
Abstract
Background:
Longer cecal withdrawal time has been linked to a higher adenoma detection rate (ADR), with a minimum duration of 6 min recommended. Therefore, we developed the cecal withdrawal vocal timer (CWVT), a novel software tool that is command-activated at cecal intubation and vocally informs the endoscopist of the withdrawal duration every minute.
Objectives:
Evaluating the efficacy of the CWVT in enhancing adenoma detection.
Design:
A retrospective, single-center study of screening colonoscopies with adequate preparation and documented cecal intubation.
Methods:
The primary endpoint was the change in the department’s ADR before (2022) and after the CWVT introduction (January 2023–February 2024). Secondary endpoints included the ADR change between procedures with and without CWVT after its introduction and the ADR change among individual endoscopists.
Results:
The study included 1098 and 1330 eligible colonoscopies pre- and post-CWVT introduction, respectively. Following CWVT introduction, 67.3% of colonoscopies were performed with activated CWVT, with a median withdrawal time of 8.7 (interquartile range: 6.9–11.8) min. The department ADR was 25.5% following CWVT introduction, without a significant difference compared to the year before (26.2%, p = 0.71). During the post-CWVT implementation period, colonoscopies with activated CWVT had higher ADR than those without (28.4% vs 19.5%, respectively, p < 0.001). The improvement was mainly driven by the detection of adenomas smaller than 10 mm and was consistent across 11 out of 12 months in this period and among most endoscopists.
Conclusion:
While an overall ADR improvement was not achieved with the CWVT, the ADR was higher in post-CWVT procedures that utilized the CWVT than those that did not, warranting further prospective studies to evaluate CWVT’s contribution to screening colonoscopy performance.
Plain language summary
A cecal withdrawal time of more than six minutes is an established quality measure for screening colonoscopies, as it allows adequate inspection of the colon lining. We developed a novel real-time cecal withdrawal vocal timer (CWVT), which is activated by voice command when the endoscopist reaches the cecum with the scope and announces the withdrawal time every minute. After introducing the CWVT, the overall adenoma detection rate (ADR) in our department did not improve compared to the previous year. However, during this period, colonoscopies performed with the CWVT had a higher ADR than those without, particularly for adenomas smaller than 10 mm. While the overall ADR remained unchanged, the increased detection with CWVT activation suggests that further studies are needed to explore its potential benefits.
Keywords
Introduction
Colorectal cancer (CRC) is the third leading cause of cancer death for both men and women, 1 underscoring the importance of effective prevention strategies. High-quality screening colonoscopy is a fundamental element in CRC prevention efforts. Over the years, several quality indicators for the assessment of screening colonoscopy performance have been suggested, including adenoma detection rate (ADR), withdrawal time, quality of bowel preparation, and cecal intubation rate. 2 ADR, representing the proportion of screening colonoscopies performed by a physician that detected at least one histologically confirmed neoplastic lesion, is of particular significance. Studies have shown an inverse association between ADR and the risk of interval CRC, with each 1.0% increase in ADR correlating with a 3% decrease in interval cancer risk.3,4 ADR is currently recommended as a quality benchmark by professional societies with performance targets of 20% for women and 30% for men.2,5
An additional essential quality metric for screening colonoscopies is the withdrawal time, which refers to the duration of the withdrawal phase of the colonoscope once the cecum has been intubated and inspected. Longer withdrawal time during screening colonoscopy was associated with higher ADR in several studies.6,7 A threshold of 6 min was found as the minimum duration allowing adequate inspection of the colonic mucosa and is therefore endorsed by professional societies.2,5,6 Several studies have explored the efficacy of interventions to prolong withdrawal time in enhancing ADR, such as human-based monitoring of withdrawal time or protocolized instructions, and yielded conflicting results.8–10
We hypothesized that real-time feedback on withdrawal duration would extend the duration of colonoscope withdrawal and prevent endoscopists from withdrawing the scope too quickly. This, in turn, may improve screening colonoscopy performance, as reflected by the ADR. Therefore, we developed the cecal withdrawal vocal timer (CWVT), a novel software patch that is command-triggered once the cecum has been intubated. The CWVT informs the physician of the withdrawal duration in real-time and announces every minute vocally. In this study, we assessed whether CWVT implementation in our endoscopy Unit has improved the ADR.
