
Abstract
Background:
Disease-modifying therapies (DMTs) for multiple sclerosis (MS) are approved for the treatment of disease activity and are effective in reducing relapses and new magnetic resonance imaging (MRI) lesions. However, disease activity generally subsides with time, and age-dependent changes in DMT efficacy are not well-established. We aimed to investigate whether age impacts the efficacy of DMTs in treating disease activity in patients with relapsing–remitting MS (RRMS).
Methods:
DMT efficacy related to age was assessed through a meta-analysis of clinical trials that evaluated the efficacy of DMTs in RRMS patients as measured by reductions in the annualized relapse rate (ARR), new T2 lesions, and gadolinium-enhanced lesions on MRI. Using the mean baseline patient age from each trial, a weighted linear regression was fitted to determine whether age was associated with treatment efficacy on a group level.
Results:
Group-level data from a total of 28,082 patients from 26 trials of 14 different DMTs were included in the meta-analysis. There were no statistically significant associations between age and reductions in ARR, new T2 lesions, and gadolinium-enhanced lesions of the treatment group compared with placebo.
Conclusion:
DMTs for RRMS show efficacy in treating disease activity independent of age as demonstrated by group-level data from DMT clinical trials. Nevertheless, clinical trials select for patients with baseline disease activity regardless of age, thereby not representing real-world patients with RRMS, where disease activity declines with age.
Introduction
Multiple sclerosis (MS) is a chronic immune-mediated inflammatory disorder of the central nervous system characterized by demyelination and neurodegeneration. 1 Two broad categories divide the disease into relapsing–remitting (RRMS) and progressive (PMS) phenotypes. RRMS is characterized by attacks of new or worsening neurological deficits with or without return to baseline while PMS commonly presents with progressive worsening of neurologic disability. 2 While there is currently no cure for the disease, over a dozen disease-modifying therapies (DMTs) are approved by regulatory agencies for the treatment of disease activity primarily based on reducing relapses and formation of new magnetic resonance imaging (MRI) lesions.
The majority of DMTs treat disease activity by depleting inflammatory cells, preventing their migration into the central nervous system and mitigating formation of new focal white matter lesions. This efficacy for treating disease activity has prompted trials of many of the same DMTs in people with PMS, but most failed to halt disease progression, likely due to the late intrathecal inflammatory process occurring in the setting of an intact blood–brain barrier that is more difficult to target.3–6
Age appears to be a strong predictor of MS disease activity. With increasing age, relapse frequency and new inflammatory MRI lesions decline;7–9 however, there is scarce evidence on age-dependent changes in DMT efficacy in treating disease activity. The goal of this study was to perform a meta-analysis of all blinded, randomized clinical trials of DMTs for RRMS to examine whether reductions in disease activity on a group level as measured by annualized relapse rate (ARR), new T2 lesions, and gadolinium-enhanced lesions are dependent on age. We hypothesized that age will negatively correlate with reductions in ARR, new T2 lesions, and gadolinium-enhanced lesions in people with RRMS. Establishing an association between aging and DMT efficacy will help predict treatment response in patients and inform treatment decisions given the inherent risks of adverse effects, particularly in elderly patients with MS, and the high cost of DMTs.
