
Abstract
Until the early 1990s, a limited number of antiepileptic drugs (AEDs) were available. Since then, a large variety of new AEDs have been developed and introduced, several of them offering new modes of action. One of these new AED families is described and reviewed in this article. Levetiracetam (LEV) and brivaracetam (BRV) are pyrrolidone derivate compounds binding at the presynaptic SV2A receptor site and are thus representative of AEDs with a unique mode of action. LEV was extensively investigated in randomized controlled trials and has a very promising efficacy both in focal and generalized epilepsies. Its pharmacokinetic profile is favorable and LEV does not undergo clinically relevant interactions. Adverse reactions comprise mainly asthenia, somnolence, and behavioral symptoms. It has now been established as a first-line antiepileptic drug. BRV has been recently introduced as an adjunct antiepileptic drug in focal epilepsy with a similarly promising pharmacokinetic profile and possibly increased tolerability concerning psychiatric adverse events. This review summarizes the essential preclinical and clinical data of LEV and BRV that is currently available and includes the experiences at a large tertiary referral epilepsy center.
Introduction
Since the introduction of bromides as the first effective antiepileptic drugs (AEDs), 1 chronic AED treatment that consisted of the sustained prevention of epileptic seizures has remained the standard of epilepsy therapy. 2 Before to the introduction of the newer generation of AEDs, a limited number of drugs were available that addressed the blockade of sodium channels, acting on gamma-aminobutyric acid (GABA) type A receptors, or interacting with calcium channels as the leading modes of action. 3 With the introduction of the newer AEDs a heterogeneous group of drugs appeared, some of them offering new mechanisms of action 2 including the blockade of GABA aminotransferase (vigabatrin [VGB]), GABA re-uptake from the synaptic cleft (tiagabine [TGB]), the modulation of calcium channels (gabapentin [GBP], pregabalin [PGB]), the selective non-competitive α-amino-3-hydroxy-5-methyl-4-isoxazolproprionic acid (AMPA) receptor antagonism (perampanel [PER]), and the binding to the presynaptic SV2A receptor site which is the unique mode of action of levetiracetam (LEV) and brivaracetam (BRV), the AEDs this review will cover. The authors will summarize the development of both compounds as derivatives of piracetam, review the currently available preclinical and clinical data, and discuss the question of whether BRV has the potential to be recognized as being superior to LEV and if it can replace it as the standard AED with the main mode of action both AEDs reflect.
Chemistry and developmental history
LEV ([S].alpha-ethyl-2-oxo-1-pyrrolidineacetamide) (C8H14N2O2) 4 (LEV) and BRV ([2S]-2-[(4R)-2-oxo-4-propylpyrrolidin-1-yl] butanamide) (C11H20N2O2) 5 (BRV) belong to a group of pyrrolidone compounds 6 derived from piracetam and are subjects of a development plan of the Belgian pharmaceutical company UCB. 7 After the preclinical work described in the pharmacology section of this chapter, a clinical development program was carried out that finally led to the labeling and launch of LEV in 1992.
Piracetam was synthesized in 1964. Initially, its development targeted sleep induction by γ-GABA analogs. 8 However, whereas GABA-ergic effects were not demonstrated, atypical psychotropic effects were revealed 9 that indicated a selective and direct telencephalic action and made piracetam the founding agent of nootropics. 9 Further work led to etiracetam, an ethyl analog of piracetam. LEV (ucb L059, ((S)-α-ethyl-2-oxo-1-pyrrolidineacetamide)) is the S-enantiomer of etiracetam. 10 LEV failed to show beneficial effects on cognition in humans but was investigated in epilepsy models because piracetam had shown efficacy in the treatment of photoparoxysmal responses and myoclonus.11–14 In fact, pilot studies supported the efficacy of LEV in myoclonus and against photosensitivity.15–18 Clinical investigations rapidly showed that piracetam belonged to the group of nootropics, whereas LEV was unequivocally identified as a very potent AED. 6 BRV was developed subsequently in order to develop an anticonvulsant compound with a higher affinity to the binding site described in the following section that was identified as the main and unique mode of action of LEV.
Pharmacology
Pharmacokinetics and pharmacodynamics of levetiracetam
The pharmacokinetic profile of LEV is extremely promising. It undergoes rapid and almost complete absorption resulting in a bioavailability of more than 95%. 19 The time of peak serum concentration (Tmax) occurs at 1,3–5,2 h. 20 Plasma steady state is reached 24–48 h following initiation of treatment. 21 Tmax is slightly delayed by food intake but the maximum concentration (Cmax) is not affected. 22 Mean elimination half-life is 7, 6 and 10,5 h in adults, children and elderly patients respectively. 19 LEV can be taken without regard to mealtimes. 20 LEV enters the cerebrospinal fluid (CSF) compartment with a Tmax of 3–7.3 h. 21 The mean half-life in CSF is 24 h. Thus, LEV remains in the central nervous system (CNS) compartment twice as long as in the blood. This supports clinical observations of a prolonged anticonvulsant efficacy despite of low serum concentrations.15,23 LEV appears to have a prolonged duration of action irrespective of its peripheral pharmacokinetics, supporting a twice-daily dosing strategy. 21 Even once-daily dosing is possible with the extended-release formulation of LEV.24,25 One case report even described a beneficial effect of once-weekly dosing of LEV. 26
LEV is not bound to plasma proteins and it does not affect the protein binding of other drugs.19,22 It is not metabolized in the liver19,22 and is independent of the hepatic cytochrome P450 system. LEV does not inhibit or induce hepatic enzymes to produce clinically relevant interactions.19,22 It has been shown that LEV does not influence the concentration of carbamazepine (CBZ), clobazam, clonazepam, diazepam, gabapentin (GBP), lamotrigine (LTG), phenytoin, phenobarbital, primidone, valproic acid, vigabatrin (VGB), and ethosuximide.15,27 In contrast, enzyme-inducing AEDs, including CBZ, may lower the serum concentration of LEV and increase its clearance.28–30 However, the almost complete lack of interactions qualifies LEV as a suitable candidate for combination therapies of AEDs. In a large survey of 517 patients, it was the most frequently used antiepileptic drug in case of combination therapies. 31 Pharmacodynamic interactions with CBZ, topiramate, and lamotrigine have been reported19,32–34 but more on an anecdotal than on a systematic basis. A recent review did not confirm clinically relevant pharmacodynamic interactions.35,36 LEV is primarily excreted unchanged in the urine (64%) and dose adjustments may be necessary for patients with renal impairment, 19 and 24% is metabolized into an inactive metabolite that may be detected in blood and urine. 22
The teratogenic safety profile of LEV is very favorable. In monotherapy, the risk of major malformations is 2.8% and dose-independent. 37
LEV is available for both oral (tablet or liquid formulation) and intravenous application. 20
Pharmacokinetics and pharmacodynamics of brivaracetam
Similar to LEV, the pharmacokinetic profile of BRV is extremely promising. It undergoes rapid and almost complete absorption resulting in complete bioavailability. 38 The time of peak serum concentration (Tmax) occurs at 1 h.39,40 Plasma steady state is reached less than 48 h after initiation of treatment. 38 High-fat food delays Tmax and decreases Cmax but has no effect on the area under the plasma concentration-time curve (AUC). 40 Twice-daily dosing is possible and recommended. Protein binding rate is below 20%. The volume of distribution is slightly lower than that of total body water. Mean elimination half-life is 9 h. 38 BRV shows a fast and unrestricted passage across the blood-brain barrier. The passive diffusion permeability is superior to that of LEV, with no evidence of transporter-mediated extrusion from the brain. 7 Thus, a faster onset of brain activity results. 7 After intravenous administration of BRV, brain concentrations peak within minutes compared with 1 h after injection of LEV. 41 Proton-emission tomography (PET) imaging studies using the SV2A radioligand PET tracer [ 11 C] UCB-J supported the faster drug-entry half time of BRV versus LEV in rhesus monkeys 41 and in human volunteers with a similarly fast brain entry and SV2A binding.42,43 There is no evidence of a transporter-mediated efflux from the brain. 44
BRV is extensively metabolized, primarily by hydrolysis of the acetamide group, to the carboxylic acid metabolite by an amidase.45,46 Thereafter, hydroxylation by cytochrome P450 (CYP)2C9 takes place to form a hydroxyl-acid metabolite. A secondary pathway is the β-oxidation of the propyl side chain, primarily by CYP2C19. The three main metabolites (acid, hydroxyl, and hydroxic acid) are not active. More than 95% of BRV is eliminated in the urine within 72 h, and 8.6% remains unchanged. The remainder consists of metabolites. 38 Thus, comedication of BRV, with substances with interfering pathways, may potentially cause interaction problems.
