
Abstract
Background:
Ulcerative colitis (UC) is a chronic inflammatory disorder that can lead to physical, psychological, and social disabilities among patients.
Objectives:
To evaluate the disability level in a cross-sectional study of Chinese patients with UC and identify factors associated with disability.
Design:
This was a cross-sectional study.
Methods:
Between April 2022 and March 2023, UC patients from the Affiliated Hospital of Nanjing University of Chinese Medicine responded to questionnaires including the Inflammatory Bowel Disease Disability Index (IBD-DI), Fatigue Severity Scale, Patient Health Questionnaire-9, and Generalized Anxiety Disorder-7. In addition, demographic characteristics and clinical data of the patients were collected. Associated factors were identified by univariate and multivariate logistic regression analyses.
Results:
A total of 345 patients completed the questionnaires. The median (interquartile range) IBD-DI score was 16.2 (9.6–26.5), and the overall prevalence of disability was 39.7%. IBD-DI correlated with Mayo score, fatigue, anxiety, depression, hemoglobin (HGB), albumin (ALB), and erythrocyte sedimentation rate (ESR). Furthermore, the self-reported disability (IBD-DI > 20) was associated with lower BMI, active UC, disease severity of moderate and severe, disease location of left-sided UC (E2), using corticosteroids or biologics for treatment, Mayo score, fatigue, depression, anxiety, HGB, ALB, complement 3 (C3), and ESR. Notably, lower BMI, higher Mayo score, fatigue, and depression were identified as independent risk factors of disability in UC patients.
Conclusion:
This study revealed a significant level of disability among the Chinese UC population. Several clinical factors were identified to affect the level of disability, notably the risk factors including BMI, disease severity, fatigue, and depression.
Plain language summary
Ulcerative colitis (UC) is a lifelong inflammatory disease with a high risk of disability. Previously, several studies from different regions have evaluated the level of disability among UC patients using the Inflammatory Bowel Disease Disability Index (IBD-DI), but the situation in China is still unknown. This study enrolled 345 patients with UC in China, indicating a significant disability level. Several associated factors of disability have been identified, including disease activity, inflammatory status, nutritional deficiencies, and psychological comorbidity. Our results indicated the importance of paying attention to the disability accompanied by UC, and targeted interventions could be taken in clinical practice.
Introduction
Ulcerative colitis (UC) is a chronic, progressive, and potentially destructive disease, which cannot be cured thoroughly and may result in long-term intestinal impairment and loss of function. 1 UC is a subtype of inflammatory bowel disease (IBD). The harm caused by the disease meets the World Health Organization’s (WHO) definition of disability, including physical impairment, reduced function, and limited activity. 2 In 2023, the prevalence of UC is estimated to be 5 million cases around the world. 3 With the change in lifestyle and diet structure, the incidence and prevalence of UC in China have been increasing rapidly in the past 20 years, with the incidence reaching about 8.95 per 100,000 person-years according to a report. 4 Contrary to the global trend, UC patients in China face a higher disease burden, such as repeated recurrence, hospitalization, and surgery. 5 On top of that, patients often experience a decline in quality of life (QoL), fatigue, depression, and anxiety. 6 By report, the risk of work disability in people with UC is about 1.8 times higher than that of the general population. 3
Patient-reported outcomes (PROs) serve as a pivotal therapeutic goal in IBD. 7 The Inflammatory Bowel Disease Disability Index (IBD-DI) is a scale designed to quantify the level of disability in IBD patients. 8 Proven to be reliable and effective, this index has been translated into a Chinese version and validated for use in clinical research and practice. Previously, several population-based studies from different countries have validated the IBD-DI and revealed the correlation with factors such as disease activity, steroid use, and extraintestinal manifestations (EIMs).9–11 Nevertheless, there is a lack of large sample clinical studies to evaluate IBD-related disability among UC patients in China. Therefore, this study was conducted to assess the level of disability and associated factors in patients with UC.
Methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Table S1). 12
Study design and study population
A cross-sectional study was conducted on UC patients recruited from the outpatient department and ward of the gastroenterology department at the Affiliated Hospital of Nanjing University of Chinese Medicine from April 2022 to March 2023. This hospital serves as a regional center for the diagnosis and treatment of IBD in China.
