
Abstract
Objectives:
The cumulative safety and efficacy measures of percutaneous transluminal angioplasty and stenting (PTAS) for secondary stroke prevention in patients with symptomatic intracranial arterial stenosis (sICAS) have not previously been evaluated using a meta-analytical approach.
Methods:
We conducted a systematic review and random effects meta-analysis of all available randomized controlled trials (RCTs) evaluating the safety and efficacy of PTAS (in comparison with medical therapy) for sICAS.
Results:
Three RCTs (678 total patients) were included in the quantitative analysis. PTAS was associated with a higher risk of recurrent ischemic stroke in the territory of qualifying artery both within 30 days [risk ratio (RR) = 2.21, 95% confidence interval (CI) 1.10–4.43] and 1 year (RR = 1.92, 95% CI 1.10–3.36). PTAS was also related to a higher risk of any ischemic stroke within 30 days from the index event (RR = 2.08, 95% CI 1.17–3.71). The risk for intracranial hemorrhage was found to be higher in PTAS patients both within 30 days (RR = 10.60, 95% CI 1.98–56.62) and 1 year (RR = 8.15, 95% CI 1.50–44.34). The composite outcome of any stroke or death within 1 year (RR = 2.29, 95% CI 1.13–4.66) and 2 years (RR = 1.52, 95% CI 1.04–2.21) was higher in PTAS than in medical therapy. PTAS was associated with a higher risk of any stroke or death within 2 years in the sICAS subgroup located in posterior circulation (RR = 2.37, 95% CI 1.27–4.42).
Conclusions:
PTAS is associated with adverse early and long-term outcomes and should not be recommended in patients with sICAS. Further research to identify subgroups of patients who could also serve as candidates for future interventional trials along with efforts to reduce procedure-related complications are needed.
Keywords
Introduction
The risk of recurrent stroke in patients with symptomatic intracranial arterial stenosis (sICAS) remains high and is more pronounced in the territory of the stenotic artery with stenosis ⩾70% and following recent symptoms [Reith et al. 2015; Kasner et al. 2006]. Although percutaneous transluminal angioplasty and stenting (PTAS) is technically feasible in this patient subgroup, it did not meet the expectations in randomized, controlled trial (RCT) settings and was less effective than best medical therapy (BMT) [Chimowitz and Derdeyn, 2015].
The aim of the present systematic review and meta-analysis was to evaluate both the safety and efficacy of PTAS for sICAS, in comparison with BMT, using data from available RCTs.
Methods
