
Abstract
Background:
Factors influencing the timing to endoscopic retrograde cholangiopancreatography (ERCP) drainage in patients with periampullary cancer diagnosed due to jaundice, as well as the impact of drainage delay on survival, remain poorly understood.
Objectives:
To evaluate the impact of clinical and social determinants on time to ERCP and 1-year mortality in patients with periampullary cancer diagnosed due to jaundice.
Design:
Multicenter retrospective study.
Methods:
All ERCP performed for periampullary cancer diagnosed due to jaundice between January 2010 and December 2020 were included. Determinants associated with early ERCP (defined as ⩽3 days from diagnostic imaging) were assessed using logistic regression. Factors associated with 1-year mortality were analyzed using a multivariate Cox model.
Results:
Five hundred ninety-four ERCPs were performed, with a median time to intervention of 9 days. Early ERCP (⩽3 days) was associated with improved survival in univariate analysis (hazard ratio (HR) = 0.66; 95% confidence interval (CI) (0.45–0.96)), but not in the multivariate model. In multivariate analysis, acute cholangitis (HR = 1.51; 95% CI (1.03–2.22)), age (HR = 1.03; 95% CI (1.01–1.04)), metastatic disease (HR = 1.76; 95% CI (1.21–2.57)), and ERCP technical success (HR = 0.59; 95% CI (0.42–0.83)) were associated with 1-year mortality. Only total bilirubin (odds ratio (OR) = 2.24; 95% CI (1.18–4.23)) and prothrombin time (OR = 1.02; 95% CI (1.01–1.04)) influenced time to ERCP. Social determinants had no significant impact on time to ERCP or overall survival.
Conclusion:
Time to ERCP does not appear to influence overall survival in patients with periampullary cancer diagnosed due to jaundice. Overall survival and time to ERCP seem to be influenced by clinical factors, with no apparent effect of social determinants.
Plain language summary
Cancer of the biliary-digestive junction is a common clinical situation, most often discovered upon the onset of jaundice caused by obstruction of the bile ducts. In most cases, this condition requires biliary drainage via endoscopy (ERCP). The time taken to manage the cancer may impact its prognosis. However, very little is known about the factors influencing the time to access endoscopic drainage. Beyond the classic clinical determinants, it is now well established that social and/or geographic factors can also influence the prognosis and management of many diseases. In terms of access to endoscopic drainage, jaundice would lead to faster management than other functional symptoms such as pain or general deterioration. Regarding non-clinical determinants, access to ERCP could depend on the place of residence, with more limited access for populations living in rural areas. We therefore conducted a study aimed at identifying clinical and non-clinical (social or territorial) factors that influence the time to access ERCP in patients diagnosed with biliary-digestive junction cancer based on jaundice. We also studied the impact of these factors and the delay in access on disease prognosis. To do this, we collected all ERCPs performed for endoscopic drainage of jaundice leading to the diagnosis of biliary-digestive junction cancer in a specific region: Calvados (France), between 2010 and 2020. In a cohort of 594 ERCPs, we showed that only clinical factors (particularly the severity of the jaundice) influenced the time to endoscopic drainage. This delay and nonclinical determinants have no impact on one-year survival, in contrast to classical clinical factors such as age or disease stage. Acute cholangitis, which corresponds to an infection of the bile ducts due to the obstruction, also appeared to be an independent factor of poor prognosis. Our work shows that the prognosis of this disease is still primarily determined by clinical factors.
