
Abstract
Background:
Endoscopic retrograde appendicitis therapy (ERAT) has emerged as a minimally invasive approach to treating appendicitis.
Objectives:
This study aimed to assess the long-term safety and efficacy of ERAT and to develop a model predicting 1‑year appendicitis recurrence in patients with acute appendicitis, to guide clinical decision-making.
Design:
This is a multicenter retrospective study. Consecutive patients were referred to the three participating centers.
Methods:
A retrospective analysis was conducted on clinical data from 435 patients with acute appendicitis who underwent ERAT at three hospitals between October 2017 and October 2024. Twenty-four clinical variables were screened, and Spearman correlation analysis revealed correlation coefficients exceeding 0.6 between some variables. To address multicollinearity, LASSO regression was employed to identify key predictive factors in the training set. A predictive model was constructed using multivariate logistic regression, and a nomogram was developed.
Results:
All ERAT procedures were technically successful, and a clinical success rate of 92.4% was achieved. The median follow-up period was 37 months, and the overall recurrence rate was 16.1%; most recurrences (13%) were observed in the first year. Based on LASSO regression analysis, the final predictors identified were: age >60 years (odds ratio (OR) = 2.981, 95% confidence interval (CI): 1.368–6.497, p = 0.006), recurrence appendicitis (OR = 4.048, 95% CI: 1.931–8.587, p < 0.001), Alvarado score >6 (OR = 5.649, 95% CI: 2.586–12.339, p < 0.001), fecalith (OR = 2.680, 95% CI: 1.146–6.267, p = 0.023), inexperienced operator (OR = 2.286, 95% CI: 1.141–4.580, p = 0.020), procedure time >40 min (OR = 2.472, 95% CI: 1.240–4.927, p = 0.010), appendix lumen distortion (OR = 7.634, 95% CI: 1.414–41.219, p = 0.018), and stent placement (OR = 5.970, 95% CI: 0.121–0.793, p = 0.015). Based on these eight predictive factors, a nomogram model was constructed to predict recurrence risk within 1 year after ERAT.
Conclusion:
ERAT is a safe and effective treatment for acute appendicitis. The risk of recurrence is highest within the first year. Eight independent risk factors for recurrence within 1 year after ERAT were identified, and a recurrence risk prediction model based on these predictive factors can assist in future clinical decision-making for ERAT.
Plain language summary
ERAT is a minimally invasive endoscopic treatment for appendicitis. Doctors reach the appendix opening through a colonoscope, drain pus, wash the lumen, remove “appendix stones” (appendicoliths), and place a small temporary stent if needed to keep the passage open.
We reviewed 435 people with acute appendicitis who had ERAT at three hospitals in China (2017–2024). We assessed long‑term safety and effectiveness and built a simple tool to estimate a patient’s risk of appendicitis coming back within 1 year.
Technical success was 100%; symptoms improved in 92.4% of patients. Median follow‑up was 37 months. Overall, 16.1% had recurrence; most recurrences (13%) happened in the first year. After recurrence: 64% had appendectomy, 29% were treated with antibiotics, and 7% had ERAT again (most then did well). Factors linked to a higher chance of recurrence included:
Age over 60
A previous episode of appendicitis
Higher Alvarado score (>6)
Presence of an appendicolith
Less‑experienced operator
Longer procedure time (>40 minutes)
Distorted (twisted) appendix lumen
Placing a stent was associated with a lower risk of recurrence, especially when the lumen was narrow or distorted. Using these factors, we created an easy‑to‑use risk chart (nomogram) that showed good prediction in internal testing.
ERAT is generally safe and effective. The first year after ERAT is the critical period for follow‑up. For patients who are older, have high Alvarado scores, an appendicolith, or difficult appendix anatomy, ERAT should be performed by experienced endoscopists with thorough stone removal, ample washing, and stent placement when indicated to reduce recurrence. The risk tool can support shared decision‑making when choosing between ERAT and surgery.
Keywords
Introduction
Acute appendicitis is a leading cause of hospitalization worldwide, and appendectomy is a widespread abdominal surgery. 1 Endoscopic retrograde appendicitis therapy (ERAT) is the leading treatment for appendicitis due to its effectiveness and minimally invasive approach.2–4 Recurrence is the main clinical concern for both ERAT and conservative antibiotic treatment across patient populations.