Methods
Search strategy and selection criteria
We searched PubMed from the database inception to May 2020 for clinical trials of DMTs for the treatment of RRMS. The “clinical trial” filter in PubMed was applied and key words for screening included “multiple sclerosis” in conjunction with either “interferon” (n = 908), “glatiramer acetate” (n = 211), “dimethyl fumarate” (n = 35), “fingolimod” (n = 89), “siponimod” (n = 5), “ozanimod” (n = 6), “teriflunomide” (n = 25), “cladribine” (n = 37), “alemtuzumab” (n = 34), “mitoxantrone” (n = 54), “natalizumab” (n = 107), “rituximab” (n = 22), “ocrelizumab” (n = 10), “daclizumab” (n = 36), and “laquinimod” (n = 13). Eligibility criteria included blinded randomized phase III clinical trials in adult patients with RRMS, intervention with any of the aforementioned pharmacological agents for at least 1 year, the inclusion of a placebo control arm or interferon beta as the active comparator arm, availability of baseline patient characteristics including mean age, and outcome measurements including ARR, new T2 lesions, and/or gadolinium-enhanced lesions. Studies were excluded if more than 10% of the trial population consisted of patients with PMS. Full texts of all articles were obtained based on the assessments of titles and abstracts, and additional information from supplementary data was gathered when applicable. The screening process is depicted in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (Figure 1). 10
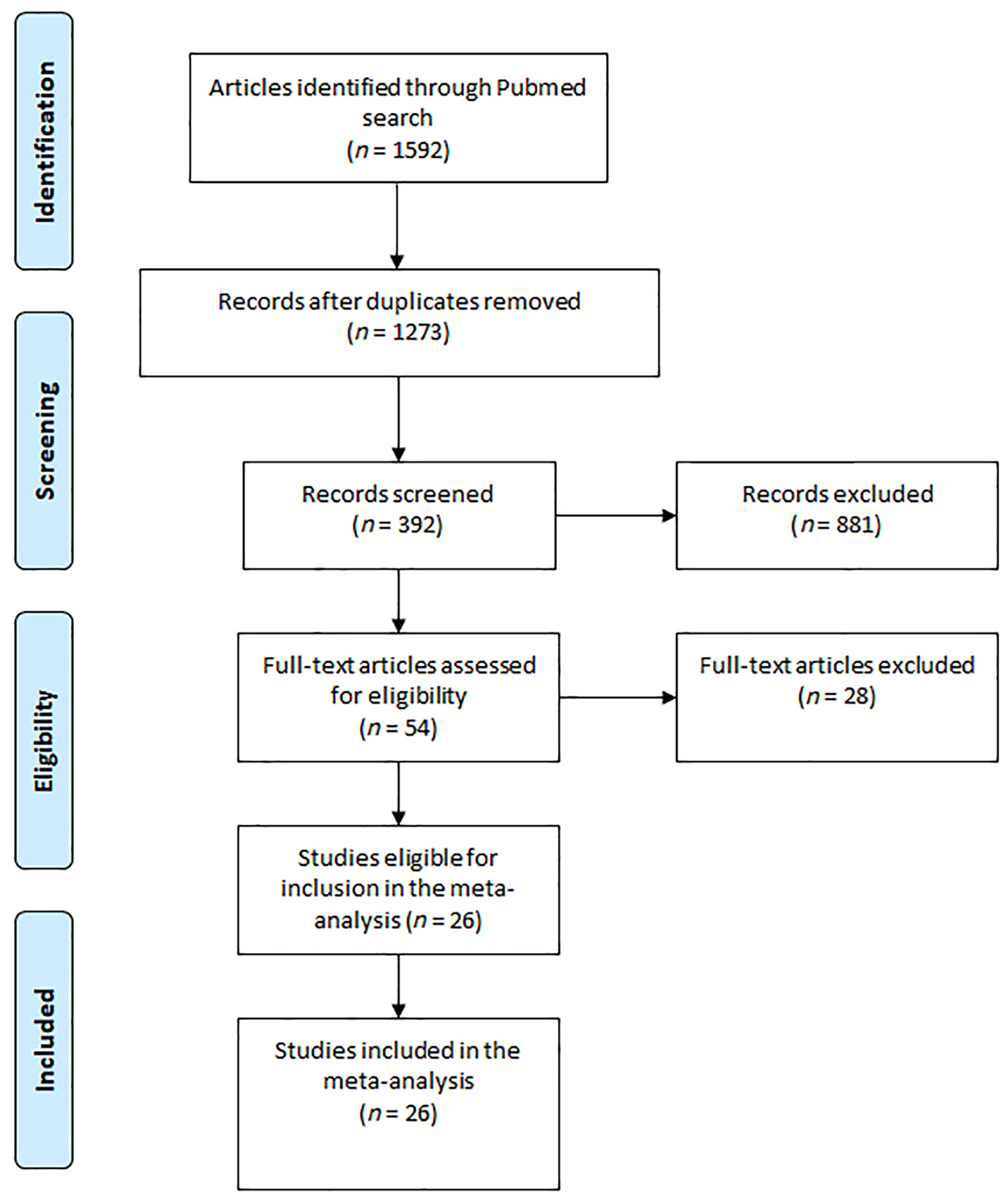
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram illustrating search strategy and study inclusion in the meta-analysis.