The pharmacokinetics of BRV is not influenced by age, sex, race, and creatinine clearance. Enzyme-inducing AEDs increase BRV clearance. 47 However, this effect is not considered to be clinically relevant.38,48 In contrast, BRV exposure is increased by 11% under the influence of valproate in a pediatric population. 49 Although a 21% increase of BRV exposure with a higher proportion of acid, hydroxyl, and hydroxic acid metabolites was found in volunteers with severe renal impairment it is unlikely that dose adjustments are required. 50 BRV clearance is increased in people with hepatic impairment and dose adjustments may be necessary38,51
BRV has no apparent or clinically relevant effect on CYP450 enzymes. 38 Potent CYP2C8 or CYP2C9 inhibition has no effect on BRV exposure 52 whereas the co-administration of rifampicin may require a dose increase of BRV. 46 In a sample of 1771 patients undergoing clinical trials with BRV (see below) the effects of BRV on plasma concentrations of other AEDs was investigated.38,53 BRV had no effect on the steady state plasma concentration of LEV, CBZ, lacosamide, LTG, 10-hydroxy-oxcarbazepine, phenobarbital, pregabalin (PGT), phenytoin, topiramate, valproate, or zonisamide. The plasma concentration of CBZ epoxide, an active major metabolite of CBZ, was significantly increased by the BRV-mediated inhibition of epoxide hydrolase. 54 However, clinical adverse events were not observed in this study38,53 and in post hoc analysis,48,55 but may occur in clinical practice. 56 Recently, an increase of BRV levels by 95–280% was reported if cannabidiol was added. It was suggested that the inhibition of CYP2C19 by cannabidiol might be responsible for this interaction. 57 No relevant interactions have been observed between 100 mg BRV per day and combined oral contraceptives (30 µg ethinyl estradiol, 150 µg levonorgestrel). 58 Usually, supratherapeutic doses of 400 mg BRV per day resulted in a 27% reduction pf plasma levels of ethinyl estradiol and a 23% reduction in levonorgestrel levels. However, no ovulation occurred in any individual investigated. 59 To the best of the authors’ knowledge data concerning its safety in pregnancy is not yet available.
BRV is available for both oral (tablet or liquid formulation) and intravenous applications all with appropriate bioequivalence profiles. 38
Due to the close relationship of LEV and BRV, an immediate switch from LEV to BRV at a ratio from 10:1 to 20:1 is possible and easily performed. The reverse is similarly easy.48,56,60
Mechanism of action
For LEV a brain-specific stereoselective binding site was identified that piracetam had no affinity with. This difference is responsible for the different clinical profiles of piracetam and LEV. 6 At the time the decision to carry out further clinical development of LEV was taken in epilepsy, it was notable because LEV had failed in two crucial and traditional seizure models, namely the maximal electroshock seizure (MES) and the subcutaneous pentylenetetrazol (PTZ) tests in mice and rats. 4 However, it showed potency in amygdala-kindled rats4,61 and was, therefore, further investigated in clinical trials. In addition, potent activity was found against generalized epileptic seizures in electrically and PTZ-kindled mice, secondarily generalized activity from focal seizures induced by pilocarpine in mice, and by pilocarpine and kainic acid in rats, in corneal kindled mice and in Genetic Absence Epilepsy Rats from Strasbourg. 61
Of interest, and in contrast with traditional AEDs, LEV, in spite of a significant effect against epileptiform activity in vitro and in vivo, showed no intrinsic activity on neuronal function. This suggested an absence of interaction with ion channels and receptor targets that are typically involved in the action of conventional AEDs 10 and thus a completely unique preclinical profile. 7
Indeed, binding studies revealed a reversible, saturable, and stereoselective brain-specific binding site in rats. 62 Further studies demonstrated a correlation between affinities for this binding site and anticonvulsant activity 62 and identified this binding site as synaptic vesicle protein 2A (SV2A) 63 that conventional AEDs do not bind to. 7 The anticonvulsant activity of LEV was reduced in SV2A knockout mice 64 which supports the evidence that this mechanism is essential for the anticonvulsant properties of LEV.65,66 LEV has only moderate affinity to SV2A and has several other mechanisms of action, 7 namely the inhibition of N-type calcium channels67–70 and as an AMPA receptor antagonist. 7 Therefore, UCB initiated a major development program in order to identify more selective, high-affinity SV2A ligands with potentially superior anticonvulsant efficacy compared with LEV. 7 From approximately 12,000 compounds that were tested two promising anticonvulsants were identified, BRV and selectracetam (SEL).
