS at any time point. During the study, six participants used disallowed medications, 14 used nondrug treatments while receiving peginterferon beta-1a SC, and 10 used nondrug treatments while receiving peginterferon beta-1a IM, primarily to treat AEs. Non-drug treatments included heat therapy, cooling therapy, and constipation prophylaxis. However, none of these treatments was considered by the investigator to affect the study results. Demographics and baseline characteristics were generally similar in the two groups (Table 1). A majority of participants were 40–55 years old (57.4%), male (55.1%), and Black/African American (51.5%) (Table 1).
Participant demographics and baseline characteristics (safety population).

BMI, body mass index; IM, intramuscular; SC, subcutaneous; SD, standard deviation.
p values are based on a Chi-square test for categorical variables and a two-sample t test for continuous variables.

Study flow diagram.
Pharmacokinetic
The PK profiles for peginterferon beta-1a over time were similar for the SC and IM administration routes (Figure 2). With both IM and SC administration, Cmax was observed a median of 40.0 h post dose, after which point serum concentrations declined monophasically and produced a median t½ of 75.3 h (range, 26.3–233.3 h) for IM administration and 90.9 h (range, 29.1–239.9 h) for SC administration. Results for the primary and secondary PK endpoints are detailed in Table 2. The geometric mean Cmax values were 1.31 ng/ml with IM administration and 1.21 ng/ml with SC administration, and the geometric mean AUCinf values were 168.46 h × ng/ml with IM administration and 156.64 h × ng/ml with SC administration. With both administration routes, PK parameters showed moderate to high variability between participants, with geometric coefficient of variation (CV%) values ranging from 48.6% to 60.0% (IM) and from 52.6% to 78.0% (SC).
Pharmacokinetic parameters of peginterferon beta-1a following IM and SC administration (PK population).

AUC, area under the curve; AUC0–336, AUC from time zero to 336 h post dose; AUC0–504, AUC from time zero to 504 h post dose; AUC0–last, AUC from time zero to the last measurable concentration; AUCinf, AUC from time zero extrapolated to infinity; CL/F, apparent total plasma clearance; Cmax, maximum serum concentration; IM, intramuscular; PK, pharmacokinetic; SC, subcutaneous; t½, terminal elimination half-life; Tmax, time to maximum plasma concentration; λz, terminal elimination rate constant.

Serum concentration profiles for peginterferon beta-1a following single 125-mcg SC and IM doses (PK population).
Bioequivalence
The LS mean ratios of IM to SC for Cmax and AUCinf and the associated 90% CIs were within the 0.80–1.25 range of bioequivalence, at 1.083 (90% CI, 0.975–1.203) for Cmax and 1.089 (90% CI, 1.020–1.162) for AUCinf. In addition, the LS mean ratio for AUC0–last and the associated 90% CI was 1.130 (90% CI, 1.058–1.207), supporting the primary endpoint findings of bioequivalence.
Pharmacodynamic
IM and SC administration of peginterferon beta-1a had similar peak neopterin concentrations, effect AUCs, and time to maximum neopterin concentration (Table 3). Overall systemic neopterin levels were similar between administration routes. With both IM and SC routes, serum neopterin concentrations peaked approximately 2 days post dose and returned to near-baseline values within 312 h (13 days) post dose (Figure 3). The CV% values for PD parameters were 34.1–40.5% with IM administration and 33.8–44.2% with SC administration, demonstrating moderate variability among participants.
Pharmacodynamic parameters of peginterferon beta-1a following IM and SC administration (PD population).
