
Abstract
Patients with multiple sclerosis (MS) are at increased risk for comorbid sleep disturbances, which can profoundly contribute to poor functional status and fatigue. Insomnia, sleep-disordered breathing, and restless legs syndrome are among the most common sleep disorders experienced by patients with MS. Despite their impact, these underlying sleep disorders may escape routine clinical evaluations in persons with MS, thereby leading to missed opportunities to optimize functional status and quality of life in patients with MS. A practical, systematic approach to the evaluation and treatment of sleep disorders in MS, in the context of MS-specific variables that may influence risk for these conditions or response to therapy, is recommended to facilitate early diagnosis and successful treatment. This review summarizes the most common sleep disorders experienced by persons with MS, and offers a practical approach to diagnosis and management of these conditions.
Keywords
Introduction
Multiple sclerosis (MS) is an autoimmune disease of the central nervous system (CNS) that causes inflammation and destruction of the brain and spinal cord. This debilitating neurologic disorder affects nearly half a million Americans, and is the leading cause of nontraumatic disability among young adults.
In addition to neurological morbidity, MS is associated with a disproportionately high prevalence of sleep disorders. Obstructive sleep apnea (OSA), restless legs syndrome (RLS), and chronic insomnia in particular are frequent problems in the MS population, and play a key role in the development of debilitating fatigue and other poor functional outcomes in MS. Yet, despite their impact, sleep disorders in MS remain critically under recognized in most clinical settings.
This review offers a practical approach to the diagnosis and treatment of the most common sleep disorders experienced by patients with MS, with a focus on insomnia, sleep-disordered breathing, RLS, and periodic limb movement disorder (PLMD). Each sleep disorder is discussed within the context of specific clinical features of MS that may exacerbate or mimic these conditions, or influence treatment options. Rapid eye movement (REM) sleep behavior disorder and narcolepsy are also briefly discussed. A recommended approach to the fatigued patient with MS is also highlighted.
Fatigue and other consequences of sleep disorders in MS
Fatigue affects up to 90% of patients with MS at some point during their disease course [Krupp et al. 1988; Janardhan and Bakshi, 2002; Krupp, 2006; Lerdal et al. 2007]. This highly debilitating symptom imposes significant socioeconomic consequences, and is a leading cause of diminished quality of life among individuals with MS [Janardhan and Bakshi, 2002]. Although MS-related fatigue is often multifactorial, identification of treatable causes that may contribute to its severity is an essential element of care for patients with MS (Figure 1).

Systematic approach to the identification of reversible causes of fatigue and sleepiness.
While the primary mechanism(s) underlying fatigue in MS are still largely speculative [Roelcke et al. 1997; Flachenecker et al. 2004; Tartaglia et al. 2004; Heesen et al. 2006; Tellez et al. 2008], several treatable comorbidities, including sleep disorders, are well recognized as important secondary causes of fatigue in MS. Recent studies suggest that insomnia, OSA, and RLS are independent predictors fatigue in MS [Veauthier and Paul, 2012; Braley et al. 2014b; Brass et al. 2014]. Early data also suggest that successful treatment of these conditions may improve fatigue [Cote et al. 2013; Veauthier et al. 2013]; yet, these conditions remain significantly under recognized in this population [Braley et al. 2014b; Brass et al. 2014]. Several reasons may exist. At first glance, complaints of fatigue in a patient with MS may not trigger a detailed survey of underlying causes, as clinicians often assume that most patients with MS are fatigued by virtue of their neuroimmunological condition. Consequently, many fatigued patients with MS with sleep disorders may escape thorough sleep evaluations.
Furthermore, fatigue is a highly individualized symptom with overlapping descriptors and concomitant symptoms [Braley et al. 2012a]. Although common synonyms include tiredness, lack of energy, lassitude, decreased motivation, weariness, and asthenia, patients with sleep disorders may also use the term fatigue interchangeably with sleepiness – a term more readily recognized as an indication that problems with sleep may exist [Chervin, 2000].
An improved understanding of these subjective symptoms will provide the best chance of identifying treatable causes of fatigue and related symptoms in patients with MS. One useful strategy is to start by asking the patient about his or her level of energy. Often patients will endorse terms such as ‘low energy’, ‘fatigue’, or ‘tiredness’; but they should be asked to provide their own descriptions of what these terms mean to them to avoid any misconceptions. As patients with sleep disorders often prefer terms other than sleepiness to describe their symptoms [Chervin, 2000; Braley et al. 2012a], it is possible that the term ‘sleepiness’ might not be endorsed by the patient, even with close-ended questioning.
More specific queries regarding associated symptoms, as well as aggravating and alleviating factors, are also useful. For example, if the problem is reported to be worse during sedentary, monotonous activities rather than during extended physical or cognitive activity, or if the patient endorses a propensity to doze off during sedentary activities, excessive sleepiness is more likely than fatigue.
Another helpful approach is to ask the patient about his or her ability to sustain daily tasks. The Multiple Sclerosis Council for Clinical Practice Guidelines defines fatigue as ‘a subjective lack of physical and/or mental energy that is perceived by the individual or caregiver to interfere with usual or desired activity’ [Paralyzed Veterans of America, 1998]. In contrast to excessive daytime sleepiness, if the patient feels most energized at the start of their day or at the beginning of a specific activity, but develops a sense of diminishing physical or mental energy over time or with prolonged activity [Claros-Salinas et al. 2010; Feys et al. 2012], fatigue is more likely to be a medically accurate characterization of the problem. Nonetheless, while such descriptions may be useful to distinguish symptoms of fatigue from sleepiness, few if any data exist that directly contrast phenotypic differences in fatigue that arises from MS versus fatigue secondary to an underlying sleep disorder in this population.
