
Abstract
Background:
The feasibility of performing complete endoscopic retrograde cholangiopancreatography (ERCP) for acute cholangitis during weekends or holidays remains controversial due to concerns over increased risks of adverse events (AEs) in off-hour procedures.
Objectives:
To evaluate whether weekend drainage-only ERCP affects the incidence of AEs compared to standard weekday ERCP, and to identify risk factors for post-ERCP pancreatitis (PEP).
Design:
Prospective observational study.
Methods:
Patients with acute cholangitis, diagnosed based on the Tokyo Guidelines 2018 and naïve major papillae, were prospectively enrolled between 2018 and 2023. Patients were categorized into two groups: the “Weekend ERCP” group, in which initial biliary drainage was performed on weekends with subsequent therapeutic ERCP on weekdays, and the “Weekday ERCP” group, in which all procedures were completed during weekdays. The primary outcome was the incidence of PEP; secondary outcomes included overall AEs and risk factor analysis.
Results:
A total of 1772 patients were included (Weekend group: n = 148; Weekday group: n = 1624) in this study. The incidence of PEP was 4.1% in the Weekend group and 4.9% in the Weekday group (p = 0.810). Overall AEs occurred in 3.4% and 4.9% of patients, respectively (p = 0.540). Multivariable analysis identified age ⩽60 years, female sex, history of acute pancreatitis, difficult cannulation, and endoscopic papillary balloon dilation as independent risk factors for PEP. Timing of ERCP (weekend vs weekday) was not associated with increased risk of PEP.
Conclusion:
Weekend ERCPs limited to drainage-only strategies are as safe as weekday procedures in terms of AE rates, effectively managing resources and providing timely biliary decompression for acute cholangitis emergencies, although they often require subsequent definitive interventions.
Trial registration:
The International Clinical Trials Registry Platform (identifier KCT0005950; https://cris.nih.go.kr).
Plain language summary
Endoscopic retrograde cholangiopancreatography (ERCP) is an important procedure used to treat patients with acute cholangitis, a serious infection of the bile ducts. There has been debate about whether full ERCP treatment should be done during weekends or delayed until weekdays due to concerns about safety and complications such as pancreatitis. This study followed 1,772 patients with acute cholangitis to compare two approaches: One group received a "drainage-only" ERCP on weekends, followed by additional treatment on a weekday. The other group received complete ERCP on a weekday. The study found that the risk of complications, especially post-ERCP pancreatitis (PEP), was not higher in the weekend drainage-only group. In fact, the rates of PEP and overall adverse events were slightly lower on weekends, but the differences were not statistically significant. Other factors, such as being younger than 60, female, having a history of pancreatitis, or having a difficult cannulation, were more strongly linked to complications than whether the procedure was done on a weekday or weekend. These results suggest that performing drainage-only ERCP during weekends is a safe and effective strategy. It allows hospitals to provide timely care even with limited weekend staffing, without increasing the risk to patients.

Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a complex, high-risk procedure requiring advanced expertise and specialized equipment. 1 It requires a skilled endoscopist, nursing staff, technicians, and radiology technologists to operate fluoroscopy equipment. Due to its extensive human and technological demands, ERCP requires substantial time, effort, and financial resources. 2 ERCPs are typically performed during regular weekday hours when clinical support and resources are readily available.
However, some cases necessitate ERCP as an emergency procedure during off-hours, including weekends and holidays. Research3–5 suggests that off-hours ERCPs are as safe and effective as weekday procedures despite reduced clinical and administrative support. Even in non-emergent cases, weekend ERCPs can reduce the length of hospital stay (LOS) by facilitating earlier discharges. Reducing LOS enhances healthcare efficiency and minimizes hospital-related adverse events.6,7 Performing complete ERCP procedures, such as stone removal, for acute cholangitis during weekends is debated due to conflicting evidence. Studies show that endoscopic sphincterotomy (EST), in these cases, increases bleeding risks, compounded by acute cholangitis, which heightens the likelihood of post-EST bleeding. 8
In our institution, weekend ERCPs are reserved for on-call cases of acute cholangitis, typically presenting with high fever or severe abdominal pain. However, per hospital policy, weekend ERCPs are limited to drainage-only procedures, such as stent placement, with therapeutic ERCP deferred to weekdays. The safety of this weekend drainage-only strategy remains uncertain due to limited evidence, particularly concerning adverse events (AEs), including post-ERCP bleeding, exacerbation of cholangitis, and pancreatitis. We hypothesize that weekend ERCP procedures limited to drainage strategies do not increase the incidence of adverse events compared to weekday procedures. In this study, we aimed to assess whether weekend drainage-only ERCP increases AEs, including pancreatitis, compared to weekday procedures, using data from a large prospective cohort.
