
Abstract
Objectives:
The aim of this study was to assess the relative importance of features of a hypothetical injectable disease-modifying treatment for patients with multiple sclerosis using a discrete-choice experiment.
Methods:
German residents at least 18 years of age with a self-reported physician diagnosis of multiple sclerosis completed a 25–30 minute online discrete-choice experiment. Patients were asked to choose one of two hypothetical injectable treatments for multiple sclerosis, defined by different levels of six attributes (disability progression, the number of relapses in the next 4 years, injection time, frequency of injections, presence of flu-like symptoms, and presence of injection-site reactions). The data were analyzed using a random-parameters logit model.
Results:
Of 202 adults who completed the survey, results from 189 were used in the analysis. Approximately 50% of all patients reported a diagnosis of relapsing–remitting multiple sclerosis, and 31% reported secondary progressive multiple sclerosis. Approximately 71% of patients had current or prior experience with injectable multiple sclerosis medication. Approximately 53% had experienced flu-like symptoms caused by their medication, and 47% had experienced mild injection-site reactions. At least one significant difference was seen between levels in all attributes, except injection time. The greatest change in relative importance between levels of an attribute was years until symptoms get worse from 1 to 4 years. The magnitude of this difference was about twice that of relapses in the next 4 years, frequency of injections, and flu-like symptoms.
Conclusions:
Most attributes examined in this experiment had an influence on patient preference. Patients placed a significant value on improvements in the frequency of dosing and disability progression. Results suggest that changes in injection frequency can be as important as changes in efficacy and safety attributes. Understanding which attributes of injectable therapies influence patient preference could potentially improve outcomes and adherence in patients with multiple sclerosis.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic, autoimmune, inflammatory disorder of the central nervous system characterized by axonal demyelination and eventual axon loss [Kamm et al. 2014; Saidha et al. 2012]. First-line treatment for MS in Germany has evolved over the past 3 years to now include oral treatments such as dimethyl fumarate and teriflunomide [Warnke et al. 2013; Weber et al. 2012]. However, historically, the mainstay of disease-modifying treatments (DMTs) for MS are injectable immunomodulatory drugs [Patti, 2010; Wingerchuk and Carter, 2014]. The injectable DMTs are well-established therapies with a wealth of real-world safety and efficacy data that span two decades [McGraw and Lublin, 2013]. In 2014, a pegylated interferon (peginterferon) beta-1a administered subcutaneously was approved in the European Union (EU) and United States (US) for relapsing MS (RMS) [Biogen 2014a, 2014b]. This new, injectable DMT has the longest dose interval compared with alternative injectable treatments: administered only once every 2 weeks [Biogen 2014a, 2014b], allowing patients the option of having injection-free weeks. All injectable DMTs are associated with a number of adverse events (AEs) that differ in severity depending on the treatment regimen. The most common, nonserious AEs include flu-like symptoms (FLS) and injection-site reactions (ISR) (including pain, erythema, pruritus) [Patti, 2010; Wingerchuk and Carter, 2014].
Adherence to injectable DMTs is an ongoing issue for patients and physicians [Patti, 2010]. A phase IV study of DMT therapy in approximately 2500 patients with relapsing–remitting MS (RRMS) reported that 25% of patients were nonadherent [Devonshire et al. 2011]. A total of 50% of these nonadherent patients stated that they forgot to administer the injection, and 32% stated injection-related reasons for their nonadherence [Devonshire et al. 2011]. Adherence rates have been shown to decline as more frequent injections are needed. Indeed, an analysis of more than 6600 patients with MS showed greater treatment adherence in those needing once-weekly injections than those with a more frequent injection regimen [Halpern et al. 2011]. Consequently, poor treatment adherence due to frequent injections is an important factor for physicians, healthcare authorities, and the pharmaceutical industry to consider [Devonshire et al. 2011; Steinberg et al. 2010].
Injection-related reasons for nonadherence include physical or cognitive difficulties, perceived lack of treatment efficacy, treatment-related AEs occurring with each injection, injection anxiety, needle phobia, and injection fatigue [Lugaresi, 2009; Patti, 2010; Menzin et al. 2013]. New treatments with prolonged efficacy that allow for increased time between doses have now been developed; these require fewer overall injections when compared with older treatments, thereby reducing injection-related factors experienced by patients [Menzin et al. 2013; Patti, 2010; Shingler et al. 2013].