To screen for fatigue and sleepiness in clinical practice, brief self-report instruments can be useful (Table 3). The Fatigue Severity Scale is a nine-item questionnaire that assesses the impact of fatigue on multiple outcomes. It is validated for use in MS, and is sensitive to change over time, making it a useful took to track the effects of interventions [Krupp et al. 1989]. The Epworth Sleepiness Scale is an eight-item questionnaire that measures subjective sleepiness, or likelihood of dozing in various situations. While not specifically validated in patients with MS, it has been extensively utilized in a variety of outpatient settings and as a primary measure of sleepiness in MS research studies [Johns, 1991; Veauthier et al. 2011; Kaminska et al. 2012; Braley et al. 2014b; Brass et al. 2014].
Sleep disturbances are also associated with mood disorders and poor quality of life in MS, and should be recognized as potential contributors to these conditions. Bidirectional relationships between sleep disturbances, pain, and depression are common [Boe Lunde et al. 2012; Neau et al. 2012]. Sleep disturbances may also be key mediators of relationships between some of the most debilitating chronic symptoms in MS [Amtmann et al. 2015].
Insomnia
Definition/epidemiology
In simplest terms, insomnia is characterized by difficulty initiating or maintaining sleep. Insomnia can exist as a symptom, or as a disorder, in which case symptoms of insomnia must be associated with some form of distress about poor sleep, or lead to impairments in social, academic, or vocational functioning. The International Classification of Sleep Disorders Diagnostic Manual Third Edition (ICSD-3) defines insomnia as ‘a persistent difficulty with sleep initiation, duration, consolidation, or quality that occurs despite the opportunity and circumstances for sleep, and results in some form of daytime impairment’ [American Academy of Sleep Medicine, 2014]. Impairments in daytime functioning may include symptoms of fatigue, impaired concentration or memory, mood disturbances, excessive daytime sleepiness, behavioral problems, reduced motivation or energy, impaired social, family, academic, or occupational performance, proneness to errors, and concerns or dissatisfaction with sleep (Table 1). The ICSD also specifies that the sleep/wake difficulty cannot be better explained by another sleep disorder [American Academy of Sleep Medicine, 2014].
Summary of common diagnostic features, differential diagnoses, diagnostic testing and treatment modalities for chronic insomnia, obstructive sleep apnea (OSA), and restless legs syndrome (RLS) in persons with multiple sclerosis.

PLMD, periodic limb movement disorder; PSG, polysomnography; GERD, gastroesophageal reflux disease; ETOH, alcohol.
Importantly, the ICSD also delineates specific clinical and pathophysiological subtypes of insomnia based on etiology. Subtypes include insomnia due to a medical condition and insomnia due to another mental disorder. Within this framework, up to 40% of patients with MS may therefore be at risk for this disorder [Braley et al. 2014b; Brass et al. 2014]. Some of the most common symptoms experienced by patients with MS, including chronic pain, symptoms of neurogenic bladder, spasticity, and comorbid anxiety and depression, all have the potential to interfere with sleep initiation, sleep maintenance, or sleep perception [Stanton et al. 2006; Braley et al. 2014b], and should be viewed as potential exacerbating factors for insomnia. Concomitant sleep disorders can also contribute to insomnia symptoms in MS. Additional epidemiological studies that more precisely estimate the prevalence of primary chronic insomnia in MS, in the absence of a concomitant sleep disorder, are still needed.
Diagnostic approach
We recommend that all patients with MS who endorse daytime impairment or express concerns about prolonged sleep latency, fragmented sleep, unrefreshing sleep, or early terminal awakenings be evaluated for insomnia. A useful screening tool to identify such patients is the Insomnia Severity Index (ISI) [Morin et al. 2011]. The ISI is a seven-item questionnaire designed to assess the nature, severity, and impact of insomnia in adults (Table 3). It is also a useful tool to monitor the effects of insomnia interventions. It is important to note that this tool does not allow for the assessment of opportunity and circumstances for sleep, so this must be assessed separately to ensure that the patient’s habits and environment are not contributing to the sleep disturbance.
Elevated ISI scores or other sleep complaints should prompt a systematic approach that integrates a comprehensive sleep history with a thorough assessment of MS-specific comorbidities and symptoms. If not initially volunteered, a thorough review of daytime symptoms should also be conducted to characterize any associated daytime distress or impairment. As with patients without MS, further inquiries should be directed toward external factors or habits that may interfere with sleep hygiene.
An in-depth review of systems is crucial to identify potential exacerbating factors that can influence insomnia diagnosis or treatment [Chesson et al. 2000]. Patients should be asked about the frequency and severity of nocturnal pain, spasticity, urinary frequency, depression, and anxiety, preferably in conjunction with the sleep history.
