
Abstract
Background:
Physician assessments of patient symptoms may not align with the patients’ subjective experiences, potentially affecting disease management. The key drivers of patients with Crohn’s disease (CD) regarding their physicians’ engagement in treatment decision-making are unknown.
Objective:
This study aimed to compare cognitive differences between patients and gastroenterologists in the diagnostic and treatment processes of CD.
Design:
Retrospective multicenter study.
Methods:
This study was conducted at 39 inflammatory bowel disease (IBD) centers across China, ultimately recruiting 601 patients with CD and 181 gastroenterologists.
Results:
Regarding symptom focus, physicians were more concerned about abdominal pain, while patients, particularly inpatients, were more concerned about frequent medical visits. There were also significant differences in the treatment goals. Patients prioritized improving their quality of life, whereas physicians showed a hierarchical difference in their focus: resident and attending physicians emphasized mucosal healing, while deputy chief physicians and above placed greater importance on long-term remission (clinical, endoscopic, and histological). Regarding knowledge gaps about CD, physicians significantly overestimated patients’ understanding of biologics (93.37% vs 71.55%, κ = 0.117), with inpatients showing slightly higher awareness than outpatients (73.96% vs 70.42%). Regarding follow-up compliance, the discrepancy was especially prominent: 46.96% of physicians recommended follow-up every ⩽2 months, while 61.73% of patients preferred follow-up every 6 months. The economic burden of CD revealed that 21.30% of patients were willing to spend over 50% of their household income on treatment, which far exceeded physicians’ expectations (9.94%). Lastly, there was a significant divergence in decision-making models: 49.17% of physicians advocated for shared decision-making, but only 14.31% of patients agreed with this model (κ = 0.353).
Conclusion:
There are notable cognitive disparities between patients with CD and physicians in their approaches to disease management, particularly concerning follow-up frequency and treatment options. These differences underscore the need for targeted interventions to bridge the gap between patient and physician perspectives. Therefore, future research should focus on enhancing communication between doctors and patients and enabling them to play a more active role in health management and treatment decisions.
Plain language summary
A multi-center study in China revealed significant cognitive differences between Crohn’s disease patients and doctors in areas such as symptom focus, treatment goals, follow-up frequency, and decision-making patterns. The study highlights the need for collaborative decision-making between doctors and patients to optimize disease management.
Introduction
Crohn’s disease (CD) is a chronic, relapsing inflammatory bowel disease (IBD) characterized by unpredictable episodes of active disease alternating with periods of remission.1–3 In moderate-to-severe cases, complications such as abscesses, strictures, and fistulas can necessitate hospitalization and surgical intervention. Although CD is less prevalent than other chronic conditions, its recurring symptoms significantly affect patients’ physical, mental, and emotional well-being and overall quality of life (QoL).4–7
As treatment options become increasingly complex, careful consideration of the individualized benefits and risks associated with each therapy is essential. The “targeted therapy” approach has shifted treatment goals from merely controlling symptoms and improving QoL to interrupting disease progression, promoting mucosal healing, and maintaining long-term remission (clinical, endoscopic, and histological remission).8,9 Despite these advancements, the understanding of diseases among patients with CD is often underestimated in many healthcare systems. 10 In addition, research on specific treatment targets crucial for Chinese patients with CD remains relatively limited. Self-assessment of clinical conditions and disease severity, along with the choice of various medications and surgical options, significantly influence patients’ treatment decisions and information-seeking behaviors.11,12 Physicians often underestimate the impact of the disease on patients. 13 However, the perspectives of patients and physicians on how these issues are handled in clinical practice have not yet been thoroughly evaluated. Understanding the views of these two groups is critical for identifying gaps, unmet needs, and differences in viewpoints. Identifying such disparities could help implement measures to improve two-way communication and foster a deeper mutual understanding.
In light of these considerations, we report the findings from a multicenter retrospective study in China, an international web-based survey encompassing physicians’ and patients’ perspectives on diagnosis and treatment of CD, the social burdens associated with the disease, and the dynamics of physician–patient relationships. Our objective was to identify patient preferences and expectations regarding treatment goals, rather than focusing solely on treatment, to promote more effective disease management approaches.
Materials and methods
Study design and participant recruitment
This multicenter study was conducted between July 2020 and July 2021 across 39 IBD centers in China using convenience sampling to recruit physicians (registered with ClinicalTrials.gov, identifier ChiECRCT20200202). Eligible physicians were required to diagnose, identify, and treat CD and complete detailed questionnaires (Figure 1). Subsequently, these physicians recruited outpatients or inpatients with CD who met the inclusion criteria. All data from these patients were used for the analysis and description. The inclusion criteria were at least 1 year of follow-up with the participating physician, with one or more visits in the first 6 months, adherence to CD treatment recommendations from the Third European Evidence-based Consensus on Diagnosis and Management of CD, Chinese consensus on IBD diagnosis and treatment,14–16 and the ability to complete the questionnaire independently. Data from eligible patients were analyzed.