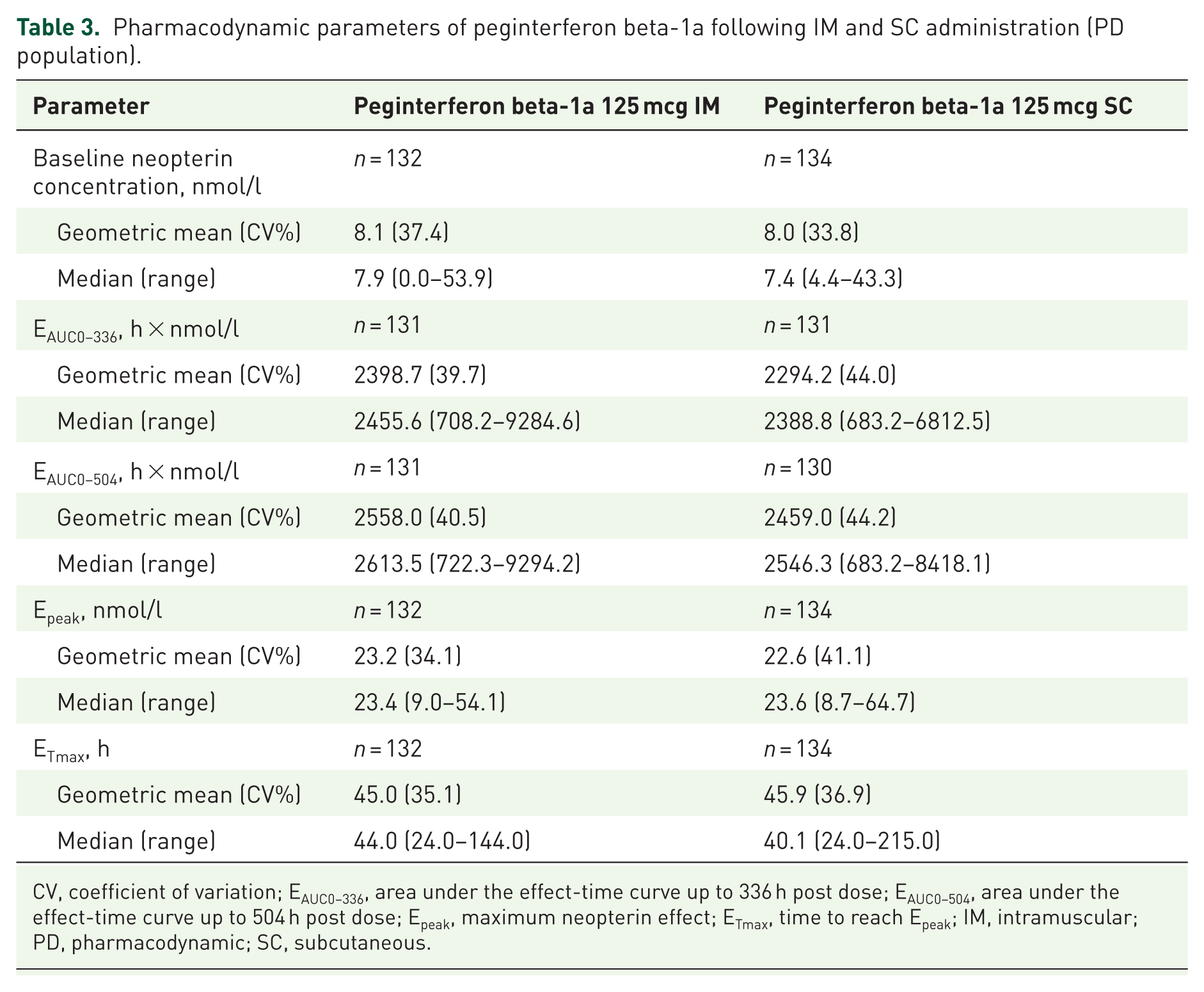
CV, coefficient of variation; EAUC0–336, area under the effect-time curve up to 336 h post dose; EAUC0–504, area under the effect-time curve up to 504 h post dose; Epeak, maximum neopterin effect; ETmax, time to reach Epeak; IM, intramuscular; PD, pharmacodynamic; SC, subcutaneous.

Serum concentration profiles for neopterin following single 125-mcg SC and IM doses (PD population).
Safety
Treatment-emergent adverse events (TEAEs) were reported for 87 of 132 participants who received peginterferon beta-1a IM (65.9%) and 92 of 134 participants who received peginterferon beta-1a SC (68.7%). The most commonly reported TEAEs were headache (35.6% and 41.0% in the IM and SC groups, respectively), chills (35.6% and 26.9%, respectively), pain (22.0% and 14.2%, respectively), injection site pain (11.4% and 14.9%, respectively), injection site erythema (2.3% and 25.4%, respectively), and pyrexia (9.8% and 9.0%, respectively). All TEAEs were mild (62.9% and 64.9% in the IM and SC groups, respectively) or moderate (3.0% and 3.7%, respectively) in severity.