Medications used to alleviate MS-related symptoms, including over-the-counter medications, also have the potential to interfere with sleep. Given the high frequency of utilization of these medications in this population, careful efforts should be directed at screening for these medications and assessing possible effects on sleep. Selective serotonin reuptake inhibitors, while helpful for depressive symptoms, may worsen insomnia [Byerley et al. 1988]. Stimulants and wake-promoting agents, which are commonly used for fatigue, may interfere with sleep initiation if taken during the late afternoon or early evening hours. Antihistamines, which are used as sleep aids by up to 25% of patients with MS [Braley et al. 2015] have the potential to worsen RLS [Bliwise et al. 2014], and thereby worsen sleep-onset insomnia.
Formal sleep testing [nocturnal polysomnography (PSG)] is not routinely indicated to confirm a diagnosis of insomnia unless a concomitant sleep disorder such as OSA or PLMD (which may contribute to insomnia symptoms) is suspected.
As concomitant sleep disorders such as RLS, PLMD, and OSA have the potential to disturb sleep, according to ICSD guidelines, associated symptoms of insomnia in the setting of another primary sleep disorder do not necessarily warrant a concomitant primary diagnosis of chronic insomnia. Only in cases when the insomnia symptoms show some independence in terms of time course, or in cases when adequate treatment of the concomitant sleep disorder does not result in significant improvement of insomnia symptoms, should a diagnosis of concomitant chronic insomnia be considered.
Management
Amelioration of any precipitating causes of insomnia is a cardinal step in management, either prior to or in tandem with the initiation of first-line therapies (Table 1). Medications or substances that may contribute to insomnia should be reduced or discontinued, if possible. If stimulants are necessary, alternative dosing schedules that allow for earlier dose administration should be discussed. For patients with urinary urgency, a trial of an anticholinergic medication at bedtime can be considered. Those who endorse persistent urinary symptoms should be referred to urology.
Another important yet often overlooked contributor to insomnia in MS is β interferon use. β interferons are a class of immunotherapies used to prevent exacerbations in relapsing–remitting MS. Flu-like side effects, fatigue, reduced sleep efficiency, and insomnia are common side effects of these medications [Jankovic, 2010; Mendozzi et al. 2010; Nadjar et al. 2011; Boe Lunde et al. 2012], and may be minimized by switching from an evening to morning administration schedule [Nadjar et al. 2011].
If neuropathic pain or spasticity are contributing factors, effective medications that also have sedating properties may be reasonable first options. Tricyclic antidepressants and the α-2-δ ligand pregabalin [Cardenas et al. 2013] are useful agents for neuropathic pain in MS, and also have the potential to cause sleepiness. Similarly, antispasmodic agents such as baclofen or tizanidine may offer secondary benefits of hypersomnolence. Diazepam is also an effective antispasmodic agent in selected cases, but use should be restricted to early evening hours to avoid next-day carryover effects of sedation.
If comorbid symptoms are not significant, or if insomnia symptoms persist despite adequately addressing these issues, psychological and behavioral therapies can be considered. Enforcement of appropriate sleep hygiene is a reasonable first step. In many cases, however, a more formalized regimen is necessary.
Cognitive behavioral therapy for insomnia (CBT-I) promotes healthy sleep habits and applies strategies to correct psychological processes and cognitive distortions that can perpetuate insomnia. Multiple randomized controlled trials have demonstrated the effectiveness of CBT-I [Edinger et al. 2001; Edinger and Means, 2005; Sivertsen et al. 2006; Morin et al. 2009]. Cognitive behavioral therapy for insomnia is also an effective approach when treating patients with MS with comorbid depression [Baron et al. 2011]. Depression affects approximately 50% of patients with MS at some point during the disease course, and shares a common bidirectional relationship with insomnia [Figved et al. 2005]. Recent data show that rates of insomnia are higher in patients with MS and depression than in those with MS who do not have depression, and suggest that insomnia management should commence beyond the treatment of the underlying comorbid psychological disorder [Baron et al. 2011].
Pharmacological therapies can be considered if more conservative strategies have been exhausted or are not fully effective. While no MS-specific contraindications exist to use such agents, selection should be made with consideration of other comorbid symptoms or diseases. Benzodiazepines, benzodiazepine agonists (zolpidem, zolpidem extended release, zaleplon, eszopiclone), and a melatonin receptor agonist (ramelteon) are the most extensively studied pharmacologic hypnotic therapies for chronic insomnia.
Orexin receptor antagonists are also gaining recognition as novel therapies for insomnia. In August 2014, the US Food and Drug Administration (FDA) approved the first orexin receptor antagonist (suvorexant) for the treatment of chronic insomnia [Herring et al. 2012; Michelson et al. 2014]. While generally well tolerated, potential side effects include increased daytime somnolence or sedation, vivid dreams, worsening depression, and complex nighttime behaviors. Orexin antagonists are contraindicated in patients with concomitant narcolepsy.
Although the affordability and widespread availability of over-the-counter antihistamine-containing products make them a popular treatment for insomnia, it is recommended that these agents be avoided in patients with MS. Antihistamines have the potential to cause psychomotor impairment, and recent evidence suggests that antihistamines are independently associated with increased daytime fatigue in patients with MS [Braley et al. 2015].
Sleep-disordered breathing
Definition/epidemiology
OSA is characterized by repeated episodes of upper airway obstruction and hypoxia during sleep. This disorder affects at least 3% of the US population and represents a major public health challenge in the USA [Chervin, 2000; Mulgrew et al. 2007; Gottlieb et al. 2010; Redline et al. 2010; Ju et al. 2012; Peppard et al. 2013].
