
Abstract
Imaging plays several key roles in managing brain tumors, including diagnosis, prognosis, and treatment response assessment. Ongoing challenges remain as new therapies emerge and there are urgent needs to find accurate and clinically feasible methods to noninvasively evaluate brain tumors before and after treatment. This review aims to provide an overview of several advanced imaging modalities including magnetic resonance imaging and positron emission tomography (PET), including advances in new PET agents, and summarize several key areas of their applications, including improving the accuracy of diagnosis and addressing the challenging clinical problems such as evaluation of pseudoprogression and anti-angiogenic therapy, and rising challenges of imaging with immunotherapy.
Keywords
Introduction
The roles of imaging in neuro-oncology primarily consist of diagnosis, prognosis, and treatment response assessment of central nervous system (CNS) tumors. Imaging assessment is currently an important surrogate endpoint for clinical trials. With ongoing evaluation and discovery of novel treatment agents, including immunotherapy agents, the ability to accurately assess progression and discern treatment-related changes is a central goal of neuro-oncologic imaging. In this review, we will summarize several clinically available imaging techniques as well as some novel methods under development, and provide an up-to-date review of some clinical challenges in treatment of glioblastomas where imaging can have important roles.
Update of advanced imaging techniques in neuro-oncology
Diffusion-weighted magnetic resonance imaging (DW-MRI) can characterize tissues based on the differences in the degree of free movement of protons. It has been shown that the cellularity or cell density of tumor is associated with apparent diffusion coefficient (ADC), a calculated metric from DW-MRI. 1 This property allows one to distinguish between both tumor subtypes and tumor grades (low versus high). More recently, high b-value DW-MRI, using a b-value >3000 s/mm2, has been demonstrated to be superior to standard DW-MRI in distinguishing tumor tissue from normal brain parenchyma. 2 DW-MRI data can also be further quantified to generate imaging markers using techniques such as diffusion kurtosis imaging (DKI), 3 histogram curve-fitting, 4 and functional diffusion map (fDM). 5 Restriction spectrum imaging (RSI) is an DW-MRI technique that can isolate the diffusion properties of tumor cells from extracellular process such as edema, potentially improving specificity of tumor detection and characterization. 6 Diffusion tensor imaging (DTI) measures the directionality of proton motion as fractional anisotropy (FA), which is often altered in the presence of brain tumors. 7 Applications of these methods will be reviewed in the following sections.
Perfusion-weighted magnetic resonance imaging (PW-MRI) techniques assess blood flow to tissue by calculating parameters derived from the time–intensity curve. Using the normal brain as reference, these techniques can detect pathological alterations of tissue vascularity that commonly occur among brain tumors due to increased vascular permeability as well as intravascular blood volume because of tumor-induced angiogenesis. Dynamic susceptibility contrast magnetic resonance imaging (DSC-MRI) quantifies first-pass bolus of paramagnetic contrast agent,8,9 and is currently the most common perfusion-weighted imaging method in clinical use. Dynamic contrast enhanced magnetic resonance imaging (DCE-MRI) can characterize vascular permeability within or surrounding tumors by using pharmacokinetic models to quantify the movement of contrast agents crossing the blood–brain barrier.10–12 DCE-MRI has an advantage over DSC-MRI due to its greater signal-to-noise ratio and spatial resolution, although imaging acquisition time is also longer. Perfusion imaging measurements are highly dependent on imaging acquisition parameters and postprocessing techniques, including variations in postprocessing software tools. 13 Clinical application of this technique therefore requires efforts in standardization, particularly in multicenter settings.
Magnetic resonance spectroscopy (MRS) measures concentrations of metabolites within tissues noninvasively. 14 The single-voxel spectroscopy (SVS) method collects average MRS data within a target region of interest selected on standard MRI images. The multivoxel spectroscopy (MVS) method can obtain two- or three-dimensional maps of the region of interest to detect voxel-wise spatial changes of specific metabolites. Both SVS and MVS approaches have been evaluated in tumor diagnosis, grading, pre-therapy planning and post-therapy assessment. One major limitation of the technique is its operator dependency, requiring experienced staff to manually select regions of interest during acquisition. It is also less sensitive to lesions with volume <1.5 cm3.