Methodology
Study population and design
We enrolled patients with naïve major papillae who underwent diagnostic or therapeutic ERCP at two referral hospitals (Chonnam National University Hospital and Hallym University Dongtan Sacred Heart Hospital) in South Korea between June 2018 and June 2023. Patients with acute cholangitis, defined by the Tokyo Guidelines 2018 (TG 18) 9 criteria, were included. A suspected diagnosis requires systemic inflammation (e.g., fever or elevated inflammatory markers), signs of cholestasis (e.g., jaundice or abnormal liver tests), or imaging findings such as biliary dilatation or an identifiable cause. By contrast, a definite diagnosis requires all three. Exclusion criteria were (1) prior chronic pancreatitis diagnosis; (2) acute pancreatitis within 2 weeks of ERCP or ongoing acute pancreatitis; (3) surgically altered anatomy impeding access to the major papilla; and (4) non-adherence to research protocols.
Patients were divided into two groups based on ERCP timing: the “Weekend ERCP” group, limited to initial drainage procedures over the weekend or holidays, with therapeutic ERCP performed later on weekdays, and the “Weekday ERCP” group, where all procedures were completed on weekdays. Patient demographics, endoscopy-related findings, and clinical outcomes, including post-ERCP pancreatitis (PEP) incidence, were prospectively collected. In this study, the term “drainage-only strategy” referred to ERCP procedures conducted during weekends that were primarily intended for biliary decompression, most commonly via plastic stent placement. Although complex therapeutic procedures such as extensive stone extraction or complete clearance were intentionally deferred to weekday sessions, minor adjunctive interventions—such as limited balloon sweeping of small, non-impacted stones near the ampulla—were occasionally performed at the discretion of the endoscopist. To minimize procedural complexity during weekend ERCPs, endoscopic sphincterotomy was not routinely performed and was reserved only for cases in which it was strictly necessary to achieve effective biliary drainage. Nasobiliary drainage was not utilized in our institutions.
We will submit the results of the study to relevant national and international journals with the intention of publishing the results widely. We will also make national and international presentations to stakeholder groups, including those involving patients, researchers, clinicians, managers, and policymakers. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement guidelines for observational cohort studies (Supplemental Material). 10
Study endpoints and definitions of outcomes
The primary objective of this study was to evaluate the incidence of PEP in patients undergoing ERCP for acute cholangitis on weekdays versus weekends. Secondary endpoints involved identifying risk factors for PEP, assessing the impact of timing (weekends vs weekdays) on AEs, and evaluating clinical outcomes based on the intervention timeframe (within or beyond 24 h).
Difficult cannulation was defined as requiring more than five contacts with the papilla, exceeding 5 min for cannulation after papilla visualization, or multiple unintended pancreatic duct (PD) cannulations or opacifications. 11 Total procedure time was measured from duodenoscope insertion to removal, while selective cannulation time was measured from papilla positioning to successful deep cannulation. AEs, including pancreatitis, bleeding, perforation, post-ERCP cholecystitis, and sedation-related events, were graded using established consensus guidelines.12,13
PEP was diagnosed in patients with new or worsening abdominal pain suggestive of acute pancreatitis, fulfilling at least one of the following criteria: serum lipase or amylase levels exceeding three times the upper normal limit or characteristic features of acute pancreatitis on contrast-enhanced computed tomography (CT) approximately 24 h post-ERCP. PEP severity was classified based on hospitalization duration: mild (2–3 days), moderate (4–10 days), and severe (more than 10 days), with complications such as hemorrhagic pancreatitis, pancreatic necrosis, pseudocysts, or requiring interventions like percutaneous drainage or surgery. 14 Hyperamylasemia was defined as serum amylase levels exceeding 100 IU/L, measured pre-ERCP and 24 h post-procedure.