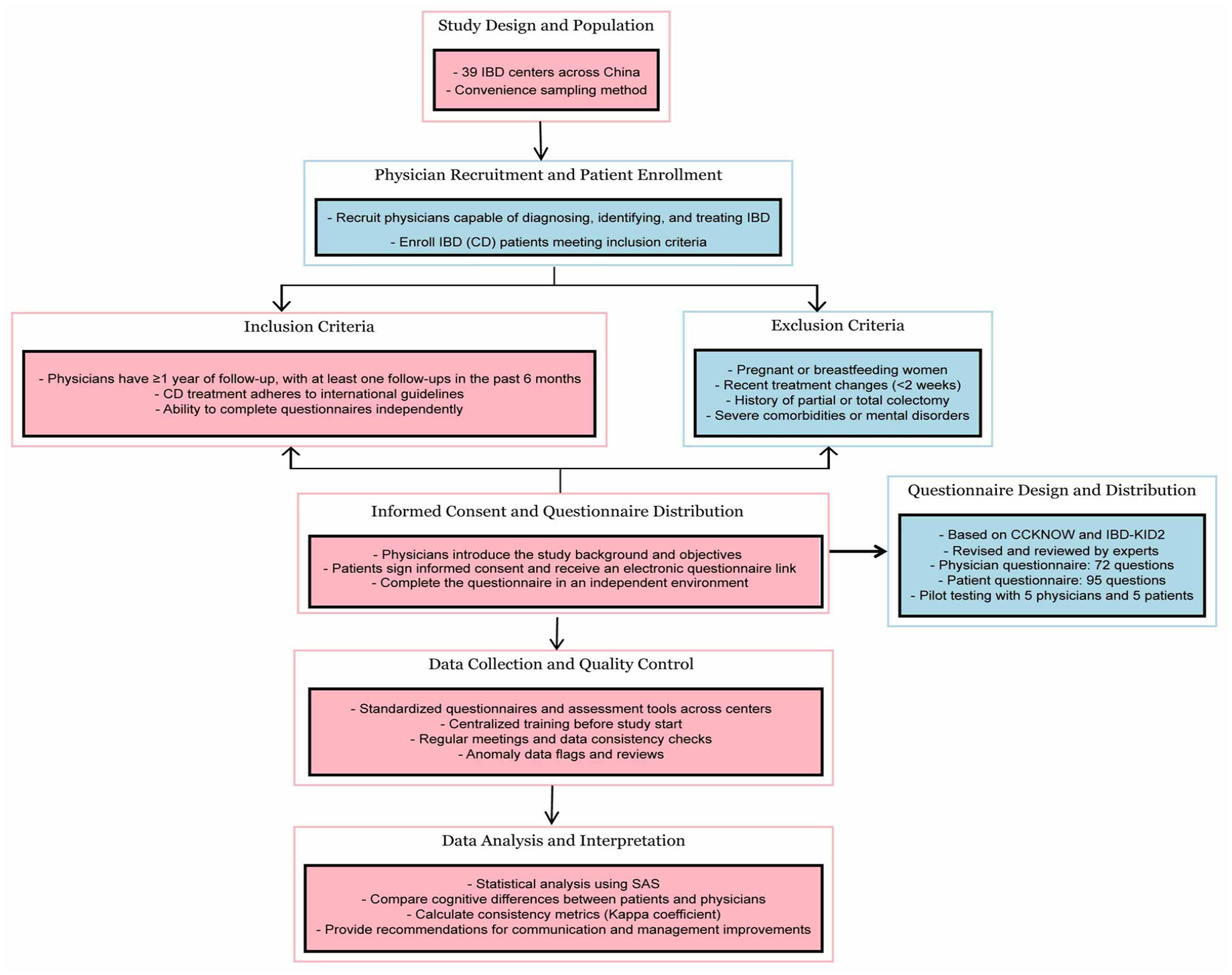
Research flowchart.
The study was reviewed and approved by the Ethics Committee of Xijing Hospital affiliated to the Fourth Military Medical University (Xi’an, China; approval number ChiCTR2000034872) and the ethics committees of all other participating sites. The research was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Informed consent was obtained from all participating doctors and patients through signed consent forms. We ensured that any details that could potentially reveal the identities of the research subjects were omitted. This study conforms to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) statement. 17
Questionnaire design and implementation
The questionnaires used in this study were based on the Crohn and Ulcerative Colitis Knowledge Score (CCKNOW) 18 and Inflammatory Bowel Disease Knowledge Inventory 2 (IBD-KID2). 19 They were modified by the head of the IBD Research Group of the Chinese Medical Association and reviewed by 10 IBD experts. The physician questionnaire (Supplemental Appendix 1) contains 72 items, covering 4 dimensions: basic information, disease symptom knowledge, medication treatment, and doctor–patient relationship. The patient questionnaire (Supplemental Appendix 2) consists of 95 items addressing 5 dimensions: basic information, disease symptom knowledge, medication treatment, and doctor–patient relationships. To comprehensively assess the overall QoL of patients with IBD, this study also employed the SF-36 Health Survey, which encompasses various dimensions, including physical, mental, social, and environmental health.