18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) is an important imaging tool in oncology. 15 Similar to systemic cancers, brain tumors often exhibit increased metabolic activity resulting in elevated 18F-FDG uptake that can be detected by PET. 16 The role of FDG-PET in brain tumor imaging, however, has been quite limited due to its relative lack of specificity and high background uptake by the normal brain. This limitation is particularly important for small lesions, as currently the resolution of PET imaging is limited to 5 mm. More recently, amino acid PET tracers including 11 C-methionine, 18F-fluorothymidine (FLT), 18F-fluoro-ethyl-tyrosine (FET), and 18F-dihydroxyphenylalanine (DOPA) have been developed and evaluated for brain tumor imaging. This class of radiotracers is avidly taken up by malignant brain tumors that have higher cellular proliferation compared to the normal brain.17–20 The advantage of high lesion-to-background uptake ratio makes amino acid PET suitable for imaging of brain tumors, including applications such as predicting tumor grade, detecting recurrent tumor, and assessing treatment response. Novel PET radiotracer (18)F-fluoromisonidazole (18F-FMISO) has been evaluated as a marker of tissue hypoxia before and after treatment.21,22
With increasing computing speed and availability of pre-engineered algorithms, imaging data can be analyzed for voxel-level intensity variations to generate texture-type features that can be correlated with tumor biology or treatment response. This approach can be applied to any imaging modality individually or simultaneously through spatial co-registration. As a result, imaging features can be regarded as tumor phenotypes and this type of biomarker can be summarized by the term ‘radiomics’. 23 Screening or combining a large number of radiomic features allows generation of models that can aid oncologic diagnosis, prognostication, and treatment response prediction. This approach has been successful in a number of systemic cancers.24–28 The radiomic approach is particularly suitable for evaluating high-grade gliomas, a tumor type that is well known for its genetic heterogeneity and highly complex imaging phenotypes.
Preoperative evaluation of brain tumor: diagnosis and prognosis
Imaging plays a key role in the diagnosis of brain tumors and has become one routine management step during preoperative evaluation to aid determination of tumor grade and prognosis. It can also provide important spatial information on tumor tissue characteristics for some tumor subtypes that can influence surgical and radiation treatment planning. In addition, imaging has shown increasing ability to detect tumor genetic profile that can further provide valuable prognostic and predictive information for optimal treatment planning. Finally, imaging findings are often combined with clinical data such as age, gender, and presenting symptoms and signs to increase the accuracy of diagnosis for various tumor types, as well as identifying non-tumor mimics.
One common clinical dilemma during preoperative diagnosis of brain tumors is to distinguish between high-grade glioma and lymphoma. Standard management of CNS lymphoma is nonsurgical and biopsy is the preferred approach if lymphoma is suspected preoperatively, whereas maximal surgical resection provides the best prognosis for high-grade glioma. On conventional imaging sequences, these tumor types commonly exhibit contrast enhancement and peritumoral edema, which make it challenging to differentiate. Lymphomas typically exhibit low ADC values due to high cellularity.29,30 However, this histological feature can be seen in high-grade gliomas and metastases.