Endoscopic procedures for ERCP
All ERCP procedures followed standardized protocol and were performed by expert endoscopists with over 10 years of experience (E.C., K.J.L., and S.W.P.). Cannulation was performed using a conventional catheter or a pull-type sphincterotome with a wire-guided technique. Contrast media were administered only after successful selective cannulation. Difficult cannulation cases could be managed with rescue infundibulotomy. Primary infundibulotomy was performed for impacted stones at the major papilla or anatomically prominent papillae. Endoscopic papillary balloon dilation (EPBD) was used for large bile duct stones or coagulopathy to minimize the risk of hemorrhage. Pancreatic stents were placed in cases of PD cannulation, endoscopic papillectomy, or pancreatic sphincterotomy. Rectal nonsteroidal anti-inflammatory drugs (NSAIDs) were not utilized for PEP prophylaxis due to their unavailability in South Korea.
Statistical analyses
Continuous variables were presented as means with standard deviations, and categorical variables as frequencies and proportions. Continuous variables were compared using the Student’s t-test and categorical variables with the chi-square (χ2) test. Univariate and multivariate logistic regression analyses identified risk factors for PEP and AEs, with variables showing p < 0.2 in the univariate analysis included in the multivariate analysis. Statistical significance was set at p < 0.05. Analyses were performed using the R software (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
A total of 2800 patients with naïve major papillae who underwent diagnostic or therapeutic ERCP were enrolled in the study (Figure 1). After evaluating acute cholangitis using the TG 18 diagnostic criteria, 636 patients who did not meet the criteria were excluded. An additional 392 patients were excluded due to acute pancreatitis within 2 weeks before ERCP (n = 236), a history of chronic pancreatitis (n = 117), or failure to access the major papilla (n = 39). As a result, the data of 1772 patients were included in the final analysis. Patients were categorized based on ERCP timing into the “Weekend ERCP” group (n = 148), which underwent initial drainage procedures over the weekend or holiday with therapeutic ERCP scheduled on weekdays, and the “Weekday ERCP” group (n = 1,624), where all procedures were performed during weekdays.

Study flow diagram.
Baseline characteristics and procedure-related findings of the study population
Table 1 presents the patients’ baseline characteristics. The mean age and proportion of male patients were comparable between the groups (Weekday vs Weekend: age, 66.8 ± 16.5 vs 69.0 ± 16.6 years, p = 0.117; male, 57.7% vs 60.1%, p = 0.625). No significant differences between the groups were observed in BMI or history of acute pancreatitis. However, laboratory parameters such as liver function tests (AST, ALT, total bilirubin) and white blood cell counts were significantly higher in the Weekend group than in the Weekday group. Percutaneous transhepatic gallbladder drainage (PTGBD) and percutaneous transhepatic biliary drainage (PTBD) were performed with comparable frequency in both groups. The total procedure time was significantly shorter in the Weekend group than in the Weekday group (13.1 ± 8.7 vs 16.4 ± 11.5, p < 0.001), though cannulation times were comparable. The groups did not differ significantly in detailed endoscopic protocols (e.g., sphincterotomy, balloon dilation, stent placement), although the proportion of difficult cannulations was significantly higher in the Weekday group than in the Weekend group (37.8% vs 29.1%, p = 0.043). The primary indication for ERCP in both groups was bile duct stones, followed by malignant biliary strictures.
Baseline characteristics and endoscopic findings of the patients with acute cholangitis.