Patient preferences, and consequent trade-offs for specific features and attributes of injectable DMTs, are not captured by health-related quality of life (HRQoL) instruments, such as the EQ-5D, or quality-adjusted life year (QALY) models [Shingler et al. 2013; Whitehead and Ali, 2010]. A discrete-choice experiment (DCE) is an established methodology for quantifying patient preference for attributes of medical treatments. DCEs are based on the concept that a treatment can be described as a combination of features, or attributes, and that choice of alternative treatments depends on the relative preferences for the different attributes of those treatments. Attributes are described as a series of levels; for instance, the attribute of dosing frequency could include the levels of weekly, bi-weekly or monthly dosing. In a DCE study, participants are presented with a series of treatment pairs with different attributes and levels. Statistical analysis of patients’ treatment choices across a series of paired comparisons reveals the importance of individual attributes and the trade-offs between attributes that patients are willing to make (for example, the reduction in efficacy that patients would accept in exchange for an improvement in dosing frequency).
DCEs have been used previously to study preferences for MS treatments [Johnson et al. 2009; Shingler et al. 2013; Utz et al. 2014; Wicks et al. 2015; Wilson et al. 2014, 2015]. Shingler and colleagues assessed patient preference for features of injection devices and treatment efficacy, showing that while efficacy is of primary importance, device attributes can play an important role in patient preference. They did not assess patients’ aversion to side effects [Shingler et al. 2013]. Johnson and colleagues assessed patient preferences for risk of serious AEs as the efficacy of treatment improved, indicating that patients would be willing to accept a degree of increased risk associated with their treatment if there was a corresponding increase in treatment efficacy. However, they did not assess preferences for dosing features, such as dosing frequency or mode of administration [Johnson et al. 2009]. Utz and colleagues examined preferences for dosing features of DMTs and found that pills were preferred to injections [Utz et al. 2014]. However, by varying dosing frequency independently from mode of administration and side effects, they found that injections were preferred when pills had more frequent mild side effects or more frequent dosing. However, Utz and colleagues did not assess preferences for efficacy attributes. The studies described by Wicks and colleagues and Wilson and coworkers examined preferences for a broad range of treatment attributes, including efficacy, serious and mild side effects, and mode and frequency of administration [Wicks et al. 2015; Wilson et al. 2014, 2015]. Wicks and colleagues examined preferences for oral DMTs only, while Wilson and coworkers focused on oral and parenteral DMTs. Mode of administration and dosing frequency were not varied independently, which limited their ability to assess acceptable trade-offs among dosing frequency and other treatment features and health outcomes.
The objective of this study was to assess the relative importance of a number of features of a hypothetical injectable DMT for patients with MS in Germany. This study used a DCE to quantify patients’ preferences for features of injectable DMTs, including efficacy, side effects, and features related to administration, such as dosing frequency and injection time.
Methods
Study design
The study investigators employed an online DCE, similar to the design previously used to examine US patient preference for injectable treatments for MS [Poulos et al. 2015]. The survey design, administration, and analysis followed the guidelines for DCE applications in healthcare [Bridges et al. 2011]. The choice and descriptions of each treatment attribute and its associated levels were informed by: (i) consultation with clinical experts; (ii) features of currently available injectable DMTs; (iii) selected clinical study findings; and (iv) the relevance to patients. The final six treatment attributes were: the number of years until MS symptoms get worse (i.e. disability progression), the number of relapses in the next 4 years, injection time, frequency of injections, FLS, and ISRs (Table 1). A draft survey was pretested using in-depth, in-person interviews with patients.
Specific attributes and the corresponding levels for the treatment-choice questions used in the study.
