
Abstract
Background:
Discrepancies between symptoms and endoscopy exist in patients with ulcerative colitis (UC). Most studies focused on patient-reported outcomes-2 rather than their overall perception of disease activity.
Objectives:
The objectives were to assess the concordance between the patient global assessment (PtGA) and the endoscopic evaluation, to analyse the factors associated with agreement and to describe the concordance between the patient’s and the physician’s perception of UC activity.
Design:
Prospective, observational study.
Methods:
Patients with UC were consecutively included at the time of flexible sigmoidoscopy. The concordance between the Mayo endoscopic subscore (MES) and the PtGA was evaluated. The factors related to concordance were investigated, including the inflammatory bowel disease (IBD)-Disk items that were completed by all patients.
Results:
Out of 104 analysable patients, 32.7% demonstrated complete alignment with the MES. The more the disease was objectively active, the more the patients were concordant, as reflected by the statistically significant differences between concordant and discordant patients in the median (interquartile range) MES (2 (1–2) vs 1 (0–2), respectively (p = 0.002)), Ulcerative Colitis Endoscopic Index of Severity (3 (2–5) vs 1 (0–3), respectively (p = 0.001)) and physician global assessment (whether on a qualitative scale as part of the Mayo score (p = 0.003) or on a 10 cm-visual analogue scale: (4 (1–6) vs 1 (0–3), respectively (p < 0.001)). Over two-thirds of discordant patients perceived their disease as more severe than the endoscopy suggested. While stool frequency did not differ between concordant and discordant patients (p = 0.093), rectal bleeding (p = 0.002) – predictably – and more interestingly, abdominal pain (p = 0.006) and bowel urgency (p = 0.006), emerged as symptoms strongly associated with improved concordance between patient perception and endoscopic evaluation.
Conclusion:
Discrepancies between patient-reported disease activity and endoscopy are prevalent in UC. In addition to rectal bleeding, abdominal pain and bowel urgency may be more accurate to reflect clinical disease activity than stool frequency.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease (IBD) responsible for digestive symptoms, mainly diarrhoea and rectal bleeding, but also abdominal pain and bowel urgency, which alter the quality of life, cause fatigue and may affect the psychological, family and socio-professional dimensions of patients’ lives, even in the absence of active inflammation. 1
Over the last decade, the therapeutic paradigm has dramatically changed. While in the past the therapeutic strategy was based solely on symptoms, the STRIDE international consensus, published in 2015, recommended both clinical and endoscopic remission (Mayo endoscopic subscore (MES) 0 or 1) as treatment goals. 2 In the STRIDE-II consensus, updated in 2021, clinical remission and endoscopic healing are still the ultimate goal to reach in patients with UC, but with more stringent definitions. 3 Clinical remission is now defined as the resolution of rectal bleeding and the normalization of bowel movement (patient-reported outcomes (PRO)-2 = 0). Endoscopic remission is defined as complete healing of mucosal lesions, namely, an MES of 0. Moreover, the STRIDE-II consensus added the restoration of quality of life and absence of disability as long-term targets. 3 This reflects the importance attached to the patient’s feelings regarding the impact of the disease on his/her life (PRO-1).
But at present, endoscopy is still considered as the gold standard to assess disease activity and to guide therapeutic decisions in UC. 3 Indeed, even if clinical disease activity correlates much better with endoscopy in UC than in Crohn’s disease (CD), 4 there may still exist some discrepancies between symptoms and the aspect of the mucosa. This may have an impact on follow-up and compliance with treatment, on patient satisfaction and on the doctor–patient relationship. Indeed, some patients may feel that they are over-treated or, conversely, that their symptoms are not taken into account in treatment decisions. Improving communication between patients and doctors and helping the physicians to understand the patients’ perspective are essential for the management of their diseases. 5
Several studies have already explored the agreement between PRO-2 and endoscopy. All of them demonstrated the concordance between endoscopic remission and the absence of rectal bleeding, while stool frequency may still be increased due to sequelae of parietal changes.6 –8 However, data are scarce regarding the concordance between the mucosal aspect as assessed by endoscopy and the patient’s perception of disease activity, a more global outcome than PRO-2 alone.
The main objective of the RectEVA (‘RECTocolite hémorragique : EVAluation de la concordance entre l’endoscopie et la perception du degré d’activité par le patient’) study was to assess the concordance between the patient’s perception of UC activity and the endoscopic disease assessment. The secondary objectives were to analyse the factors associated with poorer agreement and to describe the concordance between the patient’s and the physician’s perception of UC activity.
Patients and methods
Study design and population
The RectEVA study was a multicentre prospective cohort study conducted in two French University Hospitals (tertiary care centres) and in a private hospital (secondary care centre) from June 2020 to February 2021.
Adult patients (>18 years) were consecutively included in the study if they met the following criteria: affiliated to a healthcare system, with a diagnosis of UC for more than 6 months, with an indication for flexible sigmoidoscopy as part of the standard of care, regardless of previous, ongoing or concomitant treatments. Non-inclusion criteria were as follows: patients who did not speak and/or read French or who had comprehension difficulties according to the investigator’s assessment, patients under legal protection and patients who had undergone a total coloproctectomy with ileo-anal anastomosis.