Quantitatively, the FA and ADC values of primary cerebral lymphoma are significantly lower than those of glioblastoma.31,32 There is also evidence that DSC-MRI and DCE-MRI parameters of the enhancing regions of the tumor can discriminate between lymphomas and glioblastomas as well as between lymphomas and metastasis,32,33 although a direct comparison of DCE-MRI and DW-MRI shows that ADC measurement is superior to DCE-MRI in differentiating the two tumor types. 34 Detection of intratumoral microhemorrhage using the susceptibility-sensitive MRI technique also allows differentiation of glioblastoma and primary CNS lymphomas. 35 Texture features generated from post-contrast images of lymphoma and glioblastoma also allow diagnostic differentiation. 36
Analysis of nonenhancing signal abnormalities surrounding brain lesions can provide independent diagnostic information. ADC values measured within fluid-attenuated inversion recovery (FLAIR) abnormalities surrounding the enhancing regions can differentiate high-grade gliomas from solitary metastases.37,38 The difference could be due to the presence of tumor infiltration by glioma, resulting in higher cellularity than tumor-induced edema. 39 This is also supported by MRS and DSC-MRI measurements of the peritumoral region showing higher choline to N-acetylaspartic acid (NAA) ratio and greater vascularity among high-grade gliomas compared to brain metastases.32,40,41 Combined evaluation of both the enhancing and nonenhancing regions can potentially enhance diagnostic accuracy.32,42 Beyond the margins of signal abnormalities outlined by conventional MRI, including T1- and T2-weighted imaging, MRS can identify regions of brain containing tumor and improve surgical resection and patient outcome.43,44
Molecular data of gliomas have demonstrated prognostic significance and have been incorporated into the 2016 World Health Organization (WHO) criteria. 45 The imaging characteristics of brain tumors can be directly related to a specific set of tumor genomics, providing opportunities to noninvasively predict tumor genotype preoperatively. Radiomic models have been developed based on conventional MRI, DTI, and DSC-MRI for predicting gene expression profiles of newly diagnosed glioblastomas. 46 Specific genetic alterations of tumors can also be predicted by analysis of MRI data and predictive models have been generated for O6-methylguanine-DNA methyltransferase (MGMT) methylation status,47,48 epidermal growth factor (EGFR) amplification status,25,49 and EGFR receptor variant III status. 50 Isocitrate dehydrogenase 1/2 (IDH) mutations are commonly present in low-grade gliomas as well as secondary glioblastomas. These mutant tumors accumulate 2-hydroxyglutarate (2HG), an onco-metabolite that can be detected by MRS (Figure 1). 51 Measurement of 2HG concentration allows diagnosis of IDH mutant tumor preoperatively and also opportunities to monitor tumor activity during treatment.52,53 Static and dynamic FET-PET measurements have also been correlated with IDH and 1p/19q status. 54 More recently, multimodal MRI imaging can be evaluated by machine learning algorithms to generate predictive models for IDH status in gliomas.55–57
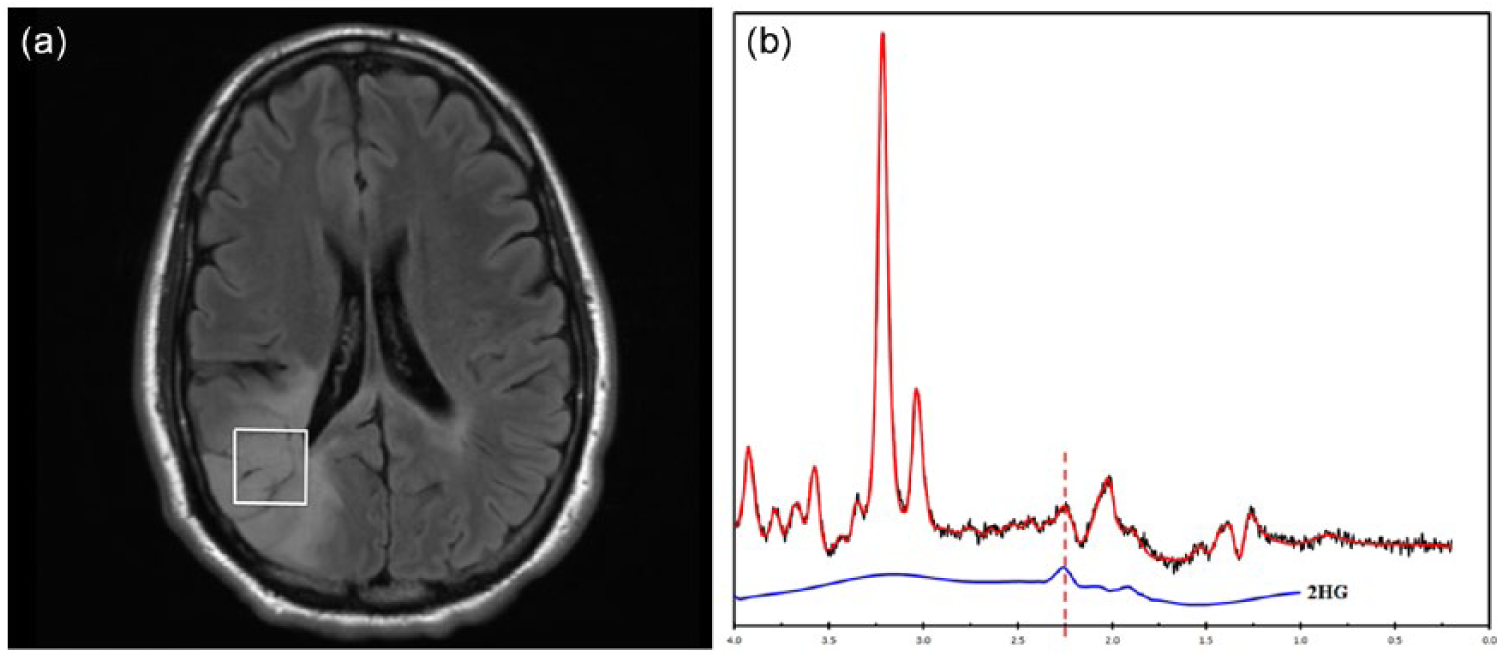
2-hydroxyglutarate (2HG) magnetic resonance spectroscopy. (a) Axial FLAIR image of a 34-year-old woman with a right parietal lobe nonenhancing mass. (b) Single-voxel magnetic resonance performed at 3T, TE of 97 ms, demonstrates a peak at 2.3 ppm (dashed line), indicating presence of 2HG.
