
Abstract
Background:
The objective of this study was to analyze published literature on autoimmune epilepsy and assess predictors of seizure outcome.
Methods:
From PubMed and EMBASE databases, two reviewers independently identified publications reporting clinical presentations, management and outcomes of patients with autoimmune epilepsy. A meta-analysis of 46 selected studies was performed. Demographic/clinical variables (sex, age, clinical presentation, epilepsy focus, magnetic resonance imaging [MRI] characteristics, time to diagnosis and initiation of immunomodulatory therapy, and type of immunomodulatory therapy) were compared between two outcome groups (responders and nonresponders). Clinical response was defined as >50% reduction in seizure frequency. Unstandardized effect sizes were collected for the studies for responder and nonresponder groups. Sample size was used as the weight in the meta-analysis. The random effects model was used to account for heterogeneity in the studies.
Results:
The 46 reports included 186 and 96 patients in responder and nonresponder groups respectively. Mean age of the responders and nonresponders was 43 and 31 years (p < 0.01). Responders were more likely to have cell-surface antibodies (68% versus 39%, p < 0.05), particularly voltage-gated potassium channel complex antibodies (p < 0.01). Mean duration from symptom onset to diagnosis, and symptom onset to initiation of immunomodulation was significantly lower among the responders (75 versus 431 days, p < 0.05, and 80 versus 554, p < 0.01, respectively). There was no outcome difference based on gender, MRI characteristics, seizure type, type of acute immunomodulatory therapy, or use of chronic immunomodulation.
Conclusions:
Among published cases to date, older age, presence of cell-surface antibodies, early diagnosis and immunomodulatory treatment are associated with better seizure outcomes among patients with autoimmune epilepsy.
Introduction
Seizures are a common manifestation of autoimmune encephalitis [Dubey et al. 2015a]. Other clinical manifestations include psychiatric symptoms, memory loss, involuntary movements, autonomic dysfunction and sleep disturbance [Dubey et al. 2016]. There are subtle differences in age of onset, progression and clinical presentation of various antibody associated encephalopathies [Dubey et al. 2015b].
The true prevalence of immune-mediated epilepsy syndromes remains unclear, but based on a study from Oxford it may be as high as 11% of all epilepsies [Brenner et al. 2013]. Another study evaluating the prevalence of antibodies in new-onset seizures in a pediatric cohort, reported a prevalence of 8% [Suleiman et al. 2013b]. Many cases with presumed autoimmune etiology are refractory to approved anti-seizure medications (ASM) [Dubey et al. 2014]. Immunomodulatory therapies such as steroids, plasma exchange, intravenous immunoglobulin (IVIg), rituximab, and cyclophosphamide have been utilized in management of these syndromes [McKeon, 2013].
To date, there are many individual case reports and small case series describing autoimmune epilepsy but no meta-analysis summarizing these reports to evaluate predictors of outcomes among patients with immune-mediated epilepsies. The purpose of this study was to delineate characteristics that may serve as important factors predicting seizure outcome.