This study strictly adhered to the design process of “pilot testing, optimization, and formal study.” All participants in the formal study completed the final version of the questionnaire, which was optimized through pilot testing. We added additional information to the basic details of the patient and physician questionnaires, such as initials and contact numbers, to facilitate better follow-up and data tracking. These additions did not alter the core assessment questions of the questionnaire, and therefore did not impact its validity as a validation tool. For data collection, a pilot test was conducted with five doctors and five patients before the official launch, modifying the questionnaires based on their feedback. After their outpatient visits, patients immediately filled out the questionnaires in a private room at the hospital to ensure data independence and accuracy and minimize external interference. Patients could request assistance from the hospital staff when needed to ensure smooth completion of the questionnaires. The doctors completed the corresponding questionnaires based on their clinical observations after the patient’s visit. All questionnaires were designed using standardized and easily understandable language and underwent multiple rounds of pilot testing to ensure consistent comprehension. The questionnaires were distributed via an electronic system that tracked completion time and automatically sent reminders.
To ensure consistency, all participating research centers used standardized questionnaires and evaluation tools. Prior to data collection, all participating doctors and researchers underwent centralized training, and consistency was assessed through simulated case tests. During the study, the research team monitored progress through regular meetings, online supervision, and data consistency checks (including calculation of the Kappa coefficient) to ensure the consistency of results across centers and doctors. The electronic system also featured an outlier detection function to flag potential biases in physician assessments and analyzed the completion times to identify abnormal patterns. Finally, some patients provided feedback after completing the questionnaires, which helped further optimize the clarity and acceptability of the questionnaires.
Classification and assessment of CD activity
Patients with CD were classified using the Montreal classification system. Age at onset was categorized into A1 (⩽16 years), A2 (17–40 years), and A3 (>40 years). Disease location was defined as L1 (ileal disease confined to the small intestine), L2 (colonic disease limited to the colon), L3 (ileocolonic disease involving both the small intestine and colon), or L4 (upper gastrointestinal involvement). According to the recommendations of the European Crohn’s and Colitis Organisation (ECCO), disease activity in CD is defined using the Crohn’s Disease Activity Index (CDAI) and the Simple Endoscopic Score for CD (SES-CD). CD remission was defined as a CDAI score <150, whereas a CDAI score >150 indicates active disease. 19 When the SES-CD score is 0–2, it is considered endoscopic remission, and a score ⩾3 is considered endoscopic activity. 20
Statistical analysis
All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and RStudio 4.3.2 (RStudio, Boston, MA, USA). Continuous data were presented as mean ± standard deviation. Categorical data were described as frequencies (percentages). Agreement is a measure of the difference between physicians’ reports on patient signs or symptoms and self-reports of the same parameters. Considering the impact of the opportunity agreement rate on the results, we used the Cohen Kappa (κ) coefficient to describe agreement (0.2 = very low agreement, 0.2–0.4 = low, 0.4–0.6 = moderate, 0.6–0.8 = high, and 0.8–1 = perfect).
Results
Demographic characteristics
A total of 834 patients with CD from 24 provinces and cities in China participated in the study, with 601 patients completing the survey. Among the completers, 192 were outpatients and 409 were inpatients (Table 1). Among them, 392 (65.22%) were male. Urban residents accounted for the highest proportion, reaching 65.6%. Most (78.70%) patients were 17–40 years old, and 28 (4.66%) were under the age of 16 years. More than 70% of patients attained a higher education level (bachelor’s degree or higher). Patients were mainly middle-income and low-income; 77.20% had an income of <6000 RMB. Only 2% of the patients with CD had relatives who also had CD. Among these, 0.50% were immediate family members (parents or children). The most common CD type was L1 (50.90%), followed by L3 (40.60%). Among the patients, 37.10% were in the active phase, of whom >50% had moderate or severe disease. Among the patients, 4.49% had extraintestinal manifestations, with erythematous nodules and ankylosing spondylitis accounting for the highest proportions. A total of 29.95% and 35.77% of patients had undergone CD-related abdominal and perianal surgery, respectively.
Demographic and baseline characteristics of patients with CD.

CD, Crohn’s disease; L1, terminal ileum; L2, colon; L3, ileum colon; L4, upper gastrointestinal tract.
A total of 181 physicians from class A tertiary hospitals completed the survey, with each IBD specialist corresponding to 3–5 patients (Table 2). Among the physicians, 48.62% held the title of Deputy Chief Physician or above. The majority (95.58%) specialized in IBD research, and over 40.33% had 2–5 years of independent clinical experience in diagnosing and treating CD. Detailed demographic and professional characteristics of patients and physicians are summarized in Tables 1 and 2, respectively.
Demographic and baseline characteristics of CD physicians.