Prognosis and tumor-grading
A prognostic imaging marker can be identified by correlating the marker with histological grading of the tumor or with patients’ clinical outcomes. With its noninvasive nature, imaging prognosticators can benefit patient care throughout the clinical course of disease, most importantly at the time of diagnosis for surgical or radiation planning, as well as early after treatment to determine efficacy. In patients with glioblastomas, the most common malignant primary brain tumors, the median survival is 14–16 months with best available standard treatment. 58 The ability to predict progression-free or overall-survival outcomes for these patients can impact their treatment decision-making.
Compared to low-grade gliomas, high-grade gliomas demonstrate higher cellularity on DW-MRI,59,60 higher choline to NAA ratio on MRS,60–64 high relative blood volume on DSC-MRI,60,65,66 and increased uptakes on FDG and FLT PET.67–69 Increased time activity curves of FET in tumor cells also have been shown to correlate with high-grade tumor.70,71 Radiomic models predicting WHO grade of gliomas have been generated using conventional MRI sequences. 72
For glioblastomas, a number of imaging modalities can provide prognostic information of overall survival, including DSC-MRI,73–75 DCE-MRI, 76 high b-value DW-MRI, 77 and FET-PET. Early time to peak on time activity curves of FET-PET has been shown to correlate with worse outcome in patients with high-grade glioma. 70 Furthermore, longer median time to peak was found to correlate with better outcomes with FET-PET in IDH1/2 mutant and1p/19q non co-deleted subgroup of patients with glioma. 71 Multiparametric volumetric analysis combining data from diffusion and perfusion imaging of patients with glioblastomas can predict survival. 78 A prospective evaluation of several imaging modalities including DCE-MRI, DSC-MRI, and 18F-FMISO PET prior to standard chemoradiation treatment in newly diagnosed glioblastoma revealed poor prognosis associated with increased tumor perfusion, vascular volume, vascular permeability, and hypoxia. 22 Prognostic models based on radiomic features have been generated from preoperative imaging of newly diagnosed glioblastomas.46,79–86
Imaging can provide location-specific diagnostic or prognostic information within brain tumors to identify regions associated with higher tumor grade, high risk of recurrence, or poor survival. It can also have a valuable role during preoperative and preradiation planning, as well as intraoperative imaging guidance. For example, choline to NAA ratio measured by MRS can localize the site within the tumor with the highest cellularity, which can be targeted for biopsy87,88 and gamma knife radiosurgery. 89 Applying machine learning algorithms to multiparametric MRI data, several groups have developed voxel-based models to classify glioma into tissues of different tumor grades or tumor cell density, verified by subsequent histological analysis.90,91 MRI features extracted from tumor and peritumoral tissues have been used to build models that can identify high-risk sites for tumor recurrence. 92 Dynamic FET-PET has been shown to help stratify prognosis, with 18 F-FET positive gliomas with decreasing time activity curves in kinetic analysis showing shorter progression-free survival and faster malignant transformation. 93 Furthermore, FET-PET is useful in biopsy planning, with focal regions of high-grade FET kinetics or ‘hot spots’ on FET-PET correlating with increased diagnostic yield for stereotactic core needle biopsy and also correlating with higher tumor grade. 94
Prediction of patient outcome prior to antiangiogenic treatment
Two phase III clinical trials have revealed no significant survival advantage when bevacizumab, an antibody targeting vascular endothelial factor (VEGF), was added to the standard treatment for patients with newly diagnosed glioblastoma.95,96 There is a need to identify pretreatment predictive markers that can accurately identify patients who may benefit from antiangiogenic treatment.