The patients were selected consecutively. Patients with a confirmed diagnosis of UC based on clinical, endoscopic, and histological criteria were recruited. The exclusion criteria included unwillingness to participate in the study, an inability to comprehend or complete the questionnaire, and diagnosed psychiatric disorders. Patients with serious cardiovascular, lung, liver, and kidney diseases, or other serious diseases affecting survival were also excluded.
The eligible patients were asked to complete the questionnaire, including questions about the patient’s demographic and clinical data, such as age, gender, body mass index (BMI), employment status, smoking status, exercise frequency, disease duration, and medications. The colonoscopy report and medical records were consulted to gather information on the disease location and the presence of any EIMs. Disease location was defined according to the Montreal classification, 13 as E1 refers to ulcerative proctitis, E2 represents left-sided UC, and E3 stands for extensive colitis. Clinical disease activity was measured using the modified Mayo score. 14 A Mayo score of 2 or less was defined as remission, and a score greater than 2 was defined as active disease. Scores of 3–5 were classified as mild, 6–10 as moderate, and 11–12 as severe.
The questionnaire contained all the following validated PROs: disability (the IBD-DI), 6 fatigue (the Fatigue Severity Scale, FSS), 15 depression (the Patient Health Questionnaire-9, PHQ-9), 16 and anxiety (the Generalized Anxiety Disorder-7, GAD-7). 17
Concurrently, this study provided free laboratory testing, including blood routine examination, albumin (ALB), immunological and inflammatory indicators such as C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and fecal calprotectin (FC). Approximately half of the patients were willing to undergo the tests, and the subsequent results were recorded.
Questionnaire administration and data collection procedures
The questionnaires were completed in person, and patients completed the paper questionnaires under the guidance of researchers. With reference to the Chinese version of IBD-DI (Supplemental Table S2), as well as most translated versions, 11 the questionnaire we finally adopted consisted of 17 questions, covering limitations in 5 domains: overall health, body functions (sleep/energy, affect, body image, pain, diarrhea, BMI, and weight loss), activities participation (regulating defecation, looking after one’s health, interpersonal activities, and work/education), and body structures (hematochezia, arthralgia/arthritis). The first 12 questions were scored by patients on a 5-point Likert scale ranging from 0 to 4. The 13th question on defection frequency was scored as follows: 0 for “0,” 1–7 for “1,” 8–18 for “2,” 19–29 for “3,” and >29 for “4.” BMI was scored as “0” for a BMI >18.5, and “4” for a BMI ⩽18.5. Binary items were scored as “0” for no and “4” for yes. The 16th question on hematochezia was scored as “0” for no, “2” for mild, and “4” for severe. The total score was scaled according to the following formula: score × 100/(p × 4), where p referred to the number of questions answered. Scores range from 0 to 100, with 0 indicating no disability and higher scores indicating greater disability. A score greater than 20 is considered to have IBD-related disability and is graded as follows: 20–35 (mild disability), 35–50 (moderate disability), and 50–100 (severe disability).
Psychological status was assessed using the PHQ-9 16 for depression and GAD-7 17 for anxiety, respectively. The PHQ-9 is composed of nine items with scores ranging from 0 to 27. The GAD-7 encompasses seven items, with scores ranging from 0 to 21. The severity classes of both questionnaires are defined as follows: 0–4 (normal), 5–9 (mild), 10–14 (moderate), and ⩾15 (severe). The FSS 15 is used to assess the level of fatigue experienced by patients, as well as the subsequent influence of this fatigue on their physical function, working productivity, and social interactions. It consists of nine questions with each question scored 1–7, then the total score is averaged to produce a global score. The scores range from 1 to 7 with higher scores reflecting greater fatigue. Fatigue was defined as a mean FSS score >4 points.
Statistical analysis
All of the PROs and other quantitative variables were analyzed using nonparametric techniques, as the normality analysis performed with the Kolmogorov–Smirnov test on the variables showed non-normal distributions. Nonparametric scores were expressed as median (interquartile range (IQR)), and we employed the Mann–Whitney U test to assess differences between groups. Qualitative variables were expressed as numbers (percentages), using Chi-square tests.
Relationships between PROs, Mayo score, and laboratory indicators were quantified using Spearman’s rank correlation coefficient (SRCC). A correlation greater than 0.4 was considered “acceptable.” A correlation coefficient less than 0.3 was interpreted as “poor,” 0.3–0.5 as “fair,” 0.5–0.8 as “moderately strong,” and anything above 0.8 as “very strong.”