Both BRV and SEL inhibited neuronal hyper synchronization with BRV demonstrating a more pronounced effect. 7 In contrast with LEV and SEL, BRV demonstrates seizure protection in the MES and the subcutaneous PTZ tests though at high doses. Its significant protection against the partial seizure phase in animal models of focal epilepsy finally prompted the decision to focus on the further clinical development of BRV. 7 BRV demonstrated higher potency than LEV in a variety of animal seizure models, including MES and PTZ tests in cornea-kindled mice, hippocampus-kindled rats and the 6 Hz seizure model in mice, and in models of primary generalized epileptogenesis.7,38,71–74 In addition, potent efficacy was evident in a model status epilepticus. 75
It has been demonstrated that BRV has a 15- to 30-fold increased affinity for SV2A compared with LEV and that at doses more than 100 fold higher its affinity for SV2A BRV did not bind, activate or inhibit a panel of 55 other receptors, channels and enzymes. 76 The differential effect of the allosteric SV2A modulator on the binding of LEV and BRV suggests that they influence different conformations of the SV2A protein. 7 Mutations of several amino acids in the SV2A protein had marked effects both on the binding of LEV and BRV but three were identified with a differential effect on the modulation of LEV and BRV binding, respectively. Therefore, it was concluded that LEV and BRV bind to SV2A at closely related sites but interact with these sites differently. 77
In contrast to earlier reports, it has been repeatedly demonstrated that the anticonvulsant effect of BRV is not related to an effect on voltage-gated sodium, calcium or potassium channels. 7 In addition, there is no evidence for relevant interactions of BRV with any inhibitory or excitatory receptors. 7
Indications
In April 2019 LEV was labeled as add-on antiepileptic drug for patients with focal epilepsies from the age of 1 month upward, and in patients with juvenile myoclonic epilepsy and with idiopathic generalized epilepsy from the age of 12 years upwards. It is indicated as a monotherapy in patients with focal epilepsies from the age of 12 years upwards. This labeling includes Algeria, Argentina, Armenia, Australia, Bosnia and Herzegovina, Brazil, Canada China, Croatia, the Czech Republic, the European Union, Georgia, India, Ivory Coast, Japan, Jordan, Serbia, Slovenia, South Korea, Macedonia, Mexico, Montenegro, New Zealand, Oman, the Russian Federation, Senegal, Switzerland, Turkey, Ukraine, the United Arab Emirates, the United States, and many more.
In April 2019 BRV was labeled as an add-on antiepileptic drug for patients with focal epilepsy in Australia, Belgium, Canada, Denmark, Finland, Germany, Greece, Hungary, India, Ireland, Israel, Italy, Luxembourg, Mexico, The Netherlands, Norway, Qatar, the Russian Federation, Slovakia, Spain, Sweden, Switzerland, the United Kingdom, the United Arab Emirates, and the United States where a monotherapy license also exists.
Clinical studies
The potential efficacy of LEV and BRV was evaluated first in patients with photosensitive epilepsies.15,78 Both AEDs were effective in suppressing the photosensitive responses in the electroencephalogram in these short-term, patient-blinded studies.
The pivotal trials with LEV and BRV that lead to the actual labeling are listed in Tables 1 and 2. Since numerous randomized controlled trials were performed especially with LEV, only the randomized controlled double-blind studies are listed. Open-label trials are mentioned and discussed in the main text of this article.
Randomized controlled trials with levetiracetam.

CBZ, carbamazepine; LEV, levetiracetam; LTG, lamotrigine.
Randomized controlled trials with brivaracetam.
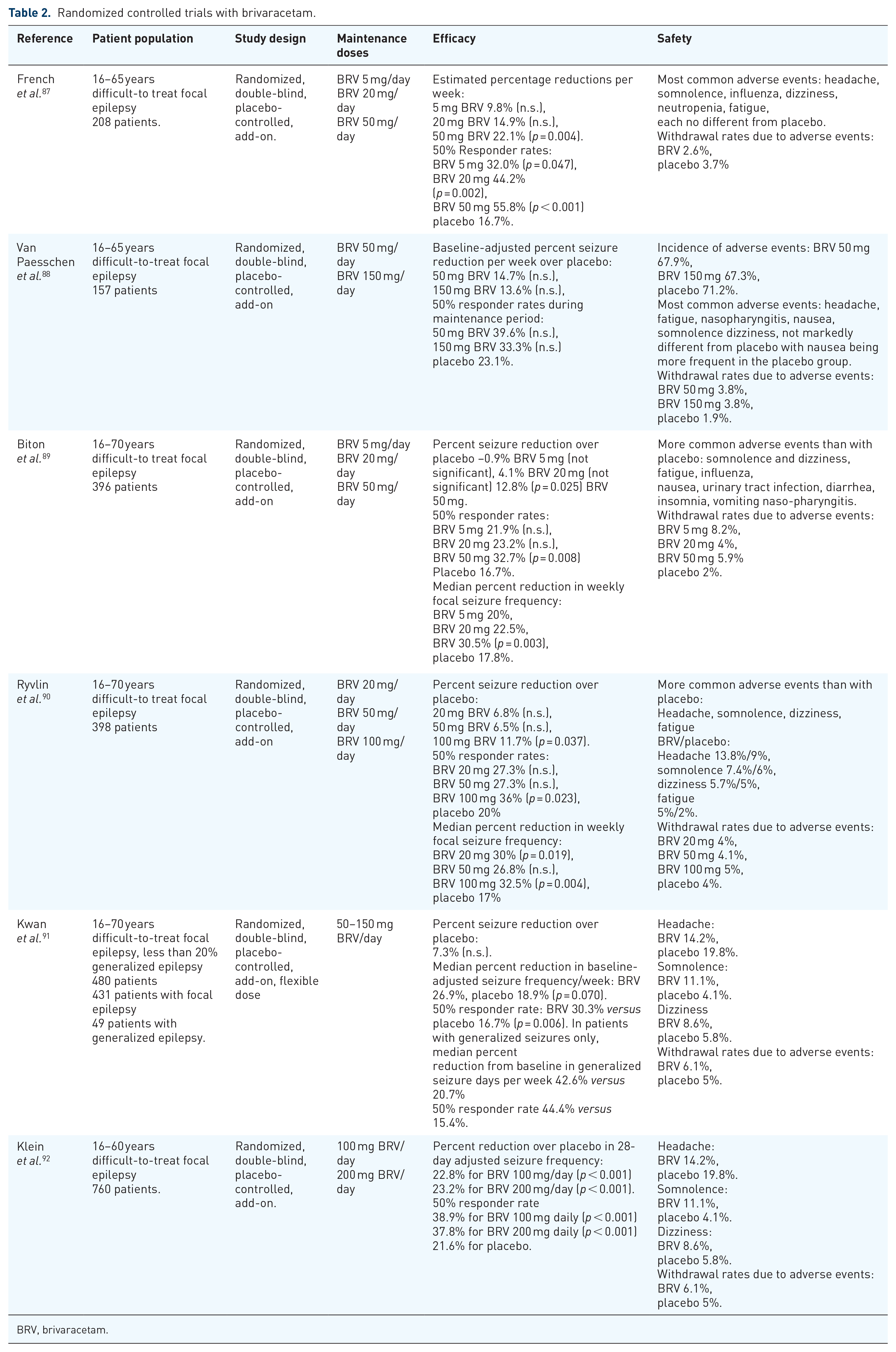
BRV, brivaracetam.