Patients were included in the study at the time of the lower endoscopy. Six senior endoscopists participated in the study, all familiar with IBD endoscopic scoring systems.
Ethics
Eligible patients were proposed to participate in the study when scheduling the endoscopy. This research was conducted in accordance with French legislation on research involving human subjects (known as the ‘Jardé Law’). As this study falls under Category 3 (minimal-risk, non-interventional research), after they had been given written and oral information, oral non-opposition consent was obtained from all participants and notified in the patient’s clinical record, which is compliant with French regulatory requirements for this type of research. The study protocol was approved by the local Research Ethics Committee (Groupe Nantais d’Ethique dans le Domaine de la Santé (GNEDS)) on 21 February 2020.
Patient-reported disease activity
In the waiting room before the endoscopy was performed, patients rated their disease activity on a 4-point semi-quantitative ordinal scale similar to that included in the total Mayo score: inactive, mildly active, moderately active, severely active. They also rated it on a visual analogue scale (VAS) from 0 (no active disease) to 10 (most severe disease) (patient global assessment (PtGA)). Patients were asked to complete this assessment based on the last 7 days before any bowel preparation was performed.
At the same time, patients also completed the IBD-Disk questionnaire in its French version that has been already validated. 9 This questionnaire rates the global impact of the disease on the patient’s life using 10 criteria based on their experience over the previous 7 days: abdominal pain, regulating defecation, social life, professional life, sleep, energy, mental health, body image, sexual life, joint pain. Each of these criteria is rated on a scale ranging from 0 to 10 (0 corresponding to the lowest impact and 10 to the highest impact). 10
Clinical data collection and physician global assessment
Clinical data were collected at the time of lower endoscopy: age, gender, disease duration, disease location (E1, E2 or E3 according to Montreal classification), indication of endoscopy (disease flare i.e. recurrence of UC-related symptoms before change of therapy, vs control of mucosal healing i.e. assessment of response to therapy between 3 and 6 months as recommended by the STRIDE guidelines 2 whether the patient had achieved complete clinical remission or simply clinical response), extra-intestinal manifestations, IBD-related ongoing treatments (none, 5-aminosalicylic acid (5-ASA), corticosteroids, immunosuppressants, anti-tumour necrosis factor (anti-TNF) alpha agents, vedolizumab, ustekinumab, tofacitinib).
After the lower endoscopy had been performed, blind to the patient-reported disease activity, physicians rated their own perception of disease activity using the 4-point semi-quantitative ordinal scale included in the total Mayo score: inactive, mildly active, moderately active, severely active. In the same way as patients did, physicians also rated disease activity on a VAS from 0 (no active disease) to 10 (most severe disease) (physician global assessment (PGA)).
The total Mayo score was calculated using each of its subscores (including PGA, PRO-2 and the MES). The Ulcerative Colitis Endoscopic Index of Severity (UCEIS) and the Nancy histological index were also collected. The highest Nancy index was considered in patients who had two different scores depending on the location of the biopsies.
Study outcomes
The primary outcome was the concordance between the MES and the PtGA as assessed by the 4-point scale. Clinical factors associated with agreement were evaluated.
The secondary outcomes were the concordance between the UCEIS and the PtGA as assessed by the 4-point scale, and between the PtGA and the PGA on both scales (ordinal scale and VAS).
Statistical analysis
The number of 100 patients to be included was arbitrarily chosen because no prior data were available for the calculation of the sample size due to the lack of studies comparing the patient’s overall perception of disease activity and endoscopic activity. This sample size was sufficient to carry out parametric analyses of the distributions.
Clinical and socio-demographic characteristics of the patients are described using raw counts and percentages for categorical variables, and means and standard deviations (SDs) for continuous variables, or median and interquartile range (IQR) for those of which distribution did not follow a normal distribution.
Comparative analyses between variables were assessed by Student’s t test, the Chi-square test of homogeneity, the Mann–Whitney–Wilcoxon test and Fisher’s exact test, respecting the conditions of application of these tests. The correlation between the PtGA and the PGA as assessed by the VAS was assessed using the Spearman’s correlation test. Type I error risk was set to 5%.
The number of missing data is systematically presented. Data were analysed using R software version 4.0.4 (R Core Team 2021).
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 11
Results
Description of the study population
One hundred and six patients were included in the RectEVA study from June 2020 to February 2021 (Figure 1). Clinical characteristics at baseline are described in Table 1. Forty-four patients (41.5%) were followed in a tertiary referral centre and 62 patients (58.5%) were followed in a private clinic (secondary care centre). The endoscopy was performed to assess mucosal healing in 66 patients (62.3%) and in case of a flare in 40 patients (37.7%).