Previous studies reported that 24%–59% of acute appendicitis patients experience recurrences and require an appendectomy.5–7 Hence, understanding the predictors of post-ERAT recurrence will enhance clinical decision-making and outcomes. Several risk factors for appendicitis recurrence after conservative antibiotic therapy have been identified.8–10 Appendicolith is the most common predictor of recurrence and subsequent appendectomy.11,12 In addition, a high Appendicitis Activity Score, which incorporates white blood cell counts (WBCs) and C-reactive protein (CRP) into a risk stratification score, is a predictor of clinical failure in patients treated with antibiotic therapy.13,14 ERAT mitigates the probability of recurrence by eliminating appendicoliths. Studies reporting recurrence rates and risk factors after ERAT are limited, and many studies involve small sample sizes and short follow-ups with no definitive conclusions. Therefore, we conducted a retrospective multicenter analysis of clinical data from three Chinese hospitals to assess the long-term safety and efficacy of ERAT and to develop a model predicting 1‑year appendicitis recurrence in patients with acute appendicitis, to guide clinical decision-making. The results of this study can be applied to improve decision-making and create personalized treatment strategies for appendicitis.
Methods
Patients enrollment
This multicenter retrospective study included all consecutive patients who underwent ERAT for acute appendicitis from October 2017 to October 2024 at the First Affiliated Hospital of Zhengzhou University, Shijiazhuang Western Medical Center, and Tai’an Central Hospital. This study was approved by the Institutional Review Board of the First Affiliated Hospital of Zhengzhou University (approval number: 2024-KY-2356) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. Informed consent was obtained from all patients; for minors or those unable to provide consent, consent was obtained from their legal representatives. The inclusion criteria for patients were as follows: (1) a confirmed diagnosis of acute appendicitis; (2) no prior history of ERAT; (3) all enrolled patients underwent ERAT and agreed to postoperative follow-up by telephone or outpatient visit; (4) complete clinical data. The exclusion criteria were as follows: (1) inability to tolerate colonoscopic treatment; (2) presence of other diseases that severely affect quality of life; (3) exclusion of appendicitis after ERAT; (4) failure to complete follow-up (Figure 1). All patient data were anonymized. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Table 1).

Study enrollment flowchart.
Data collection
Clinical data were collected, including basic clinical information (gender, age); disease characteristics (recurrent appendicitis, periappendiceal abscess, Alvarado score, migration of pain, visual analog scale (VAS) score, anorexia, nausea or vomiting, right lower quadrant (RLQ) tenderness, rebound tenderness, fever, appendicolith); preoperative laboratory results (leukocytosis, neutrophils, CRP); intraoperative treatment parameters (operator experience, procedure time, use of transparent cap, appendix lumen stenosis, appendix lumen dilation, appendix lumen distortion, use of cholangioscope, stent placement); and postoperative complications (time to appendicitis recurrence, readmission treatment methods, and prognosis). All data were obtained from clinical records, with no missing values, so imputation was not required.
ERAT procedure
Before the ERAT, patients underwent a bowel preparation protocol similar to the preparation for colonoscopies. ERATs were performed as previously described.2,3 The colonoscope was advanced into the cecum. Appendiceal intubation was achieved under X-ray guidance using a guidewire. Diluted water-soluble contrast was instilled to image the appendiceal morphology. The intraluminal pressure was relieved by aspiration of the purulent fluid and debris, and the lumen was flushed with saline. Appendicoliths were removed with a retrieval basket or balloon. A 5–7 cm plastic stent was placed over the guidewire in patients with signs of suppurative appendicitis, stenosis of the appendiceal lumen, or suspected appendicolith residue (Figure 2).

ERAT procedure. (a) The colonoscope was advanced into the cecum. (b) Appendiceal intubation. (c) Appendiceal morphology. (d) The intraluminal pressure relieved by irrigation. (e) Appendicolith removed. (f) Re-appendiceal morphology. (g, h) Stent placement.
