
Abstract
The diagnosis of a glioblastoma is mainly made on the basis of their microscopic appearance with the additional determination of epigenetic as well as mutational analyses as deemed appropriate and taken into account in different centers. How far the recent discovery of tumor networks will stimulate novel treatments is a subject of intensive research. A tissue diagnosis is the mainstay. Regardless of age, patients should undergo a maximal safe resection. Magnetic resonance imaging is the surrogate parameter of choice for follow up. Patients should receive chemoradiotherapy with temozolomide with the radiation schedule adapted to performance status, age and tumor location. The use of temozolomide may be reconsidered according to methylguanine DNA methyltransferase (MGMT) promoter methylation status; patients with an active promoter may be subjected to a trial or further molecular work-up in order to potentially replace temozolomide; patients with an inactive (hypermethylated) MGMT promoter may be counseled for the co-treatment with the methylating and alkylating compound lomustine in addition to temozolomide. Tumor-treating fields are an additive option independent of the MGMT status. Determination of recurrence is still challenging. Patients with clinical or radiographic confirmed progression should be counseled for a second surgical intervention, that is, to reach another macroscopic removal of the tumor bulk or to obtain tissue for an updated molecular analysis. Immune therapeutic approaches may be dependent on tumor types and molecular signatures. In newly diagnosed and recurrent glioblastoma, bevacizumab prolongs progression-free survival without affecting overall survival in an unselected population of glioblastoma patients. Whether or not selection can be made on the basis of molecular or imaging parameters remains to be determined. Some patients may benefit from a second radiotherapy. In our view, the near future will provide support for translating the amazing progress in understanding the molecular background of glioblastoma in to more complex, but promising therapy concepts
Keywords
Background
Glioblastoma is a fatal disease with the majority of patients dying within 15–18 months from diagnosis, with less than 5% of patients alive at 5 years. 1 Even within the more favorable selected clinical trial patient population the 5-year survival rates are around 10%. 2 Age <50 years and a complete macroscopic tumor removal are associated with longer survival; on a molecular level these tumors often exhibit two favorable molecular aberrations: O6-methylguanine DNA methyltransferase (MGMT) promoter methylation2,3 or isocitrate dehydrogenase (IDH) mutation. 4 There is a large disconnect between enormously evolving preclinical concepts and a very limited clinical therapeutic armamentarium, which is somewhat resistant to the novel biological concepts, that is, to apply the available biomarkers for treatment decisions, and on the other hand easy to impact by nonconventional strategies, that is, by regionally different one-fits-all approaches with drugs like cannabis, valaciclovir or methadone.
Epidemiology
The incidence of primary brain tumors between 2007 and 2011 was 21.4 per 100,000 individuals, with an incidence of gliomas of 6.6 per 100,000 people of which about half were glioblastomas. 1 For reasons unknown, there is regional variability in the incidence. The rate for glioblastoma in Japan is <50% of that in Scandinavia or the United States. The incidence of glioblastoma in general increases with age, with the most pronounced increase in glioblastoma incidence (per 100,000 people) ranging from 0.15 in children and 0.41 in young adults to 13.1 in those aged 65–75 years and 15.0 in individuals between 75 and 84 years of age. 5
Risk factors
Overall, manageable risk factors are hardly known. Specifically, therapeutic radiation in long-term survivors seems to have a dose and volume dependent impact. 6 These doses are not reached with diagnostic doses of radiation, for example, by regular cranial computed tomographies (dose in the range of 1–3 milli Sievert, comparable with the annual environmental radiation exposure or a long-distance flight). Relevance of other factors, like cytomegalie virus infection or mobile phone use has not been confirmed. In addition to the well described familial tumor syndromes, there are genetic associations for example, rs4977756 in the cyclin-dependent kinase inhibitor 2A (CDKN2A) and the CDKN2B gene,7,8 a retinoic acid modulator CCDC26 on 8q24, 9 pleckstrin homology-like domain family B member 1 (PHLDB1) on 11q23.3, 10 the TP53 (cellular tumor antigen p53) polyadenylation site rs78378222 on 17p13.1, 11 and rs11979158 and rs2252586 in the epidermal growth factor receptor (EGFR) gene on chromosome 7 12 with a higher likelihood of glioblastoma in one family.