Recent data suggest an increased prevalence of OSA among patients with MS [Braley et al. 2014b; Brass et al. 2014]. Two recently published studies that assessed the frequency of patients with MS already diagnosed with OSA demonstrated a 4–21% prevalence. Furthermore, both studies also showed a strikingly high prevalence (38–56%) of patients who were at elevated risk for OSA, based on a validated screening tool [Chung et al. 2012].
Underlying neuroanatomical and immunological features associated with MS may in part explain this elevated prevalence. Maintenance of upper airway patency during sleep requires an increase in pharyngeal tone that is primarily mediated by efferent motor output from cranial nerves X and XII to the palatal and genioglossus muscles, respectively. This process is largely influenced by afferent sensory input from pressure receptors in the upper airway, peripheral chemoreceptors in the aortic and carotid bodies, and brainstem respiratory generators [Fogel et al. 2005; Jordan and White, 2008]. Pathophysiological processes that disrupt these tightly regulated brainstem pathways have the potential to impair nocturnal respiration [Losurdo et al. 2013; Brown et al. 2014]. In a previous cross-sectional study, subjects with MS referred for overnight polynsomnography, and particularly those patients with radiographic evidence of brainstem involvement, were found to have more severe OSA than control subjects also referred to a sleep laboratory but without MS [Braley et al. 2012b]. Among the subjects with MS, progressive MS subtypes and MS disease-modifying therapy use also predicted apnea severity. Disease-modifying therapy use in particular emerged as a strong predictor of reduced apnea severity, raising interesting possibilities about the role of local and/or systemic inflammation in OSA.
Like OSA, central sleep apnea (CSA) involves repeated complete or partial reduction of airflow, caused by an intermittent lack of respiratory effort. While the prevalence of CSA is less than that of OSA, patients with CNS disorders that affect pontine and medullary respiratory generators, including MS, may be at increased risk for this condition as well [Dyken and Im, 2009; Braley et al. 2012b; Dyken et al. 2012; Losurdo et al. 2013].
The detrimental effects of OSA in MS are well documented. Patients with MS who have a diagnosis of OSA and those at elevated risk for OSA have increased fatigue compared with undiagnosed or low-risk patients [Veauthier et al. 2011, 2012; Kaminska et al. 2012; Braley et al. 2014b; Brass et al. 2014]. OSA is also a predictor of diminished quality life in MS [Trojan et al. 2012], and preliminary research suggests that apnea severity may correlate with impaired cognition in MS [Braley et al. 2014a]. Given the frequent and possibly disproportionate effects of OSA in this population, early identification and treatment is critical.
Diagnostic approach
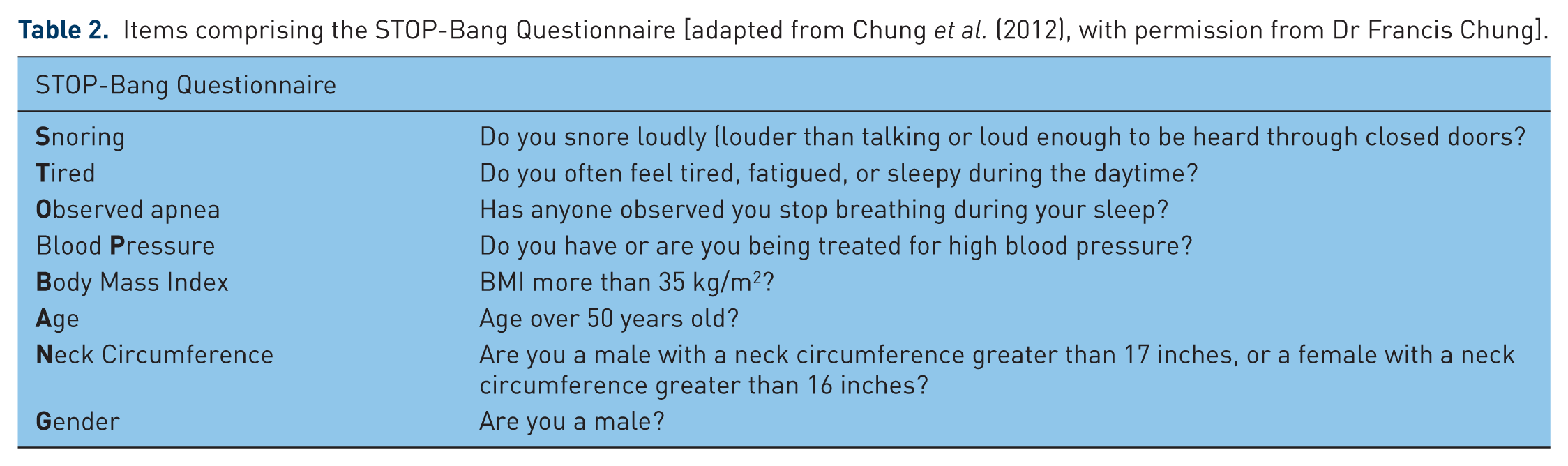
Given the high prevalence of OSA in MS, all patients with MS should be asked about symptoms of snoring, pauses in breathing witnessed by a bed partner, gasping or choking upon awakening, non-restorative sleep, excessive daytime hypersomnolence or fatigue, cognitive disturbances, and nighttime awakenings, any of which may arise in part from underlying OSA. Dysarthria or dysphagia, signs of brainstem dysfunction, may also signal high risk for OSA or CSA. Obesity, increased neck circumference, crowded oropharyngeal inlet, retrognathia, or micronathia are common physical exam findings associated with OSA and should, in conjunction with the above symptoms, prompt clinicians to consider a sleep clinic referral. No algorithm for OSA risk, specific for patients with MS, has been validated. However, considerable literature from the general population is likely to be relevant to screening among patients with MS. To facilitate a thorough screen of the most common symptoms and physical exam findings associated with OSA, several questionnaires are commonly used. The STOP-Bang questionnaire (Table 2) is a screening tool consisting of eight questions and measures that form the acronym STOP-BANG [Chung et al. 2012]. Scores of 3 or higher indicate elevated risk for OSA.