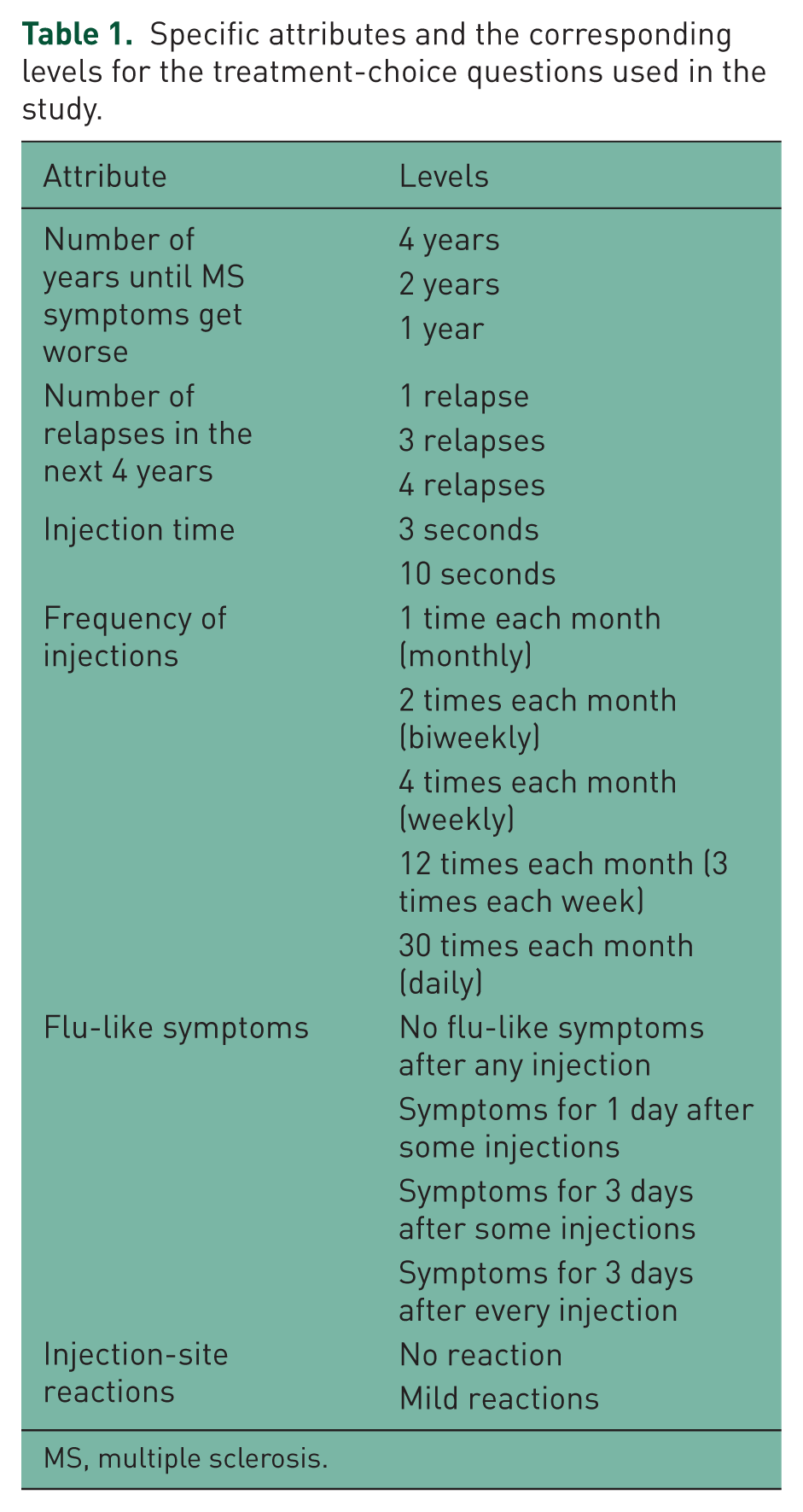
MS, multiple sclerosis.
Patients were asked to choose one of two hypothetical injectable treatments for MS, defined by the attributes and levels in Table 1. An example treatment-choice question is shown in Figure 1. During the survey, patients were asked to consider the cost of all medications as equal, since cost was not chosen as an attribute for analysis.

An example treatment-choice question.