Clinical studies with LEV and BRV as an add-on in patients with focal epilepsies
LEV
Efficacy and tolerability of LEV as an adjunct in patients with difficult-to-treat focal epilepsy was assessed in several multicenter, double-blind, placebo-controlled studies.
Shorvon and colleagues, 79 carried out a 61 center study that comprised 324 patients and investigated the efficacy and tolerability of LEV at doses of 500 mg or 1000 mg twice-daily versus adjunct placebo after a baseline of 8 or 12 weeks, a titration period of 4 weeks and an evaluation period of 12 weeks, according to parallel-group design. A total of 106 patients were randomized to LEV 1000 mg/day or 2000 mg/day, respectively, and 112 patients were randomized to placebo. The median reduction of weekly seizures was 26.5% for 2000 mg/day LEV, 17.7% for 1000 mg/day LEV, and 6.1% for placebo. Both LEV doses were statistically superior compared with the placebo (p ⩽ 0.001). The efficacy between the two doses was not significantly different. Responder rates (rate of seizure reduction of at least 50%) were 22.8% with 1000 mg/day LEV, 31.6% with 2000 mg/day LEV, and 10.4% with placebo (p ⩽ 0.001for 2000 mg LEV, p = 0,019 for 1000 mg LEV). There was no statistically significant different efficacy between the two LEV doses investigated.
There were no significant differences in the incidence of adverse events between the three groups. The most frequently reported adverse events with LEV were somnolence, asthenia, and headache. Serious adverse events potentially related to the study drug in the opinion of the investigator were observed in 2.7% with placebo, 1.9% with 1000 mg/day LEV and in 7.5% with 2000 mg/day LEV. LEV had no impact on the serum concentrations of concomitant AEDs, blood chemistry, urine analysis, vital signs, or electrocardiogram.
The study by Ben-Menachem and Falter 81 compared a maintenance dose of 3000 mg LEV daily with add-on placebo in 286 patients at 47 sites according to a multicenter, randomized, double-blind, parallel-group design in patients at age 16–70 years old with difficult-to-treat focal epilepsies. In addition, conversion to monotherapy was an open-label option. The responder rate was significantly higher with LEV (42.1% versus 16.7%, p < 0.001). A total of 49 patients entered the monotherapy with a median seizure percentage reduction of 73.8%. The most frequent adverse event significantly different from placebo was asthenia (13.8% versus 6.7%).
Several pooled studies supported the beneficial efficacy-safety ratio of LEV in the pivotal trials. 20
The pivotal trial in the USA was a 38 week study at 41 sites with 294 patients and addressed maintenance LEV daily doses of 1000–3000 mg, respectively compared with placebo according to a randomized, double-blind, parallel-group design. 80 After a baseline of 12 weeks patients were randomly assigned to placebo (n = 95), LEV 1000 mg daily (n = 98) or LEV 3000 mg daily (n = 101). After a 4 week titration, the evaluation period lasted 14 weeks. Both median seizure frequency reductions and responder rates differed significantly (p ⩽ 0.001 for both groups and variables) from placebo. Adverse events were reported in 88.4% of patients in the placebo group, in 88.8% in the low-dose LEV group and in 89.1% in the high-dose LEV group. Treatment-emergent adverse events occurred more frequently than with the placebo and included asthenia, dizziness, flu-like symptoms, headache, infection, rhinitis, and somnolence.
Betts and colleagues 82 carried out a 24 week multicenter parallel-group study at 37 sites.
After a 1–4-week baseline patients were treated with adjunct placebo or daily doses of 2000 mg or 4000 mg LEV, respectively, which were initiated without titration. The double-blind evaluation period lasted for 24 weeks. Thereafter patients had the opportunity to enter an open-label phase on 4000 mg LEV daily. A total of 119 patients were randomized with 42 in the group receiving 2000 mg LEV daily, 38 in the group receiving 4000 mg LEV daily and 39 in the placebo group. The incidence of adverse events was 83.3% with LEV 2000 mg, 84.2% with LEV 4000 mg and 84.6% in the placebo group. The most common adverse events were somnolence and asthenia. Somnolence occurred more frequently (44.7%) with 4000 mg LEV daily compared with 2000 mg LEV daily (26.2%) and with placebo (26.6%).
Efficacy could be assessed in 86 patients. Responder rates were 48.1% with 2000 mg LEV daily and 28.6% with 4000 mg LEV/day compared with 16.1% with placebo. Only the difference between LEV 2000 mg and placebo was statistically significant (p = 0.01). In the open-label phase, patients switching from placebo to LEV showed a decline of seizures.
Asthenia occurred most frequently in the LEV 2000 mg group (31%) and was similar to LEV 4000 mg (13.2%) and with placebo (15.4%). In no case, serious adverse events were considered to be related to the study drug. No significant changes were reported concerning clinical laboratory parameters, physical or neurological examinations or concomitant AED serum levels. Premature discontinuations happened in 25.6% under placebo, in 33.3% under 2000 mg LEV/day and in 23.7% under 4000 mg LEV/day. The most common reason was adverse events (15.4%, 26.2%, and 13.2%).