Data analysis
Extracted data included clinical trial characteristics (name of trial, year of publication, interventions, study duration, sample size), mean age of trial subjects, and outcome measures (ARR, new T2 lesions, and gadolinium-enhanced lesions). When mean values were not available, the reported median values were used. The analytic methods were adopted from a meta-analysis by Weideman et al. 11 Data analysis was conducted in statistical software R v.3.3.1 (RStudio v.1.0).12,13
Calculating ARR, new T2 lesions, and gadolinium-enhanced lesions reduction
Drug efficacy was measured by percent reduction in ARR, new T2 lesions, and gadolinium-enhanced lesions of the drug group against the placebo group. Using ARR as the example, this was calculated as

where ARRdrug represents the ARR of the drug group and ARRplacebo represents the ARR of the placebo group at the end of the trial. The ratio of ARRdrug to ARRplacebo can be viewed as the number of relapses occurring on treatment to the number of relapses occurring while on placebo. Thus, ARR reduction is roughly equivalent to the relative risk reduction in relapse occurrences.
Assigning trial weight
A weighted regression was used to account for the varying sample size and duration of clinical trials. Using methods from previous meta-analyses,14,15 the estimated weight of each trial was calculated using the following formula:

where n is the trial sample size and D is the trial duration in years. Therefore, trials enrolling more subjects and lasting longer will carry a larger weight. For trials with two treatment arms and one control arm, each pair of treatment versus control arms was considered an independent trial. To avoid double counting patients and falsely inflating the trial weight, the placebo group size used in calculating each trial sample size was divided by the number of treatment arms.
Estimating efficacy against placebo in active comparator trials
For trials not using placebo, various interferon beta formulations were used as the active comparator. To estimate drug efficacy against placebo in active comparator trials, we factored in an estimated additional efficacy of interferon beta preparations against placebo on top of the known efficacy of the drug against the interferon beta control. Using ARR as the example, the ARR reduction of the drug versus placebo in active comparator studies using interferon beta can be thought of as

This represents the additional ARR reduction that a drug that was compared with interferon beta (IFN-β) would have against placebo by factoring in the ARR reduction that interferon beta preparations as a group have against placebo. By rearranging the equation for ARR reduction, it holds true that

An estimated single average efficacy of interferon beta versus placebo was determined by taking a weighted average for each interferon beta preparation in their respective trials against placebo.
Simple weighted regression
To assess the relationship between age and ARR, new T2 lesions, and gadolinium-enhanced lesions reduction, we fitted a simple weighted regression to all drug trials as follows using ARR as the example

The parameter estimates of (β) [standard error (SE) and R2] are reported for each model, the subscripts
Results
There were 26 trials of 14 DMTs enrolling 28,082 subjects published between 1995 and 2019 that fulfilled inclusion criteria for the meta-analysis. ARR or a relapse-related metric was the primary or coprimary outcome in all trials except in the high-dose interferon beta-1a trial, which reported time to onset of sustained disability worsening as the primary outcome. 16 New T2 lesions were reported as an outcome in 18 trials and gadolinium-enhanced lesions were reported in 19 trials. Each trial was assigned a weight dependent on the trial sample size and duration. Eleven active comparator trials compared the study drug with interferon beta instead of placebo. Six trials compared efficacy of interferon beta with placebo. Individual trial characteristics are shown in Table 1. For active comparator trials, the efficacy of the drug against placebo was estimated by combining the added estimated ARR, new T2 lesions, or gadolinium-enhanced lesion reduction of interferon beta against placebo with the ARR, new T2 lesions, or gadolinium-enhanced lesion reduction of drug to interferon beta.
Characteristics of clinical trial included in the meta-analysis.