SAS 9.3 (SAS Institute, Cary, NC, USA), an analytics software program, was used to generate the experimental design [Johnson et al. 2013]. The attribute levels and the pairs of profiles were optimized for design efficiency, level balance, correlations between level differences, and number of choice tasks [Huber and Zwerina, 1996; Kanninen, 2002; Dey, 1985; Kuhfeld et al. 1994; Kuhfeld, 2010]. To maximize the quality of responses and to minimize cognitive burden, SAS 9.3 generated 48 pairs of profiles that were split into six versions of eight questions. Patients were assigned randomly to one of the six versions, and the order of the questions was randomized for each patient. One question was repeated later in the sequence to assess the stability of patients’ choices (data not shown).
To ensure that all patients were considering the same level of initial disability and the same improvements in efficacy when evaluating the hypothetical treatments, they were asked to answer the questions as if their health status conformed to a hypothetical reference scenario. According to the reference scenario, patients’ ‘baseline’ or initial disability was ‘mild’ on the Hohol disease steps scale, and disability would progress to ‘moderate’ when their symptoms got worse [Hohol et al. 1995]. Data on patient demographics and socioeconomic characteristics and experiences with MS and MS treatments were also collected.
Study sample
E-mail invitations were sent to an online panel of individuals in Germany. To take part in the survey, individuals needed to be at least 18 years of age, be a resident of Germany, and have a self-reported physician diagnosis of MS. The online survey, administered in September 2013, took approximately 25–30 minutes to complete. Patients who completed at least one treatment-choice question in the survey were compensated €5 for their participation in the study.
Analyses
A random-parameters logit (RPL) model was used to analyze the discrete-choice data using NLOGIT Software Version 5.0 (Econometric Software, Inc.; Plainview, NY, USA). The RPL model approximates mean log-odds preference, and accounts for the panel nature of the data set (multidimensional observations obtained over multiple time periods) as well as the heterogeneity in preferences amongst patients [Train, 2003; Train and Sonnier, 2005]. Treatment choice was the dependent variable, and levels for each attribute were the independent, effects-coded, categorical variables [Hensher et al. 2005]. All independent variables were specified to be normally distributed random parameters. To examine whether treatment choice depends on a combination of attributes, models with interactions between frequency of injections per month and injection time, FLS, or ISR were estimated. Also, the analysis examined whether preferences differed among subgroups of patients by interacting dummy variables indicating subgroup membership with independent variables in the regression model. Preferences are considered to vary across the subgroups in a model if the parameters estimated for interaction terms are jointly statistically significantly different than zero.
The estimated parameters for attribute levels can be interpreted as ‘preference weights’. Within each attribute, preference weights are relative to the mean effect for that attribute; as part of the effects-coding methods, all mean attribute effects were normalized to zero. If the confidence intervals (calculated at the 95% level) around any two preference weights did not overlap, the differences between the preference weights were statistically significant at the 5% level or better (p ⩽ 0.05).
The preference weights can be interpreted in two ways [Hensher et al. 2005; Train, 2003; Train and Sonnier, 2005]. First, within each attribute, the vertical distance between any two preference weights is called the relative importance. The greater the vertical distance, the greater the importance placed on that change between the attribute levels. Second, the relative importance of changes within one attribute can be compared with the relative importance of changes within a different attribute to examine the trade-offs that patients would be willing to make across treatment features.
Results
Sample characteristics
Of 202 adults who responded and completed the survey, 13 (6%) were excluded from data analysis because they always chose either medication A or medication B in the treatment-choice questions; this may indicate that they did not pay close attention to the choice tasks. As a result, the final sample size for analysis was 189 patients.
Approximately 50% of all patients reported a diagnosis of RRMS, 31% reported secondary progressive MS (SPMS), 11% reported primary progressive MS (PPMS), and 3% reported progressive relapsing MS (PRMS) (Table 2). On most days, 10% had no limitations due to MS, 22% had mild symptoms (according to the Hohol scale), 30% had moderate symptoms on the Hohol scale, 18% of patients needed a cane for walking long distances, 9% needed a cane for short and long distances, and 4% needed bilateral support. Approximately 53% of patients had experienced FLS caused by their MS medication (Table 2), and 47% had experienced a mild ISR to their medication. Approximately 71% of patients had current or prior experience with injectable MS medication, and 12% had never been prescribed medication to take on a regular basis to manage their MS (Table 2).