ADC histogram analysis of MRI imaging data of recurrent glioblastoma performed prior to anti-VEGF therapy has been shown to predict response and survival based on several retrospective studies,97,98 as well as evaluation of imaging data from several phase II trials. 99 Pretreatment DSC-MRI has also been shown to correlate with survival outcome for patients with recurrent glioblastoma receiving bevacizumab.100,101 Radiomic evaluations using multiparametric MRI data have identified pretreatment prognostic imaging features for overall survival.102–106
Response assessment and treatment monitoring
Pseudoprogression versus true progression in glioblastomas
Following standard-of-care upfront treatment including maximal safe resection, radiation with adjuvant temozolomide, 20–30% of patients with glioblastoma develop increased contrast enhancement within 3 months from end of radiation treatment that resolves without changes in treatment. 107 If patients with pseudoprogression were treated the same way as the true progressors, they may not continue to receive potentially beneficial adjuvant temozolomide chemotherapy and may be inappropriately included in trials of progressive/recurrent glioma. 107 To mitigate this problem, the Response Assessment in Neuro-Oncology (RANO) criteria require a minimum of 12 weeks after completion of radiation treatment before tumor progression can be confirmed unless the site of progressive disease is distant from the radiation field or there is pathologic evidence of progressive/recurrent tumor. 107 In a phase III trial of bevacizumab or placebo plus radiotherapy/temozolomide for newly diagnosed glioblastoma (AVAglio), 9.3% had confirmed pseudoprogression in the placebo arm, 108 indicating that the incidence of pseudoprogression appears lower than initially reported. Nevertheless, pseudoprogression can affect progression assessment in a small but non-negligible number of patients. In actual clinical practice, it remains a challenge to determine the true status of tumors that show early apparent progression based on conventional imaging assessment. In recent years, there have been tremendous efforts in discovering and applying advanced imaging techniques to improve the diagnosis of pseudoprogression.
Compared to normal brain tissue or necrosis, recurrent or progressive tumor more commonly demonstrates lower ADC values.109,110 Voxel-wise analysis of ADC maps can differentiate pseudoprogression from true progression in glioblastoma using ADC parametric response maps. 111 High b-value DW-MRI appears to improve the accuracy of diagnosing pseudoprogression compared to standard DW-MRI. 112
A number of prior studies have examined the ability of DSC-MRI to distinguish pseudoprogression from tumor progression in glioblastoma.113–117 Compared to true tumor progression, treatment-related necrosis or pseudoprogression exhibits lower relative blood volume (Figure 2). DCE-MRI can also differentiate tumor progression from radiation necrosis,118–120 although there is also evidence that there is no significant difference between DSC-MRI and DCE-MRI when either is added to standard MRI. 121 Parameters derived from combined approaches including DTI and DSC can classify tissues into true progressive tumor, treatment necrosis, and mixed response. 122

A 62-year-old man with glioblastoma treated by concomitant temozolomide and radiation. Axial gadolinium-enhanced T1-weighted (a) and fluid-attenuated inversion recovery (FLAIR) (b) images demonstrate a small area of enhancement in the left inferior frontal lobe after three cycles of adjuvant temozolomide treatment. At the fifth cycle of adjuvant treatment, there is increased nodular enhancement (c) and surrounding T2/FLAIR signal abnormalities (d) suspicious for progression. (e) Dynamic susceptibility contrast magnetic resonance imaging (DSC-MRI) perfusion imaging showed no evidence of elevated blood volume. Subsequent surgical resection revealed evidence of necrosis without tumor cells.