Several papers reporting pooled data supported the evidence for a satisfying efficacy of LEV as an add-on in patients with focal epilepsy. 20 According to the pooled data analysis by Privitera, 93 Shorvon and van Rijckevorsel, 94 and Meencke and Buyle 95 there was a better dose-responsive efficacy with increasing doses if 1000 mg, 2000 mg, and 3000 mg LEV daily were compared with each other whereas adverse events did not show a similar dose-relationship. 95 Later studies and the authors’ practical experience indicate that this dose-relationship is questionable under real-world experiences because more than 95% of seizure-free patients in a cohort of 425 patients were on LEV doses of 2000 mg or below per day. Serum concentration in seizure-free and not seizure-free patients did not differ in a recent survey from South Korea. 96 Numerous observational open-label trials were performed with LEV and have been published in the literature. Open-label long-term data from patients who had been recruited for the pivotal trials, five follow-up studies, and 26 phase II continuation trials comprising 1422 patients with focal epilepsies. 97 The median daily dose was 3000 mg. Retention rates were 60% after 1 year, 37% after 3 years and 32% after 5 years. The median percentage of seizure reduction over the whole time was 39.6%. No evidence for tolerance was found. Similar results were reported by Bauer and colleagues. 8
The two largest phase IV trials were the KEEPER and the SKATE trial.99,100 The KEEPER trial comprised 1030 patients with ongoing focal seizures from the age of 16 years or older. LEV was given at between 1000 mg and 3000 mg daily. During the 16 weeks of the trial, 57.9% experienced a seizure reduction of at least 50%, and 20% were seizure-free. 99 The SKATE trial recruited 1541 patients with the identical inclusion criteria as the KEEPER trial. 50.1% had a seizure reduction by more than 50%, 15.8% were seizure-free. 101
A randomized controlled comparative trial versus sulthiame in patients with benign epilepsy with centrotemporal spikes in childhood showed significantly higher dropout rates with LEV. The sample size was not large enough to generate conclusive data concerning the primary variable which was non-inferiority of LEV. 102
BRV
Two double-blind phase II trials addressing efficacy and tolerability of BRV were carried out in patients aged between 16 and 65 years, with difficult-to-treat focal epilepsies according to a prospective, placebo-controlled design. French and colleagues 87 investigated maintenance doses of 5 mg, 20 mg and 50 mg versus placebo in a 7 week study in 208 patients. 197 patients completed the study. At 50 mg daily a statistically significant estimated weekly seizure reduction was observed (p = 0.004). Concerning secondary outcome variables (median percentage of seizure reduction, 50% responder rate), both 50 mg and 20 mg showed a statistically significant superiority. The study by Van Paesschen and colleagues 88 investigated the efficacy and safety of add-on BRV at maintenance doses of 50 and 150 mg daily. A 3 week titration period was followed by a 7 week evaluation period. A total of 157 patients were randomized and 148 completed the study. The percent reduction in baseline-adjusted weekly seizure frequency during the 7 week maintenance period did not reach statistical significance. During the entire 10 week treatment period a statistically significant difference was observed for both BRV groups (50 mg p = 0.026, 150 mg p = 0.043). The median percent reduction from baseline in partial-onset seizure frequency/week showed a statistically significant superiority over placebo only for 50 mg daily. For 50% the responder rates were only significantly different from placebo for 50 mg BRV daily during the entire treatment period.
Four multicenter, randomized, double-blind, placebo-controlled studies with add-on BRV were performed.89–92
Biton and colleagues 89 investigated maintenance doses of 5 mg, 20 mg, and 50 mg daily in 396 patients aged between 16 and 70 years. Patients were randomized according to a 1:1:1:1 ratio. BRV was started with the maintenance dose without titration and according to a twice-daily regimen. The primary efficacy endpoint was percent reduction over placebo in baseline-adjusted partial-onset seizure frequency per week during the 12 week treatment period. Percent seizure reduction over placebo was 0.9% for BRV 5 mg daily (not significant), 4.1% for BRV 20 mg daily (not significant), and 12.8% (p = 0.025) for BRV 50 mg/day. Statistical significance was also achieved for the percent reduction over placebo in baseline-adjusted focal seizure frequency per 28 days for BRV 50 mg/day (22.0%, p = 0.004) but not for the other BRV doses. In the BRV 50 mg group, statistical significance was also seen for the ⩾50% responder rate (BRV 32.7% versus placebo 16.7%, p = 0.008) and median percent reduction from baseline in partial-onset seizure frequency per week (BRV 30.5% versus placebo 17.8%, p = 0.003).
The study of Ryvlin and colleagues 90 addressed BRV maintenance daily doses of 20 mg, 50 mg, and 100 mg daily. The study comprised 398 subjects aged between 16 and 70 years. Percent seizure reduction over placebo was 6.8% for 20 mg BRV daily, 6.5% for 50 mg BRV daily and 11.7% for 100 mg BRV daily. Only the latter difference was statistically significant (p = 0.037). The 50% responder rates were 27.3%, 27.3%, 36%, and 20% for BRV 20 mg, 50 mg, 100 mg and placebo, respectively. Again, only 100 mg BRV was significantly superior (p = 0,023).
Given that the dose finding appeared to be difficult another randomized controlled trial 91 using a flexible dose regimen, and including generalized epilepsies, was carried out. This trial recruited 480 patients according to a 3:1 ration (359 on BRV, 121 on placebo). Patients were started with 20 mg BRV add-on daily, which could be increased up to 50–150 mg daily during an 8 week dose finding period. This was followed by an 8 week maintenance period. A total of 431 patients had focal epilepsy and 49 had generalized epilepsy. In patients with focal seizures, the baseline-adjusted percent reduction in seizure frequency per week over placebo was 7.3% (p = 0.125). The median percent reduction in baseline-adjusted seizure frequency per week was 26.9% with BRV versus 18.9% with placebo (p = 0.070). The 50% responder rate was 30.3% with BRV versus 16.7% with placebo (p = 0.006).
Due to the partially negative outcomes of the phase III trials the largest study concentrated on higher BRV doses, namely 100 mg and 200 mg daily according to a multicenter, randomized, double-blind, placebo-controlled trial. 92 In total 760 patients aged between 16 and 80 years were recruited. Percent reduction over placebo in a 28 day adjusted seizure frequency was 22.8% for BRV 100 mg/day (p < 0.001) and 23.2% for BRV 200 mg/day (p < 0.001). The ⩾50% responder rate was 21.6% for placebo, 38.9% for BRV 100 mg daily (p < 0.001), and 37.8% for BRV 200 mg daily (p < 0.001).
A specific aspect is the relationship between LEV and BRV. Pooled analysis of the phase II and III trials revealed that the combination of LEV and BRV is not effective and that the prior unsuccessful use of LEV is a negative predictor for the efficacy of BRV. 38 In real-world observational studies, however, patients switching from LEV to BRV, or with LEV in their history, could benefit from adjunct BRV.56,60,103–105
Following the launch of BRV, several real-world observational open-label studies were published. From the authors’ own experience in 101 adult patients 56 with difficult-to-treat focal epilepsies, a mean maintenance dose of 168.8 mg daily was used (median 200 mg, range 50–400 mg). For a period of 3 months, the 50% responder rate was 27.8% with 7% seizure-free patients. In 43 cases, LEV and BRV were switched. The switch was performed abruptly without complications. In 26 cases (60%) BRV was discontinued and re-switched to LEV within weeks, mainly due to a lack of better efficacy. After the switch from LEV to BRV, the authors saw an aggravation in both seizure frequency and severity in five cases. The retention rate in patients who had not been on LEV was 57%.
Another survey in 262 patients 60 in a less refractory patient cohort reported a mean BRV daily dose of 175.7 mg. Half of the patients were switched from LEV to BRV in a 10:1 or 15:1 ratio. These authors did not switch between LEV and BRV abruptly in every patient. The 50% responder rate at 6 months was 40.5% with 15.3% seizure-free patients and a 6 month retention rate of 75.8%.
Hirsch and colleagues 104 concentrated on 102 patients who had been treated with LEV previously (n = 42) or had an overnight switch to BRV (n = 60). The 50% responder rate was 32.6%, 21.7% had an increase in seizures. The 6 month retention rate was 80.4%.