Characteristics of the patients enrolled in the survey.
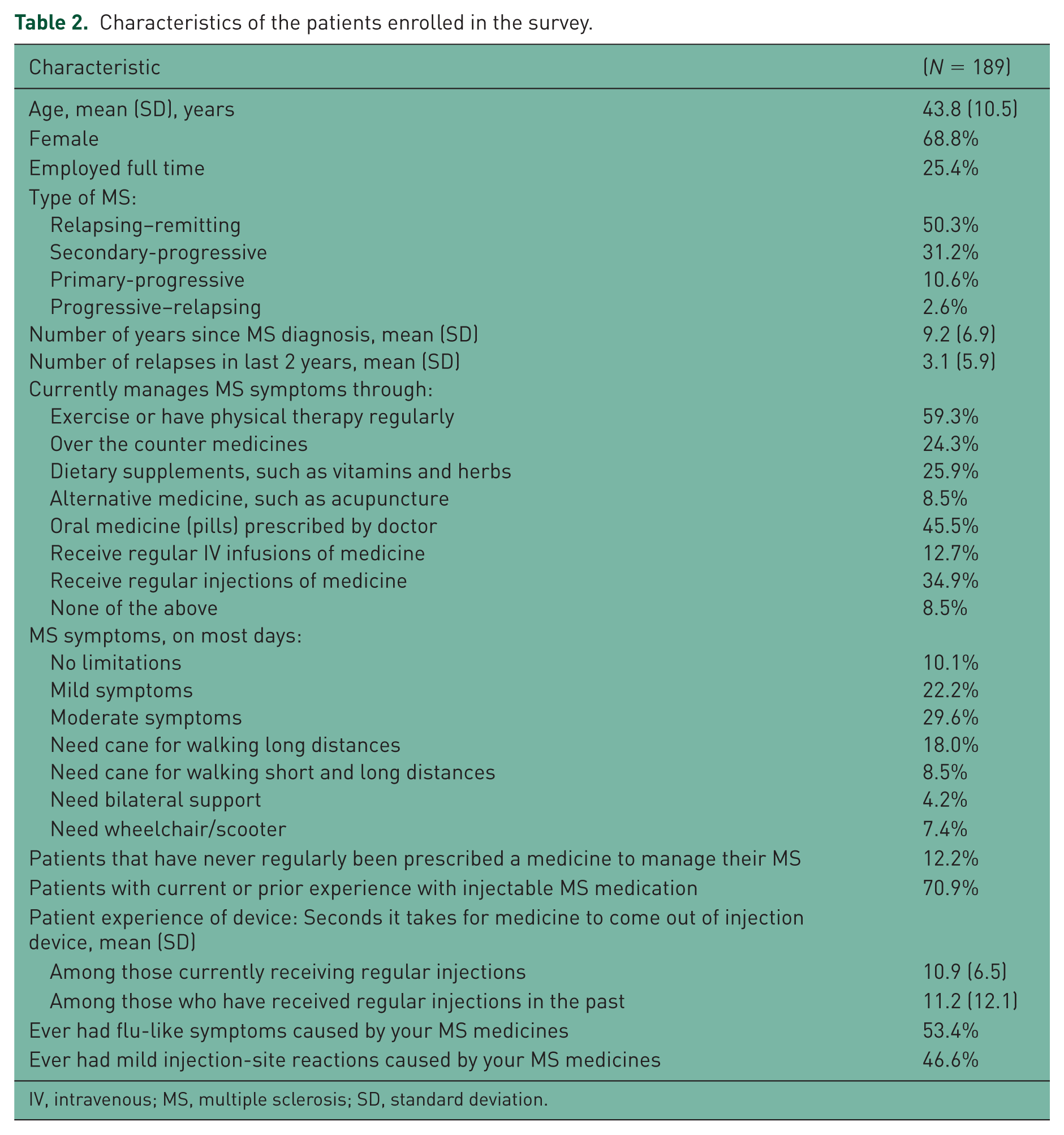
IV, intravenous; MS, multiple sclerosis; SD, standard deviation.