Introduction
Jaundice is the presenting symptom in up to 80% of patients with neoplastic lesions at the biliopancreatic junction. 1 Patients presenting with jaundice at diagnosis tend to have a poorer prognosis,2–5 a trend that persists even among those with resectable disease. 3
In the majority of cases, this diagnostic situation necessitates biliary drainage prior to treatment, most often via an endoscopic approach. 6
Studies have shown that time to treatment initiation does not appear to influence the prognosis of pancreatic cancer in the global population,7,8 among resected patients 9 or in those with metastatic disease.10,11 However, when focusing specifically on potentially resectable patients—as opposed to those who have already undergone resection—time to surgical intervention does appear to affect prognosis.12,13 In a registry-based study of 29,167 potentially resectable patients, those who began oncologic treatment within 6 weeks of diagnosis had significantly better overall survival compared to those treated after 7 weeks. 12 In the study by Sanjeevi et al., the interval between imaging and surgery impacted the final resectability of lesions, even in patients with tumors smaller than 3 cm at diagnosis. 13 More recent studies have demonstrated an effect of treatment delays on survival in general population, possibly reflecting the increased importance of timely management in the current era of novel therapies, such as FOLFIRINOX in metastatic settings, as well as the use of adjuvant and neoadjuvant strategies.14,15
Given that jaundice can delay the initiation of cancer treatment, delays in accessing endoscopic drainage might, in turn, impact the time to treatment initiation and consequently affect patient prognosis. However, the factors influencing the time to endoscopic drainage remain poorly studied.
Among nonclinical determinants, socioeconomic and geographic deprivation significantly influence the management, morbidity, and mortality of many diseases.16,17 In pancreatic cancer, these factors have been shown to affect access to treatment and overall prognosis. 18 However, little is known about the potential impact of such determinants on access to endoscopic drainage for neoplastic disease. In this context, one U.S. study reported more limited access to endoscopic retrograde cholangiopancreatography (ERCP) in rural areas, a finding that has also been confirmed in the management of biliary stones by ERCP.19,20
The aim of this study is to assess the impact of both clinical and nonclinical determinants (including socioeconomic and geographic factors) on the time to ERCP drainage and 6-month mortality in patients with periampullary cancer diagnosed due to jaundice.
Methods
Study design and population
We conducted a retrospective multicenter study including all patients who benefited from an ERCP for periampullary cancer diagnosed due to jaundice between January 2010 and December 2020.
In the three principal centers in Lower-Normandy performing ERCP during this period (one university hospital and two private establishments), all patients who consecutively underwent an ERCP, whatever the indication for ERCP, were identified based on the codes of coding ICD-10 (International Classification of Diseases) system: HGQE002, HMQH003, HMQH005, HMPE001, HMGE002, HMNE001, HMJE001, HMLE002, HMLE003, HMQH007, HMKE001, HMKE002, HMGE001.
The patients included in the study were therefore patients over 18 years of age who underwent ERCP for periampullary cancer diagnosed due to jaundice. Patients with insufficient data to establish the indication for ERCP, as well as those who underwent percutaneous drainage prior to any endoscopic attempt, those drained for a cause other than tumor obstruction or for obstruction due to lymph node invasion from a cancer other than periampullary cancer were excluded.
Over the 10-year period in the three centers performing ERCP, a total of 5555 ERCP procedures were identified. We excluded 148 cases due to coding errors and cases were the indication for ERCP was not provided. Among these 5407 remaining procedures, 594 patients (11%) underwent drainage for obstruction due to an initial diagnosis of periampullary cancer. These 594 cases were included in the analysis (Figure 1).
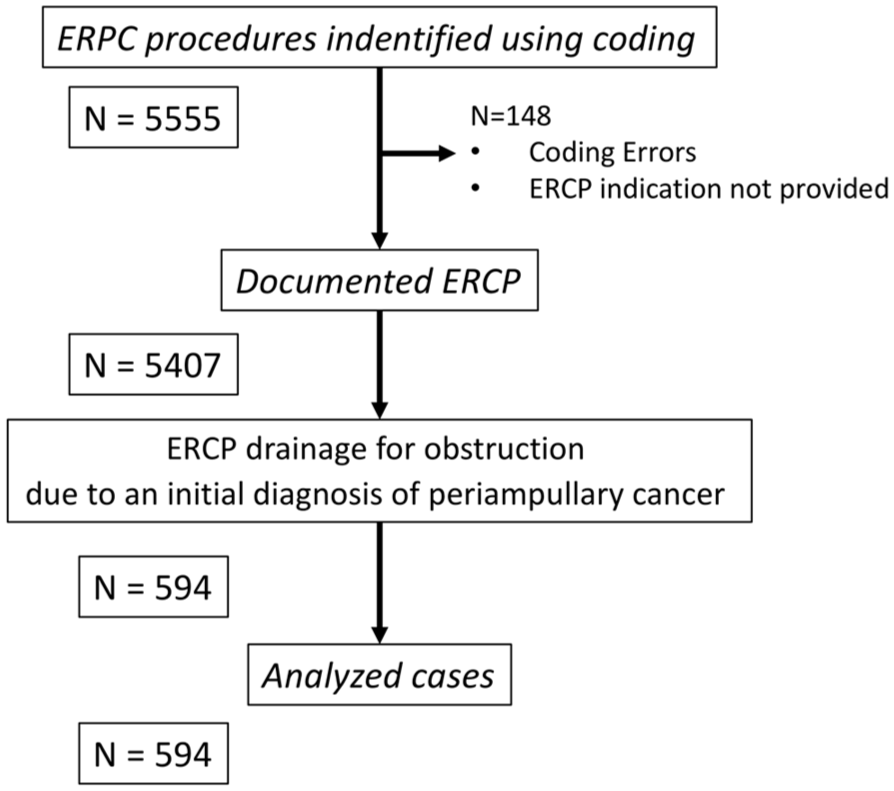
Study flowchart.
