
Abstract
Background:
The efficacy of anti-tumor necrosis factor (TNF) therapy in inflammatory bowel disease (IBD) is often compromised by the development of antidrug antibodies. In this setting, the human leukocyte antigen (HLA)-DQA1*05 allele has been significantly associated with the formation of antidrug antibodies to anti-TNF agents, loss of response, and treatment discontinuation.
Objectives:
We aimed to determine whether HLA-DQA1*05 genotyping is associated with clinically meaningful outcomes in patients with IBD.
Design:
A single-center, prospective study was conducted on patients with IBD who were naïve to biological treatment and were initiating therapy with anti-TNF agents, vedolizumab, or ustekinumab.
Methods:
All patients were genotyped for HLA-DQA1*05. The primary endpoint was the achievement of a composite outcome encompassing clinical, biochemical, and endoscopic remission at week 54, stratified by HLA-DQA1*05 status. The secondary endpoints included the evaluation of therapeutic persistence and the development of antidrug antibodies.
Results:
One hundred biologic-naïve patients with IBD initiating biological therapy were included in the study (72 on anti-TNF, 18 on vedolizumab, and 10 on ustekinumab); of these, 43% were HLA-DQA1*05 positive. The presence of the HLA-DQA1*05 allele was not associated with worse clinical outcomes, defined as the composite of clinical, biochemical, and endoscopic remission at week 54, in patients treated with anti-TNF agents, vedolizumab, or ustekinumab. In addition, no significant correlation was observed between the HLA-DQA1*05 genotype and reduced therapy persistence or increased immunogenicity.
Conclusion:
In our cohort of patients with IBD, the HLA-DQA1*05 genotype was not associated with a higher risk of treatment cessation or worse clinical outcomes.
Trial registration:
Can we rely on HLA to predict resistance to biological therapy in patients with IBD?
URL: https://clinicaltrials.gov/study/NCT05040854?cond=Can%20we%20rely%20on%20HLA&rank=1. Registration number: NCT05040854 (clinicaltrials.gov).
Introduction
Inflammatory bowel disease (IBD), which includes Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic, relapsing, and remitting gastrointestinal inflammatory disease.1,2
Therapeutic targets in IBD have evolved over the decades, shifting from clinical remission to both clinical and endoscopic remission, as outlined by the Selecting Therapeutic Targets in Inflammatory Bowel Disease II consensus. 3 Mucosal healing is now recognized as a key treatment target and a strong predictor of reduced surgeries, fewer hospitalizations, and long-term clinical remission. 4 However, transmural healing in CD has been associated with improved long-term outcomes and may represent a more suitable treatment goal than mucosal healing.4,5
Regarding pharmaceutical interventions, monoclonal antibodies have revolutionized IBD therapy. Anti-tumor necrosis factor (TNF) antibodies, such as infliximab, adalimumab, golimumab, and certolizumab, were the first biologics introduced for clinical use. Other therapies are now available, including anti-integrin (such as vedolizumab), anti-interleukin-12/23 (such as ustekinumab), anti-interleukin-23 agents targeting the p19 subunit (such as mirikizumab, guselkumab, and risankizumab), and small molecules (ClinicalTrials.gov identifiers: NCT04033445, NCT03105128, NCT03104413).6–8
Ideally, IBD treatment should be effective, safe, and affordable. The introduction of infliximab and adalimumab biosimilars has helped anti-TNF therapy meet the affordability requirement. However, treatment failure with anti-TNF agents is common, with 10%–40% of patients classified as primary non-responders9–11 and 23%–46% experiencing secondary loss of response even after dose intensification. 12
The mechanisms underlying anti-TNF treatment failure can be divided into pharmacokinetic factors (including adherence to treatment, formation of antidrug antibodies, and increased drug clearance) and disease-related factors. 13 Among these, the development of immunogenicity via antidrug antibodies is common in anti-TNF therapy and is the main cause of low drug trough levels, infusion reactions, and treatment nonresponse. To mitigate this, biological therapy is often combined with immunosuppressants to reduce immunogenicity and improve clinical outcomes in CD and UC.14,15
Therefore, predicting which patients will develop anti-TNF antibodies could offer valuable insights for guiding treatment selection, particularly the need for combination therapy with immunosuppressants. In this context, the Personalized Anti-TNF Therapy in CD (PANTS) study was conducted to address the challenges of anti-TNF treatment failure in IBD. It provided insights into the factors influencing primary nonresponse, loss of response, and immunogenicity to infliximab and adalimumab, ultimately guiding more personalized treatment approaches. The study identified a significant association between the human leukocyte antigen (HLA)-DQA1*05 allele and the development of antidrug antibodies in patients with CD.16,17 This finding has been corroborated by subsequent studies, including systematic reviews and meta-analyses, in both CD and UC.18–21 However, more recent studies have not consistently found a significant association between HLA-DQA1*05 and immunogenicity or loss of response to first-line anti-TNF agents in patients with IBD, suggesting that this allele may not serve as a reliable predictor of therapeutic outcomes.22,23 Studies with non-TNF biologics, such as ustekinumab and vedolizumab, had similar results.24–26 Thus, the association between HLA-DQA1*05 positivity and loss of response to anti-TNF therapies in IBD populations remains under investigation and lacks confirmation in specific patient subsets.