Items comprising the STOP-Bang Questionnaire [adapted from Chung et al. (2012), with permission from Dr Francis Chung].
To confirm the diagnosis of OSA, a full-night PSG is necessary to demonstrate the presence of obstructive respiratory events during sleep. These events may be partial (hypopneas) or complete (apneas), but must demonstrate evidence of a reduction in airflow during sleep, despite continued effort to breathe. A diagnosis of CSA requires PSG evidence of reduction in airflow in the absence of respiratory effort.
Management
Management strategies for sleep-disordered breathing should take into account the patient’s primary apnea subtype, apnea severity, comorbidities and behaviors, and other MS-specific symptoms or limitations. Guidance by a sleep medicine physician is often helpful.
The gold standard treatment for OSA, positive airway pressure (PAP) therapy, is delivered by a mechanical device and mask to splint the upper airway open during sleep. In addition to improvements in nocturnal oxygen saturation and sleep quality, previous studies suggest that PAP therapy effectively ameliorates fatigue in patients without MS [Chotinaiwattarakul et al. 2009].
Although the general benefits of treatment of OSA by continuous PAP are likely to be similarly beneficial among patients with MS, rigorous demonstration of effectiveness in patients with MS specifically has yet to be published. A previous noncontrolled study suggests that compliant PAP use ameliorates fatigue in patients with MS [Cote et al. 2013], but large-scale, controlled clinical trials that minimize selection bias are still needed to demonstrate its effects on fatigue and other MS-specific consequences.
If PAP therapy is selected, existing neurological deficits and symptoms should be taken into consideration when selecting a mask interface. For example, if patients have significant dexterity issues or hemiparesis, masks that involve complex fasteners or setup should be avoided. Patients with a history of trigeminal neuralgia may benefit from masks that minimize facial contact.
Although surgical approaches for OSA are also available, the underlying anticipation of changing neurological function among patients with MS usually makes surgery less attractive as a potentially permanent solution. Careful consideration of potential postsurgical risks is also necessary, and should involve consultation with an MS specialist, especially if patients are on concomitant immunosuppressive therapies.
In select cases, oral appliances may also be considered for the treatment of OSA. Oral appliances work by repositioning the mandible in the anterior and inferior position. These devices are considered by many as a useful conservative nonsurgical approach for the treatment of mild to moderate OSA, or snoring without OSA, due to their portability, size, and low cost [Ramar et al. 2015]. Although there are generally no MS-specific contraindications to oral appliances if otherwise clinically indicated, additional studies are necessary to determine their clinical utility and feasibility in MS. These devices may also be inappropriate for patients with trigeminal neuralgia who experience pain triggered by oral stimulation.
For the treatment of CSA, the current level of evidence suggests that treatment options be selected based on underlying pathophysiology and be tailored to the primary cause of CSA. Such treatment may include supplemental oxygen, bilevel PAP, adaptive servoventilation, or discontinuation of offending medication [Eckert et al. 2007]. As use of CNS depressing medications such as opiates or antispasmodics may also worsen CSA, these agents should be minimized whenever possible.
RLS/PLMD
Definition/epidemiology
RLS (also known as Willis–Ekbom disease) and PLMD are motor disorders of sleep [Allen et al. 2003; Hening et al. 2007]. Although considered separate clinical entities, both conditions have the potential to cause disrupted sleep, share a similar pathogenesis, and have an increased prevalence among persons with MS [Manconi et al. 2007, 2008; Deriu et al. 2009].
RLS is defined as a restlessness or uncomfortable sensation of the lower extremities that is exacerbated by rest and inactivity, has a tendency to occur in the evening or before bedtime, and is relieved with movement [Allen et al. 2003; Hening et al. 2007]. This condition affects approximately 10% of the general population [Rothdach et al. 2000] and is frequently present in patients with sleep initiation insomnia [Chesson et al. 2000]. RLS is classified as idiopathic or primary if no other cause can be identified, or secondary if caused by another comorbid medical condition known to increase vulnerability, such as MS. In MS, the prevalence of RLS is at least three times that of the general population [Auger et al. 2005; Manconi et al. 2007, 2008; Italian et al. 2008; Deriu et al. 2009; Li et al. 2012].
Periodic limb movements of sleep (PLMS) consist of rhythmic, stereotyped movements of the lower extremities during sleep. Although they are mentioned in this review due to their frequent association with RLS, PLMS also occur frequently in the absence of RLS. In the absence of sleep disturbances or daytime impairment, PLMS are considered a nonspecific polysomnographic finding, as opposed to a distinct disorder. PSG is required to assess for PLMS, whereas RLS is a clinical diagnosis that does not usually require PSG. If frequent PLMS are associated with significant sleep disruption or impairments in daytime functioning, in the absence of RLS or another sleep, neurological, or medical disorder, a diagnosis of PLMD may be made. Approximately 80% of patients with RLS also have PLMS [Montplaisir et al. 1997], yet only a limited proportion of individuals with PLMS have RLS.