Data
Clinical data
We collected population clinical and demographic data at admission (body mass index, age, sex, treatment, initial symptoms), along with the clinical and biological parameters necessary to establish the diagnosis and to describe the case (date of diagnostic, date of ERCP drainage, biological data at admission and disease stage). The cases of acute cholangitis at diagnosis were retained when the clinical situation met the 2018 Tokyo diagnostic criteria. 21 The 1-year mortality, when not available in the clinical record, data could be exhaustively collected for all the patients in the study by consulting the “Institut National de la Statististique et des Etudes Economiques” (INSEE) registry data, which records all deaths in France. The date of last follow-up was March 20, 2025.
We assumed that the date of diagnosis was the same as the date of the imaging that allowed for the diagnosis of a periampullary tumor. The time to ERCP in our study was defined as the interval between the date of diagnosis and the date of the ERCP procedure.
Nonclinical determinants
The European Deprivation Index (EDI) was used to approximate material deprivation for each patient. This index is based on a European survey (European Union Statistics on Income and Living Conditions: EU-SILC) that provides information on living conditions in each country of the European Union.22,23 It is widely used in France and combines 10 different census variables: low level of education, lack of access to a car, living in overcrowded conditions, lack of access to central electric heating, non-homeownership, unemployment, foreign nationality, unskilled or farm worker, household with more than six persons, and single-parent household. The EDI was obtained from the address of each study patient using a geolocation platform and classified into five quintiles, ranging from the least deprived (quintile 1) to the most deprived (quintile 5). Quintiles were defined according to the national distribution of the EDI. Quintile 5 represents patients living in the 20% most deprived areas of France. However, by design, the EDI is a continuous variable. Therefore, we also performed univariate analysis with the EDI in its continuous form.
The spatial accessibility multiscalar index (SCALe) provides an overall score for accessibility to primary care in Metropolitan France, as previously described. 24 This index includes primary care clinicians and secondary specialists who can be accessed without an initial referral by a GP (gynecologist, ophthalmologist, or pediatrician). The health care professionals included in this index are as follows: GPs, physiotherapists, nurses, pharmacists, dentists, medical obstetricians and gynecologists, maternity wards, pediatric specialists, ophthalmologists, short-stay care services, and accident and emergency departments (Permanent Facilities Database of 2013, INSEE). Access to primary care combines the proximity and availability of facilities. The SCALe Index was computed for all residential areas to obtain a detailed representation of the French metropolitan territory. Therefore, this index is multiscalar and can be used at different geographical levels. The SCALe Index is a distance-based index, where a higher scale indicates lower accessibility.
Travel time was defined as the time required to travel between the patient’s home and the ERCP drainage center. A road-network database was used to determine the minimum travel time considering speed limits, direction . . . Travel speeds, computed in minutes, were estimated according to legal speeds for the different road classes.