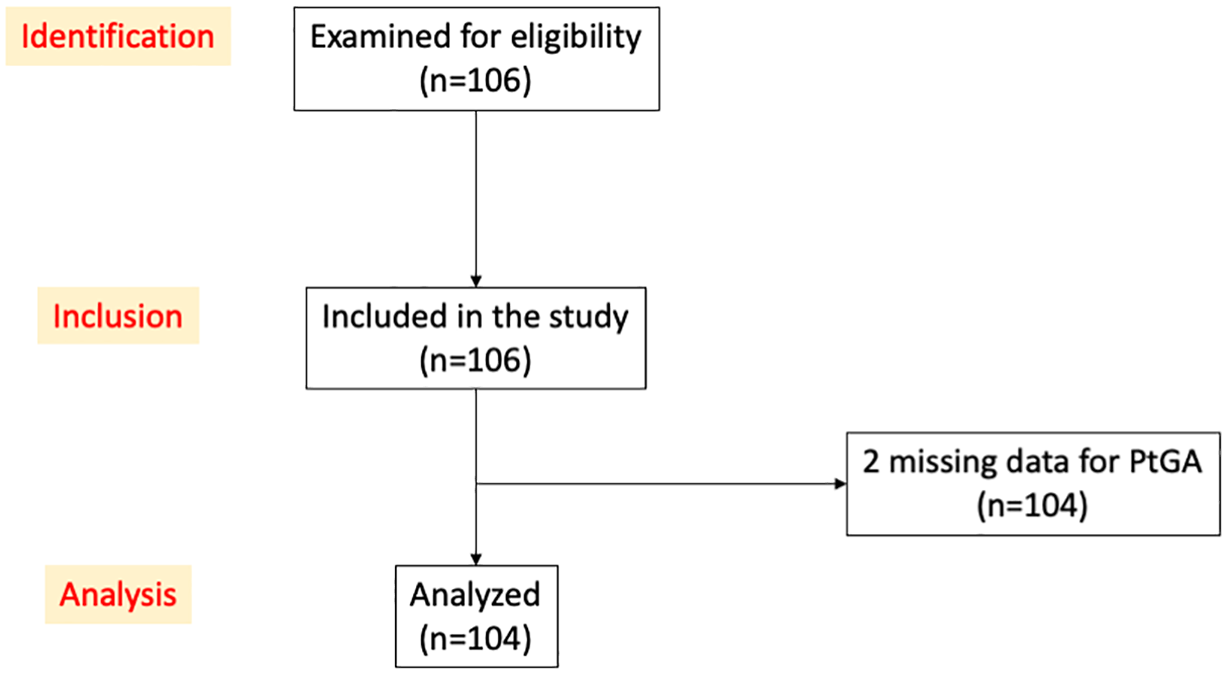
STROBE flow diagram.
Clinical characteristics of the study population (n = 106 patients).

Patients could have more than one treatment.
5-ASA, 5-aminosalicylic acid; EIM, extra-intestinal manifestation; IBD, inflammatory bowel disease; SD, standard deviation; TNF, tumour necrosis factor; UC, ulcerative colitis.
Table 2 describes the clinical, endoscopic and histological markers of disease activity. Physicians rated UC as inactive in 33% of cases, mildly active in 30.1%, moderately active in 32% and severely active in 4.9% (three missing data) (Figure 2), and their mean (± SD) VAS was 2.5 (± 2.7) (three missing data). By contrast, patients rated their disease as inactive in 9.6% of cases, mildly active in 38.5%, moderately active in 42.3% and severely active in 9.6% (two missing data) (Figure 2). Patients’ mean VAS was 4.0 (± 2.6) (one missing value). There was no significant difference on patients’ perception of disease activity (PtGA) on the basis of the type of treatment: 36.9% of patients with no treatment or 5-ASA alone rated their disease as inactive, versus 24.4% of patients treated with immunosuppressants or advanced therapies, 30.8% versus 26.8% rated their disease as mildly active, 24.6% versus 41.5% as moderately active and 4.6% versus 4.9% as severely active, respectively (p = 0.309).
Clinical, endoscopic and histological markers of disease activity (n = 106 patients).

Number of missing data: a4; b3; c1; d31.
IQR, interquartile range; MES, Mayo endoscopic subscore; PRO, patient-reported outcomes; UCEIS, Ulcerative Colitis Endoscopic Index of Severity.

Disease activity as assessed by a 4-point ordinal scale according to the patient (PtGA) and the physician (PGA) (n = 101 patientsa).
The mean (± SD) total score of the IBD-Disk was 37 (± 20.7). The IBD-Disk item with the highest score was the energy item, with a mean of 5.1 (± 3.1). The two digestive items of the IBD-Disk, abdominal pain and defecation, were respectively at 4.7 (± 3.0) and 4.7 (± 3.6) (Table 3).
IBD-Disk scores (n = 106 patients).

Number of missing data: a6; b2; c3; d1.
IBD, inflammatory bowel disease; SD, standard deviation.
Concordance between PtGA and endoscopic assessment
The comparison between the PtGA and the endoscopic scores was performed in 104 patients (two missing data for PtGA).