Methods
Two reviewers (Divyanshu Dubey and Zehra Farzal) independently searched MEDLINE, PubMed and EMBASE databases. The literature search was conducted in August 2015. The search terms utilized were ‘autoimmune limbic encephalitis’, ‘limbic encephalitis’, ‘autoimmune encephalitis’, and ‘autoimmune epilepsy’. The search included publications from 1968 to 2015. We identified studies reporting clinical presentations, management and outcomes of patients with immune-mediated epilepsy. Studies which did not quantify seizure frequency or document change in seizure frequency were excluded. We were careful to avoid including patients twice when they were included in more than one publication [Dubey et al. 2015a, 2015b]. Demographic/clinical variables (sex, age, race, clinical presentation, type of antibody, localization of antigen [intra-neuronal or cell surface], cerebrospinal fluid [CSF] protein, CSF pleocytosis, epilepsy focus, magnetic resonance imaging [MRI] characteristics, number of ASMs used, underlying malignancy, time to diagnosis and initiation of immunomodulatory therapy, and type of immunomodulatory therapy) were compared between two outcome groups (responders and nonresponders). Clinical response was defined as >50% reduction in seizure frequency. There was heterogeneity in the time frame for assessment of improvement in the included studies. The larger retrospective studies in the meta-analysis included evaluation at the first clinic visit after hospitalization or initial management as time to evaluate for seizure outcomes (range: 0.3–72 months). Unstandardized effect sizes were collected for the studies for responder and nonresponder groups. Sample size was used as the weight in the meta-analysis. A measure of heterogeneity was performed using Q-and I2 statistics. The random effects model was used to account for heterogeneity in the studies. The maximum likelihood option was used in the model. Modified weighted multiple least squares regression was utilized to adjust for confounding variables. SPSS meta-analysis tools were used to compare effect sizes [Wilson, 2010]. Variables which were found to be significant on univariate analysis were evaluated through a multivariate regression model with immunomodulatory therapy included as a confounding variable.
Results
Out of 711 publications screened on an initial database search, 46 reports (published between 1999 and 2015) met our criteria and were included (Table 1). Among the 46 studies (including 28 case reports and case series with <5 patients), there were 186 and 96 patients in responder and nonresponder groups respectively (Table 2). The mean age of the responders and nonresponders was 42.61 ± 0.07 years and 31.20 ± 0.10 years (p < 0.01, CI −11.66, −11.16) respectively. Among the responders there was a significantly higher proportion of patients with cell-surface antibodies (68% ± 7% versus 39% ± 10%, p < 0.05, CI −0.54, −0.04, Table 2). Specifically the proportion of patients with antibodies against voltage-gated potassium channel complex (VGKCc) antigens was significantly higher in the responder group compared with the nonresponder group (45% ± 7% versus 11% ± 11%, p < 0.01, CI −0.59, −0.09). The mean time from symptom onset to diagnosis was significantly lower among the responders (74.94 ± 68.91 days versus 431.25 ± 137.81 days, p < 0.05, CI 54.32, 658.31). Most of the reported patients received immunomodulatory therapy, 95% of the responders and 77% of the nonresponders. Patients in the responder group were also initiated on immunomodulatory therapy in a significantly shorter time, compared with the nonresponders (79.94 ± 84.37 days versus 553.83 ± 137.78 days, p < 0.01, CI 157.23, 790.56). Even after adjusting for use of immunomodulatory therapy, effect size differences in delay from symptom onset to immunomodulatory therapy (p < 0.01, CI 263.76, 872.69), age (p < 0.01, 95% CI −8.85, −8.30), presence of antibodies against cell surface antigens (p < 0.05, CI −0.56, −0.01) or VGKCc antibodies (p < 0.05, CI −0.62, −0.07) between the two groups continued to be statistically significant. There was no difference in the two groups based on type of immunomodulatory therapy used at the time of acute presentation. High dose corticosteroid was the initial immunomodulatory therapy in a higher proportion of responders compared with nonresponders (88% ± 8% versus 62% ± 11%,p = 0.06, CI −0.52, 0.01). Nonresponders more often had an underlying malignancy (21% ± 13%) compared with the responders (15% ± 10%, p = 0.74) but this difference was not significant. A higher proportion of responders (47% ± 8% versus 36% ± 11%) received chronic immunomodulation in the form of long term oral steroids, rituximab infusion, mycophenolate mofetil, cyclophosphamide or azathioprine but this difference was not significant (p = 0.44). There was no outcome difference associated with gender, MRI characteristics (medial temporal lobe T2/FLAIR signal changes), seizure focus (temporal or extra-temporal), elevated CSF protein, CSF pleocytosis or number of ASMs.
Summary of demographic and clinical characteristics of included cases from 46 studies.

AZA, azathioprine; CYP, cyclophosphamide; MMF, mycophenolate mofetil; MRI, magnetic resonance imaging; NR, nonresponders; R, responder; RTX, rituximab.