Therefore, this study aimed to determine whether HLA-DQA1*05 genotyping positivity was associated with clinically meaningful outcomes in a biologic-naïve IBD cohort.
Materials and methods
This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 27
Study design and patient selection
This single-center, prospective cohort study was conducted between July 2021 and May 2023. We enrolled adult patients (⩾18 years) diagnosed with IBD according to the European Crohn’s and Colitis Organization criteria, 26 who were followed up at the IBD consultation of the Local Health Unit Viseu Dão-Lafões (a tertiary unit in central Portugal). We consecutively included biologic-naïve adult patients with IBD who initiated biological therapy with infliximab, adalimumab, vedolizumab, or ustekinumab. Study visits were scheduled at the first infusion and at weeks 14, 30, and 54.
Sample size calculation
The sample size was calculated based on a 95% confidence interval (CI) and a 5% margin of error. Drawing on data from the PANTS study, the estimated required sample size for infliximab treatment was 114 patients. No formal sample size calculations were conducted for the remaining biologics owing to the lack of large-population studies.
Data collection and definitions
At the first visit, data were collected on demographic characteristics (age and sex), body mass index, smoking behavior, family history of IBD, and disease-related features, including IBD type (UC or CD), age at diagnosis, disease duration, localization and behavior, and history of IBD-related surgeries. Information on disease activity was collected using the Mayo clinical sub-score, Harvey–Bradshaw score, Mayo endoscopic score, Crohn’s Disease Endoscopic Index of Severity, and Rutgeerts scores. Data on inflammatory biomarkers (C-reactive protein and calprotectin) and treatment groups (biological therapy as monotherapy or in combination with immunomodulators) were also collected. At weeks 14, 30, and 54, data were collected on disease activity, inflammatory biomarkers, and pharmacokinetic parameters, including drug trough levels and antidrug antibodies.
Biological therapy was adjusted according to standardized protocols, including proactive therapeutic drug monitoring (TDM) and dose optimization. Doses were escalated to reach a target trough concentration of ⩾10 μg/mL for infliximab, ⩾7 μg/mL for adalimumab, and ⩾14 μg/mL for vedolizumab during the maintenance phase in CD and UC. According to the protocol, inflammatory biomarkers were assessed at each treatment during the induction phase and at every other treatment during the maintenance phase. Serum drug trough levels and antidrug antibodies were measured using the i-Tracker automated chemiluminescence assay (Theradiag, Croissy Beaubourg, France), a drug-tolerant test. For infliximab, adalimumab, and vedolizumab, these measurements were performed at every other treatment during the maintenance phase. Immunogenicity was defined as an antidrug antibody concentration of ⩾10 ng/mL for infliximab, ⩾10 ng/mL for adalimumab, and ⩾35 ng/mL for vedolizumab. Dose adjustments for ustekinumab were not applied, as current evidence does not support the use of TDM for this drug.
Drug persistence was defined as the duration of treatment until therapy failure for a given biological therapy used to treat IBD. Therapy discontinuation due to failure was considered when treatment was stopped due to primary nonresponse (lack of response during the induction phase), secondary loss of response (loss of response during the maintenance phase), or the development of side effects. All patients were screened for HLA-DQA1*05 at baseline. Genotyping was performed using the Luminex XMap 200® platform (Luminex Corporation, EUA) and the LABType SSO DQA1DQB1 kit (One Lambda, Inc., EUA). The results were interpreted using Fusion software (version 4.0) (One Lambda, Inc., EUA).
The primary endpoint of this study was the association between the presence of the HLA-DQA1*05 allele and achievement of the composite outcome at the end of the study, encompassing clinical, biochemical, and endoscopic remission. For CD, remission was defined as a Harvey–Bradshaw score ⩽5, calprotectin ⩽150 μg/g, and either Crohn’s Disease Endoscopic Index of Severity (CDEIS) ⩽6 or Rutgeerts score i0. For UC, remission was defined as a partial Mayo Index score ⩽2, calprotectin ⩽150 μg/g, and endoscopic Mayo score ⩽1.