Anonymized data were sent to the MapinMed geolocation platform to calculate the EDI, SCALe and travel time for each patient. To determine the EDI or the SCALe, the place of residence was geolocated using a Geographic Information System and assigned to an IRIS (Ilots Regroupés pour l’Information Statistique), a geographical unit defined by INSEE. IRIS represents the smallest geographical unit for which census data are available. Once these data were obtained, the result for each anonymized patient was integrated into the database.
Objectives and outcome
The main objective of the study was to determine the clinical and the nonclinical determinants associated with ERCP delay and 1-year mortality in patients with periampullary cancer diagnosed through jaundice.
The principal outcome was the time taken to perform the ERCP from the date of diagnosis and 1-year mortality after ERCP.
Statistical analysis
Distributions of factors in the two groups of patients drained within 3 days or after were compared using Student’s t-tests or nonparametric Wilcoxon tests for continuous variables and Chi-squared tests for categorical variables. All tests were two-tailed, and a p value of less than 0.05 was considered to be significant. The probability of early ERCP (within 3 days) was investigated using a logistic regression. First, the association of each variable was investigated using univariate analysis. Then variables that achieved the significance threshold of 0.1 were added to the final multivariate model. In the final model, the significance threshold was set at 0.05.
One-year overall survival was analyzed using Kaplan–Meier estimates and Cox proportional hazards modeling. Variables associated with mortality at p < 0.10 in univariate analysis were included in the multivariate Cox model using a stepwise selection procedure. The proportional hazards assumption was tested using graphical methods. Variables with more than 30% missing data were excluded from the multivariate analysis. A p-value <0.05 in the final multivariate model was considered statistically significant. Multivariate Cox analyses were stratified by study center. For both multivariate analyses, sensitivity analyses were performed using backward and forward variable selection procedures as well as fully adjusted model in addition to the stepwise approach. Statistical analysis was performed using SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA).
Statistical analysis
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 25
Results
Population
A total of 594 ERCP procedures were performed for biliary obstruction due to periampullary cancer diagnosed following the onset of jaundice across the three participating centers during the study period. The median time to biliary drainage was 9 days (interquartile range (IQR): 4–16). Two hundred ninety-four patients were initially managed at a biliary drainage center. The remaining 52.9% were referred from another institution. The characteristics of the overall study population are summarized in Table 1.
Characteristics of the overall study population.

ALAT, alanine aminotransferase; EDI, European Deprivation Index; ERCP, endoscopic retrograde cholangiography; GGT, gamma-glutamyl transferase; IQR, interquartile range; PAL, alkaline phosphatase; PT, prothombin time.
The median age of the treated population was 74 years, with no significant difference in the proportion of men and women. Jaundice was the first symptom reported by patients in the vast majority of cases (526/594; 88.6%), and associated abdominal pain was reported in 26% of cases (156/594). At the time of diagnosis, most tumors were nonmetastatic (432/594; 72.7%). The mean total bilirubin level at diagnosis was 244 ± 166 µmol/L. The proportion of patients receiving anticoagulant therapy was significantly higher among patients with a prothombin time (PT) <50% than among those with a PT ⩾50% (13.4% (9/67) vs 5.3% (28/528); p = 0.009). More than half of the patients belonged to the two most socioeconomically disadvantaged population quintiles. The distribution of EDI quintile did not differ significantly across centers (Supplemental Table 1). The median travel time to the drainage center was 35 min (IQR: 14–63). The technical success rate of ERCP was 83% (492/594).
One-year Survival and factors associated with survival depending on time to ERCP
The post-ERCP overall survival median was 7.5 months (Figure 2). At 1 year 65% of the population had died.

One-year overall survival of the global population.
Using univariate Cox regression analysis, the clinical variables associated with mortality were age, presence of metastatic disease, cholangitis, alanine aminotransferase, gamma-glutamyl transferase, leukocyte count, creatinine, and prothrombin time (Table 2). Patients with concomitant acute cholangitis had poorer 1-year overall survival (hazard ratio (HR) = 1.62; 95% confidence interval (CI) (1.15–2.29); p = 0.006; Figure 3). No territorial or social determinants, such as travel time, social deprivation, access to primary care, or the EDI, were associated with survival. The initial success of ERCP drainage was also associated with improved survival (HR = 0.53; 95% CI (0.39–0.72)).