Associated factors of disability were identified through univariate and multivariate logistic regression analyses. Statistically significant factors (p < 0.05) from the univariate logistic analysis were included in the multivariate analysis to identify independent influencing factors. Due to the presence of too many missing data in the laboratory indicators, we decided not to include them in the multivariable analysis to avoid biasing the outcomes. Effect sizes are expressed as the odds ratio (OR) with a 95% confidence interval (CI).
Statistical analyses were performed using IBM SPSS (version 26, IBM, Armonk, NY, USA). Statistical significance was considered as p < 0.05. Figures were drawn using GraphPad Prism (version 9.5.0, GraphPad Software, CA, USA).
Results
Demographic and clinical characteristics
A total of 353 patients with UC were enrolled in the study, with 345 patients ultimately completing the questionnaires. Of these, 274 (79.1%) were outpatients, and the others were inpatients. Characteristics of the patients are shown in Table 1. Among them, 189 were males (54.8%) and 156 were females (45.2%). The ages of the patients ranged from 10 to 80 years old. In addition, 48 (13.9%) patients reported to be smokers. The respondents exhibited diverse occupational backgrounds, including students, farmers, workers, service personnel, company employees, professionals (such as teachers and doctors), freelancers, and retirees. Regarding exercise frequency, over half of the patients did little or no exercise (n = 193), and 88 (25.5%) patients exercised 1–2 times per week.
Analysis of clinical characteristics and IBD-DI score in the study population.

Values with missing data.
5-ASA, 5-aminosalicylic acid; ALB, albumin; BMI, body mass index; C3, complement 3; CRP, C-reactive protein; E1, ulcerative proctitis; E2, left-sided ulcerative colitis; E3, extensive colitis; EIMs, extraintestinal manifestations; ESR, erythrocyte sedimentation rate; FC, fecal calprotectin; FSS, the Fatigue Severity Scale; GAD-7, the Generalized Anxiety Disorder-7; HGB, hemoglobin; IBD-DI, Inflammatory Bowel Disease Disability Index; IgA, immunoglobulin A; IQR, interquartile range; PHQ-9, the Patient Health Questionnaire-9; TCM, traditional Chinese medicine.
The majority of patients were diagnosed with the chronic relapsing type of UC (n = 293, 85%). The median modified Mayo score among all respondents was 4 (3–6). Furthermore, 254 (73.6%) patients had active disease, of whom 100 (28.9%) had moderate disease and 18 (5.2%) had severe disease according to Mayo score criteria. The distribution of disease locations was roughly equal. In addition, 21 (6%) patients presented with EIMs. At the time of the study, 245 (71.2%) patients were receiving 5-aminosalicylic acid treatment, 23 (6.7%) patients were using corticosteroids, 24 (7%) patients were undergoing biologic therapy, 48 (14%) patients were receiving traditional Chinese medicine (TCM), and 4 (1.2%) patients were using immunosuppressants for treatment.
The median (IQR) FSS score was 2.7 (1.6–4), and 91 patients (26.4%) were bothered with fatigue. In terms of psychological status, the median (IQR) GAD-7 score was 2 (0–5), and 95 (27.5%) patients exhibited different levels of anxiety condition. According to the PHQ-9 scores reported by patients, the median (IQR) score was 3 (1–6), and 108 (31.4%) patients were classified as having depression.
In the laboratory testing results, based on patient preferences, about 120–137 (34.8%–39.7%) patients tested blood routine, ALB, and inflammation indicators, while only 96 (27.8%) patients tested immunological indicators. The median (IQR) ESR was 12 (4–23), and FC levels were about 422.9 (45.8–831), significantly exceeding the threshold of 250.
Disability scores of the study population
Among the overall 345 patients with UC, the IBD-DI score ranged from 0 to 78.13, with a median (IQR) score of 16.2 (9.6–26.5). In terms of the different domains, the scores were as follows: overall health 2.9 (1.5–2.9); body function 8.8 (5.9–16.2); body structure 2.9 (0–3); and activity participation 0 (0–2.9). The distribution of disability severity was illustrated in Figure 1, as minimal, mild, moderate, and severe disability were present in 208 (60.3%), 96 (27.8%), 34 (9.9%), and 7 (2%) patients, respectively. It resulted in an overall prevalence of disability of 39.7%. In total, 314 (91%) of the questionnaires were fully completed, and the maximum percentage of missing answers per item was 1.2% (question 12).