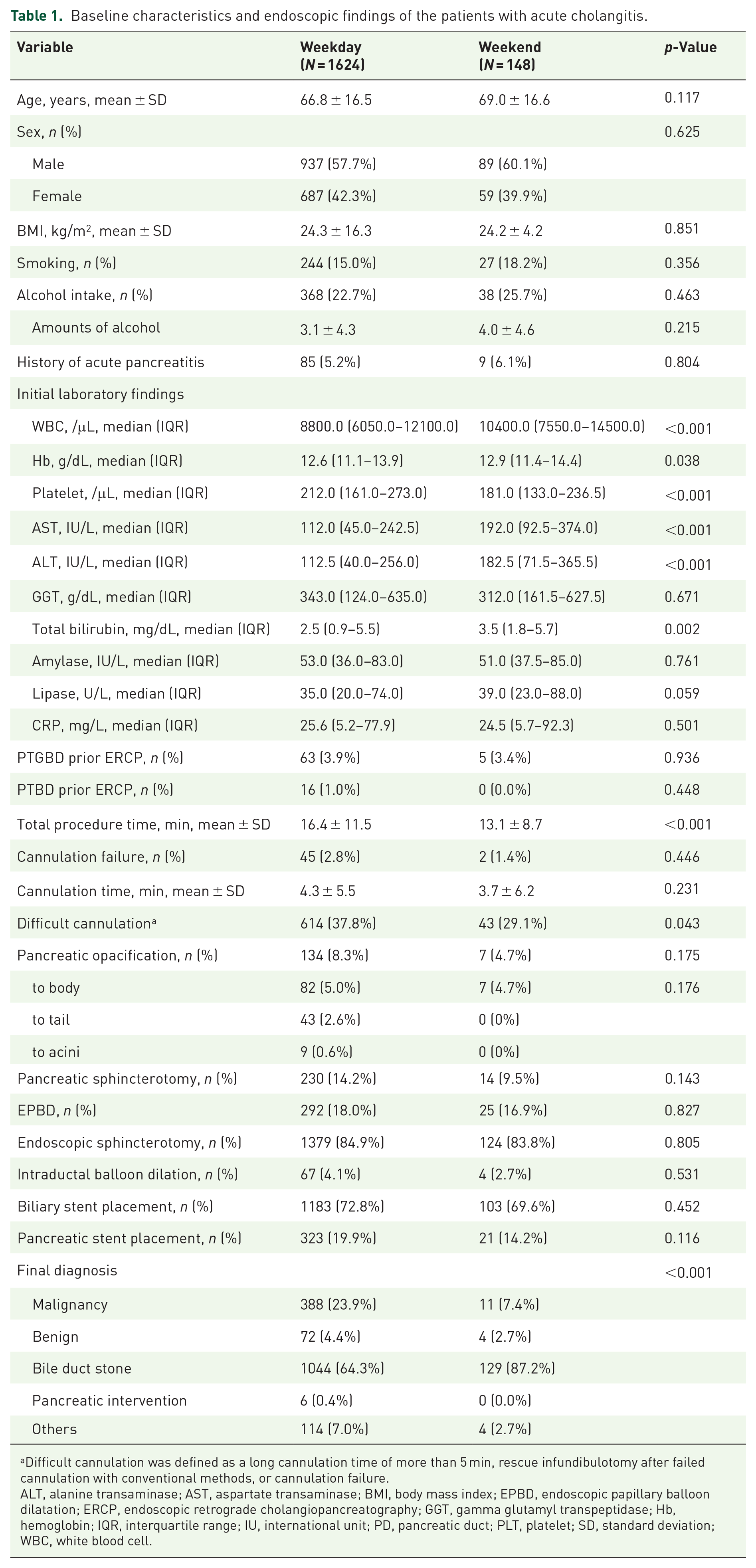
Difficult cannulation was defined as a long cannulation time of more than 5 min, rescue infundibulotomy after failed cannulation with conventional methods, or cannulation failure.
ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; EPBD, endoscopic papillary balloon dilatation; ERCP, endoscopic retrograde cholangiopancreatography; GGT, gamma glutamyl transpeptidase; Hb, hemoglobin; IQR, interquartile range; IU, international unit; PD, pancreatic duct; PLT, platelet; SD, standard deviation; WBC, white blood cell.
Clinical outcomes and AEs
Table 2 outlines the clinical outcomes and AEs of both groups. At 24 h post-ERCP, PEP was observed in 85 patients (4.8%): 79 (4.9%) in the Weekday group and 6 (4.1%) in the Weekend group, with no significant difference between the groups (p = 0.810). Moderately severe to severe PEP occurred in 34 patients (1.9%) across the cohort. PEP severity was predominantly mild. In the Weekday group, 3.0% had mild, 1.8% moderately severe, and 0.2% severe cases, compared to 2.7% mild and 1.4% moderately severe cases in the Weekend group, with no severe cases reported. All 34 patients classified as having moderately severe or severe PEP underwent contrast-enhanced abdominal CT to confirm the diagnosis and assess for complications such as necrosis or fluid collection.
Clinical outcomes and adverse events of the total cohort.