Secondary endpoints included the evaluation of therapy persistence and development of antidrug antibodies according to the HLA-DQA1*05 genotype. The latter outcome was not evaluated in patients treated with ustekinumab.
Statistical analysis
Data were analyzed using IBM Statistical Package for Social Sciences Statistics version 29 (IBM Corporation, EUA). Descriptive statistics were used to summarize patient demographics and disease characteristics. Categorical variables are presented as proportions or absolute counts, and comparisons were made using Pearson’s χ2 and Fisher’s exact tests, as appropriate. Continuous variables are expressed as mean and standard deviation (SD) for normally distributed data or as median and interquartile range for non-normally distributed data. Group comparisons for continuous variables were performed using the Student’s t test or Mann–Whitney U test, depending on the data distribution. Kaplan–Meier survival analysis was used to assess therapy persistence across different biological treatments. Stratified Fisher’s exact test and Cox hazard regression were used to assess potential confounders and risk factors associated with therapy discontinuation. Statistical significance was set at p ⩽ 0.05.
Ethical considerations
The study was approved by the local ethics committee (Ethics Committee of the Local Health Unit Viseu Dão-Lafões) and was conducted according to the guidelines of the Declaration of Helsinki.
Results
Study population
Between July 2021 and May 2023, 100 biologic-naïve patients with IBD were enrolled in the study. A total of 122 patients were invited to participate; of these, 100 accepted and signed the informed consent form, while 22 declined. Baseline characteristics of the study population are presented in Table 1. In this cohort, 53 patients (53%) were female, the mean age at diagnosis was 41.9 years (15.3), and 67 patients (67%) had a diagnosis of CD. The mean disease duration was 8.2 years (8.2).
Baseline characteristics of the study population.
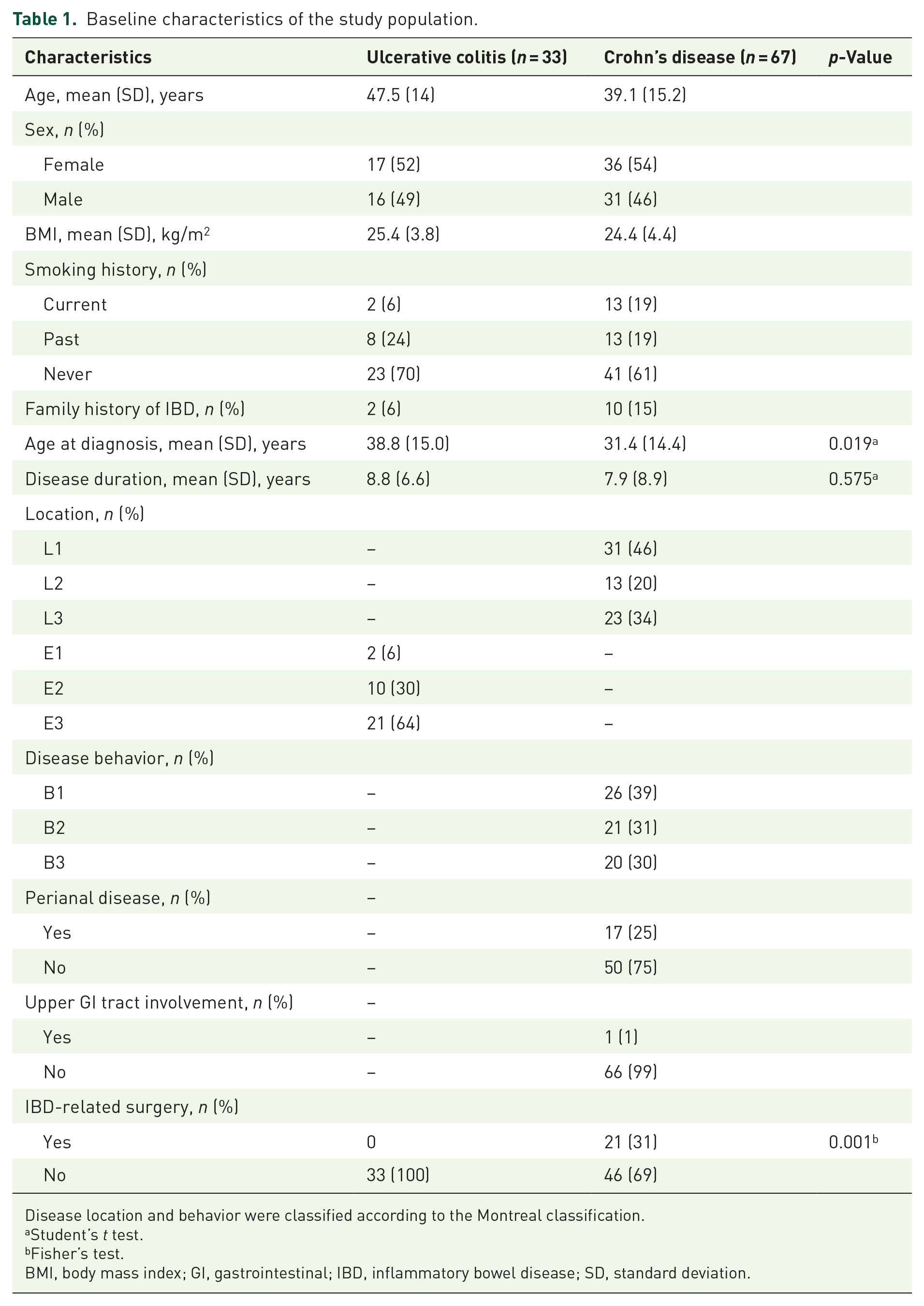
Disease location and behavior were classified according to the Montreal classification.