Age and ARR
The mean age of patients in all trials ranged from 33.1 years in the CARE-MS I trial
17
to 40.4 years in the FREEDOMS II trial.
18
We modeled the linear regression for 26 trials as a function of age, and there was no significant association between mean age and ARR reduction [

Efficacy of disease-modifying therapies against placebo on annualized relapse rate reduction (A), new T2 lesion reduction (B), and gadolinium-enhanced lesion reduction (C) as a function of mean baseline age in patients with relapsing–remitting multiple sclerosis. The corresponding trial indices are listed in Table 1. The gray area indicates 95% confidence interval estimates. The coefficient of determination (R2) and p-values are shown in the respective plots. The diameter of each circle is proportional to the weight of the corresponding clinical trial in the meta-analysis.
Age and new T2 lesions
The mean age of patients in all trials ranged from 35.4 years in the SUNBEAM trial
19
to 40.4 years in the FREEDOMS II trial.
18
We modeled the linear regression for 18 trials as a function of age, and there was no significant association between mean age and new T2 lesion reduction [
Age and gadolinium-enhanced lesions
The mean age of patients in all trials ranged from 35.4 years in the SUNBEAM trial
19
to 40.4 years in the FREEDOMS II trial.
18
We modeled the linear regression for 19 trials as a function of age, and there was no significant association between mean age and gadolinium-enhanced lesion reduction [
Discussion
Our meta-analysis found no significant association between age and DMT efficacy on disease activity as measured by reduction in ARR, new T2 lesions, or gadolinium-enhanced lesion in clinical trials of DMTs for RRMS. We chose to study ARR reduction since approvals of DMTs are mainly based on this outcome measure. In addition, MRI lesions are a surrogate of ARR and are correlated with disease activity. 20 In almost all RRMS trials, ARR or a similar relapse-related metric was used as the primary outcome, but studies have not examined whether ARR reduction is age-dependent. Seven subgroup analyses of MS drug trials studied whether there were differences in efficacy between younger versus older patients.21–26 In each of these subgroup analyses patients were separated into two age groups of above and below age 40 years (with a cutoff of 38 for one study). These results showed that patients in the younger age group had better treatment of disease activity, but due to small differences in treatment effect, these subgroup analyses were not powered to detect statistical significance of the effect differences between the two age groups. A meta-analysis of six randomized controlled trials of 6693 patients with RRMS that reported subgroup analysis showed that patients in the <40 age group achieved significantly higher reduction of disease activity than those in the ⩾40 age group. 27 Although subgroup analyses have shown that DMTs have greater efficacy in younger patients, the studies do not describe a correlation between age and efficacy, thus limiting strategies to predict the average efficacy of DMTs based on age.
Analysis of data for the study was based on methods described in the meta-analysis by Weideman et al., which evaluated the age-dependent efficacy of DMTs in trials of all MS subtypes using disease progression as the outcome. 11 The original study found a significant age-related decline in inhibition of disease progression using a weighted regression of percent inhibition of disability progression versus mean trial age. The results support observations that mechanisms driving disease progression evolve with age. While the mechanisms driving disease activity do not change with age, disease activity as the substrate for DMTs diminishes with age, which is not adequately captured in the clinical trial population that selects for patients with baseline active disease regardless of age.