Although the exact cause of idiopathic RLS is still unknown, a genetic etiology is favored [Winkelmann et al. 2007a, 2007b; Pichler et al. 2008], and dysfunction of brain circuits that require the neurotransmitter dopamine have been implicated in the pathogenesis [Cervenka et al. 2006]. Impaired iron metabolism is also thought to contribute to the pathogenesis of RLS, as iron is a cofactor for a rate-limiting step in the synthesis of dopamine. This hypothesis is supported clinically by lower serum and cerebrospinal fluid ferritin levels among patients with idiopathic RLS [Earley et al. 2005] and low brain iron stores in patients with RLS in magnetic resonance imaging (MRI) and autopsy studies [Allen et al. 2001; Connor et al. 2003].
Other investigators have proposed a role for dysfunction of downstream dopaminergic pathways, namely diencephalospinal and reticulospinal pathways [Frauscher et al. 2007], that project to the spinal cord. Via dopaminergic transmission, these pathways are responsible for the suppression of sensory inputs and motor excitability, and are susceptible to damage from diseases that affect the spinal cord. This hypothesis may explain the increased prevalence of secondary RLS in certain neurologic conditions, including spinal cord injury and MS [Manconi et al. 2007, 2008; Telles et al. 2011], and is supported clinically by work from Manconi and colleagues, who have demonstrated intriguing associations between RLS and measurements of decreased myelin integrity in the cervical spinal cord, using diffusion tensor MRI [Manconi et al. 2008]. Additional clinical evidence from Manconi’s group has also demonstrated a link between RLS and primary progressive MS subtype, as well as increased levels of neurologic disability [Italian et al. 2008], which also lend credence to a role for cervical cord pathology, given associations between progressive MS subtypes, increased neurological disability, and cervical cord pathology [Kearney et al. 2015; Kremenchutzky et al. 2006].
Currently, there is no evidence to support iron deficiency as a risk factor RLS in MS. In a case–control study of patients with MS and healthy controls with and without RLS, Manconi and authors demonstrated no significant difference in serum ferritin levels between patients with MS and controls, and no difference in ferritin levels between patients with MS with and without RLS [Italian et al. 2008].
Certain medications used in the management of persons with neurologic conditions, such as antiemetics, antipsychotic dopamine antagonists, antidepressants, and antihistamines, can also cause or worsen RLS. Our group previously demonstrated a significantly higher prevalence of RLS in patients with MS who endorsed the use of over-the-counter agents containing H1-receptor antagonists for sleep compared with patients who did not use these agents [Braley et al. 2015].
Diagnostic approach
RLS is characterized by four essential diagnostic criteria, including a restlessness or uncomfortable sensation of the lower extremities; that is exacerbated by rest and inactivity; has a tendency to occur in the evening or before bedtime; and is relieved with movement [Allen et al. 2003] (Table 1). In a busy clinical practice, if necessary, these criteria can be assessed sensitively with use of a single validated screening question: ‘When you try to relax in the evening or sleep at night, do you ever have unpleasant, restless feelings in your legs that can be relieved by walking or movement’ [Ferri et al. 2007]. Many descriptors can be used by patients to describe the restless sensation, including creeping, crawling, itching, burning, tightening, or tingling. Other patients will describe this sensation as painful [Bassetti et al. 2001].
In addition, the ICSD requires that the patient’s symptoms are not better accounted for by another medical or behavioral condition, and that these features cause some form of concern, distress, sleep disturbance, or daytime impairment for the patient.
Several other symptoms that may be particularly common in MS, such as cramping, clonus, spasticity, or in particular, neuropathic pain [Hening et al. 2009], can be difficult to discern from RLS and often require detailed, direct questioning. Neuropathic pain may be described as more noticeable to patients at night, when they are not distracted, which may suggest a circadian predilection. In this case, endorsement of relief with movement, even if the relief is only temporary while the movement continues, provides support for RLS. Persistent pain that is not ameliorated by movement suggests neuropathic pain. Spasticity or clonus may also become more noticeable to the patient at night, and during times of fatigue later in the day. In this case, queries to assess the nature of the leg movements are paramount. Symptoms of leg tightness relieved by voluntary movement suggest RLS, whereas involuntary spasms, even if a circadian component is endorsed, suggests spasticity. Rhythmic involuntary movements triggered by stretch or certain leg positions suggest clonus. In this regard, the Restless Legs Syndrome Diagnostic Index (RLS-DI) may be a useful tool to rule out false-positive diagnoses. The RLS-DI is a 10-item questionnaire designed to improve diagnostic decision making in suspected cases of RLS [Benes and Kohnen, 2009]. This instrument incorporates essential RLS diagnostic criteria with additional supportive criteria and features associated with RLS. Scores range from −22 (no RLS) to +20 (definite RLS). A score of +11 yields a 93.0% sensitivity and 96.1% specificity to accurately diagnose RLS.
Unlike RLS, a diagnosis of PLMD requires overnight PSG to assess for the presence of leg movements.
Management
To date, there are no MS-specific treatment guidelines for the management of RLS, but in the author’s experience, treatment should be tailored to the patient’s symptoms and other comorbid conditions whenever possible.