Student’s t test.
Fisher’s test.
BMI, body mass index; GI, gastrointestinal; IBD, inflammatory bowel disease; SD, standard deviation.
Among patients with CD, 46% (n = 31) had ileal involvement, 20% (n = 13) had colonic disease, and 34% (n = 23) had ileocolonic disease. Regarding disease behavior, 39% (n = 26) exhibited a non-stricturing/non-penetrating phenotype, 31% (n = 26) had stricturing disease, and 30% (n = 20) had penetrating behavior. Most patients with UC had pancolitis (n = 22; 64%). At baseline, none of the patients with UC had undergone IBD-related surgery, whereas 31% of patients with CD had a history of such surgery (p < 0.001).
Biological therapy
Regarding biological therapy, 72 patients (72%) received anti-TNF (51 on infliximab and 21 on adalimumab), 18 (18%) received anti-integrin therapy (vedolizumab), and 10 (10%) started anti-interleukin 12/23 therapy (ustekinumab). Biological therapy was selected based on the patient’s comorbidities and age. Patients receiving vedolizumab and ustekinumab had more personal histories of neoplastic and cardiac diseases than those receiving infliximab (p = 0.017 and p = 0.001, respectively). Although not statistically significant, those treated with anti-TNF agents tended to be younger, with a mean age of 40.6 ± 14.7 years for infliximab compared with 44.9 ± 16.1 years for vedolizumab and 45.7 ± 18.0 years for ustekinumab.
In total, 26 (26%) patients received combination therapy, starting with immunomodulatory treatment alongside their first biologic therapy. No differences were observed in the use of immunosuppressive drugs between HLA-DQA1*05-positive and HLA-DQA1*05-negative patients.
The mean time from IBD diagnosis to the initiation of biological therapy was 52.6 (57.4) weeks for all patients. No significant difference was observed based on HLA-DQA10*5 status, with 50.8 weeks for HLA-DQA1*05 positive patients and 55 weeks for negative patients (p = 0.307). Patients with CD had a significantly shorter mean time from IBD diagnosis to the start of biological therapy than those with UC (42.4 weeks in CD vs 73.5 weeks in UC, p < 0.001).
HLA-DQA1*05 status
Forty-three percent (43%) of the patients were HLA-DQA1*05 positive, including 12 (36%) with UC and 31 (46%) with CD (Table 2).
HLA-DQA1*05 genotyping.

HLA, human leukocyte antigen.
Evaluation by IBD diagnosis
Of the total patient population, 54 (54%) were responders, and 41 (41%) were nonresponders, including 11 primary and 30 secondary nonresponders. In addition, five patients (5%) discontinued the medication because of adverse effects. No differences were identified in achieving clinical, biochemical, and endoscopic remission at week 54 based on the HLA-DQA1*05 genotype (p = 0.155; Table 3). A subanalysis according to IBD diagnosis revealed that HLA genotyping had no impact on achieving the composite outcome (Tables 4 and 5). The mean time from IBD diagnosis to the initiation of biological therapy did not differ between patients who achieved the composite outcome at week 54 and those who did not (55.4 weeks in responders vs 50.7 weeks in nonresponders; p = 0.689).
Evaluation according to HLA-DQA1*05 genotyping.

Student’s t test.
Chi-square test.
Mann–Whitney test.
Missing values in six patients receiving ustekinumab.
Missing values in four patients receiving ustekinumab.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation.
Evaluation according to HLA-DQA1*05 genotyping in patients with Crohn’s disease.