In total, 34 patients (32.7%) evaluated their disease activity in complete agreement with the MES. The majority of discordant patients rated their disease activity in a more pessimistic manner than the endoscopy did (48/70 (68.6%)) (Table 4). The concordance between PtGA and UCEIS is presented in Figure 3.
Contingency table comparing PtGA and MES (n = 104 patients a ).

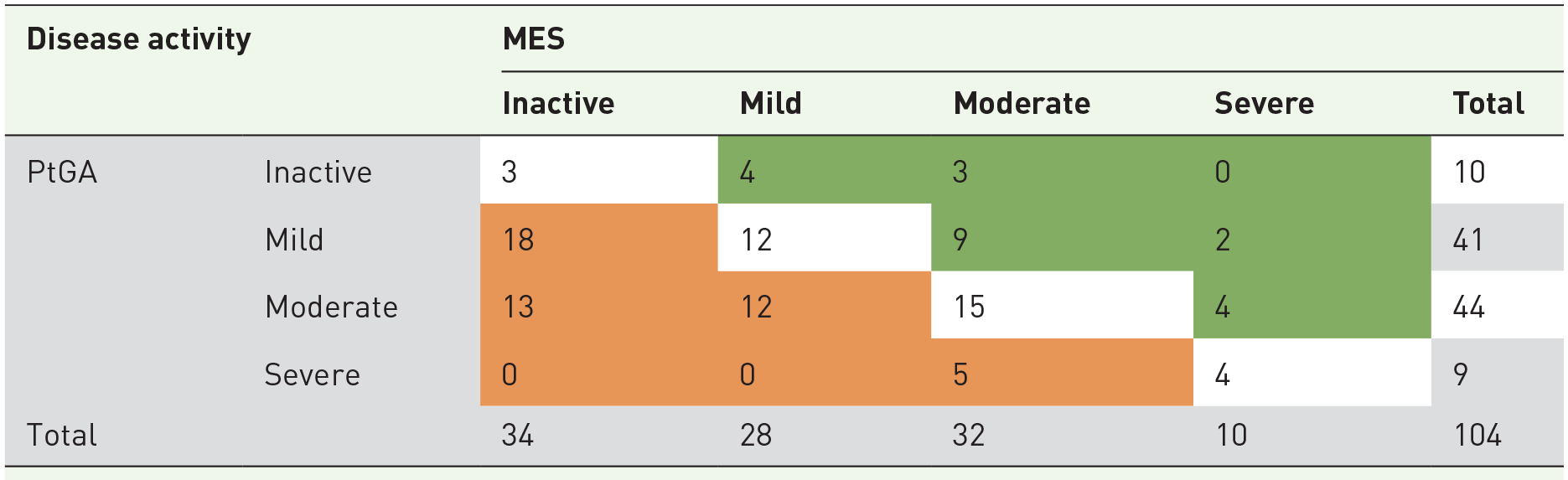
White cells highlight concordant patients; orange cells highlight patients who rated their disease activity in a more pessimistic way than endoscopy; green cells highlight patients who rated their disease activity in a more optimistic way than endoscopy.
Two missing data for PtGA.
MES, Mayo endoscopic subscore; PtGA, patient global assessment.
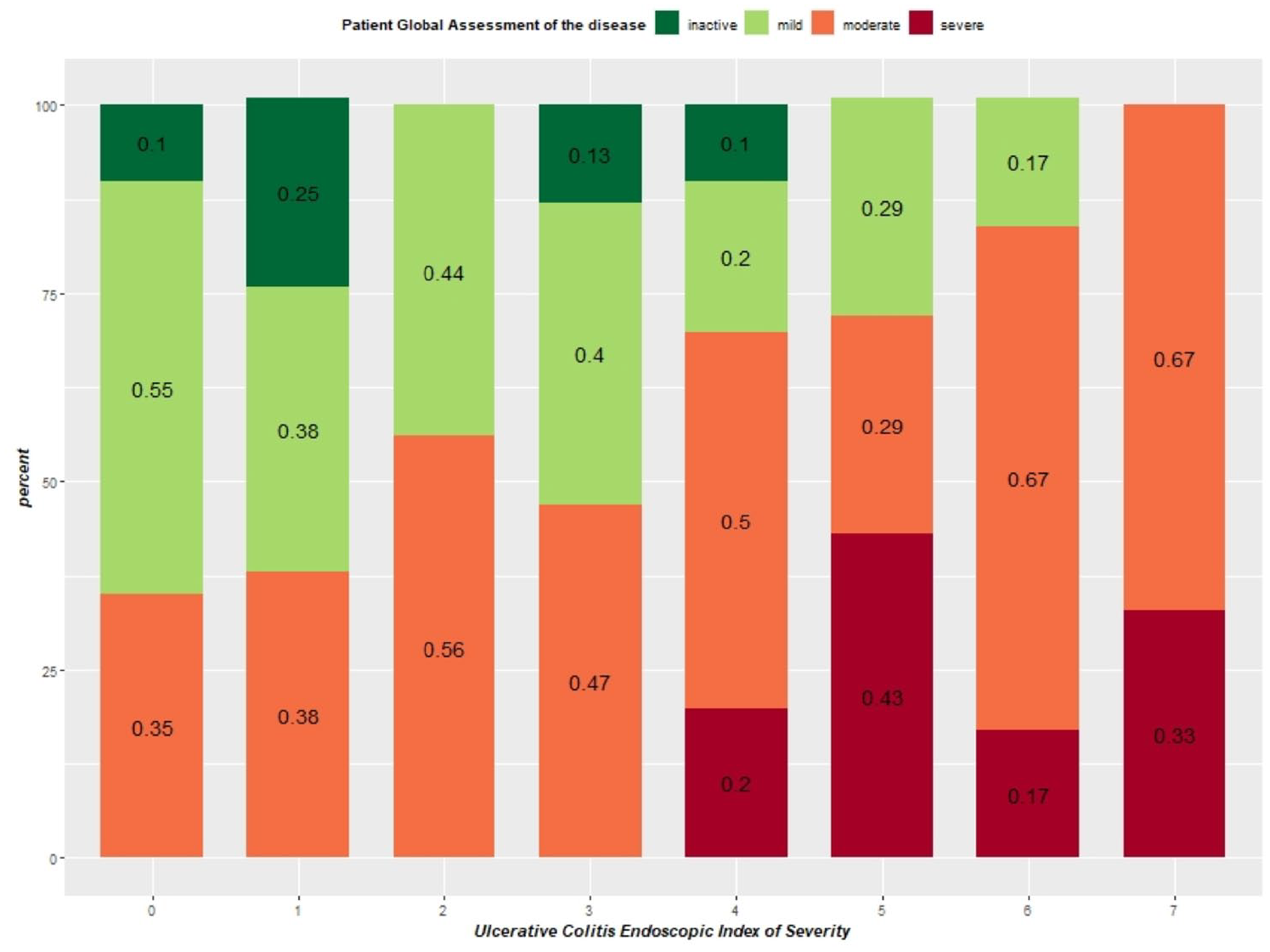
Concordance between PtGA and total UCEIS score (n = 104 patients*).
Factors associated with concordance between PtGA and endoscopic assessment
The comparison of socio-demographic and clinical characteristics between concordant and discordant patients is presented in Table 5 for the overall population. Concordant patients did not significantly differ from discordant patients on clinical characteristics such as disease duration, age at baseline and gender. Isolated proctitis was more frequent in discordant patients. Regarding PRO-2, stool frequency did not differ significantly between both groups, while rectal bleeding was more frequent in concordant patients. Objective markers of disease activity as assessed by endoscopy significantly differed between both groups, with more active disease in concordant than in discordant patients, notably in terms of vascular pattern and bleeding. Disease activity as evaluated by the physician (PGA) was also significantly higher in concordant than in discordant patients, whether on the ordinal score or the VAS. By contrast, the difference between both groups in terms of PtGA did not differ significantly. Finally, regarding the IBD-Disk, the total score tended to be higher in concordant than in discordant patients, indicating higher IBD-related disability. The items ‘abdominal pain’, ‘regulating defecation’ and ‘sexual life’ were all more impacted in concordant patients than in discordant patients. Among patients managed in the two tertiary care centres, 28.6% (12/42) were concordant, versus 35.5% (22/62) of patients enrolled in the secondary care centre (p = 0.461).