Based on altered metabolite concentrations in tissues, single-voxel MRS can distinguish suspected progressive/recurrent tumor from treatment-related changes.123–126 The overall diagnostic performance of MRS using choline to NAA ratio in differentiating glioma progression from radiation necrosis has sensitivity and specificity of 0.88 and 0.86, respectively. 127 Multivoxel MRS can evaluate spatially heterogeneous tissues containing mixtures of recurrent tumor and treatment effect.128–133
FDG-PET has been evaluated for its diagnostic accuracy in distinguishing delayed radiation necrosis from recurrent tumor,134–138 although it is unclear whether these results are applicable for the cases pseudoprogression that typically occur at earlier times following chemoradiation. Due to high background uptake by the normal brain, FDG radiotracer may also not detect small recurrent lesions. Several studies have reported utility of amino acid PET, including c-methionine, F-DOPA, FET, and FLT for diagnosing tumor progression.139–145 There is evidence of improved diagnostic accuracy comparing to FDG-PET.139,146 For patients with glioblastoma following standard chemoradiation therapy who present with suspected progression 3 months after completion of treatment, FET-PET can diagnose pseudoprogression with sensitivity 84%, specificity 86%, and accuracy 85%. 147 More recently, texture analysis has been applied to amino acid PET imaging data with some success in defining pseudoprogression. 148
Response evaluation during antiangiogenic therapy
Antiangiogenic therapies such as bevacizumab, a humanized monoclonal antibody against VEGF and cediranib, a VEGF receptor inhibitor, can result in rapid normalization of vascular permeability, reducing the intensity of contrast enhancement on T1-weighted MRI.107,149,150 This imaging phenomenon is not associated with improved patient survival and therefore has been described as a ‘pseudoresponse’.107,151 A subset of patients with progressive tumor can also manifest as enlarging nonenhancing T2/FLAIR abnormality on imaging.107,151 The RANO criteria included guidelines requiring evaluation of T2/FLAIR images for determination of progression. 107 There is evidence that development of enlarging T2/FLAIR abnormality has been associated with subsequent progression of enhancing lesions. 152 A retrospective evaluation of the imaging data from the phase II BRAIN trial of bevacizumab treated recurrent glioblastoma demonstrated that the RANO criteria resulted in a small but significant difference in median progression-free survival than did the Macdonald criteria. 153 Currently, evaluation of nonenhancing tumor as defined by the RANO criteria is qualitative based on subjective review of T2/FLAIR imaging by expert readers of progression. 107 There is an urgent need for imaging strategies that can be employed as an objective surrogate in evaluating tumor burden in the setting of antiangiogenic therapy.
Nonenhancing tumor on T2/FLAIR MRI has been categorized by morphology as circumscribed versus infiltrative lesions. 154 Patients with nonenhancing circumscribed T2/FLAIR had worse survival outcomes comparing to those with infiltrative nonenhancing lesions, as well as those with enhancing progressive disease following initiation of bevacizumab.155,156 Although this approach of characterizing lesion morphology remains subjective, the qualitative imaging descriptors provide improved specificity with respect to patient outcome. 107 Volumetric methods have been proposed as an objective criteria in measuring T2/FLAIR lesions, although in the BELOB trial data obtained using such an approach did not result in improved post-treatment prognostication accuracy as compared to the RANO criteria. 157
T1 subtraction and T2 mapping techniques have been applied to evaluating post-bevacizumab treated patients with recurrent glioblastomas.158,159 These methods utilize commercially available MRI sequences that are commonly done for brain tumor evaluation and can be readily incorporated into the clinical workflow if postprocessing can be automated. DW-MRI is also commonly performed during routine brain tumor evaluation, and low ADC lesions observed on DW-MRI following bevacizumab treatment have been associated with progressive tumor. 160 High b-value DW-MRI improves detection of pseudoresponse over standard DW-MRI in patients treated with bevacizumab. 161 The specificity of low ADC lesions for active tumor has been questioned, since there have also been reports of hypoxic or necrotic tissue associated with these lesions. 162 Pathological analysis provides evidence that progressively expanding low ADC lesions contain coagulative necrosis surrounded by viable tumor. 163 An ADC threshold value of 0.736 × 10−3 mm2/s has been shown to be a potential differentiating factor of hypercellular tumor and necrosis. 163 Patients with larger low-ADC volumes after bevacizumab treatment had worse overall survival. 164 Advanced DW-MRI techniques such as histogram analysis of ADC and RSI has also been shown to predict overall survival following bevacizumab treatment.165,166 Perfusion imaging techniques including DSC-MRI and DCE-MRI also provide prognostic information during early post-bevacizumab treatment evaluation of patients with recurrent glioblastomas.167–170 There is early evidence that amino acid PET provides greater specificity than standard MRI for evaluation of progressive tumor and provides prognosis during antiangiogenic therapy171–173 (Figure 3). Combined-modality FMISO PET and MRI evaluated patients with recurrent high-grade glioma and revealed patterns of hypoxia after antiangiogenic therapy; enlarging nonenhancing mass showed reduced diffusion, lack of hypoxia, and preserved cerebral blood volume. 21

A 58-year-old man with recurrent glioblastoma receiving bevacizumab monotherapy. Pretreatment axial gadolinium-enhanced T1-weighted image (a) and 18F-fluoro-ethyl-tyrosine (FET) positron emission tomography image (b) showed an enhancing mass centered in the body of the corpus callosum with moderate FET avidity. After one dose of bevacizumab, the extent and intensity of enhancement both reduced as evident on the axial T1-weighted image (c), but there persists a slightly increased FET uptake in the left aspect of the mass (d). This area of abnormality showed increased enhancement on the subsequent axial gadolinium-enhanced T1-weighted image (e).