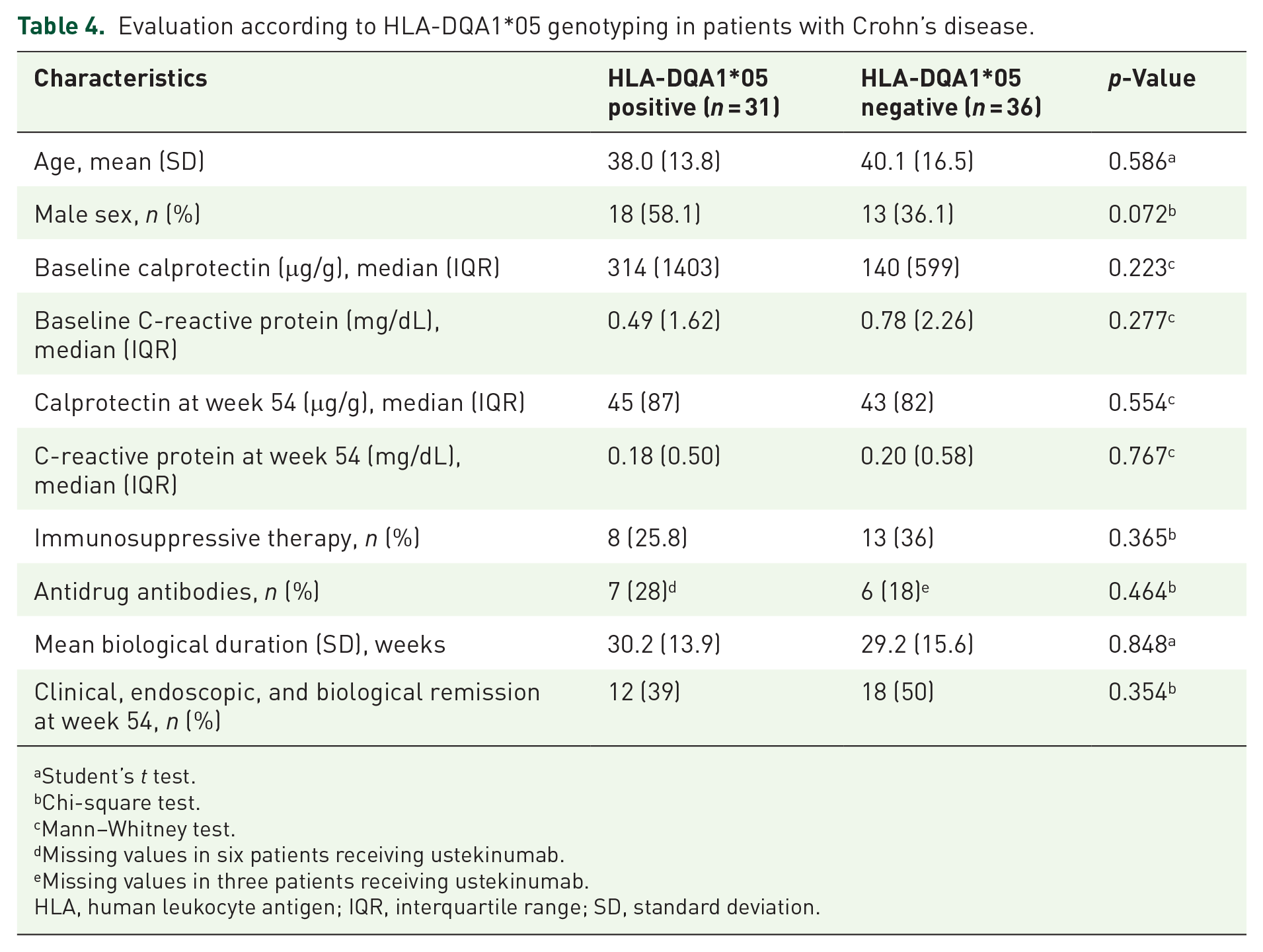
Student’s t test.
Chi-square test.
Mann–Whitney test.
Missing values in six patients receiving ustekinumab.
Missing values in three patients receiving ustekinumab.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation.
Evaluation according to HLA-DQA1*05 genotyping in patients with ulcerative colitis.

Student’s t test.
Chi-square test.
Mann–Whitney test.
Fisher’s test.
Missing values in one patient receiving ustekinumab.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation.