Comparison of socio-demographic and clinical characteristics between concordant and discordant patients based on the agreement between PtGA and MES (n = 104 patients*).

Number of missing data: a1; b3; c11; d20; e2; f4.
Two missing data for PtGA.
As part of the total Mayo score.
Bold values correspond to statistically significant results.
IBD, inflammatory bowel disease; IQR, interquartile range; MES, Mayo endoscopic subscore; PGA, physician global assessment; PRO, patient-reported outcomes; PtGA, patient global assessment; UC, ulcerative colitis; UCEIS, Ulcerative Colitis Endoscopic Index of Severity; VAS, visual analogue scale.
Given the impact of disease location on the agreement between PtGA and MES and the high proportion of the study population with isolated proctitis (42.5%), in whom symptoms (e.g. tenesmus) may be more likely to differ from endoscopic findings, potentially increasing the overall discrepancy, we next performed subgroup analyses according to disease location (proctitis vs left-sided or extensive colitis) (Table 6). Overall, results were similar to the full population analysis regarding the objective markers of disease activity. In both locations, higher concordance was associated with the total Mayo score and the PGA, as well as the two endoscopic scores (MES and UCEIS). Regarding the UCEIS, vascular pattern significantly differed between discordant and concordant patients in patients with proctitis, by contrast to bleeding that was more frequent in concordant patients with more extensive disease. Regarding PRO-2, rectal bleeding was associated with higher concordance in both UC locations; increased stool frequency was associated with higher concordance only in the subgroup of patients with left-sided or extensive disease while it did not differ between concordant and discordant patients with proctitis. Regarding IBD-Disk items, ‘abdominal pain’ and ‘sexual life’ were associated with higher concordance in patients with proctitis, while the difficulty in ‘regulating defecation’ was significantly associated with concordance only in the subgroup of patients with left-sided or extensive colitis, although the median IBD-Disk score regarding this item was numerically higher in concordant than in discordant patients also in patients with proctitis.
