
Abstract
The treatment of neuropathic pain is difficult. Oral pharmaceuticals have significant side effects, and treatment efficacy tends to be modest. The use of topical analgesics reduces the potential for systemic side effects and allows direct application of medications to the area of pain. The natural spicy substance, capsaicin, has historically been known for its topical use. Capsaicin, once applied to the skin, causes a brief initial sensitization followed by a prolonged desensitization of the local pain nerves. This occurs through stimulation of the transient receptor potential vanilloid-1 (TRPV1) expressing pain nerve fibers. While low-dose capsaicin has not resulted in good efficacy, the larger dose 8% topical capsaicin has had some of the best data currently available in the treatment of post-herpetic neuralgia (PHN) and other neuropathic conditions. This paper discusses the data currently existing for capsaicin 8% in the treatment of PHN. It further reviews data for the low-dose capsaicin products and the current status in the development of other capsaicinoids, e.g. resiniferotoxin, and high-concentration liquid capsaicin.
Introduction
The treatment of chronic neuropathic pain has been a challenge to physicians for millennia. Despite the multiple approaches used, e.g. topical, pharmaceutical, behavioral and interventional, our current treatment methods still provide only modest efficacy in this difficult pain condition. In general, treatment is very complex and single agents are rarely adequately effective.
Capsaicinoids, the hot spicy ingredients in chilies, were described in ancient writings and documents for topical analgesic use. The mechanism of action is unique. There has been renewed interest in the development of capsaicinoids for the treatment of neuropathic pain over the last few decades and new products are either on the market or in development. Low-concentration (LC), i.e. <1.0%, and over-the-counter (OTC) capsaicin preparations have been available for decades, although these products have suffered from problems of efficacy and patient compliance, due to the fact that the application has to be performed multiple times a day for multiple days and months. However, higher concentrations have been shown to circumvent some of these problems. A much higher concentration capsaicin product, such as the capsaicin 8% patch (C8P), is a fairly new therapy that produces relief after a single topical application. Other newer capsaicinoid therapies are being developed, e.g. the high-concentration (HC; 10% and 20%) liquid capsaicin and resiniferotoxin, a natural substance present in a Moroccan cactus-like plant. This article is a review of capsaicinoids in the treatment of neuropathic and chronic pain.
Transient receptor potential channels
The generation of the pain signal in small nerve fibers, i.e. the nociceptors, can be envisioned in three phases: transduction, propagation and transmission. Previously research efforts have focused on propagation and transmission. However, with the discovery of the transient receptor potential (TRP) family of ion channels, transduction can now be a focus of treatment. These channels share homology and have a six-transmembrane loop through the cell membrane [Spicarová and Palecek, 2008].
TRP channels are selective for calcium and magnesium over sodium ions and can be activated by a variety of mechanisms. For example, the group of TRP channels called vanilloid (TRPV) is activated by high temperatures and low pH [Knotkova et al. 2008]. Among these, the TRPV1 channel was the first to be cloned and has been the most studied of the 28 or more currently know TRP channels. Both morphine and cannabinoids have been proposed to interact with the TRPV1 receptor as well [Knotkova et al. 2008]. TRPV1 expressing C-fibers can be activated by exogenous substances such as capsaicin and resiniferatoxin and naturally by tissue burns, noxious heat and spider toxins. In addition, certain enzymes and inflammatory mediators will modulate the TRPV1 receptor [Szallasi et al. 2007]. All of these stimuli, through the activation of the TRPV1 channels, can cause burning pain [Knotkova et al. 2008]. These channels normally open between 37 and 45°C, but when bound, the threshold decreases below 37°C or physiologic body temperature [Spicarová and Palecek, 2008]. Binding stimulates the exocytosis of substance P (SP) from nociceptors, leading to mast cell degranulation of histamine and serotonin release from platelets. Further, TRPV1s are expressed throughout the central nervous system in areas that process pain signals, and also appear to be upregulated in the setting of neuropathic pain [Giordano et al. 2012]. Further, with nerve damage there are posttranslational changes, trafficking and expression of TRPV1s, as well upregulation of TRPV1s in the bystander uninjured nociceptors [Kim et al. 2008; Szallasi and Blumberg, 1989]. Nociceptors send signals into the dorsal horn of the spinal cord. Signals are then transmitted to higher central nervous system (CNS) centers where pain is perceived. The signal is transduced and with the lowered threshold this results in propagation and transmission to central brain areas where the signal is interpreted as pain. TRPV1 has also a number of other functions besides pain, e.g. thermoregulation, which are beyond the scope of the current paper, but discussed elsewhere [Alawi and Keeble, 2010].