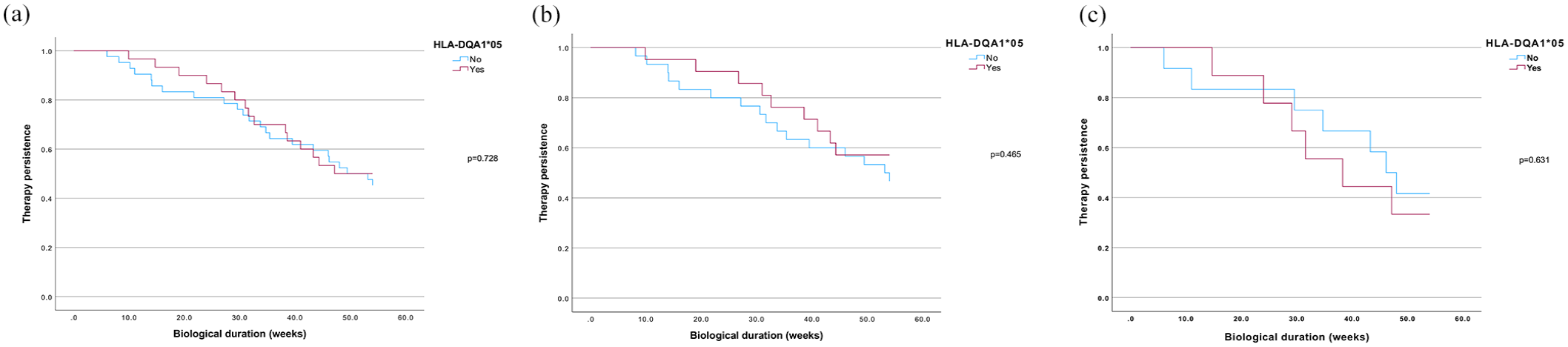
Kaplan–Meier survival analysis showed no statistically significant differences in therapeutic persistence between the HLA groups among all patients with HLA-DQA1*05 genotyping. In a sub-analysis by IBD diagnosis, HLA genotyping did not impact therapeutic persistence (Figure 1). HLA-DQA1*05 genotyping had no effect on the development of antidrug antibodies in the overall population. Ten patients who received ustekinumab were excluded from this analysis. Among patients with CD, 7 of 25 (28%) HLA-DQA1*05 positive patients and 6 of 33 (18%) negative patients developed antidrug antibodies, with no statistically significant difference. In patients with UC, 3 of 12 (25%) positive patients and 3 of 20 (15%) negative patients developed antidrug antibodies; however, this difference was not statistically significant. Serum levels of anti-TNF and anti-integrin at weeks 14 and 30 did not differ based on genotyping, and drug optimization was not statistically different between the groups.

Therapy persistence according to HLA-DQA1*05 genotyping in all patients (a), ulcerative colitis (b), and Crohn’s disease (c).
Sub-analysis by type of biologic
Anti-TNF therapy (Table 6 and Figures 2 –4)
Of the 100 patients, 72 (72%) received anti-TNF therapy: 51 received infliximab and 21 received adalimumab. Among them, 42% were HLA-DQA1*05 positive. No differences in age or sex distribution were observed in this subgroup. Among HLA-DQA1*05 positive patients, 10 of 30 (14%) developed antidrug antibodies compared to 9 of 42 (21%) HLA-DQA1*05 negative patients, with no significant difference. Antidrug antibody development showed no impact when analyzed based on concomitant immunosuppressant use or biologics as monotherapy. Thirty-eight patients required therapeutic escalation to another biological agent. The mean duration of biological therapy and the achievement of composite outcomes at week 54 did not significantly differ between groups. Kaplan–Meier survival subanalysis showed no differences in therapeutic persistence regardless of immunosuppressant therapy use. Serum anti-TNF levels at weeks 14 and 30 did not differ by genotype, and dose adjustments were not statistically different between groups.
Evaluation according to HLA-DQA1*05 genotyping in patients treated with anti-TNF.

Student’s t test.
Chi-square test.
Mann–Whitney test.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation; TNF, tumor necrosis factor.
Therapy persistence according to HLA-DQA1*05 genotyping in all anti-TNF-treated patients (monotherapy and combination therapy) (a), anti-TNF monotherapy (b), and anti-TNF combination therapy (c).

Therapy persistence according to HLA-DQA1*05 genotyping in all adalimumab-treated patients (monotherapy and cotherapy) (a) and adalimumab monotherapy (b). No statistical analyses were performed for adalimumab in combination therapy.

Therapy persistence according to HLA-DQA1*05 genotyping in infliximab-treated patients (monotherapy and cotherapy) (a), anti-TNF in monotherapy (b), and anti-TNF in cotherapy (c).