Comparison of socio-demographic and clinical characteristics between concordant and discordant patients based on the agreement between PtGA and MES in subgroup populations according to disease location (n = 104 patients*).
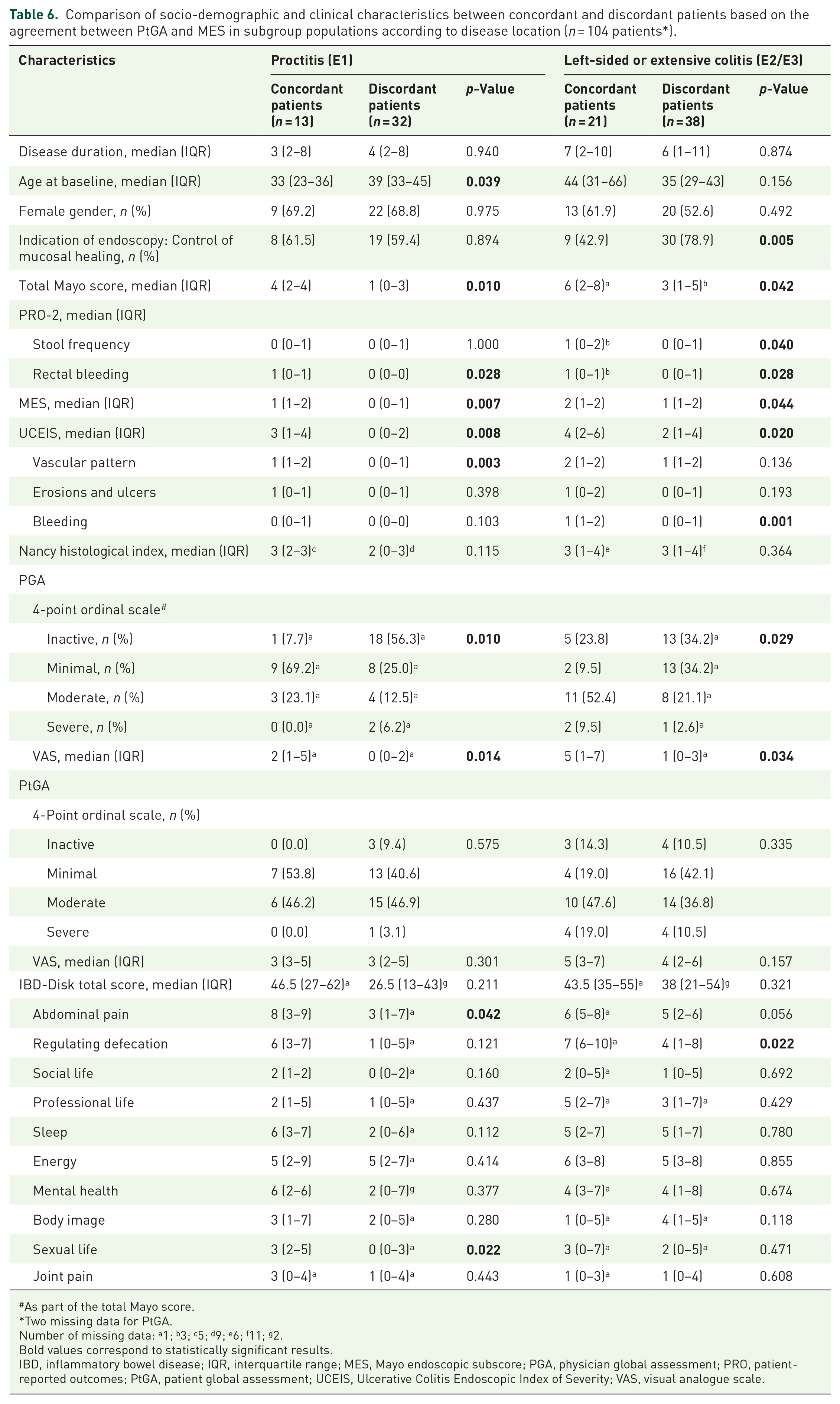
As part of the total Mayo score.
Two missing data for PtGA.
Number of missing data: a1; b3; c5; d9; e6; f11; g2.
Bold values correspond to statistically significant results.
IBD, inflammatory bowel disease; IQR, interquartile range; MES, Mayo endoscopic subscore; PGA, physician global assessment; PRO, patient-reported outcomes; PtGA, patient global assessment; UCEIS, Ulcerative Colitis Endoscopic Index of Severity; VAS, visual analogue scale.
The indication for endoscopy also had an impact. In the full population analysis, flexible sigmoidoscopy was performed to control mucosal healing more frequently in discordant patients than in concordant patients (Table 5), but it should be noted that this was true only in patients with left-sided or extensive colitis (Table 6).