Also, telomerase reverse transcriptase (TERT) and telomerase RNA component (TERC), which are both involved in regulating telomere length, have been suggested as interesting candidate genes for increased glioma risk in genome-wide association studies.13,14
Overall, until now, there is no firm manageable risk factor, no screening test or prevention concept available for glioblastoma. In turn, there is not role for regular magnetic resonance imaging (MRI) scans in relatives of glioblastoma patients.
Biological considerations
Glioblastoma is a whole brain disease with a variable focal increase in proliferation generating a tumor mass, which then may become symptomatic. These days, more weight is put on the largely invisible, diffusely infiltrating part potentially consisting of a functional network of glioblastoma cells (and other brain cells) connected by transmembrane nanotubes (tumor microtubes or ‘TMs’). 15 In addition to the classical hallmarks, such as pathological angiogenesis, necrosis and the immunologically cold environment, 16 these networks not only provide a more stringent concept for the diffuse infiltrative growth, but may also serve as the long-awaited Achilles’ heel for this disease.
Basic requirement for diagnosis
The diagnosis of a glioblastoma is made tissue-based according to the most recent update of the World Health Organization (WHO) classification of brain tumors including immunohistochemistry and selected molecular tests. 17 Recently, a high-throughput methylation-based classifier 18 has been shown to effectively diagnose glioblastoma based on quantitative methylation classes. 19
Standard of care
Surgery
The standard of care for adult patients largely irrespective of age, but with a good performance status with radiographically suspected newly diagnosed glioblastoma is a maximal safe surgical resection. This may result in a stereotactic or open biopsy in some patients with tumors in eloquent areas or in a removal of all contrast-enhancing parts of the disease in adequate patients. The goal of a complete macroscopic resection may be reached with the help of intraoperative imaging 20 or fluorescence-guided visualization of tumor tissue with the aid of 5‑aminolevulinic acid.21,22 As long as the community is not prepared to complete a controlled trial on the relevance of resection at progression, we will base our recommendations for a second surgery on some pragmatism, the need for an updated molecular or tissue diagnosis in cases with molecular-directed treatment options, the need for reduction of global or focal intracranial pressure, local expertise and patient preference.
Radiotherapy
Radiotherapy, together with surgery, has been the mainstay treatment in the management of patients with glioblastoma since the 1970s and the combination of both doubles overall survival in patients with malignant gliomas.23,24 Little clinical progress was made over the past decades. The prognosis of patients with glioblastoma remains poor with median survival of ~14 months after adjuvant temozolomide-based radiochemotherapy2,25 with relevant predictive impact of inactivation of the methylguanine DNA methyltransferase gene promoter. 26 Local recurrence within 2.0 cm of the presurgical initial tumor margin is the main pattern of failure following treatment of glioblastoma;27,28 a biomarker helping to dissect responding patients is missing. Delineation of target volumes by metabolic imaging and more sophisticated MRI techniques with focus on tumor areas with a need for higher doses or better sparing of sensitive structures is in the center of most research to optimize radiotherapy. A second pillar with little news to report is the assessment of radiosensitizers. The third aspect at least in sites with the respective technical prerequisites is the emergence of heavy ion radiotherapy using carbon ions (CIR) and raster scanning technique demarcating a landmark development in the field of high precision radiotherapy. 28 High precision radiotherapy holds the promise in escalating the dose in the tumor and improving local control while sparing normal tissue. 26 However, previous data indicate that escalating the dose alone will not suffice to improve outcome in these radioresistant tumors in the clinic. Conceptually, precision radiotherapy is an effective therapy with intrinsic limitations in highly infiltrative disease. In our view, more weight may be put on integrating radiotherapy into current biological concepts, for example, into immunotherapy, for example, by understanding ‘remote’, so-called abscopal (bystander) effects. 29 As already discussed in the surgery section, implementation of novel radiation qualities or planning strategies would require controlled trials. Similarly, it is surprising to realize that despite many thousand patients being treated each year with radiation, molecular biomarkers to predict response are still lacking.30,31
Chemotherapy
To date, the landmark contribution of the European Organization for Research and Treatment of Cancer (EORTC) with the EORTC 26981 trial defines the standard of chemotherapy, that is concomitant treatment with temozolomide at 75 mg/m2 body surface, on empty stomach approximately 2 h prior to the radiotherapy session and fasting in the mornings or later after breakfast of nonradiation days. Adaption is made with treatment pauses according to blood counts and a Pneumocystis jirovecii pneumonia prophylaxis is recommended especially in lymphcytopenic individuals. There is a 4-week break and the chemotherapy is completed by six maintenance cycles of temozolomide on 5 out of 28 days at 150 mg (cycle 1) and at 200 mg (cycles 2–6)/m2 body surface adapted according to general and more specifically hematological tolerance.2,25 Again, supportive measures may include a PcJ prophylaxis and an antiemesis. Steroid use is regarded a negative factor for the efficacy of treatment.