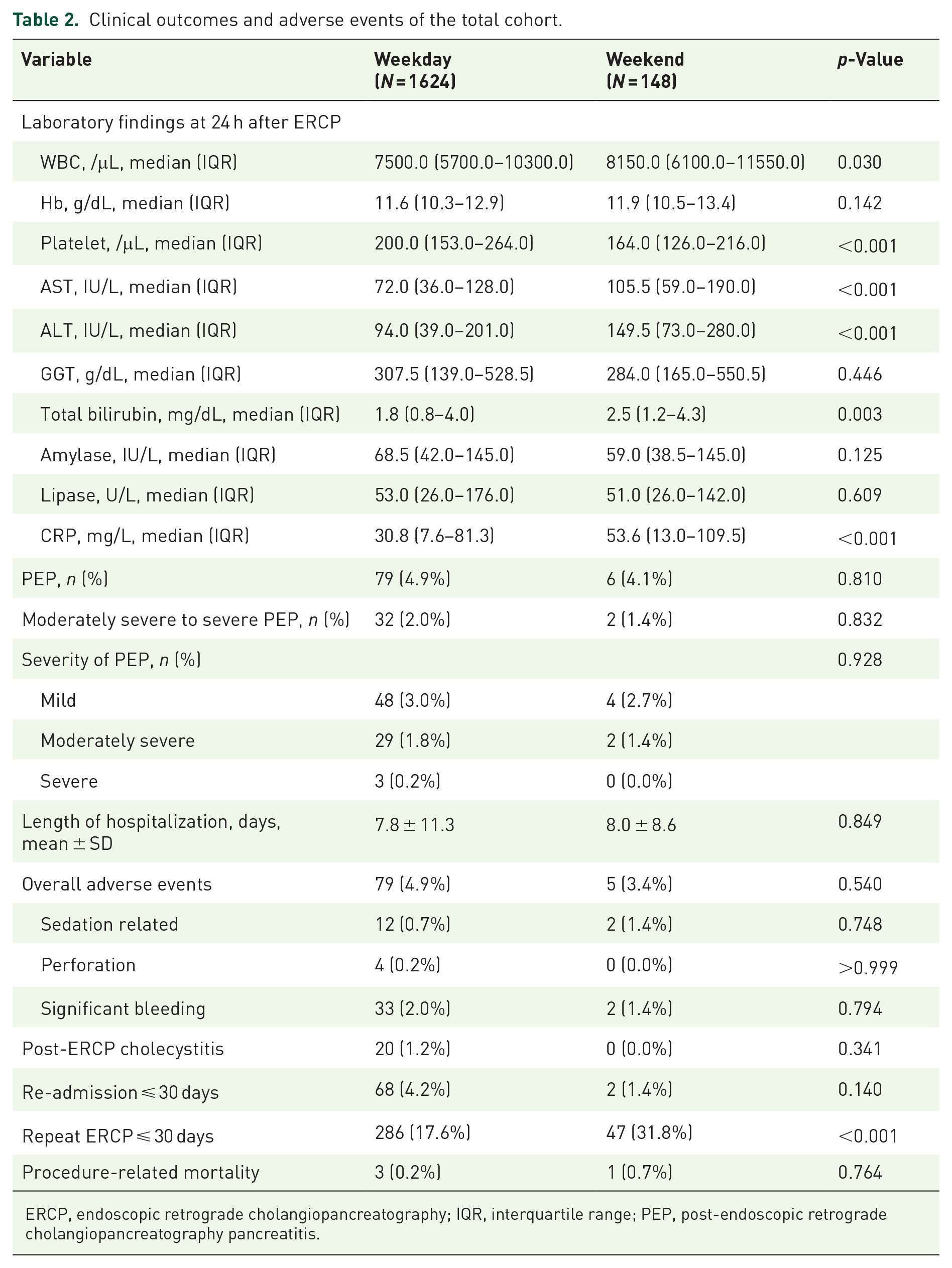
ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; PEP, post-endoscopic retrograde cholangiopancreatography pancreatitis.