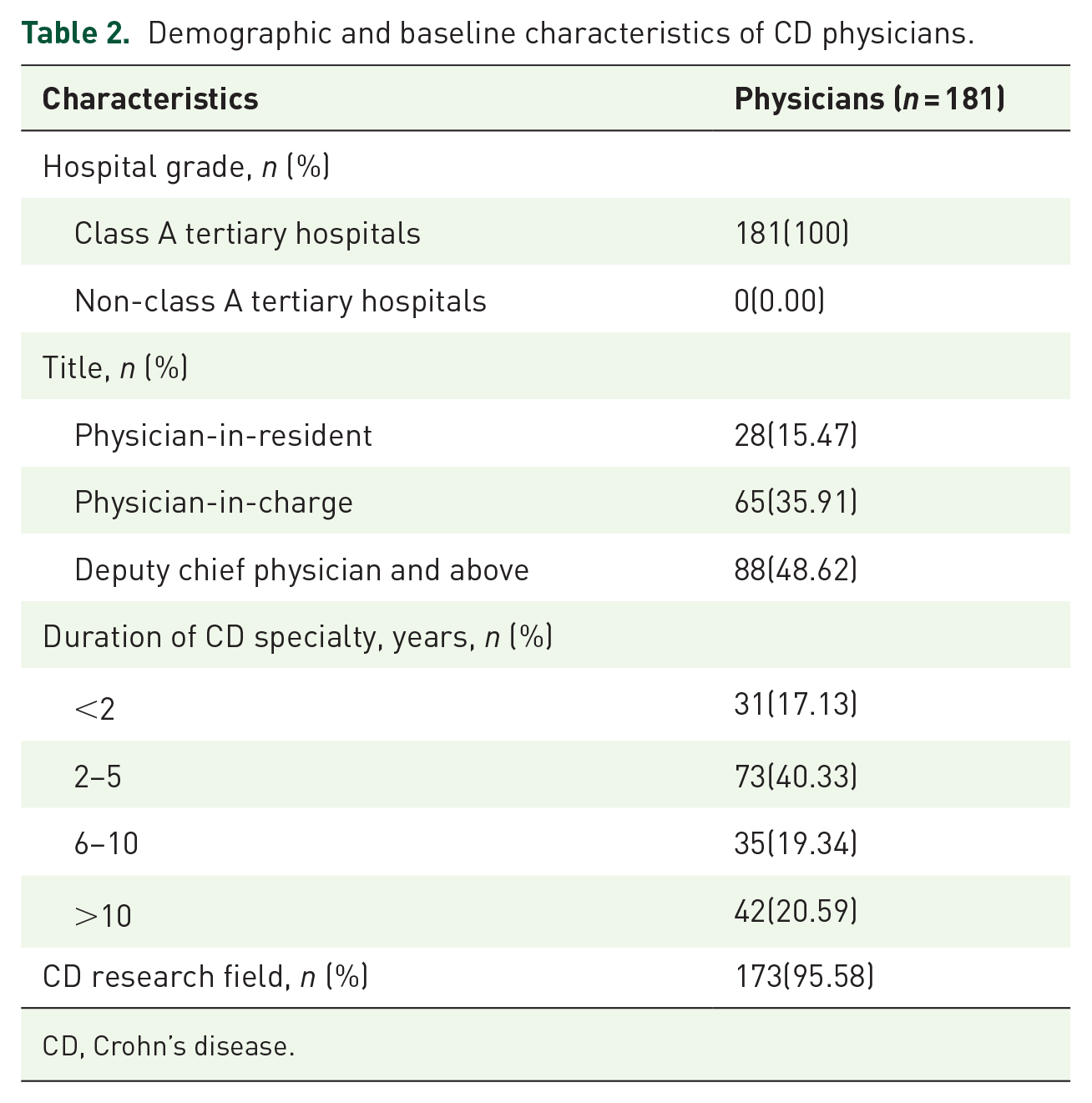
CD, Crohn’s disease.
Disease awareness
Most physicians identified abdominal pain (42.54%) as the primary concern, followed by the need for frequent medical visits (23.76%). However, patients reported that the need for frequent visits was the most pressing issue (30.95%), followed by diarrhea (28%), abdominal pain (25.29%), and fatigue (6.30%; Figure 2). Through a stratified analysis of doctors (Supplemental Table 1), we found that deputy chief physicians and above paid significantly more attention to diarrhea than attending physicians (22.73% vs 12.31%, κ = 0.093) and resident physicians (22.73% vs 10.71%, κ = 0.067). On the other hand, resident physicians (28.57% vs 17.05%, κ = 0.123) and attending physicians (30.77% vs 17.05%, κ = 0.146) were more focused on the issue of frequent patient visits compared to deputy chief physicians and above. Further analysis of patient visit types (Supplemental Table 2) revealed that inpatients were the most concerned about the issue of repeated visits (35.94%), whereas outpatients primarily focused on diarrhea (28.85%). In addition, physicians reported that 42.54% of patients had complete or major symptom control, while only 32.61% of patients agreed, κ = 0.150 (Supplemental Table 3).

The cognitive difference between physicians and Crohn’s disease patients on disease disturbance.
Significant differences were observed between patients with CD and physicians in defining disease remission. While 62.90% of patients self-reported being in remission (outpatients: 63.33%; inpatients: 61.98%), physicians’ clinical assessments indicated a lower remission rate (57.46%, κ = 0.035, Supplemental Table 3). Notably, as shown in Supplemental Table 1, deputy chief physicians and above managed a higher proportion of active-phase patients than attending and resident physicians (52.27% vs 26.15% and 42.86%, respectively). Of the outpatients, 70.90% equated remission and achieved a normal QoL, whereas 72.92% of the inpatients emphasized satisfaction with the treatment outcomes (Supplemental Table 2). In addition, physicians generally have a higher understanding of the conditions necessary for disease remission than patients. These included symptom relief, endoscopic remission, patient satisfaction, improved inflammatory activity, and corticosteroid-free remission (Figure 3).