Response evaluation during immunotherapy
With the advent of new and emerging immunotherapies such as cytotoxic T-lymphocyte-4 (CTLA-4) immune checkpoint molecules such as ipilumimab, and programmed cell 1 agents such as nivolumab and pembrolizumab for metastatic melanoma and non-small cell lung cancer, establishing progression has had its challenges.174–176 Findings of classic progression including increasing size, enhancement, and edema may not reflect progression with immunotherapies that may involve a localized and temporary inflammatory response before subsequent improvement. 177 Furthermore, patterns of initial increase in target tumor size have preceded subsequent decrease in tumor size, with metastatic melanoma treated with anti-PD/PD-L1 therapy.178,179 The Immunotherapy Response Assessment in Neuro-Oncology (iRANO) working group has sought to address this by requiring a confirmation scan at 3 months for patients who presents with enlarging enhancement within 6 months from initiation of immunotherapy (Figure 4). 180 The 6-month cutoff time was empirically determined, but presentation of pseudoprogression beyond 6 months has been reported. 181 Furthermore, the 3-month time duration until the confirmatory scan could be a challenge in clinical practice since patients are often symptomatic. While further evaluation of data from immunotherapy trials is needed to provide support for the iRANO criteria, an imaging marker allowing accurate differentiation of immunotherapy-related changes from recurrent/progressive tumor is ultimately needed to improve management of patients undergoing immunotherapy. In small case series of patients with melanoma brain metastases treated with checkpoint inhibitors, dynamic FET-PET imaging appears to correctly identify pseudoprogression, 182 highlighting the potential application for the technique in imaging of patients with high-grade glioma. Finally, PET radiotracers targeting immune response are being developed. In a syngeneic immunocompetent mice model, immune responses can be detected after immunotherapy in glioblastoma using PET radiotracer for deoxycytidine kinase (dCK). 183
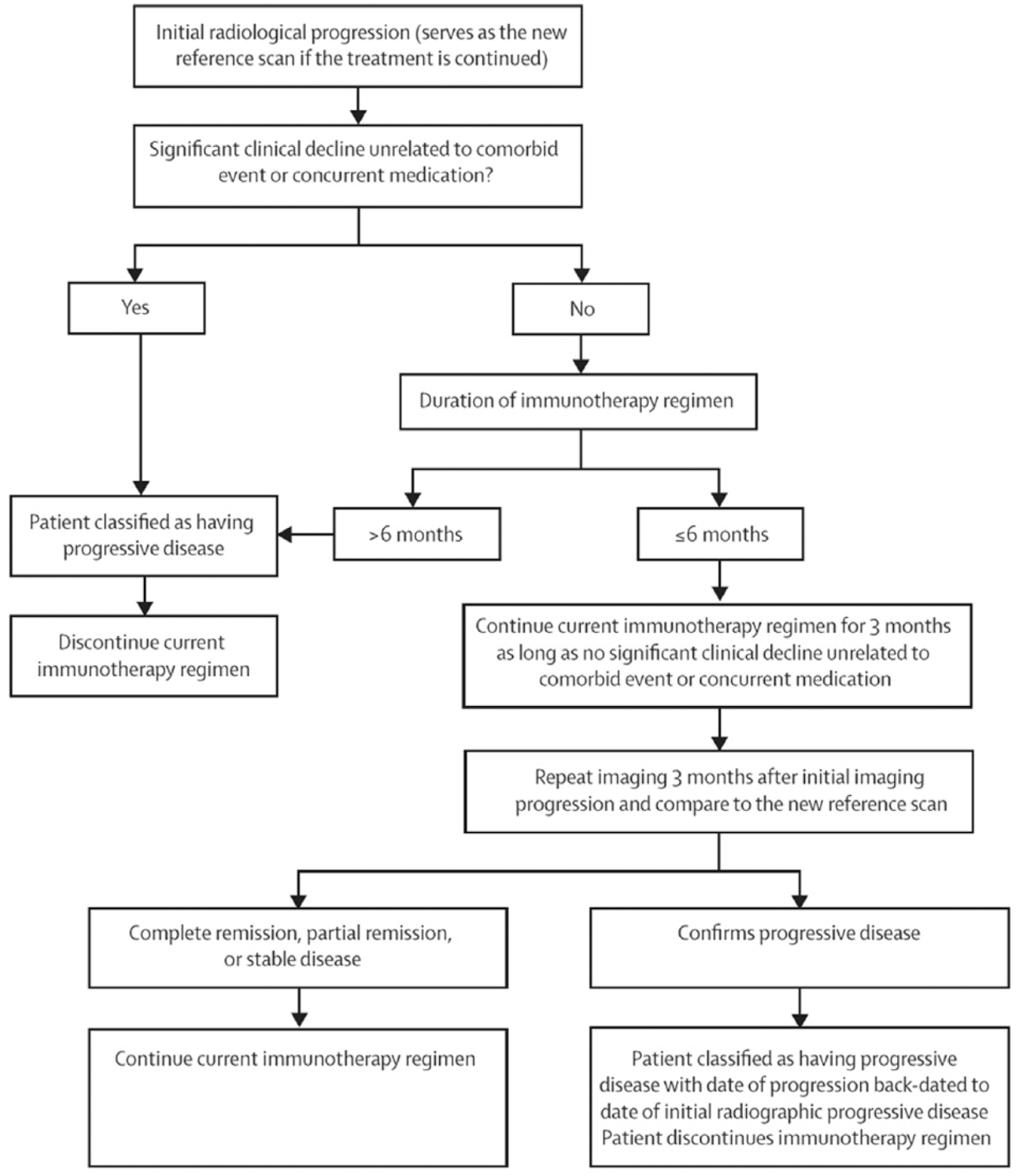
Schematic flowchart of the Immunotherapy Response Assessment in Neuro-Oncology criteria for response assessment in immunotherapy.
Challenges and outlook