Neither the adaption of the schedule, for example, 21/28 days or 7/14 days temozolomide in the maintenance phase32,33 nor the longer exposure 34 has a proven impact to date.
Impact of molecular diagnostics
According to the most recent adaption of the WHO classification, MGMT promoter methylation is predictive for efficacy and response to alkylating and methylating chemotherapy agents2,26 in glioblastoma. Long-term surviving patients have >90% glioblastoma with methylated MGMT promoter 2 versus 35% in the general glioblastoma patient population. 35
IDH1/2 mutations are relevant positive prognostic factors and in glioblastoma strongly associated with glioblastoma progressive from a lower grade glioma. 36 The existence of de novo IDH-mutated glioblastoma is a topic of controversy.
There is no consistent correlation of EGFR amplification with survival, largely irrespective of the age at clinical manifestation. The variant III of EGFR seems to get lost in the progression at east of a fraction of patients. 37 Loss of heterozygosity (LOH) 10q is the most frequent genetic alteration in glioblastoma and is associated with reduced survival. The presence of PTEN mutations is not associated with prognosis of glioblastoma patients.17,38
Adaptions/options to the standard in newly diagnosed patients
Elderly patients
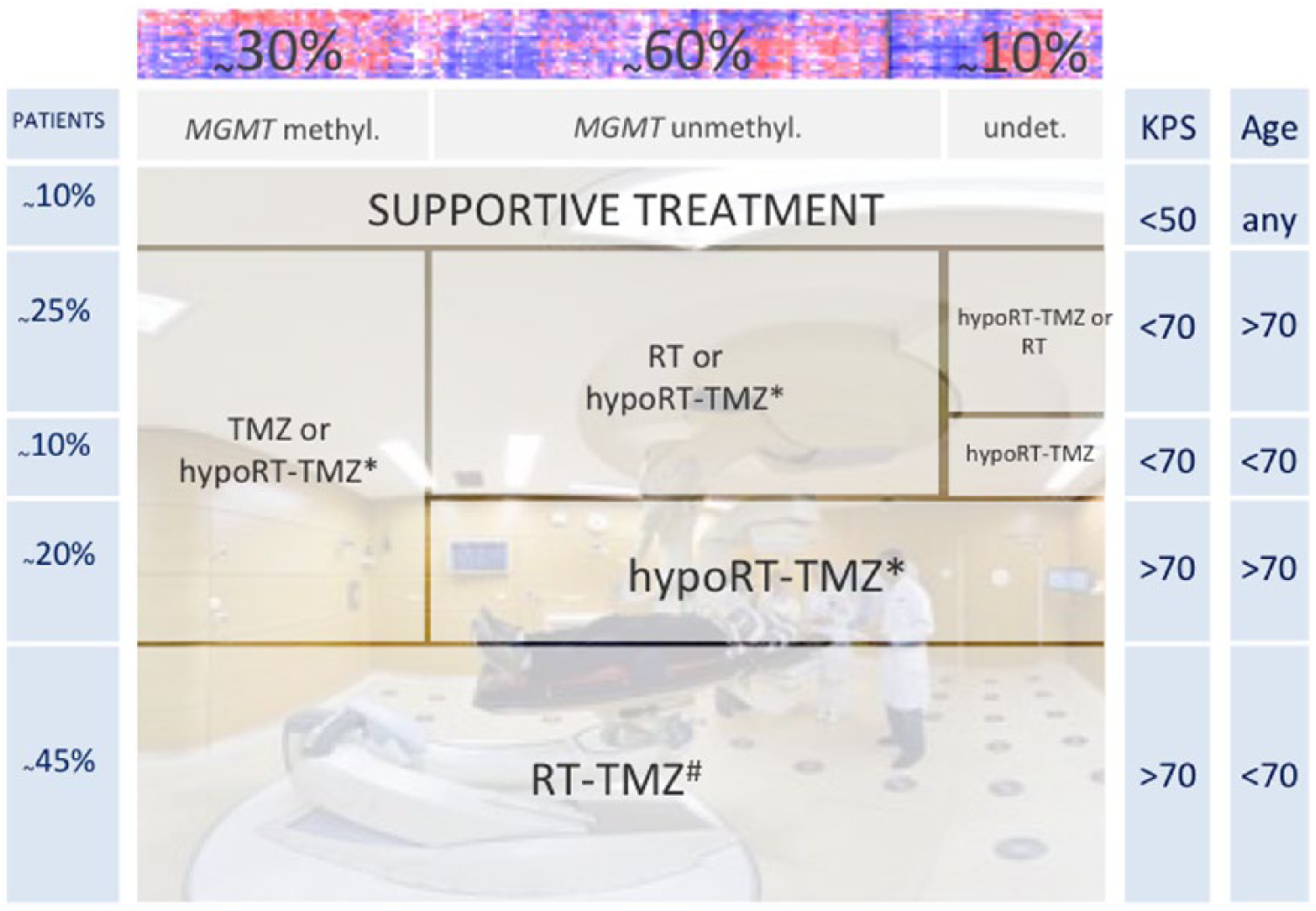
The Scandinavian Neuro Oncology Network, the Neurooncology Working Group of the German Cancer Society (NOA) as well as the CCTG (Canadian Cancer Trials Group) and the EORTC have provided randomized data for the treatment of elderly patients with glioblastoma. These trials provide evidence that hypofractionated radiotherapy over 3 weeks is equivalent to longer treatment and that chemoradiation using that shorter radiotherapy with temozolomide as well as maintenance temozolomide is superior to radiotherapy alone. 39 In the absence of comparative data between regular fractionated and hypofractionated chemoradiotherapy as well as a lack of these data compared with temozolomide alone leaves room for individualized treatment decisions based on clinical assumptions, but not data. Today, increased age (>65/70 years), relevant comorbidities, Karnofsky performance status (<70) and some considerations on frailty are used to provide guidance (Figure 1). Molecular testing is of some help. It has revealed a low prevalence of favorable prognostic markers in elderly patients. 