Despite the lack of available evidence to support a link between RLS and low ferritin levels in MS, as patients may have concomitant genetic risk factors for idiopathic RLS, iron studies are still recommended, and iron supplementation should be implemented for ferritin level less than 50 ng/ml. Reduction or discontinuation of medications and substances that can cause or worsen RLS or PLMD (dopamine antagonists, lithium, selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, antihistamines, tricyclic antidepressants, alcohol, tobacco, caffeine) [Lutz, 1978; Aldrich and Shipley, 1993; Ohayon, 2002; Pigeon and Yurcheshen, 2009; Hoque and Chesson, 2010] is also advised.
As in patients without MS, pharmacologic treatment for RLS should be individualized based on frequency and severity of symptoms. No FDA-approved treatments exist for PLMD, and off-label treatments for PLMs should be considered only if the patient endorses poor sleep quality or excessive daytime sleepiness secondary to the limb movements. Any patient receiving therapy for RLS or PLMD should be monitored for adverse side effects, augmentation, and tolerance.
Dopamine agonists (pramipexole, ropinirole, and rotigotine), and the α-2-δ ligand gabapentin enacarbil are the only FDA-approved first-line medications for moderate to severe RLS [Littner et al. 2004; Wilt et al. 2013]. Common side effects of dopaminergic agents, including nausea, hypotension, hallucinations, and dyskinesias, may dissuade use in patients with advanced MS who may suffer from concomitant autonomic dysfunction. Daytime sleep attacks and an increased risk of compulsive behaviors may also be rare consequences [Evans and Butzkueven, 2007]. Augmentation, a phenomenon that involves worsening of RLS symptoms earlier in the day with geographic spread to other body regions, is associated with dopaminergic agents in up to 80% of patients [Allen and Earley, 1996].
If dopaminergic agents are inappropriate or poorly tolerated, we favor the use of α-2-δ ligands for RLS in MS. Anticonvulsants, including gabapentin, carbamazepine, and most recently pregabalin [Allen et al. 2014], have been shown to be effective treatments for RLS and may be ideal choices for patients who suffer from concomitant conditions such as neuropathic pain or seizures, or for patients who have experienced significant issues with augmentation on dopaminergic agents (Table 1).
Benzodiazepines have also demonstrated therapeutic effect in RLS, although data supporting these agents are less robust, and their desirability is tempered by other benzodiazepine effects on sleep and daytime sleepiness [Chesson et al. 1999]. Various opioid agents, including oxycodone and methadone, may be of benefit in selected, but the addiction potential and side-effect profile associated with opioids limit their use, and they are generally not recommended in patients with MS.
Once RLS treatment has been implemented, a useful tool to track treatment response is the RLS Rating Scale [Walters et al. 2003]. Designed by the International RLS Study Group, this validated 10-item self-administered scale has been shown to predict RLS severity, and its impact, with high test–retest reliability (Table 3).
Survey instruments to consider when evaluating patients with multiple sclerosis (MS) for fatigue or sleep disorders.

For patients who meet International Restless Legs Syndrome Study Group criteria for the diagnosis of restless legs syndrome (RLS) [Walters et al. 2003].
OSA, obstructive sleep apnea.
REM sleep behavior disorder
REM sleep behavior disorder is parasomnia characterized as a loss of motor inhibition during REM sleep, resulting in excessive and sometimes violent nocturnal vocal or motor activity and dream enactment. The prevalence of RBD is less than 1% of the general population [Ohayon et al. 1997].
Both idiopathic and secondary forms exist. Idiopathic RBD is most common in male patients age 50 years or older, and is thought to be a form fruste of synucleinopathies, as the majority of patients who present with idiopathic RBD will eventually develop signs of a synuclein-mediated neurodegenerative disease [Iranzo et al. 2006; Postuma et al. 2009].
Secondary forms of RDB are most commonly associated with neurologic processes that affect pontine REM generators, including MS [Tippmann-Peikert et al. 2006]. Whereas one group reported PSG-confirmed RBD in 3 of 135 patients with MS (2 of whom were on antidepressants), population-based data are lacking and the prevalence of secondary RBD in MS is not known. Case reports have shown that in otherwise young and healthy individuals, RBD may be the first clinical manifestation of the disease [Plazzi and Montagna, 2002]. Numerous antidepressants have also been implicated in RBD or REM without atonia, but the clinical significance of this phenomenon as a possible predictor of neurodegenerative disease is still under speculation.
Overnight PSG is required to confirm loss of REM atonia, and rule out other conditions that may exacerbate or mimic RBD, such as sleep apnea, nocturnal seizures, or other parasomnias. As RBD is exceptionally rare in otherwise young adults and young women in particular, such individuals who present with symptoms of RBD should undergo a complete neurological workup with brain MRI. Patients with known MS who present with new-onset RBD should also be evaluated for signs of radiographic progression. Management includes incorporation of safety measures to avoid injurious behavior to the patient or the bed partner as a primary step. Common pharmacologic therapies that may be considered include clonazepam and melatonin.
Narcolepsy
Narcolepsy is characterized by abnormal manifestations of REM sleep intrusion into wakefulness. An irrepressible need to sleep or pathological daytime lapses into sleep are essential symptoms, often accompanied by cataplexy, sleep paralysis, and hypnagogic hallucinations. PSG with follow-on multiple sleep latency testing (MSLT) is required to establish a diagnosis.