Capsaicin
Capsaicinoids first recorded use, in the form of chilies, for the treatment of pain dates back to 4000 BC [Schumacher, 2010]. Columbus brought back the chili to Europe in the 1400s for both its culinary and medicinal properties [Schumacher, 2010]. The first formal report of the pain-reducing properties of topical chili extract in the West appeared in 1850 as a recommendation for burning or itching extremities [Turnbull, 1850]. Chilies are not true ‘peppers’; rather, they belong to the genus Capsicum and are a fruit [Wikipedia, 2004a]. The ‘hotness’ of peppers is due to a different set of chemicals, piperines, rather than capsaicin and they belong to a different family, Piperaceae [Wikipedia, 2004b; Vriens et al. 2008]. The major nonendogenous capsaicinoids are capsaicin, dihydrocapsaicin, nordihydrocapsaicin, homodihydrocapsaicin and homocapsaicin. Capsaicin and dihydrocapsaicin account for approximately 90% of the naturally occurring capsaicinoids [Reyes-Escogido et al. 2011]. There are more than 20 known capsaicinoids and all are amides [Reyes-Escogido et al. 2011]. Research in the use of capsaicinoids for obesity, as antioxidants, anticarcinogens and analgesics is still ongoing [Reyes-Escogido et al. 2011]. Capsaicin, 8-methyl-N-vanillyl-6-nonenamide is the active ingredient in chilies that provokes burning and a flare and weal response. This response occurs rapidly while a poorly localized, protracted dull pain lingers from slow conducting C nerve fibers, all as a result of TRPV stimulation. Capsaicin will also cause a release of SP and calcitonin gene-related peptide from peripheral and central nerve terminals, contributing to the local flare (neurogenic inflammation) [Winter et al. 1995]. Heat hyperalgesia is the result to the reduction of heat pain thresholds in peripheral nociceptors. Neighboring areas of mechanical allodynia occur due to central sensitization of the dorsal horn sensory neurons.
The single application of capsaicin causes pain, however repeated applications causes analgesia through a defunctionalization or desensitization state of the C-fibers [Knotkova et al. 2008]. This has been called ‘a paradox’ and multiple mechanisms have been proposed. Defunctionalization or desensitization of nociceptors appears to be caused by localized nociceptor dysfunction and terminal axons destruction [Anand and Bley, 2011].
Capsaicin is poorly absorbed from the skin therefore LC OTC preparations do not develop adequate desensitization. HC capsaicin topicals, the C8P, HC liquids and injectable capsaicinoids are attempts to dose dependently hasten the desensitization/defunctionalization state and therefore pain relief. When capsaicin is compounded in a topical preparation at HC and administered as a single application, the analgesic benefit appears to last for several weeks. Since capsaicin does not affect the large nerve fibers involved in motor and sensory function (e.g. touch, vibration), and since systematic levels of capsaicin are very low when used topically, the regional approach represents a potential dramatic improvement in the treatment of neuropathic pain (and potentially other types of pain, vide infra).
LC capsaicin
LC capsaicin has been in use for decades and is available OTC in the United States. Unfortunately this treatment approach has poor to moderate efficacy and poor patient compliance [Derry and Moore, 2012]. Even though there has been interest in using capsaicin in a number of neuropathic pain disorders such as diabetic peripheral polyneuropathy (DPPN), human immunodeficiency virus neuropathy (HIVN) and post-herpetic neuralgia (PHN), many of the older studies yielded disappointing results perhaps due in part to weakness in tolerability, efficacy and adherence, of past available strengths of capsaicin, 0.025% and 0.075% [Rains and Bryson, 1995]. For example, 0.025% capsaicin cream was determined to be no better than the vehicle (not active) cream in a randomized, double-blind study of 30 patients with temporomandibular joint pain [Gallachia and Marcolongo, 1993].