Physicians’ and Crohn’s disease patients’ understanding of remission conditions.
Treatment target
We found that the most important treatment goal for patients with CD (both outpatient and inpatient) was to improve the QoL (29.78%), while physicians prioritized endoscopic mucosal healing (34.25%; Supplemental Tables 2 and 3). Stratified analysis of the physicians’ responses revealed that both residents and attending physicians considered endoscopic mucosal healing (57.14% and 40.00%, respectively) the primary treatment goal, whereas deputy chief physicians and above placed greater emphasis on achieving long-term disease remission (44.32%; Supplemental Table 1). Among the patients with CD, 86.36% expressed satisfaction with their treatment plans, with outpatient satisfaction being slightly higher (87.04%) than inpatient satisfaction (84.90%; Supplemental Tables 2 and 3).
Biologics were the most commonly used medications in CD patients (63.89%), followed by immunomodulators (47.09%) and enteral nutrition formulations (43.09%). Fewer patients were administered antibiotics (4.99%) or corticosteroids (6.99%; Table 1). Notably, enteral nutrition formulations were predominantly used in combination with other medications to enhance treatment effectiveness. However, physicians overestimated the patients’ understanding of biologics. While 71.55% of patients reported understanding biologics, physicians believed that this figure was as high as 93.37% (κ = 0.117). Inpatients had a slightly better understanding of biologics (73.96%) than outpatients (70.42%). Furthermore, 32.45% of patients were unaware of the safety concerns associated with biologics, while physicians believed that only 8.84% of patients lacked such awareness (κ = 0.135). In this case, inpatients also showed a better understanding (71.88%) of biological safety than outpatients (65.53%). Concerns regarding the side effects of biologics (23.79% of patients vs 17.13% of physicians) were significant factors affecting patient adherence to long-term treatment. Both outpatients and inpatients expressed particular concerns about the increased risk of malignancy/lymphoma, while physicians, including residents, attending physicians, deputy chief physicians, and above, were more concerned about the risk of severe infections (Supplemental Tables 1–3). Furthermore, 60% of the physicians reported that their patients experienced symptom deterioration during maintenance therapy with biologics within a year (Supplemental Figure 1). Both outpatients and inpatients agreed that frequent medical visits were the most unsatisfactory aspect of their treatment, with a higher percentage of inpatients expressing dissatisfaction (54.69% vs 39.85%). By contrast, the physicians (including residents, attending physicians, deputy chief physicians, and above) believed that the inability to achieve long-term disease remission was the primary source of dissatisfaction (Supplemental Tables 1 and 2).
Diagnosis and treatment mode
Diagnostic delays were widespread. Nearly 50% of the patients required more than two visits during the diagnostic process before receiving a confirmed diagnosis, and 12.80% required seven or more visits (Supplemental Figure 2(A)). A total of 93.30% of the patients had been diagnosed for more than 1 year, while 96 (20%) had more than 1 year since the first symptom (Supplemental Figure 2(B)).
Based on the feedback from both doctors and patients, we analyzed the primary concerns regarding the current treatment model. Both physicians (98.34%) and patients (99.33%) considered that the most troublesome problem under the current treatment model was “frequent visits to the hospitals, which affects the work/study of patients” (Supplemental Table 3). In addition, 64.06% of patients with CD had regular follow-ups, and 29.12% only visited their physicians when they felt uncomfortable or had a relapse (Supplemental Table 3).
According to the CD treatment program, the majority of outpatients and inpatients expected follow-up once every 6 months or more, while 46.96% of physicians hoped for a follow-up frequency not below once every 2 months. Moreover, 17.68% of physicians wanted to see their patients every month (Figure 4). In addition, 14.92% of the physicians and 60.40% of the patients reported that the initial consultation lasted for more than 30 min. Stratified analysis according to physician rank indicated that deputy chief physicians and above primarily spent 16–30 min during the initial consultation, which was longer than that of residents and attending physicians. However, the consultation time for residents and attending physicians was mostly within the 5–15 min range (Supplemental Table 1).