40 The virtual absence of IDH mutations in patients over the age of 65, according to the new WHO classification, suggest that differential prognosis is not based solely on age but rather that separate entities exist with a distinct age distribution. 38 The prevalence of MGMT promoter methylation is similar to that in younger patients. Specifically, in the elderly patients a string call was made for the use of MGMT as a predictive biomarker.26,39
Treatment according to MGMT
Current (European) guidelines are explicit that only in elderly or frail patients the use of temozolomide can be adapted according to the methylation of the O6-methylguanin DNA meth-yltransferase gene promoter. Otherwise, MGMT testing though performed with increasing frequency has no practical impact in the management of patients. Some centers take recent data on the MGMT-dependence of response to temozolomide 43 or lomustine 44 at glioblastoma progression as decisive to not expose patients again to alkylating or methylating chemotherapies at progression, but this concept is neither generally supported nor explicitly stated in our guidelines. Trials in patients without MGMT promoter methylation 26 showed that leaving out temozolomide from first-line treatment was of no detriment to patients, challenging the view that temozolomide should be used in every patient despite the absence of MGMT promoter methylation. Recent data might further help to decipher the benefitting patient population. TERT expression may be necessary to ensure the MGMT methylation related benefit to alkylating chemotherapy. 45 Overall, MGMT status testing without taking consequences is unsettling for patients, creates a lot of second consulting and finally undermines trust in our profession. On the other hand, testing offers the opportunity to safe patients a treatment with no or little chances for help plus offers options for alternatives, which should be based on further precision measures by looking for molecular lesions potentially relevant for targeted or immunotherapies (see Outlook). This should be avoided in patients <70 years without the patient-physician team willing to take any consequences.