Postoperative management and follow-up
Postoperative management was based on the presence of lingering symptoms and physical examinations. No postoperative fasting was recommended after ERAT without anesthesia in patients with no perforations. A 3-h fast was recommended in patients who underwent ERAT under anesthesia. Patients experiencing fever and elevated WBCs received intravenous antibiotics for 2–3 days, followed by oral antibiotics for 4 days. If symptoms persisted after 48–72 h, a surgical consultation was deemed necessary. Patients were discharged when they exhibited no symptoms following oral consumption. Follow-up was conducted through outpatient visits or phone calls at 1, 3, and 6 months after ERAT, followed by yearly examinations. Symptoms, appendicitis recurrence, and additional medical interventions were evaluated during follow-up visits.
Definition and outcomes
A periappendiceal abscess was defined as a collection of fluid with an enhanced rim or pus visible on preoperative CT or ultrasound imaging. Pain was assessed at 6 h after ERAT, using the VAS (0–10): 1–3 for mild pain (tolerable pain), 4–6 for moderate pain (pain affecting sleep but tolerable), and 7–10 for severe pain (intense pain interfering with physiological function). Fever was defined as an axillary temperature ⩾37.2°C. Laboratory changes included WBCs >9.5 × 109/L, neutrophil percentage >75%, and CRP >5 mg/L.
Inexperienced operators were defined as operators who independently accomplished fewer than 30 ERAT procedures and had no experience in endoscopic retrograde cholangiopancreatography (ERCP). The procedure duration was defined as the appendiceal intubation to ERAT completion, including stent placement. Technical success was defined as successful appendiceal intubation, appendicolith extraction, pus drainage, and stent placement if needed. Clinical success was defined as the alleviation of symptoms, with no signs of recurrence within 1 month after ERAT. Recurrence was defined as complete remission of symptoms and signs within 1 month after ERAT, followed by imaging-confirmed appendicitis during follow-up. The time of recurrence is calculated from the completion of the ERAT procedure.
Model development
To mitigate multicollinearity effects, LASSO regression was employed, with the optimal regularization parameter λ determined through 10-fold cross-validation, thereby identifying variables with predictive significance. These variables were subsequently incorporated into a multivariate logistic regression model, with a statistical significance threshold set at p < 0.05, to ultimately identify independent risk factors influencing appendicitis recurrence within 1 year after ERAT. A predictive model for recurrence risk was constructed based on variables selected through LASSO regression and visualized intuitively via a nomogram.
Statistical analysis
The Shapiro–Wilk test was employed to assess normal distribution. Measurement data that did not conform to normal distribution were described using M (P25, P75), and count data were expressed as frequencies and percentages. Linear correlation was examined through Spearman correlation analysis. LASSO regression and multivariate logistic regression were applied to identify influencing factors for 1-year appendicitis recurrence after ERAT. The significance level was set at α = 0.05 (two-tailed). Data analysis was performed using SPSS 29.0 (IBM Corp., Armonk, NY, USA) and R 4.2.3 (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline data
A total of 535 patients were initially enrolled, and 435 were finally included in the analysis. The detailed process is shown in Figure 1. The patient demographic data and clinical details are presented in Table 1. The study included 435 appendicitis patients who underwent ERAT; 237 (54.4%) participants were males, and 198 (45.6%) were females. The median age of the participants was 34 years (interquartile range (IQR): 16–53), and the participants were stratified into age groups as follows: children (1–17 years, n = 133, 30.6%), adults (18–60 years, n = 235, 54.0%), and older adults (>60 years, n = 67, 15.4%).
Clinical features and laboratory results of patients who underwent ERAT.