As with PHN, other neuropathic pain conditions do not respond to low-dose topical capsaicin. A recent study, using OTC 0.025% capsaicin in a gel formulation, did not provide any significant pain relief in DPPN [Kulkantrokorn et al. 2012]. Substantially fewer studies examining the use of capsaicinoids for low back pain or myofascial pain have been published. In one such study, a randomized, double-blind, placebo-controlled study, compared the use of a topical capsaicin ‘plaster’, containing 11 mg of capsaicin per patch, with placebo in 154 chronic low back pain patients. A total of 60.8% of capsaicin-treated patients experienced 30% pain relief after 3 weeks of treatment (p < 0.02) versus 42.1% with placebo [Keitel et al. 2001]. A 0.1% capsaicin jelly has been tested in a pilot study for the treatment of migraine with positive results [Cianchetti, 2010].
A Cochrane review of the published randomized trials involving low-dose topical capsaicin concluded that ‘although topically applied capsaicin has moderate to poor efficacy in the treatment of chronic musculoskeletal or neuropathic pain, it may be useful as an adjunct […] for a small number of patients who are unresponsive to, or intolerant of, other treatments’ [Mason et al. 2004].
HC capsaicin: 8% patch and 10–20% liquid formulations
HC capsaicin preparations have demonstrated better analgesia. The use of the C8P has focused on three neuropathic conditions, DPPN, HIVN and PHN. In one study on HIVN, 7.5% topical capsaicin cream was applied. The patients experienced notable pain relief but required epidural anesthesia to tolerate the application [Robbins et al. 1998]. C8P capsaicin concentration is 100 times higher than OTC formulation. As mentioned previously, the C8P was designed to overcome some of the problems associated with delivery of OTC low-dose topical capsaicin formulations. In PHN it is applied for 60 minutes (for PHN) and then removed. The clinical trials were difficult to design, since blinding of a HC capsaicin presented a problem. These trials were not placebo-controlled, but rather a low concentration of capsaicin, 0.04% in patch form, was used as a comparator. They were randomized, double-blind, LC (0.04%) patch-controlled, parallel-assignment, multicenter, dose finding, 12 week clinical trials. There are six trials that have been listed in ClinicalTrials.gov (see Table 1). In phase II trials on C8P, a decrease of at least 33% was found in 42% of the patients compared with only 8% in the control group [De La Rue, 2003; Holdcroft, 2003]. In an open-label trial, pain relief was sustained for up to 12 months following a single application of the patch [Backonja et al. 2004]. However, not all clinical trials were positive. In a trial with 299 patients with PHN, the C8P was applied in a single application 30, 60 and 90 minutes for 12 weeks. There was a decrease in pain only in the 90 minute group, and the trial failed to meet significance. The open-label extension was terminated as well.
Capsaicin 8% patch and high-concentration liquid – clinical research.