Use of tumor-treating fields
Tumor-treating fields (TTFields) use alternating electrical fields to inhibit mitoses via disruption of the spindle apparatus. In a randomized trial that was published originally in JAMA, the addition of TTFields to standard radiotherapy (RT) and temozolomide (TMZ) in newly diagnosed glioblastoma extended overall survival [hazard ratio (HR), 0.64 (99.4% confidence interval (CI), 0.42–0.98); p = 0.004]. 46 The effect of the fields is maintained at long-term (final) analysis, 47 though the selected patient group, the lack of a control for the more active supportive care and the relatively small difference in long-term survival at 5 years compared with the EORTC trial 2 raised questions in the ‘expert’ community. Whether the magnitude of overall survival increase outweighs the individual burden and the societal cost is yet to be determined. The long-term relevance of the fields will be determined by whether they are routinely integrated into daily practice and the success (or not) of other concepts discussed below.
Concepts at recurrence
Re-surgery
As already stated above, we might consider reoperation to improve symptoms, in the case of early progression in patients in whom initial surgery was not adequate or later progressors, when the initial treatment might just be repeated. We are uncertain about the effect of second surgery on overall survival. It is considered that another gross total resection of enhancing tumor 48 is relevant, but prospective controlled data are lacking. Recently, there is an increasing demand for post-progression tissue extraction as targeted treatments may offer valid options and also therapy with checkpoint inhibitors 49 should be restricted to patients with the most likely benefit.
Re-radiotherapy
The efficacy of re-irradiation is uncertain until date. Its appreciation varies between sites, countries, recurrence pattern and with the time interval to the first treatment. Fractionation depends on tumor size. Fractionation between 2.0 and 2.4 Gy has been tested, but also higher doses per fraction of 5–6 Gy using stereotactic hypofractionated radiotherapy to a total dose of 30–36 Gy, and also radiosurgery with a single dose of 15–20 Gy. Overall toxicity seems not to be the main issue. 50 As with systemic therapies, there is a lack of relevant efficacy, for example, progression-free survival rate of 3.8% at 6 months in the APG101 randomized trial at 18 fractions of 2 Gy. 51 There is a clear need of a definition for a population candidate for re-irradiation, research on biomarkers involved in radioresistance 52 and also trial concepts that provide controlled information on whether or not this is a reasonable approach. The aforementioned applies to conventional photon therapy and may or may not be challenged if different radiation qualities, like C 12 ions or protons are being used.
Chemotherapy at progression
Most studies at progression are of limited size therefore impacted by the heterogeneity of the disease, non-comparative or fail to use a control arm lacking the experimental drug. In addition to re-exposure to temozolomide at standard dose, most patients will receive one of the nitrosoureas, that is, carmustine (BCNU), lomustine (CCNU), or fotemustine. They alkylate at the N7 and O6 positions of guanine and introduce interstrand crosslinks as well as act by carbamoylation of amino acids interfering with transcriptional, translational and posttransscriptional processes.53–56 These are DNA alkylating and methylating agents that cross the blood–brain barrier and have been extensively used in glioma treatment. They may induce considerable hematological toxicity with long-lasting bone marrow suppression, liver and renal toxicity, and, specifically carmustine, interstitial lung disease. Efficacy is dependent on MGMT status both in the AVAREG trial 57 and also in the EORTC 26101 trial. 44 At the same level, temozolomide re-exposure is only meaningful if patients are diagnosed with a progressive glioblastoma harboring a methylated MGMT promoter. 43 It may be extrapolated from the BR12 trial that used standard dose and dose-intensified temozolomide after radiotherapy alone (and not re-challenge after temozolomide) 58 and the dose-dense maintenance treatment of RTOG 0525 32 that conventional (5 out of 28 days) chemotherapy is not inferior to any dose-intensification 43 and the latter may not be used unless new data appear.