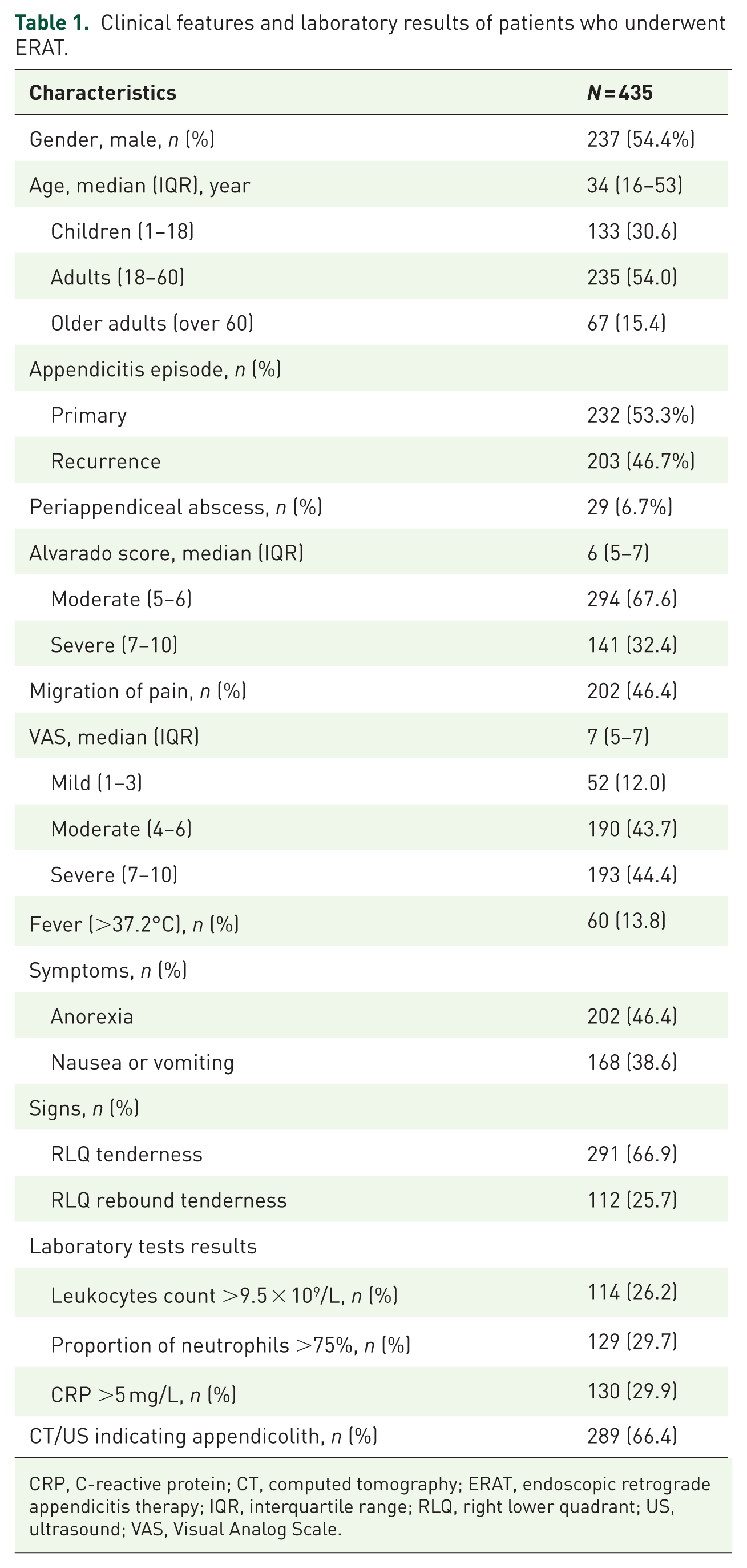
CRP, C-reactive protein; CT, computed tomography; ERAT, endoscopic retrograde appendicitis therapy; IQR, interquartile range; RLQ, right lower quadrant; US, ultrasound; VAS, Visual Analog Scale.
The diagnosis of appendicitis was the first for 232 patients (53.3%), and 203 patients (46.7%) experienced a previous diagnosis of appendicitis that was conservatively managed. Periappendiceal abscesses were preoperatively detected in 29 patients (6.7%). The median Alvarado score was 6 (IQR: 5–7); 294 patients (67.6%) had moderate scores (5–6), and 141 patients (32.4%) had high scores (7–10). Migratory abdominal pain was observed in 202 patients (46.4%), with a median VAS score of 7 (IQR: 5–7); the abdominal pain was categorized as mild (1–3) in 52 patients (12.0%), moderate (4–6) in 190 patients (43.7%), and severe (7–10) in 193 patients (44.4%). Sixty patients (13.8%) presented with preoperative fever.