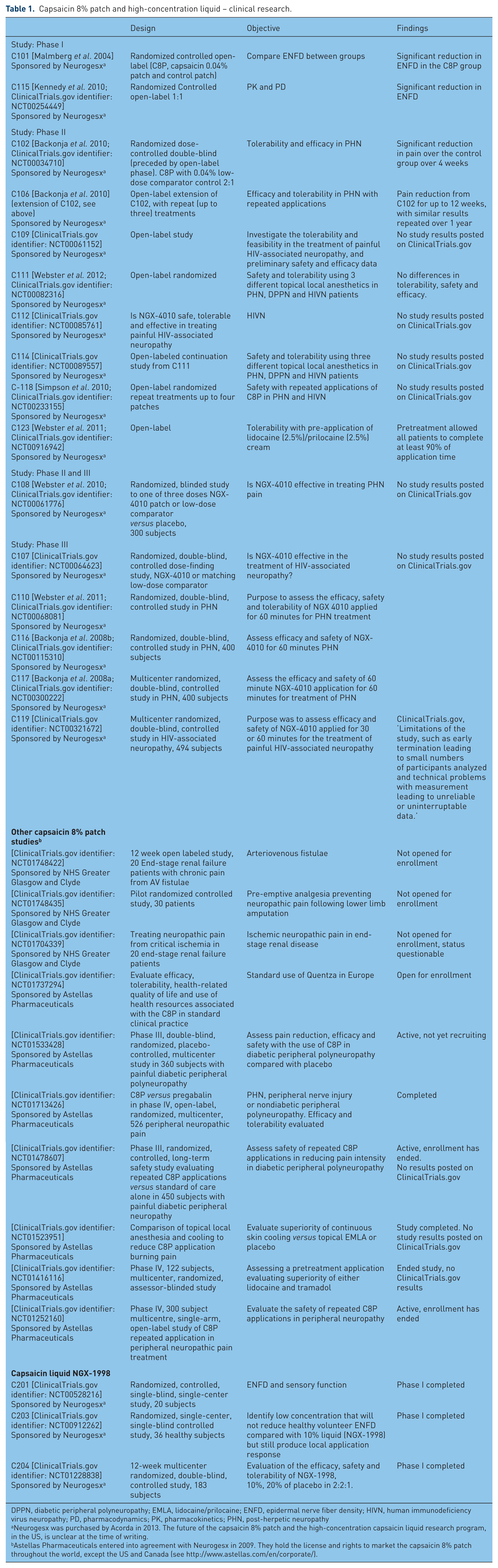
DPPN, diabetic peripheral polyneuropathy; EMLA, lidocaine/prilocaine; ENFD, epidermal nerve fiber density; HIVN, human immunodeficiency virus neuropathy; PD, pharmacodynamics; PK, pharmacokinetics; PHN, post-herpetic neuropathy
Neurogesx was purchased by Acorda in 2013. The future of the capsaicin 8% patch and the high-concentration capsaicin liquid research program, in the US, is unclear at the time of writing.
Astellas Pharmaceuticals entered into agreement with Neurogesx in 2009. They hold the license and rights to market the capsaicin 8% patch throughout the world, except the US and Canada (see http://www.astellas.com/en/corporate/).
The use of C8P, in the clinical trials, was found to be safe and generally well tolerated. The most commonly encountered side effects were dermal irritation, erythema and pain at the site of application. These were transient, but could be mild to moderate in severity. Local cooling and short-acting opioids were effective for this transient pain.
In trigeminal PHN patients, one case report suggests efficacy in the use of the C8P [Sayanlar et al. 2012]. In addition, there was a trial examining reapplication and retreatment of the C8P. The results of this trial showed that efficacy of the retreatment were similar to the initial treatment, 31%, 30% and 33% for the first, second and third retreatment cycles [Backonja et al. 2004].
A Cochrane collaboration review on ‘high concentration topical capsaicin’ (C8P) suggested that it was ‘similar to other therapies for chronic pain’ and that it is ‘likely to be used when other available therapies have failed’ [Derry et al. 2013]. The cost and need for repeated applications were part of the rationale for this statement. Of the 1272 patients treated with C8P for PHN the numbers needed to treat was 8.8 [Derry et al. 2013].
Recent studies using HC capsaicin in a liquid formulation, at 10% and 20% have been carried out (see Table 1) [Tobias et al. 2011a, 2011b]. These liquid preparations are currently in clinical trials [ClinicalTrials.gov identifiers: NCT00912262, NCT00130962]. Results from studies of the HC capsaicin liquid formulation in DPPN have not yet been published [ClinicalTrials.gov identifier: NCT01228838].
Other capsaicinoids
A much more powerful TRPV1 agonist capsaicin analog, resiniferatoxin, is currently being studied at the National Institutes of Health for intrathecal administration for intractable cancer pain in end-stage disease patients (see Table 2). This has been described as a ‘molecular scalpel’ and may achieve permanent pain relief in these patients.