Experimental options at progression
Certainly, many treatments can be tried in patients with progressive glioblastoma after the above mentioned. As present, we would recommend trial participation. Also, performance status and the general situation are impacting options. In the United States, bevacizumab is approved and may offer a further treatment line with the promise of prolonging progression-free survival and potentially in selected patients also overall survival. In the European Union, this option is very restricted due to a lack of approval. Here, we recommend a pragmatic approach that involves obtaining post-progression tissue and assess for potential molecularly informed treatment decisions. 59 The fields although sometimes advertised differently did not hold the promise at progression therapy. 60
Outlook
Antiangiogenesis
After the failure of bevacizumab to demonstrate an effect on overall survival in newly diagnosed patients, 61 the subsequent randomized, phase III EORTC 26101 compared lomustine with or without bevacizumab at progression. Despite prolonging progression-free survival (HR 0.49; CI 0.39, 0.61), combined lomustine and bevacizumab treatment does not confer an overall survival advantage (HR 0.95; CI 0.74, 1.21; p = 0.650) over treatment with lomustine alone in patients with progressive glioblastoma. 44 In this study, crossover to bevacizumab occurred in 35.5% of patients in the control arm; whereas 18.7% of patients in the combination arm continued bevacizumab at progression. However, bevacizumab continues to play a role in the treatment of glioblastoma in large areas of the world. Many practicing clinicians regard its positive effect on progression-free survival, and other palliative effects, and neurological improvement seen in many patients as meaningful benefits, in the absence of any overall survival gain in the entire patient population. Pragmatically, bevacizumab with its documented beneficial effect on radionecrosis-related edema and neurological dysfunction 62 might be particular interesting for patients with radiological and clinical deterioration, frequently called ‘pseudoprogression’.
Immunotherapy
Immunotherapy is regarded a valid option for patients with glioblastoma though data to prove this hypothesis are largely confined to case reports and by analogy to the successes in other malignancies. Independent of the approach (e.g. checkpoint inhibition, targeted vaccine, adoptive T-cell transfer), the clonal representation of the target antigen and the immunosuppressive microenvironment have to be taken into account for clinical development. For instance, EGFR vIII is a subclonal antigen with heterogeneous expression in the tumor tissue, which may, in theory, be subjected to immune evasion. Despite promising initial data, a large phase III trial failed. 37 VXM01 is encoding vascular endothelium growth factor receptor 2 (VEGFR2) in order to evoke an immune response specifically directed against the tumor vasculature. It is currently in clinical development as a treatment for solid cancer types. The oral T-cell vaccine platform of the company VAXIMM is based on the approved, live attenuated Salmonella typhi vaccine strain Ty21a, which has been applied in millions of individuals for prophylactic vaccination against typhoid fever. 63 IDH1R132H 64 and H3.3K27M 65 as early founder mutations represent clonal antigens, but controlled clinical data on their relevance are yet to be generated. The Glioma Actively Personalized Vaccine Consortium (GAPVAC) realized an immunotherapy, for which the selection of actively personalized peptide vaccines (APVAC) for treatment of newly diagnosed glioblastoma was based not only on whole-exome sequencing but also on human leukocyte antigen (HLA)-ligandome analyses providing information of the actual presentation of relevant epitopes in the tumor. Mutated peptides identified by next generation sequencing and mass spectrometry may not only be used for peptide vaccination, but serve as a platform for personalized immunotherapies with potentially more aggressive cell-based treatments. Controlled clinical trials assess the efficacy of nivolumab in progressive and newly diagnosed glioblastoma. Whereas the trials in newly diagnosed patients separated according to MGMT promoter methylation status are ongoing, results from the study in progressive glioblastoma comparing nivolumab and bevacizumab have been reported. A total of 369 patients, progressive after standard of care, were randomized to nivolumab 3 mg/kg every 2 weeks (n = 184) or bevacizumab 10 mg/kg every 2 weeks (n = 185). Progression-free survival was superior in the bevacizumab arm (HR = 1.97; 1.57, 2.48) with medians of 3.5 months (2.9, 4.6) and 1.5 months (1.5, 1.6), respectively. There was no signal for any difference in overall survival in this unselected patient population (HR = 1.04; 0.83, 1.30; p = 0.76) with medians of 10.0 months (9.0, 11.8) for bevacizumab and 9.8 months (8.2, 11.8) for nivolumab. 