The overall incidence of AEs was similar: 4.9% in the Weekday group and 3.4% in the Weekend group (p = 0.540). Procedure-related perforations occurred in four cases in the Weekday group and none in the Weekend group. All patients recovered without requiring surgical intervention. Significant bleeding occurred in 33 patients (2.0%) in the Weekday group and two (1.4%) in the Weekend group, with no significant difference. Post-ERCP cholecystitis occurred in 20 cases (1.2%) in the Weekday group, with no cases reported in the Weekend group. The LOS did not differ significantly between the groups: 7.8 ± 11.3 days in the Weekday group and 8.0 ± 8.6 days in the Weekend group (p = 0.849). Repeat ERCP procedures within 30 days were significantly more frequent in the Weekend group (31.8%) than in the Weekday group (17.6%, p < 0.001). However, re-admission rates did not differ significantly between the groups.
Risk factors for the development of PEP
Univariate and multivariate analyses identified risk factors for PEP, as presented in Table 3.
Risk factors for the development of PEP in patients who underwent ERCP on weekends and weekdays.

PEP (post-ERCP pancreatitis) was defined as new or worsened abdominal pain with either serum amylase or lipase >3 times the upper normal limit or characteristic findings of acute pancreatitis on CT performed approximately 24 h post-ERCP.
Difficult cannulation was defined as cannulation time >5 min, use of rescue infundibulotomy, or failure with standard technique.
CI, confidence interval; EPBD, endoscopic papillary balloon dilatation; ERCP, endoscopic retrograde cholangiopancreatography; OR, odds ratio; PD, pancreatic duct; PEP, post-endoscopic retrograde cholangiopancreatography pancreatitis; PTBD, percutaneous transhepatic biliary drainage; PTGBD, percutaneous transhepatic gallbladder drainage.
Multivariate analysis identified five independent risk factors for PEP: age ⩽ 60 years (OR (95% CI): 1.96 (1.20–3.13)), female sex (OR (95% CI): 1.85 (1.16–2.94)), history of acute pancreatitis (OR (95% CI): 3.47 (1.76–6.56)), difficult cannulation (OR (95% CI): 2.16 (1.24–3.70)), and EPBD (OR (95% CI): 2.41 (1.41–4.09)).
The timing of ERCP (weekend vs weekday) was not significantly associated with PEP risk.
Univariate analysis revealed that age ⩽60 years (odds ratio (OR) 95% confidence interval (CI): 1.69 (1.08–2.63)), female sex (OR (95% CI): 1.59 (1.02–2.44)), history of acute pancreatitis (OR (95% CI): 4.78 (2.58–8.44)), difficult cannulation (OR (95% CI): 2.68 (1.72–4.21)), pancreatic opacification (OR (95% CI): 3.15 (1.75–5.41)), and pancreatic sphincterotomy (OR (95% CI): 2.46 (1.47–4.00)) were significant risk factors for PEP. Traditional risk factors, including younger age, female sex, history of acute pancreatitis, pancreatic opacification, difficult cannulation, and pancreatic sphincterotomy, were significantly associated with PEP. Multivariate analysis identified the following significant risk factors for PEP: age ⩽60 years (OR (95% CI): 1.96 (1.20–3.13)), female sex (OR (95% CI): 1.85 (1.16–2.94)), history of acute pancreatitis (OR (95% CI): 3.47 (1.76–6.56)), difficult cannulation (OR (95% CI): 2.16 (1.24–3.70)), and EPBD (OR (95% CI): 2.41 (1.41–4.09)). However, the timing of ERCP (weekends vs weekdays) was not a significant risk factor for PEP.
Risk factors for the development of procedure-related AEs
Univariate and multivariate analyses identified risk factors associated with AEs, as presented in Table 4.
Risk factors for the development of AEs in patients who underwent ERCP on weekends and weekdays.

AEs (adverse events) include pancreatitis, perforation, bleeding, cholecystitis, and sedation-related events as per ASGE criteria.
Difficult cannulation was defined as cannulation time >5 min, use of rescue infundibulotomy, or failure with standard technique.
CI, confidence interval; EPBD, endoscopic papillary balloon dilatation; ERCP, endoscopic retrograde cholangiopancreatography; OR, odds ratio.
Difficult cannulation was a significant predictor (OR (95% CI): 1.72 (1.06–2.77)) of overall AEs.
In contrast, endoscopic sphincterotomy was associated with a reduced risk (OR (95% CI): 0.47 (0.29–0.79), p = 0.003) of AEs.
ERCP timing (weekend vs weekday) did not influence overall AE risk.