This meta-analysis is presented according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [Liberati et al. 2009]. Eligible placebo-controlled RCTs that compared the safety and efficacy of PTAS for sICAS with BMT were identified by searching MEDLINE, SCOPUS and the CENTRAL Register of Controlled Trials. The complete search algorithm used in the MEDLINE search was: (“percutaneous transluminal angioplasty”[All Fields] OR (“stents”[MeSH Terms] OR “stents”[All Fields] OR “stenting”[All Fields]) OR (“stents”[MeSH Terms] OR “stents”[All Fields] OR “stent”[All Fields])) AND (intracranial[All Fields] AND (“constriction, pathologic”[MeSH Terms] OR (“constriction”[All Fields] AND “pathologic”[All Fields]) OR “pathologic constriction”[All Fields] OR “stenosis”[All Fields])) AND ((“stroke”[MeSH Terms] OR “stroke”[All Fields]) OR “cerebral ischemia”[All Fields]) AND Clinical Trial[ptyp].
We excluded from further analysis all: (1) observational studies; (2) case series or case reports; (3) clinical trials with no randomization protocol; and (4) single-arm RCTs. In each eligible study we employed the Cochrane Collaboration tool to address for biases [Higgins et al. 2011], and extracted data regarding the reported events of stroke (ischemic or hemorrhagic) and/or death at any given timepoint. For each outcome we calculated the corresponding risk ratios (RRs) for each study protocol, while the pooled RRs were estimated using a random-effects model (DerSimmonian Laird). We assessed heterogeneity between studies with the Cochran Q and I2 statistics [Khan et al. 2014; Tsivgoulis et al. 2014; Katsanos et al. 2014]. All statistical analyses were conducted using the Review Manager (RevMan) Version 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
The literature search returned five potential eligible studies (Figure 1). After retrieving the full texts of the aforementioned studies, we excluded two study protocols as they were single-arm [Levy et al. 2011] or non-randomized trials [SSYLVIA Study Investigators, 2004]. The remaining three study protocols, comprising a total of 678 patients [mean age 61.4 years, 63% men, 65% with ischemic stroke (IS)], were included in both the qualitative and quantitative synthesis. The baseline characteristics of included studies [Chimowitz et al. 2011; Compter et al. 2015; Zaidat et al. 2015] are briefly summarized in Table 1.
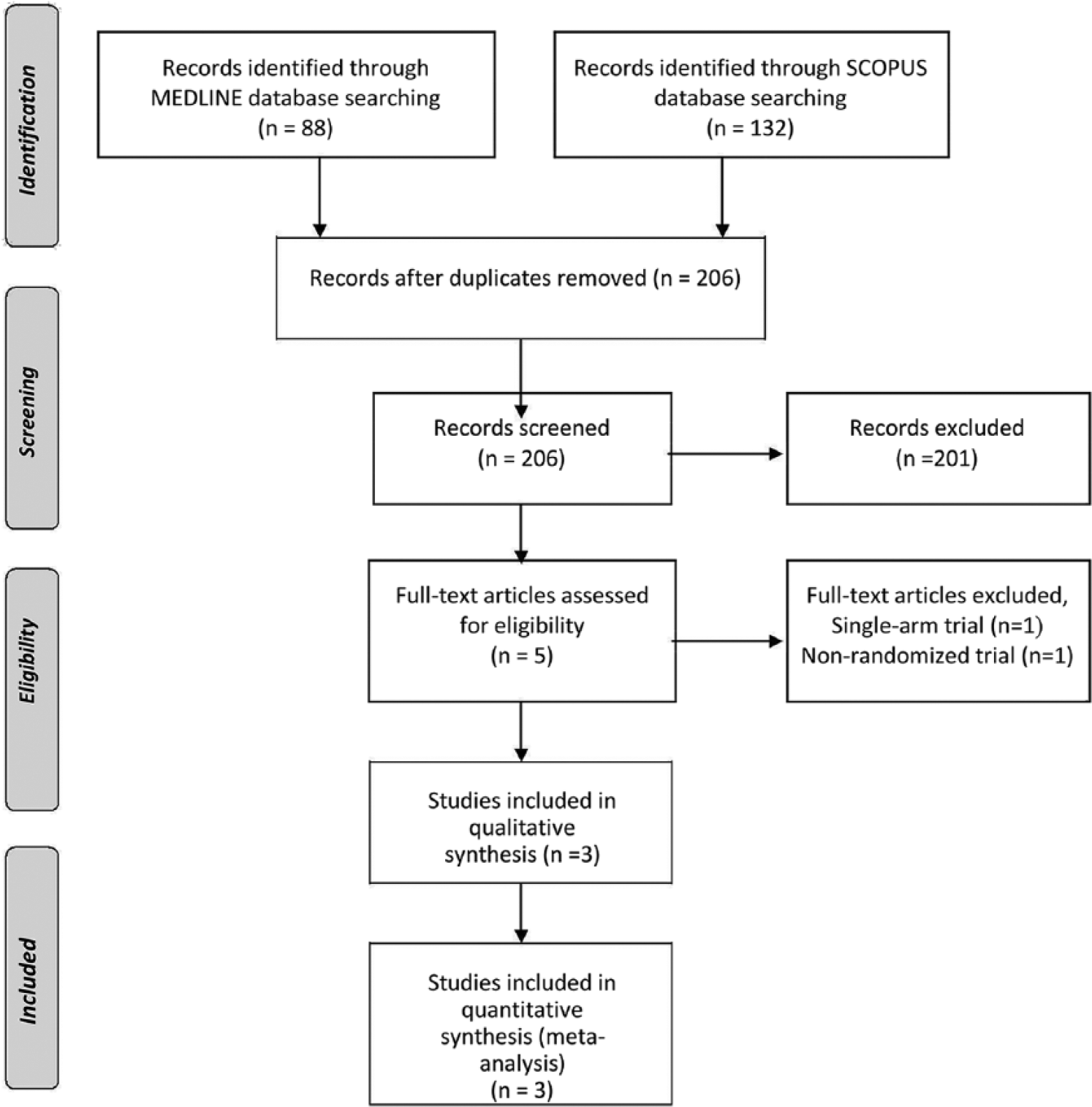
PRISMA flow chart presenting the selection of eligible studies.
Baseline population characteristics of the included studies.