Influence of clinical and nonclinical variables on 1-year mortality, Cox regression.

Variables not included in multivariate analysis due to proportion of missing data >30%. The variables in bold are included in the multivariate analysis.
ALAT, alanine aminotransferase; CI, confidence interval; EDI, European Deprivation Index; ERCP, endoscopic retrograde cholangiography; GGT, gamma-glutamyl transferase; HR, hazard ratio; PAL, alkaline phosphatase; PT, prothombin rate.

One-year overall survival depending on associated acute cholangitis.
In multivariate Cox analysis, only age (HR = 1.03; 95% CI (1.01–1.04)), metastatic disease (HR = 1.76; 95% CI (1.21–2.57)), acute cholangitis (HR = 1.51; 95% CI (1.03–2.22)) and ERCP technical success (HR = 0.59; 95% CI (0.42–0.83)) were independently associated with mortality (Table 2). No social or geographical determinants influenced the prognosis. The results of the multivariable analyses were similar regardless of the variable selection approach used (Supplemental Tables 2 and 3).
In the univariate Cox analysis, patients who underwent ERCP drainage within 3 days of diagnostic imaging had better survival outcomes (HR = 0.66; 95% CI (0.45–0.96); p = 0.03; Figure 4). However, after adjustment for covariates in the multivariate model, time to ERCP did not significantly influence survival.

One-year overall survival depending on the ERCP drainage timing.
Factors associated with timing of ERCP drainage
Among the 594 patients included in the study, “drainage timing” data were available for 456. The characteristics of this subgroup are described in Table 3 and are generally comparable to those of the overall study population. When comparing patients who underwent drainage within 3 days versus those who were drained later, those drained within 3 days more frequently presented with jaundice at the initial consultation (97.2% vs 87.5%, p = 0.004), had less pain (19.6% vs 31.3%, p = 0.02), were less often at the metastatic stage (90% vs 81, p = 0.003), had higher total bilirubin levels at diagnosis (283 µmol/L vs 201 µmol/L, p = 0.006) and a higher prothrombin time (90% vs 81%, p = 0.003; Table 3). None of the nonclinical determinants of health significantly influenced ERCP drainage time.
Comparison of population characteristics according on ERCP delay.

ALAT, alanine aminotransferase, EDI, European Deprivation Index; ERCP, endoscopic retrograde cholangiography; GGT, gamma-glutamyl transferase; IQR, interquartile range; PAL, alkaline phosphatase; PT, prothombin time.
In multivariate regression analysis, only total bilirubin ⩾200 µmol/L at diagnosis (odds ratio (OR) = 2.24; 95% CI (1.18–4.23)) and prothrombin rate (OR = 1.02; 95% CI (1.01–1.04)) were independently associated with undergoing ERCP within 3 days (Table 4). The results of the multivariable analyses were similar regardless of the variable selection approach used (Supplemental Tables 4 and 5).
Influence of clinical and nonclinical variables on ERCP within 3 days: univariate and multivariate logistic regression.

The variables in bold are included in the multivariate analysis.
ALAT, alanine aminotransferase; CI, confidence interval; EDI, European Deprivation Index; ERCP, endoscopic retrograde cholangiography; GGT, gamma-glutamyl transferase; OR, odds ratio; PAL, alkaline phosphatase; PT, prothombin time.
Discussion
In this series of 594 ERCP procedures performed for obstructive jaundice secondary to periampullary tumors, no social or geographical determinants were found to influence either the time to ERCP or the 1-year survival of patients. Survival was ultimately determined by classical clinical factors: age, tumor stage, technical success of endoscopic drainage, and the presence of concomitant acute cholangitis. As for the timing of ERCP, it appeared to be influenced solely by the severity of jaundice and coagulation status.