A Spanish survey of 575 patients reported a 36% reduction of seizures after 12 months, a 50% responder rate of 39.7% after 12 months, and 17.5% seizure-free patients. 105
Clinical studies with LEV and BRV as monotherapy in patients with focal epilepsies
LEV
The international labeling of LEV as a monotherapy in focal epilepsies resulted from the paramount monotherapy trial that was performed following a completely new study design that now has been established as the gold standard for monotherapy trials in epilepsy treatment. 83 The basic concept of this design was not to look for statistically significant superiority in a comparative trial versus an established antiepileptic drug but to prove non-inferiority. In the case of LEV, controlled-release CBZ was used as the comparator. In adults with at least two newly onset focal or bilateral tonic-clonic seizures at baseline LEV 1000 mg daily (500 mg twice-daily.) was compared with 400 mg CBZ (200 mg twice-daily) with the option to titrate LEV up to 3000 mg daily and CBZ to 1200 mg daily, respectively, if seizures occurred during a 26 week maintenance period. Patients achieving the primary endpoint (6 month seizure freedom) continued the treatment for another 6 months. A total of 73% patients on LEV and 72.8% on CBZ were seizure-free at the last evaluated dose. Thus, the non-inferiority of LEV could be demonstrated. Similar proportions of patients in the LEV (79.6%) and in the CBZ (80.8%) groups experienced at least one adverse event. Adverse events were mostly mild or moderate. Withdrawal rates due to adverse events were 14.4% for LEV and 19.2% for CBZ, respectively. Depression and insomnia occurred more frequently with LEV than with CBZ.
Werhahn and colleagues carried out a randomized, double-blind, multicenter comparative monotherapy trial with LEV, controlled-release CBZ and LTG in 361 patients aged 60 years or older whose epilepsy was newly diagnosed. 84 Daily target doses were 1000 mg for LEV, 400 mg for controlled-release CBZ and 100 mg for LTG. At week 58, the retention rate for LEV was statistically significantly higher than for CBZ and similar to LTG. The main reason was the significantly higher rate of discontinuations due to adverse events, or death, with CBZ whereas LEV and LTG did again not differ significantly. The median daily doses of the 195 completers were 950 mg for LEV, 380 mg for CBZ, and 95 mg for LTG, respectively.
BRV
Larger studies with BRV as a in monotherapy have not yet been carried out, however, the first clinical reports are encouraging.106,107
Clinical studies with LEV and BRV in generalized epilepsies
LEV
The preclinical profile mentioned previously indicates that LEV might be effective in generalized epileptogenesis, too. 61
The efficacy and safety of LEV in patients with idiopathic generalized epilepsies with generalized tonic-clonic seizures were investigated in a randomized, placebo-controlled trial in adults and children aged between 4–65 years. 85 Patients with ongoing generalized tonic-clonic seizures in spite of adequate antiepileptic baseline therapy entered an 8 week baseline (4 weeks retrospective and 4 weeks prospective) and were randomized thereafter according to a 1:1 ratio. LEV was up titrated to 3000 mg daily during a 4 week titration period prior to a 20 week evaluation period. In total 164 patients were randomized (80 on LEV and 84 on placebo). The mean weekly reduction of generalized tonic-clonic seizures was 56.5% with LEV and 28.2% with placebo (p = 0.004). The responder rates were 72.2% with LEV versus 45.2% with placebo (p < 0.001). Seizure freedom concerning generalized tonic-clonic seizures was 34.2% with LEV and 10.7% with placebo (p < 0.001) and concerning all seizure types 24.1% versus 8.3% (p = 0.009). Only 1.3% of patients under add-on LEV withdrew from the study due to adverse events compared with 4.8% withdrawals due to adverse events with placebo. Somnolence was the most frequent adverse event.
Several studies and observations indicated a good efficacy against myoclonic jerks and seizures due to juvenile myoclonic epilepsy, progressive myoclonic epilepsies, post-anoxic myoclonus, and other forms of myoclonus.16,17,108–111 Therefore, efficacy and tolerability of LEV was investigated in a multicenter randomized, double-blind, placebo-controlled study as an add-on in patients with idiopathic generalized epilepsy with myoclonic seizures. 86 Patients with ongoing myoclonic seizures in spite of antiepileptic baseline medication aged between 12 and 65 years were recruited. Following an 8 week baseline, patients were randomized according to a 1:1 ratio. LEV was initiated at 1000 mg daily (500 mg twice-daily) and increased fortnightly by 1000 mg daily until the maintenance dose of 3000 mg daily was reached. The evaluation period lasted 12 weeks. During the first week, a fall back option down to 2000 mg LEV daily was allowed. Out of 144 patients, 120 were included for the efficacy analysis (60 each with LEV and with placebo, respectively). Out of the LEV patients 4.9% remained on 2000 mg daily. Responder rates concerning myoclonic seizures were 58.3% with LEV versus 23.3% with placebo (p < 0.001). Responder rates concerning all seizures were 56.7% versus 21.7% (p < 0.001). During the 12 week evaluation period, 25% of patients receiving LEV and 5% of patients with placebo were free from myoclonic seizures (p = 0.004) and 21.7% with LEV versus 1.7% with placebo were completely seizure-free (p < 0.001). Headache was the most common adverse event, but was similar with LEV and placebo. The most frequent adverse events which occurred more often with LEV than with placebo were somnolence, neck pain, and pharyngitis. Four patients withdrew due to treatment-emergent adverse events, three of them under LEV. Five patients experienced serious adverse events (four of them with LEV). None of them were considered to be related to this study medication.
The favorable efficacy and safety of LEV in generalized epilepsies was supported by further studies.112–115 Efficacy in absence epilepsy was described, though not statistically significantly different from placebo, in a small comparative trial. 116
Two large open-label randomized controlled trials compared LEV with either CBZ or valproate after assignments of newly diagnosed patients to either drug group (assuming that generalized epilepsies would most probably be assigned to valproate) 115 or with LTG covering both focal and generalized epilepsies. 114 Both studies supported the clinical value of LEV though they did not find evidence for the statistically significant superiority of LEV. LEV is not licensed for the monotherapy of idiopathic generalized epilepsies. Nevertheless, there little doubt about its principle efficacy as demonstrated by the studies mentioned previously.114,115 In spite of the off-label status in a survey among German epileptologists, 75% reported the use of LEV monotherapies in patients with generalized epilepsies. 117
BRV
As a small part of one of the pivotal phase III trials 91 patients with generalized epilepsies were included. BRV was given as add-on and titrated up to a maintenance dose between 50 mg and 150 mg daily during an 8 week dose finding period. In patients with generalized seizures only, the median percent reduction from baseline in generalized seizure days per week was 42.6% versus 20.7%, and the 50% responder rate was 44.4% versus 15.4%, respectively. In an open-label real-world survey in generalized epilepsies, add-on BRV off-label use was associated with a retention rate of 82% at 3 months and of 69% at 6 months. The 50% responder rate was 36% after 3 months. The best results were obtained in juvenile myoclonic epilepsy. 118
Two randomized controlled studies in Unverricht-Lundborg disease demonstrated high retention on BRV but not a statistically significant superiority over placebo. 119 Due to the small sample size and the use of LEV in many patients as a potential interfering factor further studies are required to evaluate BRV in progressive myoclonic epilepsies. 120
An observational survey in 44 patients with epileptic encephalopathies 121 reported a 12 month retention rate of 42%, a 3 month 50% responder rate of 27% with 9% seizure-free patients. However, three of these four patients had been seizure-free before and were treated with BRV more for tolerability reasons.