PTAS, percutaneous transluminal angioplasty and stenting; HTN, hypertension; DM, diabetes mellitus; HLP, hyperlipidemia; CAD, coronary artery disease; IS, ischemic stroke; NR, not reported.
Qualitative assessment is presented in Figure 2. Even though all three RCTs had open-label treatment with blinded end-point evaluation (PROBE design) [Chimowitz et al. 2011; Compter et al. 2015; Zaidat et al. 2015], we considered that the outcome measure was likely not influenced by the lack of blinding. However, we assessed the risk of performance bias as high in two out of three study protocols, since they reported that follow up was performed by physicians who were not blinded to the patients’ treatment assignment [Chimowitz et al. 2011; Compter et al. 2015]. Only one of the studies reported solely funding from public sources [Compter et al. 2015], while another one reported that funding was mainly by public entities and academic institutions but also acknowledged receiving industry support [Chimowitz et al. 2011]. Finally, the risk of bias was considered high in the third study, as not only did the trial sponsor have a clear conflict of interest in the study topic, but also had crucial involvement in all study domains (design, conduction, data collection, analysis, interpretation, review of the manuscript) [Zaidat et al. 2015].

Risk of bias. (A) Summary: review authors’ judgments about each risk of bias item for each included study. (B) Graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
Overall analyses for reported outcomes are presented in Table 2. PTAS was associated with higher risk of recurrent IS in the territory of qualifying artery both within 30 days (RR = 2.21, 95% CI 1.10–4.43; Figure 3) and 1 year (RR = 1.92, 95% CI 1.10–3.36; Figure 4), as well as with the risk of any stroke within 30 days (RR = 2.08, 95% CI 1.17–3.71; Figure 5). The 30-day and 1-year risk for intracranial hemorrhage was higher in PTAS group [RR (30 days) = 10.60, 95% CI 1.98–56.62, Figure 6; RR (1 year) = 8.15, 95% CI 1.50–44.34, Figure 7]. The composite outcome of any stroke or death within 1 year (RR = 2.29, 95% CI 1.13–4.66; Figure 8) and 2 years (RR = 1.52, 95% CI 1.04–2.21; Figure 9) was higher in PTAS. PTAS was associated with a higher risk of any stroke or death within 2 years in the sICAS subgroup located in posterior circulation (RR = 2.37, 95% CI 1.27–4.42; Figure 10). Finally, PTAS tended to be associated with a higher risk of IS recurrence in the territory of the qualifying artery after 30-days (RR = 1.56, 95% CI 0.67–3.67; Figure 11) and with disabling or fatal stroke (modified Rankin scale score >3) at 1 year (RR = 1.57, 95% CI 0.86–2.87; Figure 12). Significant heterogeneity was not documented in any of the presented analyses with the exception of the composite outcome of any stroke or death within 1 year (I2 = 70%, p for Cochran Q = 0.04; Figure 8).
Overall analyses for reported outcomes in the studies included in the meta-analysis.
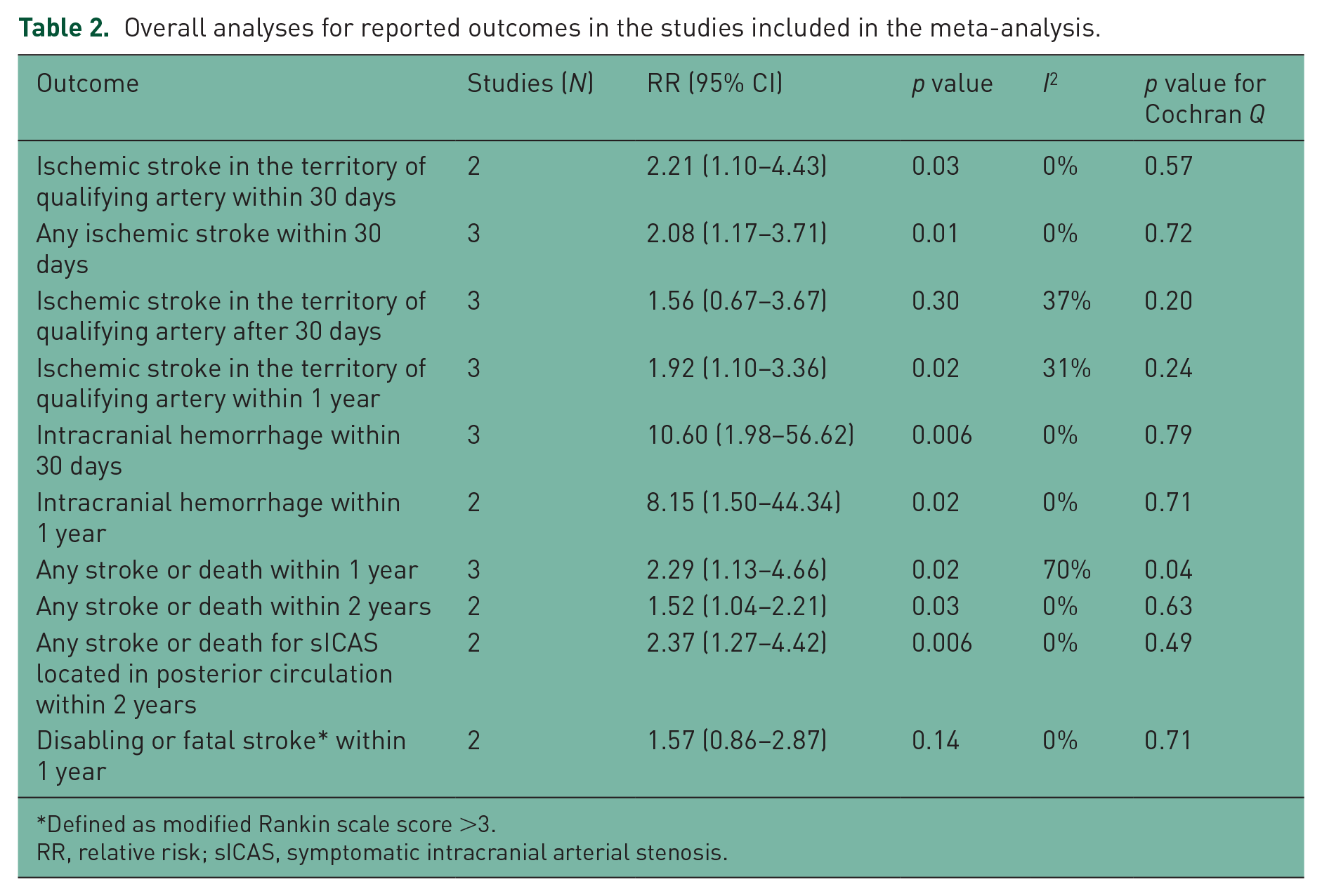
Defined as modified Rankin scale score >3.
RR, relative risk; sICAS, symptomatic intracranial arterial stenosis.