Distribution of IBD-DI score in a UC cross-sectional study (n = 345). The IBD-DI score ranged from 0 to 78.13, with a median (IQR) score of 16.2 (9.6–26.5). The IBD-DI score covered four different domains, including overall health, body function, body structure, and activity participation.
The 345 patients were classified into IBD-DI > 20 (n = 137) or IBD-DI < 20 (n = 208), for a differentiation between disability or no disability (Table 1). Analyzing the demographic and clinical characteristics, the prevalence of disability was higher in patients with active UC (p < 0.001), especially in those with moderate and severe severity (p < 0.001).
The Mayo score was elevated in those with disability (p < 0.001). Meanwhile, the levels of fatigue (FSS), anxiety (GAD-7), and depression (PHQ-9) were significantly worse in patients who reported disability (p < 0.001).
In terms of laboratory indicators, patients with disability exhibited reduced hemoglobin (HGB) and ALB, but increased levels of ESR and CRP (p < 0.05).
Correlation analysis of IBD-DI
To elucidate the potential relationships between UC disease severity, psychological comorbidities, laboratory indicators, and self-reported disability, we calculated the SRCC between Mayo score, FSS, GAD-7, PHQ-9, HGB, ALB, immunoglobulin A (IgA), IgG, IgM, complement 3 (C3), C4, ESR, CRP, FC, and IBD-DI.
Statistical results showed the SRCCs of IBD-DI with Mayo, FSS, GAD-7, PHQ-9, HGB, ALB, and ESR were statistically significant (p < 0.05), as illustrated in Figure 2. We observed the IBD-DI correlated strongly with GAD-7 (ρ = 0.6, p < 0.001) and PHQ-9 (ρ = 0.67, p < 0.001). Also, IBD-DI was positively correlated with Mayo score (ρ = 0.49, p < 0.001), FSS (ρ = 0.49, p < 0.001), and ESR (ρ = 0.18, p = 0.042), while negative correlated with HGB (ρ = −0.26, p = 0.002), and ALB (ρ = −0.2, p = 0.023).

Spearman’s rank correlation coefficients between IBD-DI and clinical parameters. The strongest correlations were observed between IBD-DI and psychological factors (GAD-7: ρ = 0.6, PHQ-9: ρ = 0.67, both p < 0.001). Moderate correlations were found with the Mayo score (ρ = 0.49) and Fatigue Severity Scale (ρ = 0.49, both p < 0.001). Weak correlations were noted for ESR (ρ = 0.18, p = 0.042), HGB (ρ = −0.26, p = 0.002), and ALB (ρ = −0.2, p = 0.023). Statistically significant correlations are indicated with *p < 0.05, **p < 0.01.
Associated factors of disability
In univariate logistic analysis (Table 2), risk factors associated with self-reported disability (IBD-DI > 20) included BMI < 18.5kg/m² (OR (95% CI) = 5.01 (2.6–9.62), p < 0.001), active UC (OR (95% CI) = 2.8 (1.62–4.84), p < 0.001), disease severity of moderate (OR (95% CI) = 3.3 (2.02–5.38), p < 0.001) and severe (OR (95% CI) = 4.78 (1.72–13.25), p = 0.003), disease location of E2 (OR (95% CI) = 2.7 (1.55–4.73), p < 0.001), and treatment with corticosteroids (OR (95% CI) = 3.07 (1.25–7.51), p = 0.014) or biologics (OR (95% CI) = 2.72 (1.15–6.47), p = 0.023).
Factors associated with disability (IBD-DI > 20) in univariate logistic regression analysis.