Patients and methods
Cecal withdrawal timer
In collaboration with the computer and digital innovations hubs of Sheba Medical Center and with Medlife LTD (Or-Yehuda, Israel) Company, our gastroenterology department has developed a novel add-on software timer for endoscopic procedures. The timer is activated by the endoscopist’s vocal command upon cecal intubation and automatically takes a concomitant cecal photo. The software patch then presents the elapsed time from cecal intubation until the end of the procedure. The measured time includes any procedure performed during the colonoscopy, such as polypectomy. In addition, the CWVT vocally announces the withdrawal duration every minute, informing the endoscopist in real-time and allowing him to pace the withdrawal phase (Supplemental Video 1). The CWVT was designed to function without requiring additional steps from the endoscopist or assistance from other medical staff, as it is automatically activated by a vocal command, with a backup option for the nurse to operate it by pressing a designated button. It was implemented across all our endoscopy suites. All tests were performed with high-definition endoscopes and an artificial intelligence-based computer-aided diagnosis system (GI Genius, Medtronic, Italy). Given that the study includes only screening colonoscopies of patients without IBD, known complex polyps, or other relevant GI background, advanced imaging techniques (e.g., NBI) were not used as they are not indicated.
Study design
A retrospective cohort study was conducted at a high-volume gastroenterology unit of an academic tertiary medical center. The CWVT was introduced in all eight endoscopy suites in January 2023. To compare the additional value of CWVT introduction, we defined the year prior to CWVT introduction (January–December 2022) as the pre-CWVT period and January 2023 to February 2024 as the post-CWVT period. Technical problems impeded the proper use of the system in 2 months (May and June), which were excluded from the analysis, resulting in 12 months included in the post-CWVT period. Data from all colonoscopies performed during this period were extracted, including demographic details, procedure-related information, and histopathology results. The study included only screening colonoscopies in adults >50 years old or colonoscopies in patients with a family history according to accepted guidelines. Colonoscopies for other indications were not included. Procedures with poor preparation, defined as a Boston Bowel Preparation Scale score below 6 or by real-time endoscopist’s judgment of poor bowel preparation, procedures that were not completed for any reason, and those in which cecal intubation was not achieved were excluded. The performing physicians’ names were anonymized by replacement with a random letter. Withdrawal time was available only for procedures with CWVT activation, as it is not routinely measured reliably without this tool. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 11 (Supplemental Table 1) and was approved by the institutional review board; written informed consent was waived due to the retrospective design and use of anonymized data.
Endpoints
The primary endpoint was the change in the Unit’s collective ADR from pre-CWVT (i.e., 2022) to the post-CWVT period (January 2023–February 2024). During the post-CWVT period, although all endoscopists were instructed to use the CWVT, it was not activated in all procedures, as part of the implementation and adjustment process. Procedures in which the CWVT was not activated for any reason comprised the non-activated group. Based on these tests without CWVT activation, secondary endpoints were defined and included the ADR change between tests with and without CWVT and among specific endoscopists during the post-CWVT period.
Statistical analysis
ADR was calculated as the proportion of procedures with a detected adenoma confirmed by pathology out of the total number of colonoscopies. Continuous normally distributed variables were presented as mean (±standard deviation), while non-normally distributed variables were presented by median (interquartile range (IQR)). Normality was assessed with the Shapiro–Wilk test and visual inspection of quantile–quantile plots and histograms. The distribution of covariates between study groups was compared by the Chi-square test or Fisher’s exact test for categorical data, and the Student’s t test or the Mann–Whitney test for normally and non-normally distributed continuous variables, respectively. Subsequently, the ADR was adjusted for variables with different distributions by estimating the predicted probabilities using a multivariable logistic regression with marginal standardization. Since CWVT usage varied among physicians, an interaction between endoscopist performance and CWVT usage frequency was also identified as a potential confounder. Therefore, we assessed for a monotonic correlation between baseline ADR and CWVT usage frequency using Spearman’s correlation coefficient. An additional sensitivity analysis was performed by stratifying the cohort into frequent and infrequent CWVT users, using the median usage as the cutoff, and calculating the adjusted ADR pre- and post-implementation for each group.
