
Abstract
Background:
The majority of ocular myasthenia gravis (OMG) patients will progress to generalized myasthenia gravis (GMG), usually within 2 years of disease onset. The aim of this meta-analysis was to evaluate the effect of early prednisolone and other immunosuppressants therapy on the generalization rate in OMG patients.
Methods:
We searched the CENTRAL, EMBASE, and MEDLINE databases via the Ovid SP database for all relevant publications on 16 July 2018.
Results:
Eight studies comprising a total of 547 participants were included in our meta-analysis. Compared with pyridostigmine treatment, prednisolone and other immunosuppressants therapy produced an odds ratio (OR) for the development of GMG of 0.19 [95% confidence interval (CI), 0.11–0.30; I2 = 37%], indicating that early prednisolone and other immunosuppressants therapy reduced the generalization rate in OMG by 81%.
Conclusions:
Early prednisolone and other immunosuppressants therapy can significantly reduce the risk of generalization in OMG patients, and should be considered in newly diagnosed OMG patients. Due to the inclusion of retrospective studies, this noted effect might have been related to corticosteroids, especially when immunosuppressants used at low dosages and in mild disease. Additionally, the data derived from Western populations, thus a prospective randomized controlled trial (RCT) is warranted to confirm this effect of early prednisolone and other immunosuppressants therapy on OMG generalization both in Western and Asian populations.
Keywords
Introduction
Myasthenia gravis (MG) is a rare organospecific autoimmune disease caused by antibodies that target the neuromuscular junction (NMJ), destroying postsynaptic molecules in the NMJ and ultimately contributing to voluntary muscle weakness. Extraocular muscles are often easily affected, and the initial symptoms of most patients are ptosis and diplopia. This condition is designated as ocular myasthenia gravis (OMG). However, the majority of OMG patients (50–80%) will develop weakness in other muscles, including the bulbar, proximal extremity, and even respiratory muscles, which can be life-threatening, giving rise to generalized MG (GMG), usually within 2 years of disease onset.1–3 Thus, it is crucial to prevent OMG generalization. Several studies have found that early immunosuppression might modify the course of OMG and prevent OMG generalization. However, the initiation time and use of immunosuppression in OMG are still controversial.
Due to the lack of randomized controlled trials (RCT) with OMG patients, and the exclusion of OMG patients from many MG trials, the management of OMG is challenging. Current clinical guidelines in Europe recommend that oral corticosteroids or steroid-sparing treatment with azathioprine should be started when symptomatic treatment fails (recommendation level C). 4 Considering the high risk of generalization in newly diagnosed OMG, early immunosuppression therapy is tempting. Thus, whether early oral corticosteroids and other immunosuppressants therapy can reduce the risk of secondary generalization and should be the standard therapy in newly diagnosed OMG patients remains uncertain. Based on this topic, we performed a systematic review and meta-analysis to evaluate the effect of early prednisolone and other immunosuppressants therapy on the generalization rate in OMG patients.
Materials and methods
Database search and selection of studies
Three of the authors (RZ, NCX, and GYW) systematically searched the CENTRAL, EMBASE, and MEDLINE databases via the Ovid SP database for all relevant publications on 16 July 2018. The search terms included ‘myasthenia gravis’, ‘ocular’ OR ‘eye’ OR ‘visual’, ‘prednisone/prednisolone AND/OR azathioprine’, ‘mycophenolate mofetil’, ‘tacrolimus (FK506)’, ‘cyclosporine’, ‘methotrexate’, and ‘rituximab’. The search was limited to English-language studies and published articles. The studies were read in their entirety to assess the appropriateness of their inclusion in the meta-analysis.
Selection criteria
The selection criteria were as follows: patients with purely ocular symptoms at presentation, that is, ptosis or extraocular muscle weakness in one or both eyes qualified as OMG in accordance with the criteria of the Myasthenia Gravis Foundation of America (MGFA); 5 patients receiving prednisolone or any other immunosuppressants treatment versus patients receiving pyridostigmine treatment for a minimum of 3 months, with treatment started within 1 year of symptom onset; patients with follow-up visits for at least 2 years; RCTs, cohort studies, and observational studies; and OMG generalization reported as a primary outcome.