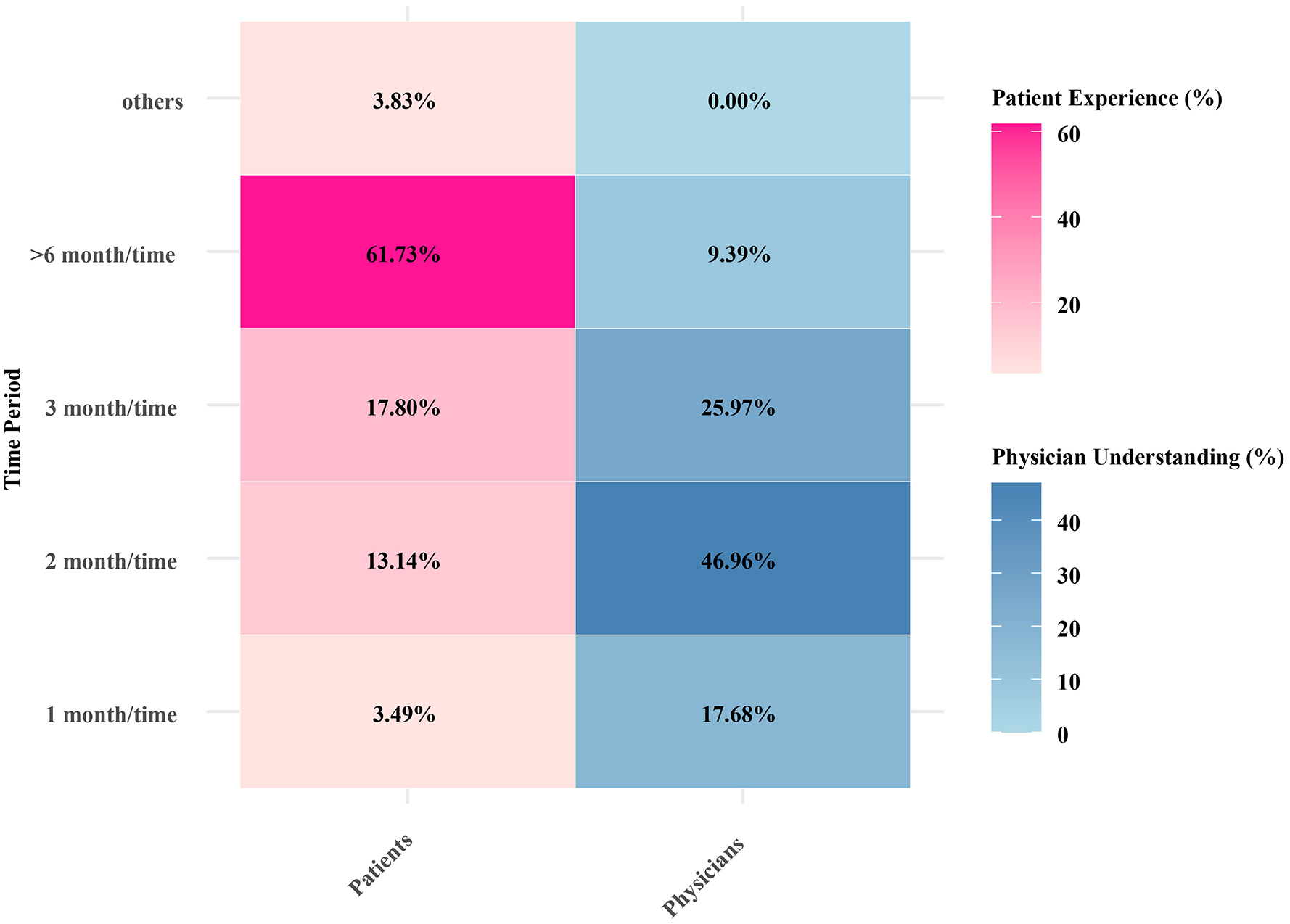
Physicians’ and Crohn’s disease patients’ expected follow-up frequency during treatment.
The perceptions of both physicians and patients regarding the treatment decision-making model differed significantly. In total, 41.99% of the physicians and 60.07% of patients believed that patients could make self-determined treatment decisions with the assistance of physicians, which included explaining the treatment options and providing recommendations. In addition, physicians were more inclined than patients to emphasize the concept of “having an equal partnership and making decisions together” (49.17% vs 14.31%, κ = 0.353; Supplemental Table 3).
Disease burden and QoL
A total of 43.92% of the patients believed that CD had an impact on QoL, and physicians (34.81%) underestimated the extent. A total of 89.18% of patients and 93.37% of physicians believed CD was disruptive to life (Supplemental Table 3). Most physicians (60.20%) and patients (37.90%) were able to accept that treatment cost 10%–30% of their household income. Notably, 21.30% of the patients were willing to pay more than 50% of their household income for CD treatment (Supplemental Table 3). However, we found that treatment costs were the most important factor affecting adherence in both outpatients and inpatients (Supplemental Table 2). Resident physicians reported higher levels of financial stress among patients (32.14% vs 23.08% vs 19.32%), while deputy chief physicians and attending physicians placed more emphasis on treatment outcomes (51.14% vs 38.46% vs 28.57%) and underestimated the impact of costs on patient adherence (Supplemental Table 1).
Discussion
This study is the first large-scale survey to systematically compare the cognitive differences between CD patients and clinicians across key dimensions such as disease burden perception, treatment control, medication use, treatment goal setting, QoL, treatment adherence, follow-up frequency, and doctor–patient relationships. This study found significant cognitive biases between patients and doctors, particularly in areas such as focusing on disease symptoms, patients’ understanding of biologic agents, and expectations regarding follow-up frequency. A stratified analysis based on physician title (deputy chief physician and above, attending physician, and resident) and patient visit status (outpatient vs inpatient) further revealed cognitive differences between doctors of different titles and patients of different types. These findings highlight the importance of improving doctor–patient communication and suggest that clinicians should pay greater attention to patients’ actual needs and expectations to better achieve patient-centered treatment goals in clinical practice.