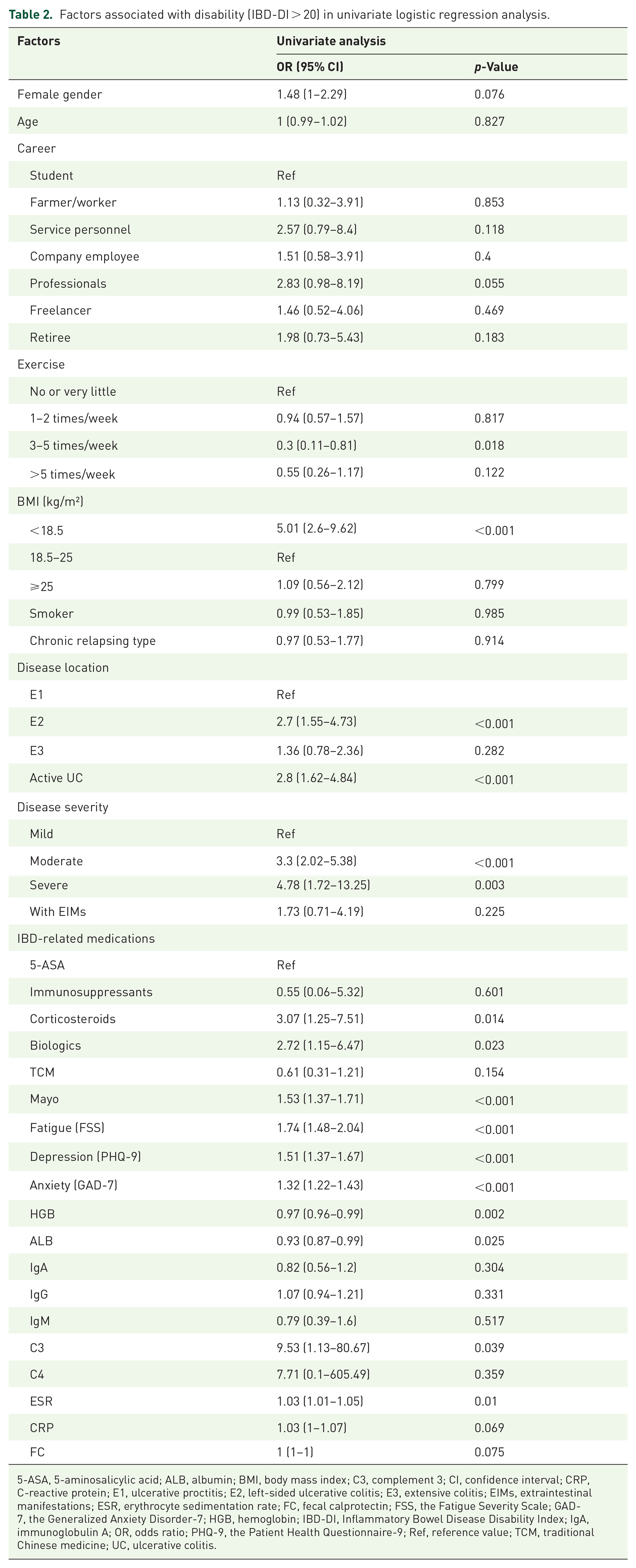
5-ASA, 5-aminosalicylic acid; ALB, albumin; BMI, body mass index; C3, complement 3; CI, confidence interval; CRP, C-reactive protein; E1, ulcerative proctitis; E2, left-sided ulcerative colitis; E3, extensive colitis; EIMs, extraintestinal manifestations; ESR, erythrocyte sedimentation rate; FC, fecal calprotectin; FSS, the Fatigue Severity Scale; GAD-7, the Generalized Anxiety Disorder-7; HGB, hemoglobin; IBD-DI, Inflammatory Bowel Disease Disability Index; IgA, immunoglobulin A; OR, odds ratio; PHQ-9, the Patient Health Questionnaire-9; Ref, reference value; TCM, traditional Chinese medicine; UC, ulcerative colitis.
The risk of disability was also significantly greater in patients with higher Mayo scores (OR (95% CI) = 1.53 (1.37–1.71), p < 0.001), fatigue (OR (95% CI) = 1.74 (1.48–2.04), p < 0.001), depression (OR (95% CI) = 1.51 (1.37–1.67), p < 0.001), anxiety (OR (95% CI) = 1.32 (1.22–1.43), p < 0.001), and higher level of C3 (OR (95% CI) = 9.53 (1.13–80.67), p = 0.039) and ESR (OR (95% CI) = 1.03 (1.01–1.05), p = 0.01), as illustrated in Table 2.
Subsequently, in a multivariate analysis, the independent risk factors of IBD-related disability included BMI <18.5 kg/m² (OR (95% CI) = 7.358 (2.695–20.087), p < 0.001), higher Mayo score (OR (95% CI) = 1.74 (1.488–2.035), p < 0.001), fatigue (OR (95% CI) = 1.261 (1.002–1.588), p = 0.048), and depression (OR (95% CI) = 1.558 (1.364–1.781), p < 0.001), as illustrated in Table 3.