Preferences for selected attributes of injectable disease-modifying therapies
The results of the RPL estimation indicate that patient preferences were consistent with the natural ordering of each of the attributes, for example, one relapse in the next 4 years was preferred to two relapses in the next 4 years (p ⩽ 0.05) (Figure 2). Further, there was a statistically significant difference between at least two preference weights within each attribute, except injection time. The relative importance of an improvement in the number of years until MS symptoms get worse from 1 to 4 years (measured as the vertical distance between preference weights corresponding to these levels) was 2.1 (Figure 2). The relative importance of this change was the greatest, when compared with the relative importance of any other change amongst other attributes included in the study. Furthermore, it is approximately twice as important as a change from four relapses to one relapse in the next 4 years (2.1 versus 1.1), a change of 30 injections to 12 injections per month (2.1 versus 1.0), or a change in FLS presenting 3 days after every injection to 1 day after some injections (2.1 versus 1.0) (Figure 2).

Mean preference weights for the total study population (N = 189).
The relative importance of a change in the frequency of injections per month from 12 to 2 was 0.7 (Figure 2). The relative importance of this change was approximately equivalent to the relative importance of the number of relapses in the next 4 years from three to one (0.6), or an improvement from 1 to 2 years in the number of years until MS symptoms get worse (0.6).
Data from the three additional RPL models explored interactions between frequency of injections per month with injection time, FLS and ISR. None of these interactions were found to be statistically significant (p > 0.05), suggesting that preferences for injection time, FLS, and ISR do not vary systematically with frequency of injections per month (data not shown).
Discussion
This study used DCE methodology to evaluate preferences of patients in Germany for different attributes of a hypothetical injectable MS treatment. As expected, patients preferred an improvement in outcomes for each attribute, which is consistent with the results of previous DCE studies [Johnson et al. 2009; Shingler et al. 2013; Poulos et al. 2015; Utz et al. 2014; Wicks et al. 2015; Wilson et al. 2014, 2015].
There were no significant differences in preferences among patients reporting a diagnosis of RRMS versus patients reporting other types of MS (including those who did not know what type of MS they had). There was also no statistically significant difference between the preferences of patients who were treatment-experienced and the patients who were treatment-naïve across all attribute levels (online supplementary material, Figure S1). Nor was there a statistically significant difference between preferences of patients who were injection-experienced versus patients who were injection-naïve, across all attribute levels (online supplementary material, Figure S2). These data suggest that although patients have different actual experiences with respect to injections, treatments, and their MS type, all patients included in the sample have similar preferences regarding features of hypothetical injectable DMTs.
Overall, frequency of injections and disability progression were the two key drivers for patient preference. Specifically, the relative importance of a change in frequency of injections from 30 injections per month to one injection per month and an improvement in the number of years until MS symptoms get worse from 1 to 4 years, were almost twice as important as an improvement in number of relapses from four relapses to one relapse or an improvement in FLS from 3 days after every injection to none. These results suggest, that patients do differentiate between injectable treatments based on injection frequency. This is consistent with data presented in previous studies [Poulos et al. 2015; Shingler et al. 2013; Utz et al. 2014; Wicks et al. 2015]. The change in injection time was not shown as being important to patients compared with the other attributes studied. Regarding the tolerability of treatments, patients showed a strong negative preference towards FLS, which would be experienced for 3 days, after every injection.
Together, these data support the evidence that a perceived lack of efficacy and treatment-related AEs remain a concern for patients with MS [Treadaway et al. 2009; Patti, 2010; Shingler et al. 2013].
Disease severity is classified by the Hohol disease step scale [Hohol et al. 1995].
Mild symptoms. These patients have mild but definite findings such as sensory abnormalities, mild bladder impairment, minor incoordination, weakness, or fatigue. There is no visible abnormality of gait. The pattern of disease is relapsing–remitting, but patients may not have a full return to baseline following attacks. These patients may use ongoing symptomatic therapy such as amantadine, baclofen, or oxybutynin.
Moderate symptoms. The main feature is a visibly abnormal gait, but patients do not require ambulation aids. The pattern of disease is relapsing–remitting or progressive.