Comparison of demographic and clinical variables amongst responders to the nonresponders.

ASM, anti-seizure medications; CSF, cerebrospinal fluid; GAD, glutamic acid decarboxylase; IVIG, intravenous immunoglobulin; MP, methyl prednisone; NMDA, N-methyl D-aspartate; PLEX, plasmapheresis; SE, standard error; VGKCc, voltage-gated potassium channel complex.
Significant heterogeneity was noted with regards to the age of patients across the included studies (Table 3). Other variables including duration of symptoms and cell-surface receptor antibody status were fairly homogenous between the studies.
Q-statistic and I2 values for the significant variables as a measure of heterogeneity among the studies included in the meta-analysis.
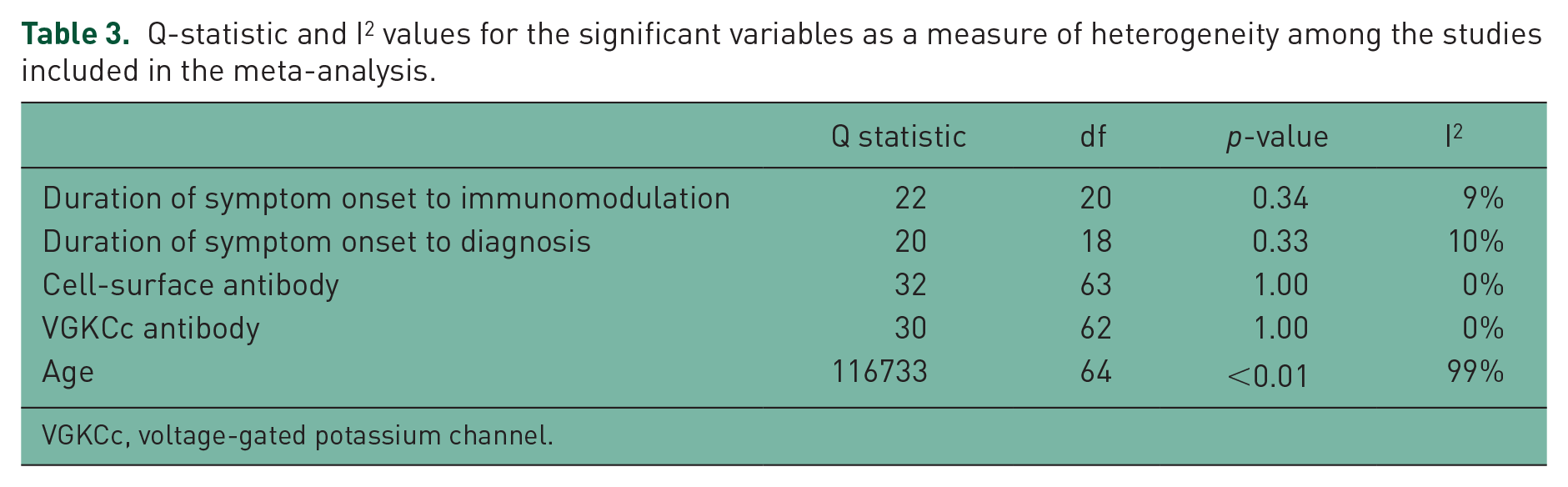
VGKCc, voltage-gated potassium channel.
Discussion
Our study demonstrates that among published cases of immune-mediated epilepsy, older age, presence of antibodies against cell surface antigens, early diagnosis, and early utilization of immunomodulatory treatment are associated with better seizure outcomes. On the other hand, there was no significant outcome difference based on MRI characteristics, seizure type, the type of acute immunomodulatory therapy utilized, or the use of chronic immunomodulation. Reanalysis of the data after excluding case reports or series of <5 patients showed similar trends, although some of the predictors of good outcome did not reach statistical significance (Table 2).