Our study population is generally comparable to data reported in the literature. The median age of 74 years is close to the average age of 72 years observed in the series by Balzano et al., which included all cases of pancreatic cancer presented at multidisciplinary tumor boards. 26 However, it appears higher than the median age reported in single-center hospital series where patient selection may occur.3,14 The distribution of resectable, locally advanced, and metastatic lesions also aligns with previously published data.14,27 The observed 1-year mortality rate of 65% is slightly higher than overall survival rates reported in general series, which range between 57% and 61%.12,26,28 This finding supports the poorer prognosis of patients diagnosed based on jaundice.3,5 Studies specifically analyzing this subgroup report mortality rates comparable to ours, with a median survival of approximately 7.5 months. 3
Beyond the classical prognostic factors commonly reported in the literature, such as age and tumor stage, our study demonstrates the prognostic impact of acute cholangitis in this patient population. While the neoplastic etiology is a well-documented adverse prognostic factor for acute cholangitis,29–31 few studies have investigated the converse question of how acute cholangitis affects cancer prognosis. A recent study by Singh et al., which collected cases of pancreatic neoplasia complicated by episodes of acute cholangitis during cancer follow-up, reported a poor prognosis in these patients. 32 The median survival after the first episode of acute cholangitis was only 4.1 months, with an overall 12-month survival rate of 18.9%. Studies have shown that acute cholangitis is associated with poorer outcomes in patients undergoing surgery for pancreatic cancer.33,34 To our knowledge, no study besides ours has demonstrated that acute cholangitis constitutes an independent adverse prognostic factor for tumors of the biliopancreatic junction in the general population, regardless of whether patients undergo surgery.
The technical success of ERCP was associated with survival in our series. While it might be assumed that initial failure to achieve biliary drainage may influence subsequent management of the neoplasm, this factor may also reflect the lesion’s size and extent, which sometimes causes duodenal obstruction preventing endoscopic access to the papilla. The advent of new endoscopic drainage techniques, such as lumen-apposing metal stents or endoscopic ultrasound-guided hepaticogastrostomy (which were not available in our region during the study period), is expected to reduce the impact of this factor in the coming years. 35
While the timing of ERCP appears to influence the prognosis of severe acute cholangitis cases,30,31 it was not an independent prognostic factor in our series of periampullary tumors. Instead, the time to the procedure was associated only with two clinical variables: coagulation status and the severity of jaundice. The impact of prothrombin time may simply reflect the use of anticoagulant therapy, which often necessitates delaying drainage. Severe jaundice may require earlier drainage to prevent related complications, such as acute cholangitis or renal failure due to cholemic nephropathy. 36 While the severity of jaundice may prompt earlier drainage, the timing of the procedure does not appear to influence disease prognosis. Paradoxically, jaundiced patients are often managed more promptly and tend to experience fewer treatment delays.14,26,27 The apparent benefit of early drainage observed in univariate analysis may, in fact, reflect a less complex clinical situation, which loses significance after adjusting for confounding factors in multivariate analysis. This difference may also be explained by the fact that younger patients in better general condition and/or with a more aggressive treatment strategy were prioritized for drainage, whereas older patients or those receiving palliative care underwent drainage later. This hypothesis could account for the survival difference observed when comparing drainage times alone and the loss of the benefit of shorter delays in multivariate analyses that adjust for other factors such as age, tumor stage, and related variables.
Social and geographical determinants did not appear to influence either the timing of management or the prognosis of patients in our study. Once the diagnosis is established—often prompted rapidly by the onset of jaundice—social deprivation does not seem to affect the subsequent course of care. It is possible that the protective nature of the French healthcare system mitigates the impact of social or geographical disparities on access to ERCP, as has been observed in other countries.19,20 However, since our study population was defined based on attempts at endoscopic drainage, it does not account for patients who may have never undergone ERCP—either due to poor overall clinical condition or rapidly progressive disease. These more vulnerable patients may also be more likely to come from socially or geographically disadvantaged backgrounds. In the future, with the anticipated increase in incidence and improved survival among patients receiving treatment, increased demand for ERCP may reveal disparities in access, potentially influenced by social determinants. Moreover, the emergence of novel therapeutic options such as endoscopic ultrasound-guided biliary drainage or Lumen-Apposing Metal Stent (LAMS) placement, which may have a greater prognostic impact, particularly in cases of double obstruction or surgically altered anatomy, could result in unequal availability depending on social or geographical context.37,38 It will be important to revisit this analysis in the coming years to assess the evolution of these potential disparities.