Exclusion criteria
The exclusion criteria were as follows: patients who developed signs of generalized disease within the 1st month after ocular symptoms presentation (i.e. weakness of the limbs or the facial, bulbar, neck or respiratory muscles); patients who were younger than 18 years old; inability to extract data for all patients with OMG; and case reports and studies that included fewer than two patients.
Data extraction
Three researchers (LMX, GFF, and GRJ) independently filtered published reports by screening titles and abstracts, and two neurologists (CT and LZY) subsequently reviewed the full texts of the papers that met the selection criteria. Articles that unequivocally conformed to the inclusion criteria were included. Two researchers (ZZW and ZYA) assessed the quality of the studies, and disagreements were resolved by repeated discussion and consensus. Three neurologists (LMX, LH, and CT) independently extracted the following data: the first author’s name, publication year, treatment regimens, mean onset age, total participant sample size, separate numbers of patients in prednisolone and other immunosuppressants therapy and control (pyridostigmine) groups, and numbers of patients who developed generalized disease in these two groups, protocol of drugs administration, dosage of prednisolone and immunosuppressants, outcome measurements, study design, duration of follow-up, and country.
Statistical analysis
Data were entered into and analyzed using Stata14. The odds ratio (OR) results with 95% confidence intervals (CIs) were adopted to assess the generalization rate. To assess heterogeneity among studies, we calculated I2 statistics. When the I2 statistic was <50% and the p value for heterogeneity was >0.10, we chose to use a fixed-effect model. In studies where I2 was >50% or the p value was <0.10, we used a random-effect model. Publication bias was assessed by visual examination of funnel plots.
Results
Study selection
Eight studies were included in our meta-analysis, comprising a total of 547 enrolled participants, of which 335 were male.6–13 All the studies were retrospective observational studies. A flow chart of the search strategy is shown in Figure 1. The mean onset age of the patients was 57 years, and the mean follow-up period ranged from 2 to 10 years. The number of participants ranged from 34 to 158. The number of participants was 287 in the prednisolone and immunosuppressants therapy arm and 260 in the control arm, and all trials were performed to compare prednisolone and other immunosuppressants therapy with pyridostigmine treatment. The majority of the patients in our study received prednisolone therapy. The average dosage of prednisolone ranged from 40 to 60 mg, and all drugs were administered orally. Generalization rates in OMG at least 2 years were the main outcome measurement. Of these studies, 6 were from USA,7–12 1 was from Austria, 13 and 1 was from Australia. 6 Detailed features are listed in Table 1

Flow diagram of study selection process.
Clinical characteristics of 547 patients from the eight studies included in this systematic review.
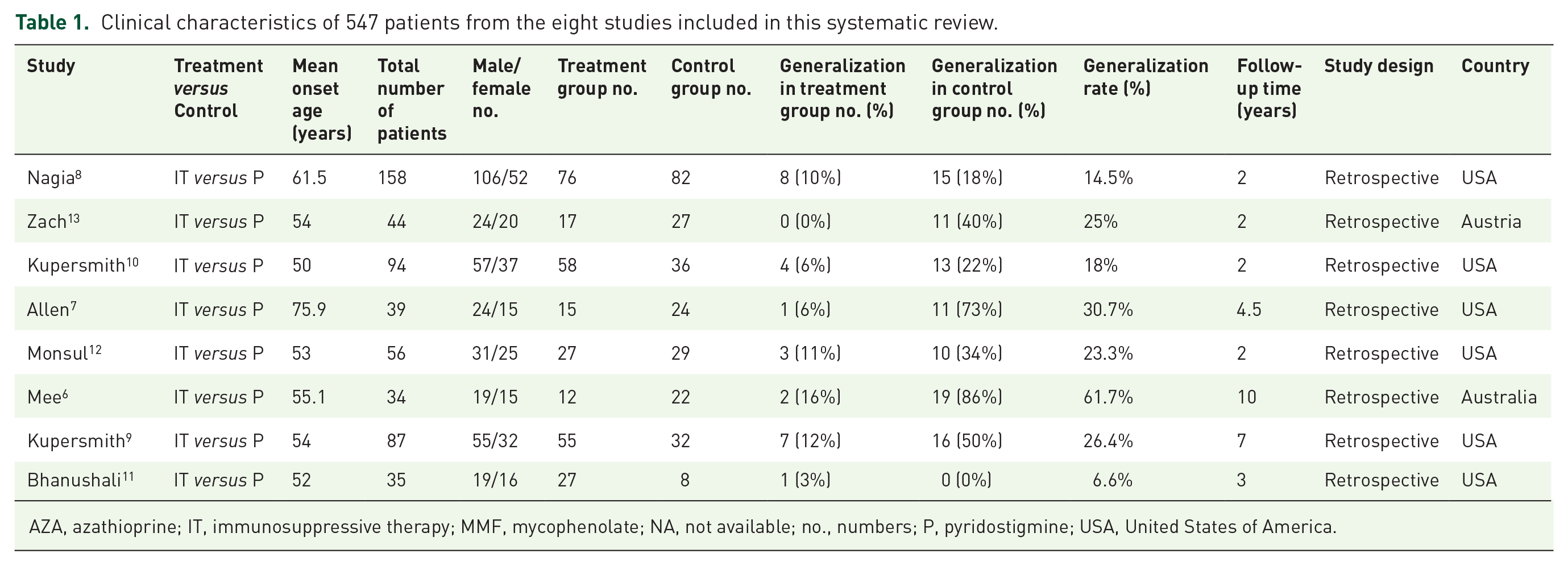
AZA, azathioprine; IT, immunosuppressive therapy; MMF, mycophenolate; NA, not available; no., numbers; P, pyridostigmine; USA, United States of America.
Effect on the generalization rate
Compared with that in the pyridostigmine treatment group, the OR for development of generalized MG in the prednisolone and other immunosuppressants therapy group was 0.19 (95% CI, 0.11–0.30; I2 = 37%), indicating that early prednisolone and other immunosuppressants therapy reduced the generalization rate in OMG by 81% (Figure 2).