Our study found significant differences between patients with CD and physicians regarding disease management priorities. Physicians typically focus on abdominal pain, whereas patients place greater emphasis on the frequency of medical visits. This result aligns with international research by Ghosh and Mitchell, 5 indicating that physicians’ assessments often fail to fully capture patients’ subjective experiences, leading to gaps in disease management strategies. Through a stratified analysis of doctors, it was found that deputy chief physicians and above paid significantly more attention to diarrhea than attending physicians and residents. This may be because deputy chief physicians and above are typically responsible for handling more complex cases, which require them to focus more on diarrhea symptoms. By contrast, residents and attending physicians were more concerned about the issue of frequent patient visits, which is closely related to their daily management of patients, allowing them to directly experience the physical and mental burden caused by patients’ frequent visits. Further analysis of the types of patient visits revealed that inpatients generally considered repeated visits to be their biggest concern because of the complexity of their conditions. By contrast, outpatients focus more on the management of diarrhea symptoms, with diarrhea being the main issue. In addition, we observed discrepancies between patients and physicians regarding their understanding of disease remission. For example, although the proportions were similar (patients 52.41% vs physicians 51.93%), statistical analysis revealed that patients were more likely to equate symptom remission with a return to normal QoL, whereas physicians had a slightly lower degree of agreement with this definition. This suggests that patients may prioritize immediate symptom relief and overlook broader disease management goals. 20 By contrast, physicians typically have a more comprehensive understanding of disease remission, including symptom relief, endoscopic remission, patient satisfaction, reduced inflammation, and steroid-free remission. This difference may stem from physicians’ professional knowledge and clinical experience, which enables them to recognize more complex disease management indicators. It is noteworthy that surgical intervention plays a crucial role in the disease management of patients with CD, influencing not only short-term symptom relief but also having a profound impact on long-term disease management strategies. The data show that 29.95% of patients with CD undergo abdominal surgery, while 35.77% undergo perianal surgery. These surgeries are generally performed in patients with more severe or complex conditions, who often prioritize rapid symptom relief and improved QoL over long-term disease remission. This may partly explain the cognitive differences between patients and physicians regarding disease remission.
Interestingly, this study shows significant differences in the treatment goals for CD; patients prioritize QoL, whereas doctors’ goals exhibit a hierarchical pattern based on their experience. Residents and attending physicians focused on endoscopic mucosal healing, whereas deputy chief physicians and above were more concerned with long-term disease remission. These differences arise from the fact that patients troubled by symptoms and side effects of treatment place more importance on their current QoL. Younger doctors, following the guidelines, emphasize mucosal healing as an objective indicator, particularly during the acute phase, to prevent complications. By contrast, experienced doctors advocate the concept of deep remission with a comprehensive approach that includes mucosal repair, symptom control, nutritional improvement, and reduction of steroid dependence. This consensus marks a significant shift in IBD management from merely controlling symptoms to achieving long-term disease remission. 3 Biologics have been widely adopted in clinical practice owing to their significant efficacy. 21 However, our study found that patient awareness of the safety and side effects of biologics was significantly lower than physicians’ expectations. Data showed that 32.40% of the patients reported an insufficient understanding of biologic safety, whereas physicians estimated this proportion to be only 8.80%. In addition, 23.79% of patients expressed high concern about the potential side effects of biologics (such as the risk of malignancies), whereas physicians estimated this figure to be merely 17.13%. This discrepancy may be attributed to patients’ inadequate understanding of biological safety and excessive concern about side effects. On the other hand, physicians tend to assess treatment risks based on their professional knowledge but may overlook patients’ subjective feelings about treatment side effects, further exacerbating communication barriers between physicians and patients. The study results indicated that inpatients have a significantly higher awareness of biologics and their safety than outpatients, which is closely related to differences in the clinical setting. Owing to the complexity of their conditions, inpatients have a stronger need for biologics and more time for doctor–patient communication, which facilitates systematic treatment education. By contrast, outpatients, with limited consultation time and milder conditions or not meeting the criteria for biologic treatment, have more restricted access to information. It is noteworthy that there is a significant difference in the dimensions of biological risk concerns between patients and clinical doctors. Both inpatients and outpatients are more worried about the risks of malignancies/lymphomas, whereas clinical doctors are more concerned about the risks of severe infections. This cognitive difference may stem from two aspects: on one hand, patients have a stronger instinctive fear of cancer, and the excessive portrayal of cancer in the media exacerbates their concerns; on the other hand, clinicians are more focused on infection risks, which have a higher actual incidence, reflecting the difference between evidence-based medicine and public perceptions. Moreover, data indicate that, compared to American patients, 20 Chinese patients have a higher usage rate of biologics (63.89% vs 50%), which may be attributed to the rapid development of healthcare resources and increased accessibility to biologics in China in recent years. However, Chinese patients still need to improve their understanding of the long-term safety and efficacy of biologics, which may be related to insufficient patient education and inadequate communication strategies among physicians.