Concordance between patients’ and physicians’ perception of disease activity
The comparison between PtGA and PGA was feasible for 101 patients at baseline (three missing data for PGA and two missing data for PtGA). There was a discrepancy between the PGA and the PtGA in 62 patients (61.4%), the vast majority of them (49/62 (79.0%)) being more pessimistic regarding disease activity than the physician (Table 7).
Contingency table comparing PGA and PtGA (n = 101 patients a ).


White cells highlight concordant patients; orange cells highlight patients who rated their disease activity in a more pessimistic way than their physician who was blinded to the patient’s response; green cells highlight patients who rated their disease activity in a more optimistic way than their physician who was blinded to the patient’s response.
Two missing data for PtGA, three missing data for PGA.
PGA, physician global assessment; PtGA, patient global assessment.
There was a moderate but significant positive correlation between the PtGA and the PGA as assessed by the VAS (r = 0.5269, p < 0.0001).
Discussion
Although less common than in CD, discrepancies between the PRO-2 and the endoscopic assessment may exist in patients with UC, especially regarding stool frequency that frequently remains increased even in the absence of active inflammation,6 –8 due to structural and functional sequelae. 12 Until now, there were no data on the concordance between the mucosal aspect as assessed by endoscopy and the overall patient’s perception of disease activity, a more global outcome than PRO-2 alone.
The multicentre prospective RectEVA study demonstrates that only one-third of patients with UC were in complete agreement with the endoscopic assessment. More than two-thirds of discordant patients rated the activity of their disease in a more pessimistic way than the endoscopy did. As expected, the less the disease was objectively active, the more the patients were discordant.
In line with the literature, rectal bleeding was more frequent in concordant than in discordant patients, while stool frequency was not different between both groups, as bowel movements may remain frequent despite the absence of active inflammation. As part of the IBD-Disk, abdominal pain and the difficulty in regulating defecation were significantly associated with a higher concordance between the patient’s perception of activity and the endoscopic evaluation. These data are consistent with recent literature. While abdominal pain is much more considered in CD, increasing attention should be paid to this poorly controlled symptom in UC patients, because it is prevalent and associated with lower quality of life and significant patient dissatisfaction, especially in those with active disease. 13
This also highlights the importance of the long-underestimated bowel urgency symptom that may be more accurate to reflect disease activity that the ‘stool frequency’ item of the PRO-2. This is of particular interest when considering the discrepancies between patients and physicians in the assessment of bowel urgency as demonstrated in recent publications.14,15 Moreover, a French survey including almost 300 patients recently showed that patients with bowel urgency have a significantly higher UC-related burden. 16 However, it should be noted that urgency may also be due to reduced rectal compliance which is not measurable on endoscopy but may influence patient’s perception of disease activity, especially in case of a medium disease duration as was the case in this cohort made up of a large proportion of young females with a 7-year-history of proctitis. This could also at least partly explain the discrepancies between patients’ and physicians’ perceptions of disease activity, as patients may perceive that urgency can be gotten from endoscopy while this is not the case.
In this study, there was no other factor that could explain the discordance of patients with endoscopy. Notably, the items ‘sleep’, ‘energy’, ‘mental health’ and ‘body image’ of the IBD-Disk were rated at equal level in both groups of patients. This suggests that discordant patients are not more ‘fragile’ but do experience persistent digestive symptoms that lead them to believe that their disease is still active, notably increased stool frequency. This may be due to structural and functional damage to the colon, such as benign strictures, colonic mobility abnormalities, microrectum and anorectal dysfunction. 12 Permeability modifications inducing mucosal hypersecretion or malabsorption may also occur and partly explain ongoing bowel symptoms in patients with IBD and mucosal healing. 17 Moreover, it is possible that these patients have other non-activity-related abnormalities that explain their symptoms, related to gut microbiota or the enteric nervous system, which were not studied here.
The presence of erosions and ulcers in endoscopy and the Nancy histological index were not statistically different between concordant and discordant patients, probably due to the relatively low proportion of included patients with moderately-to-severely active disease (about one-third of the study population) leading to insufficient statistical power.
The main strength of the RectEVA study is that it is the first study evaluating the correlation between endoscopy and overall PtGA in UC. Moreover, it is a multicentre study, conducted in a real-life setting, which prospectively and consecutively included more than 100 patients followed in two tertiary referral centres and in a secondary care centre. Patients followed in University Hospitals have frequently more severe disease, more disease-related complications, and longer proximal disease extension. 18 They are also more likely to receive more aggressive treatments. The recruitment of patients from both tertiary and secondary care centres allows a better representativeness of the sample included compared to the French general population of patients with IBD. Indeed, 70% of the patients included were treated with 5-ASA, of whom 53% exclusively.
The RectEVA study has a number of limitations. First, there was no sample size calculation because there were no prior sufficient data comparing the patient’s perception of disease activity and endoscopic activity. Most existing data on discrepancies between PRO-2 and endoscopy come from post hoc analyses of randomized controlled trials.6,8 One ‘real-life-setting’ prospective study addressed the same question focusing on the concordance between PRO-2 and MES and included 103 patients. 7 Thus, we defined a priori to include 100 patients in our study; finally, 106 patients were enrolled, which was sufficient to carry out parametric analyses of the distributions. It should nevertheless be added that a more homogeneous distribution in disease activity groups would have been desirable to limit confounding factors, given the low proportion of included patients with moderately-to-severely active disease (about one-third of the study population).