Several limitations are inherent in our meta-analysis. The most significant limitation is the inaccessibility of individual-level data from MS clinical trials, which restricts us to using the mean patient age as reported in each trial and masks any age-related changes in DMT efficacy within each trial. Another limitation is the narrow range of mean age of trials for RRMS spanning from 33 to 40 years, leaving out aggregate data for younger and older patients. In addition, we assume that class differences between DMTs exhibit similar age-related changes in efficacy and that different interferon beta preparations are equivalent when preparing the regression of drug to placebo for active comparator trials. Finally, variations among clinical trials, including trial design and changes in trial population, limit accurate assessment of comparative drug efficacies. 28
Considering that clinical trials of DMTs for RRMS exclude patients over age 55, there are no data to suggest DMTs are either effective or safe in the elderly, especially in those without disease activity. Instead, there is growing evidence showing increased prevalence of comorbidities in the aging MS population as well as greater susceptibility to treatment-related side effects such as infections and lymphopenia.29–31 In addition, evidence suggests that relapses are rare in people with MS over age 60, 31 and continuing DMTs have lower projected benefits in the elderly. 32 Despite growing concerns regarding safety and efficacy in using DMTs in the elderly, their continued use in this population may be the result of the perceived notion that disease inactivity is due to the effect of DMTs rather than the natural disease course with aging. Further contributing to the hesitation to discontinue DMT is the concern of rebound disease activity. The currently ongoing DISCOMS trial is expected to provide data on the safety of DMT discontinuation for stable MS patients over age 55. 33
The age gap between the MS clinical trial population and real-world population continues to widen with growing numbers of elderly people with MS, where the average age demographics for people with MS in North America are now cited to span the 50s to 60s.34,35 This makes clinical trial results less applicable to the general MS population in terms of age and age-related changes in disease activity. As the probability of active disease declines with age and susceptibility to side effects increases, the risks versus benefits of using DMTs in the elderly should be reexamined. Current data from clinical trials of DMTs are not suitable for establishing an age-dependent relationship with efficacy due to selection for patients with active disease. Further dedicated studies with a real-world population on the relationship between DMT efficacy and age and the safety of DMT discontinuation are still needed to address the benefits and risks of using DMTs in aging MS patients.
Footnotes
Acknowledgements
We wish to thank Weideman et al. for providing the R code for conducting the meta-analysis in the supplementary materials of their publication. 11 The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does the mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Author contributions
YZ, ASa, ASh, BB, and OS conceived the study design. YZ and NGC performed data collection for the meta-analysis and ASa and PK analyzed the data. The first draft was written by YZ with input from all authors. All authors contributed to the review and approval of the final manuscript version for submission.
Conflict of interest statement
YZ, NGC, ASa, WC, MW, PK, BB declare no competing interests related to this study. ASh is currently funded through a Clinician Scientist Development Award by the National Multiple Sclerosis Society and a Physician Scientist Training Program Award by the University of Nebraska Medical Center. GC has participated on data-monitoring and safety-monitoring boards for Avexis Pharmaceuticals, Biolinerx, Brainstorm Cell Therapeutics, CSL Behring, Galmed Pharmaceuticals, Horizon Pharmaceuticals, Hisun Pharmaceuticals, Mapi Pharmaceuticals, Merck, Merck/Pfizer, Opko Biologics, Neurim, Novartis, Ophazyme, Sanofi-Aventis, Reata Pharmaceuticals, Receptos/Celgene, Teva pharmaceuticals, Vivus, NHLBI (Protocol Review Committee), NICHD (OPRU oversight committee); participated in consulting or advisory boards for Biogen, Click Therapeutics, Genzyme, Genentech, Gilgamesh Pharmaceuticals, GW Pharmaceuticals, Klein-Buendel Incorporated, Medimmune, Medday, Novartis, Osmotica Pharmaceuticals, Perception Neurosciences, Recursion Pharmaceuticals, Roche, Somahlution, TG Therapeutics; is employed by the University of Alabama at Birmingham and President of Pythagoras, Inc., a private consulting company located in Birmingham AL. FL has participated in consulting agreements/advisory boards/DSMB for Biogen; EMD Serono; Novartis; Teva; Actelion; Sanofi/Genzyme; Acorda; Roche/Genentech; MedImmune/ Viela Bio; Receptos/Celgene; TG Therapeutics; Medday; Atara Biotherapeutics; Polpharma; Mapi Pharma; Innate Immunotherapeutics; Apitope; Orion Biotechnology; Brainstorm Cell Therapeutics; Jazz Pharmaceuticals; GW Pharma; Mylan; Immunic; Population Council. OS serves on the editorial boards of Therapeutic Advances in Neurological Disorders and on data monitoring committees for Genentech-Roche, Pfizer, and TG Therapeutics without monetary compensation, advised EMD Serono, Celgene, Genentech, TG Therapeutics, and Genzyme, and receives grant support from Sanofi Genzyme and EMD Serono.
Funding
Funding for this study was provided in part by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health.