Forest plot showing a comparison of the generalization rate between prednisolone and other immunosuppressants therapy and control groups.
Heterogeneity and publication bias
No subgroup analysis was performed due to the lack of available data, and mild heterogeneity was detected among the studies (p = 0.13, I = 37%). The results of the funnel plot did not reveal significant publication bias in this study (Figure 3).

Funnel plot does not show significant publication bias in this study.
Discussion
This is the first systematic review and meta-analysis to investigate the effect of early prednisolone and other immunosuppressants therapy on the generalization rate in OMG patients. The results indicated that immune-directed treatment could significantly reduce the risk of secondary generalization in OMG patients.
With regard to demographics, the participants in our study were predominantly male, with a male:female ratio of 1.5:1, and the median onset age was 57 years, which is consistent with a previous report indicated that this disease was reported to occur slightly more frequently in males than in females in the older age group. 14 The incidence of MG presented a bimodal age distribution, with a peak at approximately the age of 30 years, and again at the age of 50 years.15,16 It is well known that MG is a heterogeneous disease regarding onset age, thymic pathology, autoantibody profile, and affected muscles. Therefore, MG guidelines and consensus recommended patients with MG should be subgrouped by implications on diagnosis, optimum therapy, and prognosis.17,18
Except for Mee’s study, with a 10-year follow-up, all other studies demonstrated a much lower generalization rate (less than 30%) of OMG to GMG than previous report in our study. However, this outcome might be influenced by the inclusion of immunosuppressed patients in most studies, which may lower generalization rate. The difference in baseline characteristics of including populations contributed to the variable results in OMG generalization rate. A much lower generalization rate was reported in Asian populations.19,20 However, Wang and colleagues reported a higher generalization rate (85%), which might be related to the late age of disease onset or limited sample size in their study. 21
Based on onset age, MG can be classified as early-onset MG (EOMG) and late-onset MG (LOMG). LOMG patients are defined as having their first onset of symptoms after the age of 50 years. The patients in our study were all LOMG patients, and it has been reported that the patients in this subgroup are more prone to severe disease. Additionally, serum anti-AChR antibodies are always present, thymoma is more frequent, and the transformation rate of OMG into GMG is higher in this subgroup.22,23 Several retrospective studies have reported risk factors associated with OMG transformation. 9,10,24,25 Similar results were reported in Asian populations. Lili Wang’s study showed that late onset as well as thymic hyperplasia predicted generalization. 21 In the study of Korean OMG patients, anti-AChR antibodies, thymoma, early corticosteroid treatment, and possibly latent neuromuscular abnormalities might predict OMG generalization. 20 Among these factors, older age at onset is an important risk factor associated with generalization. Our results suggest that prednisolone and other immunosuppressants therapy may prevent generalization in the subgroup of LOMG.