Of the patients who reported that their ‘current’ symptoms were moderate or worse (n = 128 [67.7%]) and the patients who reported that their ‘current’ symptoms were mild or better (n = 61 [32.3%]), there were no significant differences in overall preferences for treatment attributes. However, patients with mild or better symptoms placed greater weight on having only one relapse over the next 4 years than patients with moderate or worse symptoms (p < 0.01). Interactions between frequency of injections per month and injection time, FLS, and ISR were not statistically significant. We therefore did not find any evidence that preferences for these three attributes were dependent on the level of injection frequency.
There are limitations to DCE which should be taken into consideration when evaluating these data. Not all of the attributes related to injectable DMTs which would influence or affect patients’ treatment choice were incorporated in the study. The set of attributes selected was chosen to be sufficient to cover only the fundamental aspects of injectable DMTs.
Patients were aware that the questions were regarding a hypothetical device and actual device choice may be influenced by factors not assessed in this study (e.g. financial factors such as treatment cost).
With regard, to the study populations assessed, the patients had a ‘self-reported physician diagnosis of MS’; therefore, it is difficult to evaluate how representative this sample is of a typical patient population with MS. There is a small possibility that some of the survey respondents were not patients with MS, and participated in the survey to earn modest compensation (€5). Also, given the sample size of the study population, we acknowledge that the data may not be representative of all individuals with MS in Germany. No evidence was found that preferences among patients with and without injection experience or those patients who were treatment-experienced and treatment-naïve were statistically different from one another.
The survey instrument was translated from English into German by a professional translation service, and the survey was adapted to the local context. The instrument was pretested in German and, based on the pretest findings, revised by native German speakers with expertise in DCE studies. Despite the care taken in translation and adaptation of the survey instrument, the survey was not back-translated and reconciled with the English survey to ensure that the survey content was equivalent. It is possible that patients’ perceptions of the meaning of the descriptions and survey questions were somewhat different than we have described in this manuscript due to possible discrepancies in the translation.
Finally, when interpreting these results, it should be noted that they do not indicate the overall importance of treatment attributes, but rather, the importance of changes in attribute levels that lie within the ranges included in this study. Also, despite several of the attributes that are used in this study having been previously shown to influence adherence, these results do not describe actual adherence, or even intended adherence.
Conclusions
Understanding which attributes of injectable DMTs influence patient preference could help improve wellbeing and, potentially, treatment adherence in patients with MS. This study provides evidence that patients place a significant value on improvements in the frequency of dosing and disability progression. The results also suggest that changes in injection frequency may be as important as some changes in efficacy or safety attributes of injectable treatments for MS.
The majority of the attributes examined did have an influence on preference, suggesting that DMT attributes are carefully considered by patients and may influence patient adherence. This should be taken into consideration by physicians when selecting appropriate treatments for patients with MS.
Footnotes
Acknowledgements
The authors express their gratitude to Juan Marcos Gonzalez and A. Brett Hauber of RTI Health Solutions for their contributions to the data analysis in this study. The authors would also like to acknowledge Alex Goonesinghe (CircleScience) for editorial support in the preparation of this manuscript, which was funded by Biogen.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study that is the subject of this manuscript was conducted by RTI Health Solutions and funded by Biogen.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Poulos and J. Posner are employees of RTI Health Solutions, an independent scientific research organization; J. C. Yang was an employee of RTI Health Solutions at the time of the study. E. Kinter and E. Gleißner are employees of Biogen. J. F. P. Bridges, A. Mühlbacher, and B. Kieseier were expert consultants who were paid by Biogen for participating in this research study, but not for the contributions on authoring this paper. Subsequently, B. Kieseier became an employee of Biogen. The authors have full control of all primary data and agree to allow the journal to review the data if requested.
Ethical standards
The study was approved by an institutional review board (IRB) at RTI Health Solutions in the US. The IRB operates under a Federal Wide Assurance (#3331) and is registered with both the Office for Human Research Protections and the United States Food and Drug Administration. The study was reviewed for compliance with relevant German human subjects’ regulations. All patients provided informed consent prior to their inclusion in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.