TEAEs considered by the investigator to be related to study treatment were reported for 81 of 132 participants (61.4%) after IM dosing and 89 of 134 participants (66.4%) after SC dosing (Table 4). Of the 132 participants, 2 (1.5%) discontinued treatment after the IM dose, 1 due to anemia and the other due to tachycardia, and 1 of 134 participants (0.7%) discontinued after the SC dose due to increased blood creatinine phosphokinase. All AEs were considered resolved by the end of the study. No SAEs and no deaths were reported.
TEAEs considered related to study treatment (safety population).

Events were coded using MedDRA version 21.1. A participant was counted only once within each preferred term and treatment-emergent period.
The following preferred terms were reported as ISRs: injection site edema, injection site erythema, injection site induration, injection site pain, injection site pruritus, and injection site warmth.
IM, intramuscular; ISR, injection site reaction; SC, subcutaneous; TEAE, treatment-emergent adverse event.
The IM dose was associated with a significantly lower frequency of ISR TEAEs than the SC dose. Treatment-emergent ISRs, defined as injection site pain (tenderness to digital pressure), local temperature, itching, redness, edema, and induration/infiltration, were reported for 14.4% (95% CI, 8.89–21.56%) of IM participants and 32.1% (95% CI, 24.29–40.70%) of SC participants (p = 0.0005). Injection site pain and injection site erythema were the most frequently reported ISRs, and, with two exceptions, all such reactions were mild and considered related to treatment. One instance of injection site pain was considered unrelated to treatment, and one instance of injection site erythema was moderate in severity. FLS, including chills, pain, pyrexia, influenza-like illness, myalgia, and musculoskeletal pain, were reported for 65 participants (49.2%; 95% CI, 40.44–58.08%) after the IM dose and for 53 participants (39.6%; 95% CI, 31.22–48.36%) after the SC dose (p = 0.0474). In participants who received IM followed by SC dosing and vice versa, the rates of ISRs (38.2% versus 39.7%) and FLS (55.9% versus 64.7%) were comparable between administration routes (Supplemental Table S1).
No trends or clinically significant changes were observed in clinical laboratory values such as hematology, blood chemistry (including alanine aminotransferase and aspartate aminotransferase), and urinalysis. Clinically relevant changes in vital signs occurred at similar rates with both injection routes and included decreased pulse rate (31.1% and 29.1% in IM-dosed and SC-dosed participants, respectively), increased pulse rate (20.5% and 20.1%, respectively), change in body temperature (13.6% and 13.4%, respectively), decrease in diastolic blood pressure (BP) (8.3% and 9.7%, respectively), and decrease in systolic BP (7.6% and 6.7%, respectively). However, none of the abnormal vital signs were associated with any clinical symptoms.
Discussion
The results of this study support the bioequivalence of IM and SC routes of administration for peginterferon beta-1a. The 90% CIs of the IM/SC ratios for the primary endpoints of Cmax and AUCinf and for the key secondary endpoint of AUC0–last were within the 0.80–1.25 range established by the US Food and Drug Administration as demonstrating bioequivalence. 20 Consistent with these findings, other PK and PD parameters were similar between administration routes. These results are also consistent with a previous phase I single-dose study comparing SC and IM formulations of peginterferon beta-1a with IM interferon beta-1a, in which PK parameters were similar between the SC and IM administration routes for peginterferon beta-1a. 18
The safety results in this study were generally balanced between the IM and SC dosing routes, although a significantly smaller proportion of participants reported ISRs after the IM dose (14.4%) than after the SC dose (32.1%) (p = 0.0005). This is consistent with previous reports of lower ISR incidence with IM versus SC injection. In a systematic literature review of cutaneous AEs associated with injectable DMTs, Balak et al. identified reports of ISRs in 2–33% of patients treated with IM interferon beta-1a versus 13–89% of patients treated with SC interferon beta-1a. 14 Similarly, a large observational study of patients treated with an injectable therapy reported ISRs for 13.4% of patients who received IM interferon beta-1a compared with 67.9% who received SC interferon beta-1a and 57.7% who received SC interferon beta-1b. 13
Safety results also indicated that a larger proportion of patients reported FLS after the IM dose (49.2%) than after the SC dose (39.6%) (p = 0.0474). This difference in the frequency of FLS between the two administration routes is of borderline significance and of a lesser magnitude than the difference in ISR frequency between administration routes (p = 0.0005). The incidence of FLS with IM peginterferon beta-1a administration in this study is comparable with previous studies of IM interferon beta-1a,21,22 which reported incidence rates of FLS as high as 61%. 21 Additionally, in studies comparing IM interferon beta-1a and SC interferon beta-1b 12 and IM interferon beta-1a and SC interferon beta-1a, 15 no significant differences in the incidence of FLS were reported between the IM and SC routes of administration. As discussed below, adherence rates have been shown to be higher with IM interferon beta than with SC administration.13,17 Thus, FLS associated with IM peginterferon beta-1a, which is administered every 2 weeks rather than weekly, are not expected to negatively impact treatment adherence relative to FLS associated with SC administration.