While numerous novel imaging methods have been applied to address various clinical challenges faced by treating oncologists today, most of these techniques as outlined in this review still require validation from large prospective trials. Currently the acquisition protocol for evaluating brain tumors is highly variable among imaging centers, and such variability can impact the generalizability of imaging techniques across different sites. Recently, a standardized MRI protocol has been proposed specifying the acquisition parameters of conventional and diffusion MRI sequences, 184 as well as perfusion MRI. 185 Wider adoptions of these standardized protocols in the neuro-oncology community should aid the ongoing and future efforts in the discovery and validation of imaging markers in multicenter trials.
Machine learning approaches to neuro-oncologic imaging is only in its earliest phase of development and many of the results outlined in this review are not ready to be incorporated into clinical practice. For one, the current voxel-based analysis of imaging data requires whole-tumor segmentation, which has been a bottleneck in research progress and clinical implementation. This problem is currently being automated using state-of-the-art machine learning algorithms, with promising results.186–190 Furthermore, the machine learning approach can facilitate integration of data beyond imaging, including clinical and molecular markers, making this approach integral to diagnostic, prognostic, and predictive biomarker development and implementation. It is important to note that development and validation of machine learning models require large, well-annotated datasets, and therefore multidisciplinary efforts and multicenter collaborations are necessary.
Conclusion
Imaging plays several key roles in managing brain tumors, including diagnosis, prognosis, and treatment response assessment. There have been important innovations in numerous advanced imaging techniques with the aim of improving the accuracy of tumor diagnosis and address challenging clinical problems, including evaluation of pseudoprogression and response to antiangiogenic therapy and immunotherapy. Some of these techniques have already been incorporated as routine tumor evaluation in large centers, while many others are currently being validated for accuracy and reproducibility. Understanding the advantages and limitations of these techniques is essential in advancing our goal of personalized care for patients with brain tumors.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.