Univariate analysis revealed that difficult cannulation (OR (95% CI): 1.93 (1.24–3.00)) and endoscopic sphincterotomy (OR (95% CI): 0.42 (0.26–0.71)) were significantly associated with AEs. Multivariable analysis identified endoscopic sphincterotomy as a protective factor against AEs (OR (95% CI): 0.47 (0.29–0.79), p = 0.003) and difficult cannulation (OR (95% CI): 1.72 (1.06–2.77)) as a risk factor for AEs.
Clinical outcomes categorized by the timeframe of ERCP
Table 5 presents the clinical outcomes stratified by the timeframe of ERCP.
Clinical outcomes categorized by the timeframe of endoscopic intervention.

PEP severity: Mild (hospitalization 2–3 days), moderate (4–10 days), severe (>10 days or requiring intervention). Early ERCP: within 24 h of admission; Delayed ERCP: after 24 h.
ERCP, endoscopic retrograde cholangiopancreatography; PEP, post-endoscopic retrograde cholangiopancreatography pancreatitis; SD, standard deviation.
There was no significant difference in PEP or AE rates between early and delayed ERCP groups.
However, delayed ERCP was associated with a significantly longer hospital stay and higher 30-day readmission rate.
Patients were categorized based on ERCP timing: early ERCP within 24 h of admission and delayed ERCP beyond 24 h after admission. PEP occurred in 32 patients (4.3%) in the early ERCP group and 48 patients (5.2%) in the delayed ERCP group, with no significant difference. The overall incidence of AEs was similar: 4.7% in the early ERCP group and 4.8% in the delayed ERCP group. Perforations occurred in one case in the early ERCP group and three cases in the delayed ERCP group. Significant bleeding occurred in 15 patients (2.0%) in the early group and 20 patients (2.0%) in the delayed group, with no significant difference. Post-ERCP cholecystitis occurred in 9 cases (1.2%) in the early group and 11 cases (1.1%) in the delayed group. Re-admission within 30 days was significantly more frequent in the delayed ERCP group (5.0%) than in the early ERCP group (2.5%, p = 0.013), although re-ERCP rates also showed no significant differences between the groups. The average LOS was significantly longer in the delayed ERCP group (9.6 ± 13.7 days) compared to the early ERCP group (5.4 ± 5.1 days, p < 0.001).
Discussion
To our knowledge, this is the first prospective study to investigate the association between weekend ERCP and the development of PEP. Our findings suggest that a drainage-only strategy on weekends does not increase the incidence of ERCP-related AEs, including PEP, in patients with acute cholangitis compared to weekday ERCP, despite a higher frequency of repeat procedures in the weekend group. Therefore, ERCPs performed on weekends or after-hours are as safe and effective as those conducted during standard weekday hours despite potentially reduced clinical support. ERCPs are often urgent medical emergencies that may be required after-hours or on weekends and holidays. When ERCP is necessary, physicians should prioritize drainage-only procedures over complex interventions, such as complete stone removal.
This study demonstrates that weekend drainage-only ERCPs do not adversely impact outcomes, including overall AEs, PEP, LOS, or 30-day mortality. This highlights the effectiveness of weekend ERCPs limited to essential drainage for managing acute cholangitis, comparable to complete interventions on weekdays. The study also suggests that patients receive adequate resources on weekends despite reduced staffing compared to weekdays. Despite reduced staffing on weekends, patients appeared to receive adequate care, ensuring that critical care needs were met. Hakim et al.’s study, 15 which included a larger patient sample, demonstrated that weekend ERCP significantly reduces LOS, hospital costs, and charges while improving net hospital margins without compromising clinical care quality. Furthermore, a similar study 16 by Parikh et al. demonstrated that weekend inpatient ERCP is associated with reduced patient LOS. However, our findings did not corroborate the reductions in LOS observed in other studies. The difference likely stems from strategic policies in South Korea, where weekend ERCPs are limited to drainage-only procedures due to facility constraints. As a result, more comprehensive therapeutic ERCPs are scheduled for weekdays, necessitating sequential ERCPs for the weekend group. This operational approach results in sequential ERCPs for the Weekend group, as evidenced by the higher frequency of repeat procedures within 30 days (37.5% vs 18.2%). Consequently, LOS between the groups remained comparable.