Clinical studies in status epilepticus
The availability of an intravenous formulation, the almost complete lack of interactions (at least for LEV), excellent tolerability, and the rapid entry across the blood-brain-barrier suggest that both LEV and BRV may be suitable anticonvulsant compounds in status epilepticus.
LEV
LEV is recommended as a second-line option,122,123 although the evidence from randomized controlled data is limited. 124 A recent randomized phase III trial did not show an advantage of the combination of clonazepam and LEV versus clonazepam and placebo. 125 Another randomized controlled prospective study investigated the efficacy and safety of phenytoin, valproate, and LEV in combination with lorazepam in a group of 50 patients. 126 The seizures were controlled in 68% with phenytoin and valproate, and in 78% with LEV. No statistically significant differences were found. In a prospective trial in 115 patients with ongoing status epilepticus after initial lorazepam, no difference between LEV and phenytoin were detected. LEV was effective in 82% of cases, and phenytoin in 73.3%. 127 Equal efficacy of LEV and phenytoin was also reported in another trial in 44 patients. 128 In a randomized controlled trial in 118 elderly patients with ongoing convulsive status epilepticus after initial intravenous lorazepam, LEV and valproate were likewise similarly effective. Seizure control was achieved in 68.3% of patients with valproate and in 74.1% under LEV. 129 The efficacy varied in a meta-analysis between 44% and 94%. 123 Its relative efficacy was 68.5% compared with 73.6% with phenobarbital, 50.2% with phenytoin, and 75.7% compared with valproate. 130 A recent study on status epilepticus in eight German and Austrian emergency units revealed that LEV is used as a first-line agent sporadically with inferior efficacy compared with benzodiazepines. 131
BRV
A retrospective survey of 11 patients with refractory status epilepticus reported a cessation of the status after the intravenous application of BRV in 27% of the cases. 132 Even better outcomes were reported in a series of less refractory status epilepticus at earlier stages. 133 In two further cases of absence status epilepticus BRV was not effective. 118
Side effects/adverse reactions and toxicology
LEV
In general, the safety profile of LEV as an add-on AED in patients with focal epilepsies was very promising . Several reviews on pooled data revealed that adverse reactions were often no different from those observed with add-on placebo. Adverse reactions were usually easily resolved by dose reduction or discontinuation.20,134–137 Three particular aspects of the side effect profile of LEV have been categorized: Asthenia/somnolence, coordination difficulties, and behavioral abnormalities/psychiatric adverse reactions. 136 During the controlled trials, the most commonly reported adverse reactions were somnolence (14.8% versus 8.4% in placebo), headache (13.7% versus 13.4% in placebo), infection (13.4% versus 7.5% in placebo), and dizziness (8.8% versus 4.1% in placebo).20,136 These adverse events typically occurred during the first month of treatment, and resolved over time and did not lead to discontinuation.20,135,136,137 Coordination difficulties including abnormal gait and ataxia were reported in 3.4% of patients with add-on LEV compared with 1.6% with placebo134,136 Behavioral adverse reactions are today rated as the most important potential drawback of treatment with LEV. 138 Interestingly, as mentioned above, this was not that apparent from the pivotal fixed-dose, randomized trials but later turned out to be the major drawback of LEV. In the LEV patients, 13.3% reported behavioral problems including agitation, hostility, anxiety, apathy, emotional lability, depersonalization, depression, or other behavioral symptoms, compared with 6.2% of patients in the placebo groups 136 Behavioral adverse events occur more often in children and adolescents than in adults: In a pediatric population, its incidence was 37.6% versus 18.6% in the placebo group. 138 Warnings and precautions in the summary of product characteristics meanwhile contains the wording: ‘Behavioral abnormalities including psychotic symptoms, suicidal ideation, irritability, and aggressive behavior have been observed. Monitor patients for psychiatric signs and symptoms’. 138
Only one randomized controlled trial addressed a behavior-specific endpoint (the anger-hostility subscale of the profile of mood states) to explore aggression with LEV. This study demonstrated that anger/hostility subscale scores were significantly worse with LEV relative to lamotrigine. 139 Observational trials confirmed the increased incidence of behavioral symptoms in patients treated with LEV 138 although in some instances positive changes like an improvement from anxiety and no significant changes in other aspects including a hostility subscale were also described. 140
One large, long-term comparative trial in 828 patients reported discontinuation due to behavioral adverse effects in 19% of 196 patients taking LEV, compared with 2–7% taking oxcarbazepine, lamotrigine, topiramate, and zonisamide. 141 In other studies, rates of individual behavioral adverse events with LEV ranged from 5% to 24%, 138 with the highest rate being the incidence of irritability in a retrospective chart review of 568 patients treated with LEV monotherapy/polytherapy at a tertiary epilepsy center. Discontinuations due to behavioral adverse effects, in general, were reported in 19% of patients. 142
In a small number of cases psychotic symptoms (0.7% versus 0.2% with placebo) or suicidal ideation (0.5% versus non in the placebo groups) occurred. 136 Again, as with other adverse reactions, a clear dose-relationship could not be identified.134,136
Serious adverse events with add-on LEV occurred in 14.7% of patients compared with 11.2% under placebo in the pivotal phase III trials. 20 Somnolence (3.1%), asthenia (1.6%), convulsions (1.6%), bilateral tonic-clonic seizures (1.0%), dizziness (0.7%), depression (0.7%), and personality disorders (0.5%) occurred more often in the LEV group. 136 Overall, 15% of LEV patients reduced or discontinued LEV due to adverse events.134,136
Leading adverse events in the two largest open-label phase IV trials, the KEEPER and the SKATE trial, were somnolence, dizziness, asthenia, and headache in the KEEPER trial 99 and somnolence, fatigue, dizziness and headache in the SKATE trial. 100 In both studies side effects were mild to moderate. Other large open-label studies confirmed the favorable adverse event profile of LEV.97,98 In a large open-label study comparing LEV with lamotrigine monotherapy 114 the most common adverse events with LEV were tiredness (32.8%), headache (23%), vertigo (17.2%), and upper respiratory tract infection (17.2%).