In our study, we found that patients with CD frequently experienced delayed diagnosis. Nearly 50% of the patients required more than two visits before receiving a confirmed diagnosis, and 12.80% required seven or more visits. This finding is consistent with those of previous studies, indicating that the diagnostic process for CD is often complex and time-consuming, which may lead to disease progression and a decline in QoL. 20 Our data also revealed that 93.30% of the patients had been diagnosed for over a year, and 96.20% had experienced symptoms for over a year before diagnosis, emphasizing the importance of early diagnosis and intervention. In addition, both physicians and patients agreed that frequent hospital visits were the most burdensome aspect of the current treatment models, significantly affecting patients’ work and studies. Research has shown that the frequency of hospital visits is closely linked to patients’ QoL, with more frequent visits potentially increasing the psychological burden. 22 Graff et al. 23 highlighted that, even when the disease is in remission, its impact on QoL persists. However, physicians tend to focus more on objective and scientific monitoring indicators, often underestimating the impact of CD on the QoL. 6 Furthermore, patients’ expectations for follow-up frequency were generally lower than physicians’ recommendations; 61.73% of patients preferred follow-ups every 6 months, whereas 46.96% of physicians recommended follow-ups at least every 2 months. This discrepancy may stem from patients’ desire to reduce the frequency of follow-ups to lessen their dependence on healthcare resources and avoid excessive worry, while physicians tend to recommend more frequent follow-ups to detect potential health issues early and prevent disease progression or complications.
It is noteworthy that, although patients are willing to invest more financially in treatment, the cost of treatment remains a significant factor affecting patient adherence. In fact, 21.30% of patients were willing to allocate more than 50% of their household income to CD treatment, a proportion significantly higher than the physicians had anticipated. This finding is consistent with international studies suggesting that patients, when confronted with an illness, may be willing to take on a substantial financial burden, reflecting both their expectations of treatment outcomes and their pursuit of a better QoL. 5 Therefore, when developing treatment plans, physicians should consider the patients’ financial capacity and, whenever possible, provide additional financial support and resource information to help patients better manage their condition.
The importance of the physician–patient relationship, patient education, and patient involvement in treatment decisions has been increasingly recognized in CD.24,25 However, in our study, patients’ awareness of “shared decision-making” seemed limited. Patients rely heavily on their physicians to make treatment decisions. Recently, the ECCO published a list of recommendations for physician–patient co-decision-making, including the incorporation of clinical features, markers of disease activity, balance of benefits and risks of treatment, and patient preferences. 26 The physician has the responsibility to inform patients and give them advice, whereas the actual decisions on how to act on this information are made jointly by the patient and physician, based on evidence-based medicine and the patient’s values and needs. 27
Our study has some limitations. First, the analysis of physicians’ and patients’ perspectives was limited by different geographic regions or practice settings. Regarding the selection of gastroenterologists, the sample may have been biased in favor of highly specialized professionals. However, this bias could be considered as an added value because they are professionals with in-depth knowledge of the disease. In addition, this study was primarily based on quantitative methods and did not systematically collect patients’ free-text responses. Consequently, there are limitations in capturing the depth and complexity of patients’ individualized experiences. Future research should incorporate open-ended questions to further explore patients’ subjective perceptions of the diagnosis and treatment process of CD, thereby complementing the current findings. Finally, the study was based in China, and cultural factors may have influenced both physicians’ and patients’ perspectives on disease management, potentially limiting the applicability of the findings to other populations. Future research should further explore cross-cultural comparisons by examining the disease management perceptions of physicians and patients with CD in different countries, thereby providing deeper insights into the impact of cultural backgrounds on CD management strategies.
Conclusion
In conclusion, this study provides valuable insights for both patients with CD and doctors, revealing key differences in disease awareness, treatment control, medication use, treatment goals, QoL, treatment adherence, follow-up frequency, and doctor–patient relationships. Further analysis indicated that there were significant differences in CD management between doctors of different professional titles and patients with different visit statuses. Therefore, Chinese CD doctors should emphasize patients’ subjective experiences and mental health. Simultaneously, it is essential to enhance patient education regarding the emerging CD treatment options, including novel biologics and small-molecule drugs. Future research should focus on improving communication between doctors and patients to help patients play a more active role in disease management and treatment decision-making.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251351515 – Supplemental material for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study
Supplemental material, sj-docx-1-tag-10.1177_17562848251351515 for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xiaoqi Zhang, Minhu Chen, Qian Cao, Yihong Fan, Fang Xiao, Yufang Wang, Liangru Zhu, Hong Guo, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251351515 – Supplemental material for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study
Supplemental material, sj-docx-2-tag-10.1177_17562848251351515 for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xiaoqi Zhang, Minhu Chen, Qian Cao, Yihong Fan, Fang Xiao, Yufang Wang, Liangru Zhu, Hong Guo, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-3-tag-10.1177_17562848251351515 – Supplemental material for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study
Supplemental material, sj-docx-3-tag-10.1177_17562848251351515 for Different perceptions on the diagnosis and treatment of Crohn’s disease between patients and gastroenterologists: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xiaoqi Zhang, Minhu Chen, Qian Cao, Yihong Fan, Fang Xiao, Yufang Wang, Liangru Zhu, Hong Guo, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors are grateful to the CHASE-IBD and MIMIC IBD team for support in this research project. We thank Professors Zhang Yujie, Masai, Zhao Xiaoxing, and Tang Bihua for data collection and quality control, and especially Professor Xi Peng for strategic assistance.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.