Factors associated with disability (IBD-DI > 20) in multivariate logistic regression analysis.

BMI, body mass index; CI, confidence interval; FSS, the Fatigue Severity Scale; IBD-DI, Inflammatory Bowel Disease Disability Index; OR, odds ratio; PHQ-9, the Patient Health Questionnaire-9; Ref, reference value.
Discussion
In this Chinese cross-sectional study involving 345 patients with UC, the median (IQR) score of IBD-DI was 16.2 (9.6–26.5), with a disability prevalence of 39.7%. Drawing parallels from previous large samples of IBD-DI studies, significant regional differences were observed. Notably, the severity of disability appears higher in Western countries, ranging approximately from 17.9 to 39.2.9–11,18,19 Some studies even indicate UC patients experience higher levels of disability than CD patients.11,20 A French study reported a high IBD disease burden, including poor QoL, fatigue, work impairment, and depression, with one-third of patients reporting marked disability and anxiety. 20 In another French cohort, the mean (±SD) IBD-DI score was 28.0 (±18.4), higher than our results. 19 In a European cohort, the overall disability pension rate at 10 years after diagnosis of IBD was 18.8%, with elevated relevant risks of 1.8 for UC.21,22 An Eastern European assessment of work disability and productivity loss reported a 32.3% disability pension rate and 28% work productivity loss in this IBD population. 23 According to the Global Burden of Diseases, Injuries, and Risk Factors Study of IBD, in 2017, the age-standardized rates (ASRs) of years lived with disability (YLDs) and disability-adjusted life-years (DALYs) were 12.6 and 23.2 per 100,000 population, respectively. 24 Whereas, research on IBD-related disability in Asia is relatively inadequate. In 2019, the ASRs of YLDs and DALYs of IBD in China were 7.07/100,000 and 13.1/100,000, respectively. 5 A Singaporean study reported a 28% disability prevalence within an IBD cohort. 25 Overall, our study may indicate a relatively high level of UC disability compared to other chronic diseases.
We observed that IBD-DI correlated with Mayo score, fatigue, anxiety, depression, HGB, ALB, and ESR, particularly showing strong correlations with anxiety and depression. Our results indicate that disability was associated with low BMI, disease activity, disease severity, disease location, treatment with corticosteroids or biologics, Mayo score, fatigue, depression, anxiety, HGB, ALB, C3, and ESR. In addition, BMI, Mayo score, fatigue, and depression were identified as independent risk factors for IBD-related disability in UC patients. Overall, the association of disability in UC was manifested as a positive relationship with disease severity and psychological comorbidity and a negative relationship with nutritional status.
Other investigations focusing on different dimensions have demonstrated that IBD-related surgery, hospitalization, disease activity, steroid use, and EIMs serve as indicators of increased disability in the IBD population.10,26 A meta-analysis identified disease activity and unemployment as risk factors for disability in patients with UC. 11 An international multicenter study provided strong evidence that IBD-related disability is associated with presenteeism and hospitalization. 27 Conversely, factors associated with IBD-DI vary across different regions. A multicenter study conducted in America found that IBD patients who belong to minority groups, have public insurance, or have low household income are 2–3 times more likely to report moderate-to-severe disability. 28 Another study focusing on UC patients from New York suggested that ileal pouch-anal anastomosis is associated with significant disability, particularly in female patients and those with public insurance. 29
With the changes in lifestyle and dietary structure brought about by economic globalization, the incidence of UC in China has risen rapidly. 4 The treatment goals have evolved from simple symptom control to mucosal healing and patient-centered outcome reporting.30,31 A meta-analysis demonstrated a significantly higher prevalence of psychiatric comorbidities in IBD patients compared to the general population, including depression (OR (95% CI) = 1.42 (1.33–1.52), p < 0.0001), anxiety (OR (95% CI) = 1.3 (1.22–1.44), p < 0.0001), and bipolar disorder (OR (95% CI) = 1.64 (1.20–2.24), p < 0.0001). 32 The Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) II consensus updated in 2021 and the latest UC diagnosis and treatment guidelines issued in China in 2023 both advocated a treat-to-target (T2T) therapeutic strategy as an optimized management approach for UC.31,33 This strategy aims to enhance QoL over the long term, while emphasizing both objective inflammatory status and PROs as key indicators of treatment effectiveness. Since PROs were introduced into the field of IBD, they have emerged as a research hotspot and a crucial outcome indicator for T2T.7,34 The PRO scales have enriched the evaluation methods for UC, allowing for a more objective assessment of subjective symptoms. Given that objective clinical indicators and subjective symptoms may not always align, PRO scales have effectively bridged this gap, informing clinical decision-making. Previous PRO scales primarily centered on symptoms, mental health, and QoL. However, IBD-related disability has increasingly captured the attention of researchers in recent years.20,26 IBD-related disability encompasses a range of subjective and objective symptoms, while the distinctiveness of IBD-DI resides in its ability to not only assess objective physical impairment but also reflect the subjective attitude of patients. 8
The somatic symptoms of UC, such as hematochezia, diarrhea, abdominal pain, and abdominal distension, along with disabling complications like anemia, malnutrition, EIMs, and psychological abnormalities, can significantly impair work capabilities, productivity, and overall QoL. 3 The long-term disease course may negatively affect patients’ physiology, emotions, social abilities, and QoL, ultimately leading to physical and mental disabilities.