Moreover, no calibration was carried out between the different operators, although it is well-known that the interobserver agreement of the MES and the UCEIS is not perfect. 19 However, the six endoscopists who participated in this study were all IBD specialists familiar with UC endoscopic scoring systems. Another limitation is the absence of previous validation of the PtGA used to assess the concordance between patient’s perception and endoscopy.
The high proportion of patients with isolated proctitis (42.5%), in whom discordance was more frequent, may represent a selection bias. One may think that in this subpopulation, symptoms (e.g. tenesmus) are more likely to differ from endoscopic findings, potentially increasing the overall discrepancy. First, the high proportion of E1 patients in our study is due to the fact that they were included in a consecutive manner regardless of disease location. This reflects the real-word practice in the participating centres in which faecal calprotectin and intestinal ultrasound are commonly used to assess disease activity in patients with UC extending beyond the rectum given their high correlation with endoscopy and histology, 20 while endoscopy remains the gold standard for the assessment of proctitis in which ultrasound is compromised and faecal calprotectin less sensitive. 21 A subgroup analysis according to disease location (isolated proctitis vs left-sided or extensive colitis) was performed to address this potential selection bias. This analysis confirmed our main findings, strengthening the validity of our results, with the notable exception of defecation regulation which did not reach statistical significance in the subgroup of patients with proctitis despite showing similar numerical trends. This further reinforces the importance of bowel urgency regardless of disease location, because in our study, the high proportion of patients with proctitis did not explain the impact of this symptom on the concordance between PtGA and MES.
Importantly, PtGA of disease activity is hard to capture uniformly and consistently, and what is attributable to inflammation versus impact of disease on social and personal life is hard to reconcile. The difference between patients and physicians could be explained by a different definition of relapse between patients and physicians. Many non-digestive confounding factors can influence the patient’s subjective assessment of activity, including fatigue, psychological and socio-professional impact of the disease and the presence of extra-intestinal manifestations such as joint pain which can exacerbate the disability. 22 The ENMENTE study indeed showed that there was a discrepancy between doctors’ and patients’ perceptions of the impact of psychological aspects in IBD, with patients perceiving a greater impact than doctors. 23 Likewise, the NORMAL study identified disparities between patients and physicians in the perception of the impact of UC on patients’ lives. 24 Nevertheless, when analysing the results of the non-digestive items of the IBD-Disk in our study, there was no difference between concordant and discordant patients. However, it should be noted that the physician’s assessment of disease activity was done after the endoscopy was performed. Considering that there was no concordance between low or no endoscopic activity and patient’s perception, the clinical assessment of physician’s activity was probably downgraded in front of the finding of no significant endoscopic lesion, explaining part of the physician-patient discordance.
Another limitation of the study, intrinsic to the PtGA, may be linked to the patient’s confusion between ‘disease activity’ and ‘disease severity’. While ‘disease activity’ is typically defined based on symptoms at a moment in time, ‘disease severity’ considers the long-term burden of disease. 25 In this study, it was ‘disease activity’ that was compared to endoscopy at a given time, but when rating PtGA, some patients in clinical remission may have had difficulty in ignoring previous overwhelming flare-ups of their disease.
Moreover, topical treatments, that may lead to recto-sigmoid healing, were not collected and might have contribute to the extent of the discrepancy between PtGA and endoscopy. It is also possible that our study lacks power, and that a larger number of patients would have allowed us to identify more factors associated with PtGA/MES concordance/discordance.
Finally, C-reactive protein and faecal calprotectin levels were collected if available but data are not reported in the manuscript due to the high number of missing data, related to the fact that all patients had an endoscopy.
In conclusion, the RectEVA study showed that only one-third of patients with UC were in complete agreement with the endoscopic assessment. More than two-thirds of discordant patients rated the activity of their disease in a more pessimistic way than the endoscopy did. Concordance was higher in case of objective active disease. While stool frequency showed no significant difference between concordant and discordant patients, rectal bleeding – as anticipated – and most notably, abdominal pain and bowel urgency emerged as symptoms significantly correlated with higher concordance between patient-perceived disease activity and endoscopic evaluation. This highlights the importance of these underestimated symptoms in UC that should be assessed alongside the PRO-2 to accurately reflect clinical disease activity.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251346258 – Supplemental material for Discordance between patients’ perception and endoscopic assessment of disease activity in ulcerative colitis
Supplemental material, sj-docx-1-tag-10.1177_17562848251346258 for Discordance between patients’ perception and endoscopic assessment of disease activity in ulcerative colitis by Boilève Juliette, Trang-Poisson Caroline, Flamant Mathurin, Bouguen Guillaume, Goronflot Thomas, Freyssinet Marie, Kerdreux Elise, Bourreille Arnaud and Le Berre Catherine in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.