BRV
BRV was investigated according to randomized controlled trials in four phase III studies89–92 and two phase IIb studies.87,88 However, the most common adverse events in the phase II and III trials were almost not different from the placebo rates (see Table 1) which indicates the very good tolerability of BRV. In the phase III trial of Biton and colleagues 89 with daily BRV doses of 5 mg, 20 mg, and 50 mg, respectively, treatment-emergent adverse events with a frequency >3% higher than placebo for any dose of BRV comprised somnolence, dizziness, fatigue, influenza, insomnia, nasopharyngitis, vomiting, diarrhea, urinary tract infection, and nausea. Somnolence, dizziness, and fatigue were more often reported if higher doses up to 200 mg daily were used as in the phase III trial of Klein and colleagues 38 (see Table 2).
In the trial of Ryvlin and colleagues 90 with BRV daily maintenance doses of 20 mg, 50 mg, and 100 mg, respectively, headache, somnolence, dizziness, and fatigue were the most common adverse events. Psychiatric disorders that resulted in discontinuation in more than one patient were aggression, anxiety, irritability, depression, and insomnia in a single case.
Psychiatric disorders reported by ⩾1% of patients were insomnia (BRV 4% versus placebo 2%), depression (BRV 3.7% versus placebo 1%), irritability (BRV 3.7% versus placebo 2%), anxiety (BRV 1.7% versus placebo 1%), memory impairment (BRV 1.7% versus placebo 1%), agitation (BRV 1% versus placebo 0%), and depressed mood (BRV 1% versus placebo 0%).Irritability was seen in approximately 5% of patients with 50mg daily (versus 2–4% with placebo) in three of the four studies.88–90 The incidence of psychiatric adverse events was similar for BRV and placebo in the large trial of Kwan and colleagues 91 Discontinuation of BRV was most often necessary due to psychiatric adverse events including aggression and irritability in two studies.89,90 A post hoc meta-analysis across these phase II and III studies reported that 6.8% of 1214 BRV-treated patients had nonpsychotic behavioral adverse events compared with 4.2% in the placebo group (n = 425). This incidence is lower than across the phase III studies with LEV. 143 Another meta-analysis reported that the most frequent treatment-emergent adverse psychiatric events were irritability (3.2% versus 1.1% with placebo), insomnia (2.9% versus 1.5%), anxiety (2% versus 1.3%), and depression (2% versus 1.1%). 38 In the long-term, the leading psychiatric adverse events were depression (7.1%), insomnia (6.2%), irritability (5.2%), anxiety (4.9%), suicidal ideation (2%), depressed mood (1.8%), nervousness (1.6%), and sleep disorder (1.6%). 38 In a series of 101 patients treated with add-on BRV at doses between 50 mg and 400 mg daily treatment-emergent adverse events occurred in 37% of the patients. The leading adverse events were dizziness (16%) and somnolence (11%). Psychiatric adverse events only occurred in a single case. 56
Approximately the same adverse event experiences were reported in another real-world study in 262 patients 60 . Treatment-emergent adverse events occurred in 37.8% of patients. The most common adverse events were somnolence/sedation (16%), dizziness (11.8%), and behavioral adverse events with depressive mood change being the leading one (9.1%). In a cohort of 44 adult patients with epileptic encephalopathies, psychobehavioral adverse events were the most common with an incidence of 16%. 121 A large Spanish observational survey in 525 patients 105 reported an incidence of adverse events in 39.8% of patients. Psychiatric adverse events occurred in 14.3% of patients. Somnolence, irritability, and dizziness were the most reported adverse events. In total 39.7% of patients were switched from LEV to BRV according to a 10:1 or 15:1 ratio, 17% reported psychiatric adverse events and 5.7% discontinued BRV because of the events.
The high selectivity of BRV concerning the mode of action suggests that its clinical tolerability might be superior compared with LEV. 7 A small pilot study showed that epilepsy patients who experienced behavioral adverse events under LEV benefited from a switch to BRV. 144 In another series of 25 patients with drug-resistant epilepsy and psychiatric comorbidities, depression, and aggressive behavior were reported in 8% each under add-on BRV, but in 77% of patients who had psychiatric adverse events under LEV, this did not happen with BRV. 145 In a prospective controlled study in 37 patients anger levels, depression-anxiety and quality of life were assessed by standardized tools prior to and under BRV add-on treatment. Anger levels, mood scores and quality of life improved with BRV irrespective of prior use of LEV. The beneficial effects might have been influenced by the good seizure response due to BRV in this trial. 146 The lower incidence of psychiatric adverse events were confirmed by Villanueva and colleagues. 105 The majority of patients who were switched from LEV to BRV in two large observational post-marketing surveys60,104 reported improvements of tolerability. In children, an observational trial confirmed the results of surveys in adults. 103
Comparison between LEV and BRV trials
A meta-analysis of the randomized controlled trials with LEV and BRV in 1876 patients indicated that LEV might have a slightly higher efficacy with a lower probability of dizziness compared with BRV. 147 This conclusion somewhat reflects the authors’ practical experiences following the introduction of BRV. Controlled comparative trials have not to the authors’ knowledge been carried out.
Conclusion
With a unique mode of action, LEV has opened the door to a new and convincing treatment option for epilepsy. Due to its favorable profile concerning ease of use, almost complete lack of interactions, and excellent efficacy and tolerability it has been globally established as one of the leading AEDs. The development of BRV, its derivative, was completed some years later. Compared with LEV, BRV, that acts more selectively at the SV2A binding site, offers typically better tolerability in relation to psychiatric adverse events. The authors’, and other research, found that in patients with these adverse events, an immediate switch from LEV to BRV was easily achieved with a practical routine. The pharmacokinetics and the rapid entry into the CNS allows a very rapid titration and make LEV a suitable candidate for use in emergencies. Analyzing at the results from the phase II and III trials it can be speculated whether higher doses than the currently recommended ones may result in better efficacy. Further studies will have to be carried out to demonstrate such additional potential. To the best of the authors’ knowledge controlled comparative trials between LEV and BRV are missing, and it is currently not possible to answer the question of whether BRV might potentially replace LEV in the near future. From a clinical point of view and according to the authors’ clinical experience this appears doubtful, and strongly supports the need for additional reliable comparative data.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
Bernhard J Steinhoff has received speaker’s honoraria from Al-Jazeera, Desitin, Eisai, GW Pharmaceuticals, Hikma, Novartis, Sandoz, and UCB and has served as a paid consultant for Arvelle, Bial, B. Braun, Desitin, Eisai, GW Pharmaceuticals, and UCB.
Anke M. Staack has received speaker’s honoraria from Eisai, Desitin, and UCB.