A sub-analysis of the anti-TNF subtypes was also conducted. HLA-DQA1*05 status was not associated with significant differences in achieving the composite outcome in either the infliximab monotherapy and combination therapy groups (p = 0.60 and p = 0.68, respectively) or the adalimumab monotherapy and combination therapy groups (p = 0.960 and p = 0.157, respectively).
For both therapies, Kaplan–Meier survival curves showed no differences in biological therapy duration according to HLA status, regardless of concomitant immunosuppressive therapy.
Anti-integrin therapy (Table 7 and Figure 5)
Eighteen patients were treated with vedolizumab, of whom seven (39%) were HLA-DQA1*05 positive. The mean age and sex distributions were similar between groups. Baseline C-reactive protein levels were comparable between HLA-DQA1*05-positive and HLA-DQA1*05-negative patients. Although baseline clinical scores were similar in patients with both CD and UC, calprotectin levels were significantly higher in HLA-DQA1*05 positive patients (p = 0.01). None of the patients developed antidrug antibodies. Seven patients required therapeutic escalation to other biological agents. Among those treated with vedolizumab, none of the HLA-DQA1*05-positive patients reached week 54 of treatment, whereas 10 of 11 negative patients did. Of these, 9 (90%) achieved the composite outcome. However, after stratified analysis adjusting for potential confounders, factors such as age <40 years (p = 0.143), baseline calprotectin level >150 μg/g (p = 0.286), moderate/severe baseline Harvey–Bradshaw score (p = 0.167), and moderate/severe clinical Mayo score (p = 0.333) were not significantly associated with outcome achievement. Kaplan–Meier survival analysis showed that HLA-DQA1*05-positive patients had significantly lower persistence with vedolizumab than HLA-negative patients. However, Cox proportional hazards regression analysis revealed no significant association between HLA-DQA1*05 status and therapy persistence (hazard ratio (HR) = 31.186, 95% CI: 0.229–4242.521, p = 0.170).
Evaluation according to HLA-DQA1*05 genotyping in patients treated with anti-integrin therapy.

Student’s t test.
Chi-square test.
Mann–Whitney test.
No patients.
Fisher’s test.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation.

Therapy persistence according to HLA-DQA1*05 genotyping in patients treated with anti-integrin drugs.
Anti-interleukin 12/23 therapy (Table 8 and Figure 6)
Ten of the 100 patients were treated with ustekinumab; of these, 6 (60%) were HLA-DQA1*05 positive. No differences in age or sex were observed between the HLA genotypes. One patient required therapeutic escalation to another biologic. The mean duration of biological therapy and achievement of the composite outcome at week 54 did not differ according to HLA genotype. In addition, no differences in therapeutic persistence were observed.
Evaluation according to HLA-DQA1*05 genotyping in patients treated with ustekinumab.

Student’s t test.
Fisher’s test.
Mann–Whitney test.
Chi-square test.
HLA, human leukocyte antigen; IQR, interquartile range; SD, standard deviation.

Therapy persistence according to HLA-DQA1*05 genotyping in anti-interleukin 12/23 treated patients.
Treatment optimization and escalation strategies
Table 9 summarizes treatment optimization over the 54-week period. Between weeks 14 and 30, 27 patients required dose escalation, including infliximab (dose increases or interval shortening), vedolizumab (interval shortening), and adalimumab (interval shortening). Further adjustments between weeks 30 and 54 were made in 22 patients, primarily comprising further dosing interval reductions in previously optimized cases. Serum levels of anti-TNF and vedolizumab measured at weeks 14 and 30 did not differ according to the HLA genotype, and dose adjustments were not statistically different between the groups. During follow-up, 11 patients receiving infliximab monotherapy were started on immunosuppression with azathioprine.
Number of patients with therapeutic escalation.

Previous dose shortening between weeks 14 and 30.
Previous dose shortening within the same period.
In cases of failure of the first-line biological therapy, second-line treatment strategies included switching to an alternative anti-TNF agent, with or without concomitant immunosuppression, or transitioning to vedolizumab or ustekinumab. None of the patients were treated with small-molecule therapies.
Regarding surgical interventions during follow-up, two patients underwent perianal surgery, and one required abdominal surgery for CD; no surgical procedures were reported among patients with UC.
Discussion
In this study, we explored the possible relationship between the presence of the HLA-DQA1*05 allele and the clinical response to anti-TNF, vedolizumab, and ustekinumab in biologic-naïve patients with IBD. Accurate prediction of antidrug antibody development and, more critically, loss of response to therapy in patients treated with biologics remains critical for optimizing therapeutic strategies and tailoring treatment approaches in high-risk individuals.