Treatment adherence is essential for patients to receive the maximal benefit from any DMT, and interferon beta-1a adherence rates have been reported to range from 41% to 88%.16,17,23 Adherence rates appear to be higher with IM than with SC administration. In a large observational study, patients who had initiated IM interferon beta-1a were more likely to remain on this therapy at 1 year than those who had initiated SC interferon beta-1a or -1b. 13 A post-marketing study found that patients administered interferon beta-1a via IM injection were more likely to adhere to treatment over 2 years than those administered SC interferon beta-1a 22 or 44 mcg (87.5% versus 77.8–80.0%). 17 In the Global Adherence Project, adherence rates were significantly higher with IM interferon beta-1a than with SC interferon beta-1a 22 or 44 mcg (85% versus 73–78%; p < 0.01). 16 DMT adherence has been associated with reduced likelihood of relapse as well as reduced healthcare resource utilization compared with nonadherence. 24 The reduction in ISRs with IM versus SC administration, along with the lower frequency of peginterferon beta-1a dosing compared with other interferon beta therapies, may therefore promote treatment adherence and contribute to improved patient outcomes.
Although this study was conducted in healthy volunteers rather than patients with RRMS, the results in the latter group are expected to be equivalent based on previous trials, which reported that PK profiles for SC peginterferon beta-1a 125 mcg are similar between healthy volunteers and patients with RRMS.18,25 Bioequivalence between IM and SC administration routes is similarly expected to translate to patients with RRMS. However, additional studies are needed to confirm the advantageous safety profile of IM versus SC administration with respect to ISRs in patients with RRMS receiving ongoing treatment with peginterferon beta-1a.
Conclusion
The results of this study support the IM administration of peginterferon beta-1a as an alternative option to SC administration for patients with RMS or RRMS. IM peginterferon beta-1a appears to be associated with a reduced rate of ISRs, which are a key factor in treatment nonadherence and discontinuation among patients who receive injectable DMTs. Although further studies are needed to confirm these findings in patients with RRMS and extended treatment exposure, peginterferon beta-1a treatment via IM injection may support increased treatment adherence, and, thus, improved patient outcomes.
Supplemental Material
sj-pdf-1-tan-10.1177_1756286420975227 – Supplemental material for Bioequivalence of intramuscular and subcutaneous peginterferon beta-1a: results of a phase I, open-label crossover study in healthy volunteers
Supplemental material, sj-pdf-1-tan-10.1177_1756286420975227 for Bioequivalence of intramuscular and subcutaneous peginterferon beta-1a: results of a phase I, open-label crossover study in healthy volunteers by Yuan Zhao, Kun Chen, Nancy Ramia, Sangeeta Sahu, Achint Kumar, Maria L. Naylor, Li Zhu, Himanshu Naik and Cherié L. Butts in Therapeutic Advances in Neurological Disorders
Footnotes
Acknowledgements
The authors thank the study site personnel and participants for their contributions to the study. The authors were assisted in the preparation of the manuscript by Autumn Kelly, MA, Alexandra D’Agostino, PhD, and Joshua Safran (Ashfield Healthcare Communications, Middletown, CT, USA). Writing and editorial support were funded by the study sponsor. All authors were involved in reviewing the manuscript critically for important intellectual content. The authors provided final approval of all content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by Biogen.
Conflict of interest statement
YZ, NR, SS, AK, MLN, LZ, HN, and CLB are employees of and may hold stock and/or stock options in Biogen. KC was an employee of Biogen at the time of these analyses and may hold stock and/or stock options in Biogen.
Data sharing
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.