This study has several strengths. It fills a research gap regarding disability in the Chinese UC population, which may offer valuable insights for clinical management. The research covered subjective and objective factors such as demographic characteristics, disease characteristics, treatment, physical and mental health, nutritional status, immune inflammation markers, and other dimensions. To our knowledge, no previous studies have explored correlations between the IBD-DI scale and laboratory indicators in UC patients. Although the sample size of patients who tested laboratory indicators was relatively small, our findings suggest that monitoring HB, ALB, and ESR may help reduce disability levels in patients.
According to the results of this study, clinicians may reduce the risk of disability associated with UC by addressing various aspects of patient care. The findings suggest that reducing inflammation, achieving UC remission, improving anemia and malnutrition, and intervening in psychological comorbidities may be effective strategies to prevent disability. In addition, integrating TCM into the treatment may be beneficial. TCM, as a bio-psycho-social medicine, offers advantages through its holistic, multicomponent, multi-target, and multi-pathway approach. 35 The latest Chinese UC guideline recommends incorporating TCM during the remission period. 30 While existing evidence supports the beneficial role of TCM in UC treatment,36,37 further research is needed to develop comprehensive treatment strategies, accumulate robust clinical evidence, and elucidate its underlying mechanisms of effects.
However, some limitations of this study need to be acknowledged. The findings of this study are based on patient self-reports, which show the superiority of PROs but also introduce an inherent subjective nature that could potentially influence the observed result. To address this, future studies could incorporate physician evaluations to provide cross-validation against the PROs. At the time of the study, we collected several basic demographic factors, but some important variables such as socioeconomic status (e.g., income, education level, and medical insurance), lifestyle (e.g., physical activity patterns and occupational exposures), and dietary habits (e.g., Mediterranean diet, pro-inflammatory diets, and enteral nutrition) were not included. These variables may be potential confounders affecting both disease progression and disability. Since these unmeasured confounders could potentially bias the outcomes of IBD disability, future studies should incorporate these factors to strengthen the validity of the results. As a cross-sectional study, the restricted sample size (especially the small number of patients with blood test data) may limit the generalizability of our findings to other populations. In addition, as a single-center study conducted in a Class III Grade A TCM hospital, with participants primarily recruited from outpatient clinics, the study population may have lower disease severity and specific demographic characteristics, potentially introducing selection bias. These factors may limit the generalizability of our findings to the broader Chinese UC population. For future evaluations of disability among patients, prospective studies with multiple follow-ups would be more accurate.
Conclusion
Therefore, as a lifelong disease with a high risk of disability, UC has a heavy disease burden and seriously affects the physical function, social activity, and mental health of patients, which should be paid high attention to. In conclusion, this study identified mainly association factors of disability in UC, including disease activity, inflammatory status, nutritional deficiencies, psychological comorbidity, as well as treatment received, which may enable targeted interventions to be developed for UC patients.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251333989 – Supplemental material for IBD-related disability among patients with ulcerative colitis in China: a cross-sectional study
Supplemental material, sj-docx-1-tag-10.1177_17562848251333989 for IBD-related disability among patients with ulcerative colitis in China: a cross-sectional study by Mengyuan Zhang, Xiaojuan Liu, Shichen Min, Hong Shen and Lei Zhu in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.