In contrast to Western countries, Chinese childhood-onset MG (CMG) patients predominantly present with pure ocular symptoms. It was reported the transformation rate of CMG (12.4%) was significantly lower than the rate of adult MG patients (32.5%). This result might be influenced by combined therapy with pyridostigmine and prednisone. Thus, the efficacy of prednisone in lowering generalization of CMG needs more RCTs. 26 Considering the side effects of long-term use of prednisone, especially the growth failure and Cushing’s reaction in CMG patients, the use of corticosteroids in this subgroup should be balanced between symptom improvements and side effects.
The majority of the patients in our study received treatment with prednisolone. Despite its drawbacks, corticosteroid therapy remains the first-line immunotherapeutic strategy in OMG.4,27,28 Recently, other potential immunosuppressive agents, such as azathioprine, tacrolimus, mycophenolate mofetil, cyclosporine, and rituximab, have been used increasingly as monotherapies, or in combination with corticosteroids, for MG therapy, with the aim of achieving steroid sparing and preventing relapses.29–31 It is well known that the clinical effect of immunosuppressants such as azathioprine is slow. Improvement often occurs after 3–6 months, with the full effect of the drug occurring after 1–2 years. Thus, immunosuppressants are usually combined with other immunoactive treatments, such as prednisone/prednisolone, especially in the initial phase.
Due to the inclusion of retrospective studies, there is large heterogeneity in treatment protocol and drug selection in our meta-analysis. Some patients were treated with prednisolone alone, some with steroid-sparing agents such as azathioprin, cyclosporin, mycophenolate, etc., and some with both prednisolone and steroid-sparing agents. Data on the doses and duration of immunosuppressants were not available; we speculated the effects might come from corticosteroids when immunosuppressants were given with low dosage and short duration. Additionally, there were no data comparing prednisolone and other immunosuppressants in reducing OMG generalization risk; thus, we did not perform subgroup analysis to investigate the effects of different immunosuppressants on OMG generalization. In the future, a prospective RCT is warranted to assess the impact of different immunosuppressive agents on OMG generalization.
This meta-analysis is limited in many aspects. Firstly, although there was no significant publication bias, the funnel plot was limited in this situation as fewer than 10 studies were included. Secondly, all studies included in this meta-analysis were from United States and Europe; relevant reports about Asian populations were lacking. The results of the study are likely not transferable to Asian populations, as previous studies have shown a much lower rate of generalization to GMG.19,20 Thirdly, there was mild heterogeneity among the studies, but selective biases existed on onset age and immunosuppressant type. Thus, future study design should include various subgroups with different onset age to observe the effect of different immune-directed treatment on OMG generalization. Lastly, all studies included in our meta-analysis were retrospective studies, which has limitations in determining what was responsible for the noted effects. Considering that the benefit of immunosuppressants has never been established in ocular MG, especially when used at low dosages and in mild disease, it is likely that the effects observed might have been related to corticosteroids. Therefore, prospective cohort studies and multicenter RCTs are needed to confirm the effect of early prednisolone and other immunosuppressants therapy on OMG generalization.
In conclusion, early prednisolone and other immunosuppressants therapy can significantly reduce the risk of secondary generalization in OMG patients and should be considered in newly diagnosed OMG patients. It may be time to call for a prospective RCT to confirm this effect in Western and Asian populations.
Footnotes
Acknowledgements
Authors Mingxia Li, Fangfang Ge, and Rongjing Guo contributed equally.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded by the National Natural Science Foundation of China (grants 81671233 and 81571218) and the Innovation and Development Fund of Tangdu hospital (grants 2016LCYJ006).
Conflict of interest statement
The authors declare that there is no conflict of interest.