This study has several limitations. First, due to its retrospective design, missing data were inevitable. It was also impossible to retrospectively study the factors that influenced the decision to perform ERCP quickly or not. We chose to define the timing of ERCP as the interval between the imaging study that confirmed the diagnosis and the date of the ERCP procedure. While it would have been possible to use the onset of first symptoms or the date of first medical contact as a starting point, this information was too difficult to collect retrospectively in a reliable manner. This assumption may underestimate diagnostic delays. It remains possible that certain factors influence diagnostic delay, what might be termed a “diagnostic wandering,” which we were unable to capture due to the design of our study. Although our study was multicentric, it only assessed access to ERCP within a specific geographic region. It remains to be seen whether these findings are generalizable to other regions, and whether the density and distribution of drainage centers may influence access and timing. Although the indices used (EDI and SCALe) are robust and the spatial scale applied is as small as possible, this remains an ecological approach, and therefore ecological bias cannot be excluded. Finally, this study included only patients who underwent an attempted endoscopic drainage. Patients in a severely compromised condition for whom drainage was not pursued, those who died before the procedure, and those managed with alternative drainage techniques were not included. As previously discussed, these patients may be particularly affected by social deprivation. Their exclusion may therefore have influenced the robustness of our conclusions regarding the absence of an effect of social and geographical determinants.
In contrast, our study presents several notable strengths. It is a real world, multicenter investigation that includes patients managed across both public and private healthcare facilities. As such, it offers a more representative and pragmatic view of clinical practice compared to many hospital-based series originating from specialized referral centers. Unlike most existing studies on similar topics, our analysis integrates conventional clinical variables with socio-territorial health determinants. The observed impact—or lack thereof—of each documented factor appears to reflect actual clinical influence, as opposed to confounded effects often encountered when social determinants are closely correlated with clinical status. Importantly, to the best of our knowledge, this is the first study to assess the prognostic implications of drainage delay in neoplastic disease of the biliopancreatic junction initially revealed by jaundice. Despite being a common clinical scenario, 1 and with jaundice already established as an adverse prognostic factor in such malignancies, 3 no prior work has specifically investigated how the timing of biliary drainage affects patient outcomes or the factors contributing to this timing.
Conclusion
The timing of endoscopic biliary drainage does not appear to impact overall survival in patients with periampullary cancer diagnosed through jaundice. Prognosis in this patient population is primarily influenced by traditional clinical factors, with the occurrence of acute cholangitis emerging as an independent prognostic indicator. In contrast, social or geographical determinants of health do not seem to affect access to endoscopic drainage or influence clinical outcomes in this specific context.
Supplemental Material
sj-doc-1-tag-10.1177_17562848261426095 – Supplemental material for Impact of timing of access to endoscopic drainage and social determinants of health on the prognosis of patients with periampullary cancer diagnosed through jaundice: a multicenter retrospective study
Supplemental material, sj-doc-1-tag-10.1177_17562848261426095 for Impact of timing of access to endoscopic drainage and social determinants of health on the prognosis of patients with periampullary cancer diagnosed through jaundice: a multicenter retrospective study by Benoît Dupont, Olivier Dejardin, Wendy Kam, Ludivine Launay, Laurent Mosquet, Romain Gloro, Véronique Bouvier, Marie-Astrid Piquet and Arnaud Alves in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261426095 – Supplemental material for Impact of timing of access to endoscopic drainage and social determinants of health on the prognosis of patients with periampullary cancer diagnosed through jaundice: a multicenter retrospective study
Supplemental material, sj-docx-2-tag-10.1177_17562848261426095 for Impact of timing of access to endoscopic drainage and social determinants of health on the prognosis of patients with periampullary cancer diagnosed through jaundice: a multicenter retrospective study by Benoît Dupont, Olivier Dejardin, Wendy Kam, Ludivine Launay, Laurent Mosquet, Romain Gloro, Véronique Bouvier, Marie-Astrid Piquet and Arnaud Alves in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.