Physical examination revealed RLQ tenderness in 291 patients (66.9%) and rebound tenderness in 112 patients (25.7%). Laboratory results showed elevated WBCs in 114 patients (26.2%), neutrophil percentage >75% in 129 patients (29.7%), and CRP >5 mg/L in 130 (29.9%) patients. Appendicoliths were identified in 289 patients (66.4%) during preoperative imaging or surgery.
Procedure-related data
ERATs were successful in all 435 patients. The technical success rate was 100%, and the clinical success rate was 92.4%. Experienced operators performed 230 of the procedures (52.9%). Transparent caps were used in 417 cases (95.9%), tapered caps were used in 344 cases (79.1%), and standard caps were used in 73 cases (16.8%). Intraoperative findings included appendiceal luminal stenosis in 75 patients (17.2%), dilation in 126 patients (29.0%), and tortuosity in 8 patients (1.8%). Cholangioscopes (eyeMax; Micro-Tech (Nanjing) Co., Ltd, Nanjing, China) were used in 36 patients (8.3%), and stents were placed in 97 patients (22.3%). The median procedure time was 26 min (IQR: 19–40); the procedure was completed in 1–19 min in 92 patients (21.1%), 19–40 min in 246 patients (56.6%), and >40 min in 97 patients (22.3%). Stents were placed in 97 patients (22.3%). The median hospital stay was 1 day (IQR: 1–2).
The median 6-h postoperative VAS score was 2 (IQR: 2–3); 424 patients (97.5%) experienced mild pain (1–3), 9 patients (2.0%) experienced moderate pain (4–6), and 2 patients (0.5%) experienced severe pain (7–10). The median total procedural cost was 6934 RMB (IQR: 3465–10,733; approximately 950 USD). The median follow-up period was 37 months, and the overall recurrence rate was 16.1% (70/435). The median time to recurrence was 5 months (IQR: 1–13). The cumulative rates of appendicitis recurrence at 1, 3, 5, and 7 years were 13%, 15%, 18%, and 20%, respectively (Figure 3). In cases of recurrent appendicitis, appendectomies were performed in 45 patients (45/70, 64.3%), 20 patients (20/70, 28.6%) were treated with conservative antibiotic treatment, and ERATs were repeated in 5 patients (5/70, 7.1%). Among the five patients had repeated ERAT, only one developed recurrent appendicitis 2 months later and underwent appendectomy, while no abnormalities were observed in the remaining four cases. Additional procedural details are shown in Table 2.

The cumulative rates of appendicitis recurrence.
Endoscopic treatment details and outcomes of patients who underwent ERAT for appendicitis.

ERAT, endoscopic retrograde appendicitis therapy; IQR, interquartile range.
Independent variable correlation
The dataset constructed from patient clinical data included a total of 24 variables. Spearman correlation analysis revealed strong correlations between Alvarado score and Leukocytes count >9.5 × 109/L, Leukocytes count >9.5 × 109/L and Proportion of neutrophils >75%, tapered transparent cap, and standard transparent cap (Figure 4). The correlation coefficients (r values) were 0.73, 0.77, and −0.80, respectively, all with p < 0.001. Due to multicollinearity (|r| ⩾ 0.7) among these variable pairs, redundant variables were either merged or excluded prior to subsequent LASSO regression modeling to ensure model stability.

Spearman correlation analysis.
Screening of risk prediction factors and model construction using LASSO regression model
From a dataset of 435 cases, 10 candidate variables were selected using LASSO regression: age >60 years, recurrence of appendicitis, Alvarado score >6, rebound tenderness, fecalith, inexperienced operator, procedure time >40 min, appendix lumen dilation, appendix lumen distortion, and stent placement (Figure 5). These 10 variables were simultaneously included in a multivariate logistic regression model. The results showed that age >60 years, recurrence of appendicitis, Alvarado score >6, fecalith, inexperienced operator, procedure time >40 min, appendix lumen distortion, and stent placement were identified as independent risk factors for appendicitis recurrence within 1 year after ERAT. Based on these eight independent predictive factors, a risk nomogram for recurrence prediction was constructed (Table 3 and Figure 6). Considering that stent placement may be influenced by endoscopists’ preferences, the analysis conducted after removing this variable also identified the correct predictive factors (Supplemental Figure 1).