Our study confirmed that a history of acute pancreatitis, female sex, difficult cannulation, and EPBD are significant risk factors for PEP. The strongest predictor for PEP was a history of acute pancreatitis, even after excluding patients with pancreatitis within 2 weeks before ERCP. This finding aligns with prior research17,18 and highlights the importance of considering previous pancreatitis episodes when assessing PEP risk. Difficult cannulation, another well-recognized risk factor, increases PEP likelihood19,20 due to repeated cannulation attempts and contrast injection into the pancreatic duct, which can lead to papillary edema and impaired drainage. 18 Female sex was also associated with a higher risk of PEP than male sex. While the mechanisms behind this increased risk in females remain unclear, our findings align with previous meta-analyses, 21 which identified similar trends.
We observed significant variation in outcomes based on the timing of ERCP after admission. Patients who underwent early ERCP had a shorter LOS than those with delayed ERCP. Early intervention likely reflects strategic decisions based on clinical urgency and patient-specific factors. A recent study 22 by Ming et al. found no significant differences in organ failure, ICU stays, or 30-day mortality, but the LOS was shorter in the early ERCP (<24 h) group (mean LOS, 8 vs 12 days; p = 0.01). Our study supports the hypothesis that early endoscopic intervention within 24 h of admission improves outcomes, mainly by reducing LOS.
Most ERCPs, whether elective or urgent, are performed during standard weekday hours when staff and resources are readily available, maximizing efficiencies and economies of scale that are harder to achieve on weekends. 1 Nevertheless, immediate ERCP may still be necessary during medical emergencies, weekends, or holidays. Previous studies3–5 have demonstrated that weekend ERCPs achieve comparable safety and effectiveness to weekday procedures, despite reduced clinical support. In our study, the significantly higher rate of repeat ERCPs in the Weekend group primarily reflects our institutional protocol, which limits weekend procedures to essential drainage (e.g., stent placement), with definitive interventions such as stone extraction deferred to weekdays. Most repeat procedures were planned for completion of biliary clearance or stent adjustment. Despite the increased frequency of re-intervention, patient outcomes—including AEs and length of hospitalization—remained comparable between groups. Nonetheless, the need for sequential procedures may increase patient burden, procedural costs, and resource utilization, and should be weighed carefully against the benefits of timely biliary decompression during weekends.
Despite its strengths, this study has some limitations. First, its observational design limits the ability to establish causal relationships between risk factors and the development of PEP. Second, variations in ERCP practices among endoscopists, driven by differences in technical skills, experience, and techniques, could have impacted outcomes. Such variations are particularly challenging to standardize in multicenter studies. Third, the absence of rectal NSAID prophylaxis, which is recommended by most international guidelines23–25 for PEP prevention, represents a potential limitation. In South Korea, rectal indomethacin or diclofenac is not commercially available, and thus was not administered to any patients in our cohort. This practice variation may limit the generalizability of our findings to settings where NSAID prophylaxis is standard, and should be considered when interpreting the risk factors for PEP. Fourth, the substantial imbalance in sample sizes between the Weekend and Weekday groups reflects the real-world disparity in procedural volume. While this distribution enhances external validity, it may have limited the statistical power to detect significant differences in rare AEs, such as PEP or perforation, particularly in the smaller Weekend group. Consequently, the possibility of a type II error—failing to detect a true difference—cannot be fully excluded. This limitation should be considered when interpreting the nonsignificant findings between groups.
Conclusion
Weekend ERCPs limited to drainage strategies are as safe as weekday procedures in terms of AE rates, even when performed with reduced clinical support. Although these procedures often necessitate subsequent therapeutic ERCPs, this staged approach enables timely biliary decompression and efficient resource utilization during off-hours. Further research is warranted to validate our findings and to optimize strategies for preventing and managing PEP in diverse clinical settings.
Supplemental Material
sj-doc-1-tag-10.1177_17562848251361694 – Supplemental material for Drainage-only strategy on weekend for endoscopic retrograde cholangiopancreatography on the risk of procedure-related adverse events: a prospective observational study
Supplemental material, sj-doc-1-tag-10.1177_17562848251361694 for Drainage-only strategy on weekend for endoscopic retrograde cholangiopancreatography on the risk of procedure-related adverse events: a prospective observational study by Eunae Cho, Se Woo Park, Kyong Joo Lee, Da Hae Park, Hyewon Cha, Dong Hee Koh, Jin Lee and Chan Hyuk Park in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.