In this prospective study, including 100 patients initiating treatment with TNF antagonists, vedolizumab or ustekinumab, under proactive TDM for the first two classes, HLA-DQA1*05 noncarriers did not show worse clinical outcome, defined as combined clinical, biochemical, and endoscopic remission by the end of the study. Although a considerably higher achievement of the primary endpoint was observed among HLA-DQA1*05 carriers treated with vedolizumab, this association appeared to be driven by potential confounders, as suggested by the results of the stratified analysis results. Regarding secondary endpoints, HLA-DQA1*05 genotyping was not associated with differences in therapeutic persistence or antidrug antibody development across all treatment groups. The immunogenic potential of this allele in anti-TNF therapy was not observed in our study, regardless of treatment with anti-TNF monotherapy or in combination with an immunosuppressant.
The association between HLA-DQA1*05 and increased rates of anti-TNF therapy immunogenicity was first highlighted in 2020 by the PANTS study, a large genome-wide association study involving 1240 biologic-naïve patients with IBD. This study identified a significant association between HLA-DQA1*05 allele positivity and increased antidrug antibody development, with the highest immunogenicity rate observed in patients treated with infliximab monotherapy. 16 This finding contributed to the growing interest in incorporating pharmacogenetic testing into clinical decision-making for biological therapies. However, our results did not replicate this association, which may reflect differences in cohort characteristics, sample sizes, study designs, or the implementation of proactive TDM and combination strategies in our population.
The potential effect of HLA-DQA1*05 on antidrug antibody formation has also been described for biologicals other than anti-TNF therapies. The ABIRISK consortium 28 highlighted this broader risk, while Wilson et al. 29 retrospectively corroborated the findings of the PANTS study, reporting significant associations between HLA-DQA1*05 positivity and development of infliximab antibodies, loss of response, treatment discontinuation, and adverse drug events in patients with IBD. Similar associations have been observed in other studies, linking this genotype to less favorable outcomes among anti-TNF-treated patients.19,22,23 In contrast, more recent literature challenges the clinical relevance of this allele in predicting anti-TNF treatment failure. For instance, in a retrospective study of 199 biologic-naïve patients with IBD treated with anti-TNF, Pascual et al. 30 found that HLA-DQA1*05 carrier status was not a predictor of therapy failure. 22 These findings suggest that HLA-DQA105 may not universally predict immunogenicity or treatment nonresponse.
Our results align with studies assessing the impact of the HLA-DQA1*05 allele in the context of proactive TDM. 22 In a 2022 retrospective single-center cohort study including 112 patients with IBD starting anti-TNF therapy, Fuentes-Valenzuela et al. 23 also found no association between HLA-DQA1*05 positivity and a higher risk of treatment cessation or worse clinical outcomes under proactive TDM. 22
Similarly, data from the Precision IFX study found no evidence of an association between carriage of the HLA-DQA1*05 allele and a higher likelihood of developing antidrug antibodies or shorter treatment effectiveness. In this cohort, the primary factor associated with antidrug antibody formation was failure to achieve a trough infliximab level of 17 µg/mL by the third dose (HR: 5.0; 95% CI: 1.8–13.7). 22 The extended 3-year data from the PANTS study, published in 2024, continue to identify HLA-DQA1*05 positivity as a risk factor for the development of antidrug antibodies; however, it appears limited to patients treated with infliximab. These extended analyses also highlight the crucial role of proactive TDM, as low anti-TNF concentrations at week 14 predict treatment failure and immunogenicity for both infliximab and adalimumab. 17
As for ustekinumab and vedolizumab, current evidence does not support an association between HLA-DQA1*05 and worse clinical outcomes or reduced drug persistence.24,25 These findings suggest that the impact of this allele may vary depending on the biologic used and is likely modulated by treatment strategies such as proactive TDM.
The main strengths of our study include its prospective design, use of a robust endpoint comprising clinical, biochemical, and endoscopic remission, and multiple intermediate clinical and analytical evaluations throughout follow-up.
However, this study has some limitations. First, it was a single-center study with a relatively small sample size, particularly for the vedolizumab and ustekinumab subgroups. In addition, the inclusion of biologics with different mechanisms of action and immunogenic profiles may have introduced heterogeneity, limiting direct comparisons between treatment groups.
In our real-life cohort of biologically naïve patients with IBD treated with anti-TNF, vedolizumab, and ustekinumab, the presence of the HLA-DQA1*05 allele was not a predictor of worse clinical outcomes, treatment discontinuation, or increased immunogenicity. Further prospective studies with larger cohorts and clinically meaningful outcomes are warranted to elucidate the potential predictive value of HLA-DQA1*05 genotyping in clinical practice.