Lasso regression feature selection. (a) Coefficient profiles of variables under different values of log(λ). (b) Ten-fold cross-validation for selection of the optimal λ.
Analysis of risk factors for appendicitis recurrence after ERAT.

CI, confidence interval; ERAT, endoscopic retrograde appendicitis therapy; OR, odds ratio.

Risk nomogram for recurrence prediction.
Validation of the nomogram model
Internal validation was performed using bootstrapping with 500 samples to evaluate the robustness of the prediction model. The results showed a Harrell’s C-index of 0.812, indicating good internal validation. The constructed calibration curve, apparent line, and bias-corrected line deviated only slightly from the ideal line, demonstrating excellent agreement between the predicted and observed values (Figure 7(a)). The DCA curve confirmed that the nomogram provided a significant net clinical benefit in practical applications (Figure 7(b)).
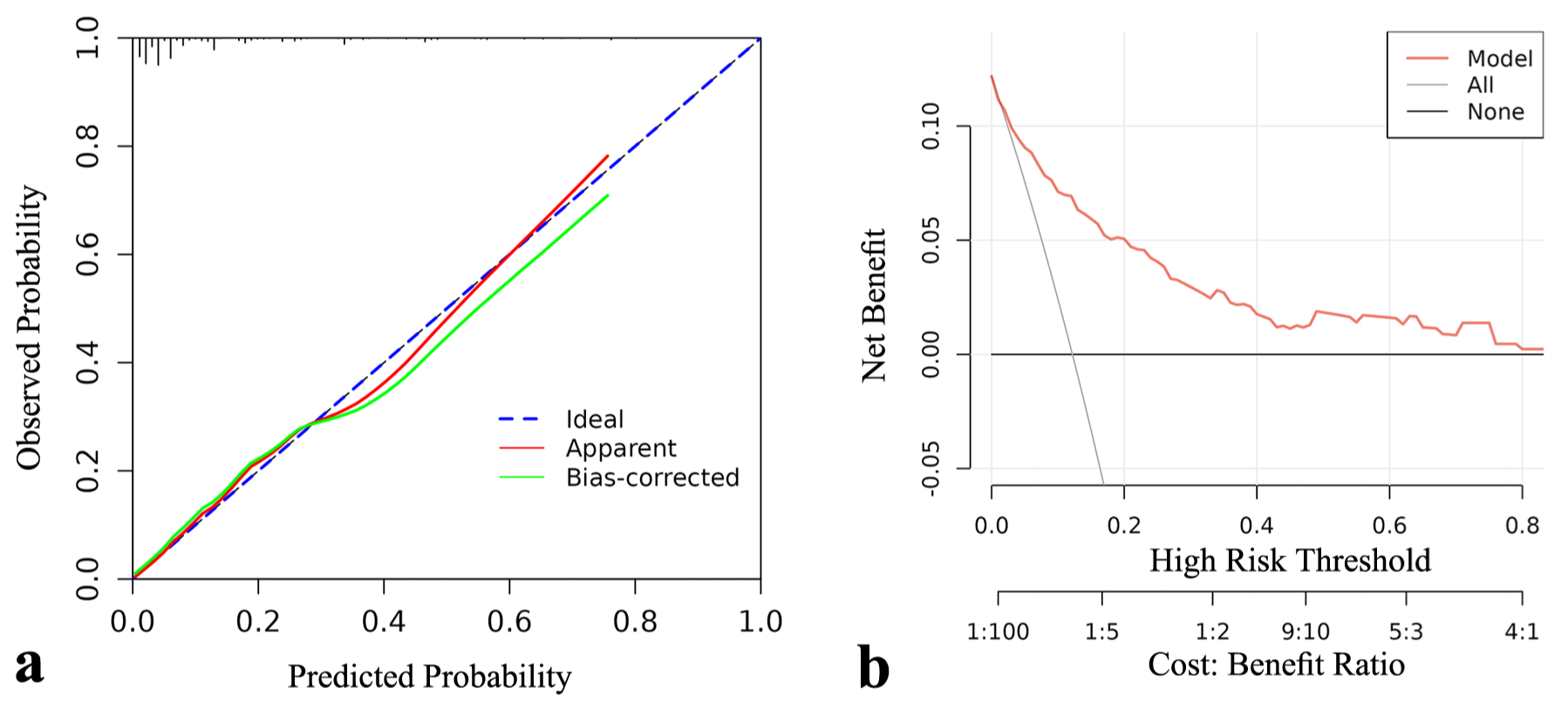
(a) The constructed calibration curve. (b) The DCA curve.