Pooled analysis for the outcome: ischemic stroke in the territory of qualifying artery within 30 days.

Pooled analysis for the outcome: ischemic stroke in the territory of qualifying artery within 1 year.

Pooled analysis for the outcome: any ischemic stroke within 30 days.

Pooled analysis for the outcome: intracranial hemorrhage within 30 days.

Pooled analysis for the outcome: intracranial hemorrhage within 1 year.

Pooled analysis for the outcome: composite outcome (any stroke or death) within 1 year.

Pooled analysis for the outcome: composite outcome (any stroke or death) within 2 years.

Pooled analysis for the outcome: composite outcome (any stroke or death) for symptomatic intracranial arterial stenosis located in posterior circulation within 2 years.

Pooled analysis for the outcome: ischemic stroke in the territory of qualifying artery after 30 days.

Pooled analysis for the outcome: disabling or fatal stroke (modified Rankin scale >3) at 1 year.
Discussion
Our meta-analysis showed that PTAS is associated with adverse early and long-term outcomes including both ischemic and hemorrhagic stroke. This association persisted for the sICAS subgroup located in posterior circulation. Finally, we documented no evidence of significant heterogeneity in eight out of nine prespecified outcome events evaluated in the present meta-analysis.
SAMMPRIS investigators have reported perforator occlusion as the most common cause of periprocedural IS, presumably due to plaque debris embolism into small perforator vessels during angioplasty or stent deployment [Fiorella et al. 2012]. Apart from the procedure-related IS both VISSIT and SAMMPRIS trials reported that the risk of cerebral ischemia in the territory of the stenotic artery remained increased even after the 30-day perioperative period, while an unexpectedly high risk of intracranial hemorrhage after stenting was consistently documented in perioperative and follow-up periods [Chimowitz and Derdeyn, 2015; Lutsep et al. 2015; Derdeyn et al. 2013]. More specifically, PTAS was associated with a higher risk of periprocedural subarachnoid hemorrhage (because of vessel perforation) and reperfusion intraparenchymal hemorrhage [Reith et al. 2015; Chimowitz and Derdeyn, 2015].
Our findings lend support to current AHA recommendations indicating that PTAS should not be offered as initial treatment in sICAS patients [Kernan et al. 2014]. Further research is required to identify patient subgroups with high risk of stroke recurrence (e.g. patients with multiple prior ischemic events unresponsive to BMT, acute stroke patients treated with PTAS during the first month following the index event). In addition, efforts to reduce procedure-related complications (regional perforator infarction, delayed intraparenchymal hemorrhage, wire perforation) need to be promoted [Chatterjee and Derdeyn, 2015]. The China Angioplasty and Stenting for Symptomatic Intracranial Severe Stenosis (CASSISS) trial is an ongoing, multicenter RCT aiming to redefine the role of PTAS in selected patients with sICAS, by overcoming the shortcomings of previous RCTs [Gao et al. 2015].
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Georgios Tsivgoulis has been supported by the European Regional Development Fund – Project St. Anne`s University Hospital, Brno - International Clinical Research Center (FNUSA-ICRC) (No. CZ.1.05/1.1.00/02.0123).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.