While narcolepsy is estimated to affect 0.02–0.05% of the general population [Ohayon et al. 2005; Dauvilliers et al. 2007], the overall prevalence of narcolepsy among persons with MS is unknown. Two subtypes of primary narcolepsy exist. Narcolepsy type 1, distinguished by the presence of hypocretin deficiency, can be established clinically by the presence of cataplexy (a reliable clinical marker for hypocretin deficiency), or with CSF studies (hypocretin ⩽ 110 pg/dl or one third of normal mean values); and narcolepsy type 2, which is associated with normal hypocretin levels.
At present, CSF hypocretin assays are only performed at a few academic institutions. Con-sequently, in clinical practice a diagnosis of narcolepsy type 1 is most often established by the presence of cataplexy and an MSLT, which must confirm a mean sleep latency of up to 8 min and at least two sleep-onset REM periods (SOREMPs), though one of these SOREMPs may be replaced by a SOREMP seen on the preceding PSG. Such MSLT findings must also be present for the diagnosis of narcolepsy type 2. A diagnosis of narcolepsy cannot be established in the presence of concomitant untreated OSA, insufficient sleep, shift work, or another circadian sleep disorder. In such cases, adequate treatment of concomitant sleep disorders must be confirmed prior to the MSLT [American Academy of Sleep Medicine, 2014].
Recent evidence suggests that an immune-mediated loss of hypocretin-secreting cells in the lateral hypothalamus plays a role in the overwhelming majority of type 1 cases [De La Herran-Arita et al. 2013]. Narcolepsy is strongly associated with specific variations in HLA protein complexes DQ and DR. DRB1*1501, and in particular DQB1*0602, are among the strongest associated allelic variants; greater than 98% of patients with narcolepsy and hypocretin deficiency express DQ0602, a heterodimeric class II protein encoded by the HLA DQB1*06:02 and DQA1*01:02 gene variants [Hayduk et al. 1997; Lin et al. 2001; Mignot et al. 2001; Mahlios et al. 2013]. Close associations between MS and the HLA DRB1*1501 and DQB1*0602 haplotypes also allow speculation that narcolepsy, even in the absence of requisite identifiable hypothalamic lesions in secondary narcolepsy (see below), may share a causal link with MS, but proof is lacking. It is also important to note that approximately 25% of patients with narcolepsy with normal hypocretin levels will also express the HLA-DRB1*1501-DQB1*0602 haplotype, similar to what is seen in the general population [Mignot et al. 1997; Overeem et al. 2008; Andlauer et al. 2012].
Conditions that may affect the hypothalmus, including MS, may also cause secondary forms of narcolepsy, or narcolepsy related to a medical condition [Aldrich and Naylor, 1989; Vetrugno et al. 2009]. A previous report suggests that MS may be one of the most common causes of secondary narcolepsy [Nishino and Kanbayashi, 2005].
Consultation with a sleep specialist is recommended for narcolepsy management. Intermittent naps throughout the day may improve alertness and psychomotor performance. Wake-promoting agents or stimulants may be used to increase wakefulness and vigilance. Sodium oxybate (an endogenous metabolite of gamma-aminobutyric acid (GABA) that is FDA approved for cataplexy and hypersomnia) may be used in select cases [Xyrem International Study Group, 2005a, 2005b]. REM-suppressing antidepressants may be useful for cataplexy and sleep paralysis. In cases of secondary narcolepsy when new hypothalamic lesions are identified, a trial of high-dose steroids should be considered.
Special considerations for sleep medicine referrals
Although thresholds for sleep clinic referrals may vary among practitioners, several situations in our experience generally do merit early referral to a sleep medicine specialist, ideally a board-certified sleep medicine physician. Patients with suspected parasomnias or narcolepsy are usually referred for diagnosis and management by sleep specialists. Patients with chronic insomnia who may be candidates for CBT-I should be referred to a sleep psychologist experienced with this therapy, preferably someone with certification in CBT-I, or to a sleep medicine physician who is experienced with CBT-I. Patients with OSA who are having difficulty tolerating PAP, or those who do not respond optimally, may also benefit from a sleep clinic referral. Treatment for refractory RLS, or augmentation in response to dopaminergic therapy, also is likely to be optimized by sleep specialty care. Finally, as patients with MS like others with sleep disturbances may not present with classic symptoms of sleepiness, persistent fatigue despite other attempts to correct it should also prompt a sleep referral to assess for any underlying sleep disorder.
Conclusion
Sleep disorders are significantly under-recognized comorbidities in persons with MS. These sleep disorders can contribute significantly to fatigue, other daytime dysfunction, and poor quality of life. A systematic, practical approach that takes into account clinical features of MS is recommended to enhance recognition of these conditions and facilitate appropriate treatment. Clinicians caring for patients with MS should routinely screen for sleep disturbances and initiate diagnostic workups if clinically indicated. Some of the most commonly encountered, consequential, and yet treatable sleep disorders among patients with MS include chronic insomnia, OSA, and RLS. Unnecessary use of sedating medications or drugs that interfere with good sleep may also offer important opportunities to improve fatigue, sleepiness, or sleep among patients with MS. Sleep specialty referrals should be considered for management of conditions that require PSG diagnosis, for complex patients who present a diagnostic challenge, and for patients who do not respond to first-line treatments.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.