Industry capsaicinoid pipeline (low-dose capsaicin studies not included).

N-palmitoyl-vanillamide (palvanil) is a nonpungent TRPV1 agonist capsaicin analog. In a recent study palvanil was injected subcutaneously using formalin-induced nocifensive behavior and carrageenan-induced edema and thermal hyperalgesia in the mice model. Analgesia was shown in a second mouse study as well [De Petrocellis et al. 2011]. Palvanil has fewer side effects than the typical TRPV1 agonists (hypothermia and bronchoconstriction), and appears to be still effective at reducing pain and edema [Luongo et al. 2012].
Endogenous TRPV1 ligands
Endogenous ligands of the TRPV1 channels, i.e. endovanilloids, have been identified. There are three lipid classes of such ligands, N-arachidonoyldop-amine, lipoxygenase products of arachidonic acid and anandamide [Van der Stelt and Di Marzo, 2004]. Anandamide, a cannabinoid receptor and TRPV1 ligand, has peripheral antinociceptive effect [Horvath et al. 2006].
TRPV1 antagonists
Further, TRPV1 antagonists have been developed and investigated as potential options for the treatment of pain. Table 3 gives a listing of what is currently listed on ClinicalTrials.gov. There is only one trial currently enrolling. These compounds have been plagued with significant side effects. TRPV1 antagonists have been included for completeness, since they were developed with the goal of pain reduction.
Industry TRPV antagonist pipeline.

TRPA1, transient receptor potential cation channel, subfamily A, member 1; TRPV1, transient receptor potential vanilloid-1; PHN, post-herpetic neuropathy
Mentioned by Szallasi and Shera [2012]; not found on ClinicalTrials.gov or on the Glenmark website.
Listed on the Glenmark website, see footnote; not listed on ClinicalTrials.gov
Mentioned by Szallasi and Shera [2012] and on the PharmEste website (http://www.pharmeste.com/home.asp?op=interna&id=2&id_pag=10&tit=Pipeline); not found on ClinicalTrials.gov.
Conclusion
In the United States, and worldwide, neuropathic pain and mixed states of chronic neuropathic–inflammatory pain still represent a tremendous challenge. The treatments that currently exist are only moderately effectively. Frequently these patients need a multidisciplinary and multimodal approach to significantly influence their pain [Gidal and Billington, 2006]. However, new treatments are being developed and higher concentrations of capsaicin, as well as other capsaicinoids, are some of these. Unfortunately due to the parent company’s shortage of funds, the future in the research program for the HC capsaicin products is unclear [Leuty, 2013]. In addition, although difficult data to obtain, topical agents do not have a large market share in the treatment of chronic pain. The total market for OTC analgesics alone is estimated at US$2.38 billion [The Pharma Letter, 2013]. In 2007 the market for topical analgesics, non-OTC, was only US$40 million [Millennium Research Group, 2013]. Data suggest that these treatments are underutilized.
The ability to determine which neuropathic pain patient will respond best to a given treatment is still an eluding challenge. However, recent data suggest that there may be approaches which might allow us this ability. Martini and colleagues and Gustorff and coworkers suggest that the actually available topical treatments reduce spontaneous neuropathic pain and affect predominantly mechanical hyperalgesia [Martini et al. 2012; Gustorff et al. 2011]. This may serve as a key marker to predict outcome with the use of these products. Clinical predictors such as pain intensity and the etiology or type of pain do not seem to serve as predictors of treatment response. However, other characteristics that seem to suggest response are intriguing and research in defining predictors of efficacy of a given treatment continues [Martini et al. 2012; Gustorff et al. 2011].
The future is daunting in both the understanding of the physiology of the TRP receptors, the development of new analogs and ligands but also in developing approaches that will select patients who will respond best. This will require extensive research in all these areas.
Footnotes
Conflict of interest statement
In the last year, JP has received consulting and advising fees from Ameritox, Endo Pharmaceuticals, INSYS Therapeutics and Zogenix Pharmaceuticals. In the last year, MP has received consulting and advising fees from Grunenthal.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.