Discussion
Among the clinical treatment options for appendicitis, ERAT stands out as a safe, effective, and organ-preserving alternative.15,16 We previously showed that ERAT was as clinically effective as antibiotic treatment or laparoscopic appendectomy.17–19 However, recurrent appendicitis poses a significant challenge after ERAT. In contrast, appendectomy renders an all-encompassing cure for appendicitis that completely removes the potential for recurrence. In this multicenter study, the long-term clinical outcomes of ERAT were evaluated, focusing on recurrence rates over a mean follow-up period of 37 months. Given the varied outcomes following ERAT in patients with appendicitis, the key risk factors for recurrence were identified.
Our results showed that the cumulative recurrence rates at 1, 3, and 5 years were 13% (95% confidence interval (CI): 10%–16%), 15% (95% CI: 12%–18%), and 18% (95% CI: 14%–23%), respectively. Most recurrences were within the first year after ERAT. This trend aligns with earlier studies focused on recurrence rates after antibiotic treatment for acute appendicitis, suggesting that the high-risk phase for recurrence was within the first year. 6 This observation emphasizes the importance of thorough follow-up during the first year after ERAT to facilitate prompt management of recurrences. Moreover, the precise moment of recurrence could influence subsequent therapy choices for patients. In patients who experienced recurrences within the first year after ERAT, 76.2% of patients (32/42) underwent appendectomies, reflecting the urgency of their situation. Conversely, patients who experienced recurrences after 1 year chose more conservative approaches; 42.9% of patients selected antibiotic treatment, and 14.3% of patients opted for another ERAT. These results highlight the myriad of responses and treatment trajectories individuals pursue based on their unique circumstances. This proclivity may correlate with patient optimism regarding therapeutic approaches and dependence on long-term therapeutic outcomes.
Appendicolith-associated appendicitis is a high-risk factor for the recurrence of acute appendicitis. Previous studies demonstrated that the recurrence rate after appendicolith-associated appendicitis is higher than the recurrence rate after appendicitis without appendicoliths, possibly due to mechanical blockage and recurring inflammation in the interior of the appendiceal cavity. The current study corroborated these findings; the recurrence rate for patients with appendicolith-associated appendicitis was higher than the recurrence rate for patients without appendicoliths (17.3% vs 13.7%). ERAT was beneficial for treating cases of appendicolith-associated appendicitis. ERAT facilitates the direct extraction of appendicoliths from the appendiceal cavity, lowering the probability of recurrence. For cases with appendicolith residue after the procedure, an appendiceal stent can be placed to maintain lumen patency and decrease the likelihood of recurrence.
The current study focused on the influence of preoperative clinical factors (including appendicolith-associated appendicitis), intraoperative factors, and operator experience on recurrence. Multivariate analysis revealed that age >60 years (odds ratio (OR) = 2.981), recurrence appendicitis (OR = 4.048), Alvarado score >6 (OR = 5.649), fecalith (OR = 2.680), inexperience operator (OR = 2.286), procedure time >40 mins (OR = 2.472), and appendix lumen distortion (OR = 7.634) were significant risk factors for recurrence, while stent placement (OR = 0.196) can reduce the risk of recurrence. These findings are consistent with previous studies. For example, Zhan et al. 20 showed that patients without stent implantation had higher recurrence rates, although their analysis excluded patients with recurrent appendicitis and did not consider the effects of operator experiences on clinical outcomes. Our study also revealed that efficient appendicolith removal, lumen irrigation, and stent implantation by trained ERAT operators dramatically minimized the likelihood of recurrence, particularly in cases involving narrowing or skewing of the appendiceal lumen. For example, six of the eight patients with appendiceal lumen distortion experienced recurrence (75%). None of these patients received stents, indicating that stent intervention may be necessary in anatomically complex cases. However, due to the limited sample size and potential selection bias, this conclusion requires further validation through prospective studies.