These findings suggest that early diagnosis and early use of immunomodulatory therapy are associated with a better outcome, as measured by reduction in seizure frequency. Early immunomodulation may reduce autoimmune and inflammatory changes before astrogliosis or irreversible neuronal injury takes place. Although there was no significant difference in efficacy in various types of acute immunomodulatory therapy, a considerably higher number of patients with good seizure outcome (>50% reduction of seizure frequency) received intravenous high dose corticosteroids as initial therapy. Corticosteroids may impact the lymphocyte activation and antibody production by affecting the chemokine and cytokine profile, and inducing lymphocyte depletion [Greaves, 1976]. Treatment algorithms suggested by prior studies have also recommended use of intravenous methylprednisolone as the first line agent in the absence of any contraindication [Dubey et al. 2015b]. Prospective randomized trials will be needed to definitively demonstrate the benefits of immunomodulatory therapy for autoimmune epilepsy. The data from retrospective studies clearly suggest the potential benefits of immunomodulation, which does raise ethical concerns in designing placebo-controlled trials.
Multiple antibodies targeting neuronal cell-surface antigens have been described in recent years (N-methyl D-aspartate-receptor [NMDA-R], α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor [AMPA-R], leucine-rich glioma-inactivated protein-1 [LGI-1], contactin-associated protein-2 [Caspr-2], γ-aminobutyric acid-A receptor [GABA-AR], γ-aminobutyric acid-B receptor [GABAB-R]), glycine-receptor, the dipeptidylpeptidase-like protein-6 [DPPX], and the IgLON5) [Nosadini et al. 2015]. It has been postulated that these antibodies may have a direct etiopathogenic role in these encephalitis syndromes, whereas immune-mediated syndromes associated with antibodies directed against intraneuronal antigens (such as anti-Hu, anti-Yo, anti-Ri, anti-Tr, and anti-CV2/CRMP5 antibodies) are hypothesized to be mediated by cytotoxic T-cells, (an epiphenomena secondary to antigenic release following T-cell-mediated neuronal cytotoxicity) [Dubey et al. 2015b; Gultekin et al. 2000; Dubey, 2016]. As supported by our study, cell-surface antigen-mediated antibody syndromes are considered to be more responsive to immunomodulation.
Despite the heterogeneity of the age of patients between the two groups, when correcting for other variable there was an association of older age with better seizure outcome regardless of immunomodulatory status. Similarly an observational cohort study of anti-NMDA receptor encephalitis also showed that older age was associated with a less severe forms of NMDA-R antibody-mediated encephalitis [Titulaer et al. 2013]. The pathophysiological basis of this age effect remains unclear. The potential etiology could be lower affinity of autoantibodies or weaker autoimmune response due to a decline in the generation of naïve lymphocytes and functional competence of memory cells [Hakim and Gress, 2007; Johnson and Cambier, 2004].
Limitations of our meta-analysis include the lack of prospective studies and the effects of bias inherent in meta-analyses, especially publication bias. Given that many of the patients included in the analysis were from case reports, over representation of positive outcomes is likely. Additionally, many of the single patient case reports and smaller case series did not mention the time frame for evaluation of reduction in seizure frequency. While the studies were identified from three different databases by two reviewers independently, ascertainment bias is also a possible limitation. Since patients falling in the ‘responder’ group were defined by a ⩾50% reduction in seizure frequency, publications that did not quantify seizure frequency or described a clear change in seizure frequency were excluded, including some prominent studies with large sample sizes. Lastly, this meta-analysis evaluates predictors of seizure outcomes in patients with autoimmune epilepsy syndrome. However, patients with autoimmune encephalopathy often have myriad clinical manifestations and reduction of seizure frequency is not the only factor associated with good clinical outcome.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
Dr Steven Vernino receives personal compensation as a scientific consultant for Athena diagnostics (Massachusetts, United States) and on speaker bureau for Lundbeck (Illinois, United States). The other authors report no conflicts of interest in this work.