66 Nivolumab or temozolomide in combination with radiotherapy in newly diagnosed patients with MGMT-unmethylated glioblastoma are treated in CheckMate 498. CheckMate 548 assesses nivolumab or placebo in combination with radiotherapy and temozolomide in patients with MGMT-methylated or indeterminate glioblastoma at first diagnosis. These trials also do not enrich for patients more likely to benefit from the immune intervention. 67
Checkpoint inhibitors in glioblastoma may work only with a specific immunogenic background, potentially to be defined by MSI-H or dMMR, or with associated treatment, for example,vaccination. The most prominent checkpoints in other malignancies may not be the most relevant in glioblastoma; 68 other factors like the CD95 system, tryptophan-2,3-dioxygenase (TDO)69,70 or other programmed death family members 71 may be of greater importance. In addition to being restrictive based on molecular stratification, there are concepts in development that promise a stronger immunoeffect. Several chimeric antigen receptors are in clinical development for glioblastoma. The currently available data are for interleukin 13 receptor (IL13R)-α2, EGFR variant III, and HER2 as targets. There are already cases and small series showing feasibility of delivery and manageable toxicity, 72 but translational research regarding efficacy and resistance mechanisms are ongoing.73,74
Targeted treatments
Biomarkers that predict response and ultimately benefit from a given therapy plus an effective treatment are the cornerstones of precision neuro-oncology. MGMT is a good example for a predictive biomarker in the field of gliomas.26,41 However, no officially accepted (accredited) test exists. Further, it is possible that predicting response to temozolomide is more complex than by just determining MGMT methylation status. The delineation of the right subgroups may also involve global methylation profiles and TERT status.75,5
Please find a strategy for treatment of newly diagnosed or recurrent glioblastoma and examples of putative predictive biomarkers in Figure 2. Importantly, the prerequisite until now is a tissue sample from the tumor that needs treatment (and not just archival information).

Sketch to show a way towards precision. Putative work flow from a glioblastoma tissue sample.
Further, there are interesting examples of drug repurposing with less intuitive compounds for the glioblastoma field. Also, these compounds may deserve testing in an otherwise difficult clinical situation and with indicative biomarkers associated (Table 1). In a pilot series that serves as model for the examples provided in the current review, compounds were recommended in combinations, following the concept that blocking multiple pathways with combination therapy may be more effective than single agent therapy especially when treating recurrent, progressive glioblastoma. 59

IDH, isocitrate dehydrogenase; MEK, mitogen-activated protein kinase; PARP, poly(ADP-ribose)-polymerase; VEGF vascular endothelial growth factor
Therefore, well-considered allocation of newly diagnosed as well as progressive patients to clinical trials based on molecular characteristics of the tumor as well as necessary retrospective validation of potential biomarkers are essential in a clinical setting. A current concept prospectively using biomarkers to enrich for potentially benefitting patients is the Nationales Centrum für Tumorerkrankungen (NCT) Neuro Master Match (N2M2), a trial of molecularly matched targeted therapies plus radiotherapy in patients with newly diagnosed glioblastoma without MGMT promoter methylation. 76 The Glioblastoma Adaptive, Global, Innovative Learning Environment (AGILE) consortium is planning to take a differential approach by reassessing potential biomarkers from an unselected cohort with given therapies first and integrating these information via adaptive processes to enrich while the trial accrues. 77