Another noteworthy finding of this study was the influence of endoscopist expertise on the long-term prognosis after ERAT. Patients treated by experienced physicians had significantly lower recurrence rates than those treated by less experienced operators (OR = 2.286). This finding provides further evidence that ERAT efficiency is proportional to the technical competence and experience of the operator. Experienced operators are more likely to place appendiceal stents, completely remove appendicoliths, and thoroughly irrigate the appendiceal lumen, resulting in reduced recurrence risk.
The technical difficulty of ERAT is relatively high in cases of appendicolith-associated appendicitis or atypical morphologies such as appendiceal lumen narrowing or distortion, necessitating enhanced professional proficiency. ERAT is an evolution of ERCP and closely mirrors many of the procedural steps and technical requirements inherent to ERCP. Experienced operators performing ERCP demonstrate higher procedural success rates and lower recurrence rates after ERAT, reflecting their proficiency and skill in effectively managing complex cases.
Limitations
This study has several limitations. First, due to the retrospective design, the features included may not be comprehensive, such as detailed results of preoperative imaging examinations. Second, the data and information in this study were collected from three hospitals in three different provinces in China, ultimately including 435 patients with acute appendicitis who underwent ERAT. The sample size was relatively small and originated from a single population, without considering factors such as other ethnicities, which limits the generalizability of the results. Furthermore, as ERAT is a relatively new technique in this field, only 15.8% of patients in this study had a follow-up period exceeding 5 years, which may affect the long-term accuracy of the recurrence risk model. Future studies with longer follow-up periods and a broader population are needed to comprehensively assess its efficacy.
Conclusion
In recent years, ERAT, as a new minimally invasive treatment technique, has developed continuously and demonstrated considerable clinical efficacy in managing appendicitis. In this multicenter observational cohort study, we found that most ERAT recurrences occurred within the first postoperative year, underscoring the necessity of close follow-up during this period. Meanwhile, we identified the major risk factors for postoperative recurrence after ERAT, including advanced age, high Alvarado score, recurrent appendicitis, fecalith, prolonged operative time, appendiceal lumen distortion, insufficient operator experience, and stent placement conditions. Improvement targeting these factors may enhance patient outcomes. These findings provide a basis for further hypotheses, which need to be verified in prospective studies employing standardized techniques, extended follow-up periods, and larger study populations to optimize patient selection and treatment strategies.
Supplemental Material
sj-docx-2-tag-10.1177_17562848251410867 – Supplemental material for Risk factors for appendicitis recurrence after ERAT in patients with acute appendicitis: a multicenter cohort study with long-term follow-up
Supplemental material, sj-docx-2-tag-10.1177_17562848251410867 for Risk factors for appendicitis recurrence after ERAT in patients with acute appendicitis: a multicenter cohort study with long-term follow-up by Jiyu Zhang, Haipeng Yuan, Jianping Fan, Miao Shi, Mohammad Serajul Islam, Ning Su, Haiyang Li, Rongjuan Zhu, Shihe Hu, Jianfei Feng, Bingrong Liu and Dan Liu in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-1-tag-10.1177_17562848251410867 – Supplemental material for Risk factors for appendicitis recurrence after ERAT in patients with acute appendicitis: a multicenter cohort study with long-term follow-up
Supplemental material, sj-tif-1-tag-10.1177_17562848251410867 for Risk factors for appendicitis recurrence after ERAT in patients with acute appendicitis: a multicenter cohort study with long-term follow-up by Jiyu Zhang, Haipeng Yuan, Jianping Fan, Miao Shi, Mohammad Serajul Islam, Ning Su, Haiyang Li, Rongjuan Zhu, Shihe Hu, Jianfei Feng, Bingrong Liu and Dan Liu in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.