All tests were two-sided with a significance level defined as p-values <0.05. Data processing and statistical analysis were performed in R statistical software version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Of 20,229 colonoscopies performed in the endoscopy unit between January 2022 and February 2024, 2428 eligible tests were included in the study (Figure 1). In total, 1098 tests were conducted during 2022, the pre-CWVT period, and 1330 post-CWVT from January 2023 to February 2024. The median age of patients was 60 (IQR: 53–68) years, and 57% were females. Overall, 39 physicians performed procedures during the study period, and 627 adenomas were detected.

Study the flowchart. The same colonoscopy test may have more than one criterion for exclusion.
The CWVT was activated in 67.3% (n = 895/1330) of the procedures performed post-CWVT. CWVT usage exceeded 50% in 11 out of 12 months included in the study (Figure 2(a)). As noted, technical issues impeded proper use of the system in two additional months, which were therefore excluded from the analysis. The mean usage percentage of CWVT in the last 5 months of the study period was 75%, likely representing physicians’ adjustment to the system and improved technical aspects. When assessing CWVT usage by different physicians, roughly 50% used the system in more than 75% of the tests, while 20% used it in less than 50% of the tests (Figure 2(b)).

Cecal withdrawal timer usage. The CWVT was used in 67% of the tests performed from its introduction to the end of the study. (a) The proportion of tests performed with the cecal withdrawal timer in each month during the period following its introduction. (b) The proportion of tests performed with the cecal withdrawal timer by each endoscopist during the period following its introduction. Each letter denotes a different endoscopist.
Among procedures using the CWVT, the cecal withdrawal time was longer than 6 min in 91.2%, with a median withdrawal time of 8.7 min (6.9–12.0). When procedures with activated CWVT were stratified by withdrawal time length, the ADR was 14.2% for the lowest quartile, progressively increasing to 17.4%, 34.1%, and 47.3% in the subsequent quartiles. Age, sex, and bowel preparation distribution did not differ between procedures performed before and after CWVT introduction, whereas endoscopist experience (using a 5-year threshold) and after-hours procedures were more prevalent following CWVT introduction. The latter was unrelated to CWVT introduction but rather to an institutional increase in after-hours sessions (32.2% vs 37.5%, p = 0.006; Supplemental Table 2).
For the primary outcome, the collective ADR was 25.5% post-CWVT compared to 26.2% during the pre-CWVT period (p = 0.71), indicating a lack of overall improvement (Figure 3(c)). When calculating ADR adjusted for patient age, colonoscopy timing (daytime vs after-hours), and endoscopist experience (using a 5-year threshold), the results remained consistent: 25.6% in the post-CWVT period versus 26.1% in the pre-CWVT period. Notably, in this multivariable model, patient age, colonoscopy timing, and endoscopist experience were significantly associated with adenoma detection, whereas the study group (pre- vs post-CWVT) was not. When limiting the post-CWVT period to the last 5 months due to higher CWVT usage, the collective ADR was also not higher compared to the pre-CWVT period (23.5% vs 26.2%, respectively, p = 0.24). In addition, a sensitivity analysis stratified by CWVT usage yielded consistent results with no ADR improvement in either frequent (pre-CWVT ADR = 28.8%, post-CWVT ADR = 28.9%, p = 0.97) and infrequent users (pre-CWVT ADR = 24.6%, post-CWVT ADR = 22.4%, p = 0.38). Notably, we found a marked ADR variability between different months, irrespective of CWVT use, which may affect the results of this analysis (Supplemental Table 4).
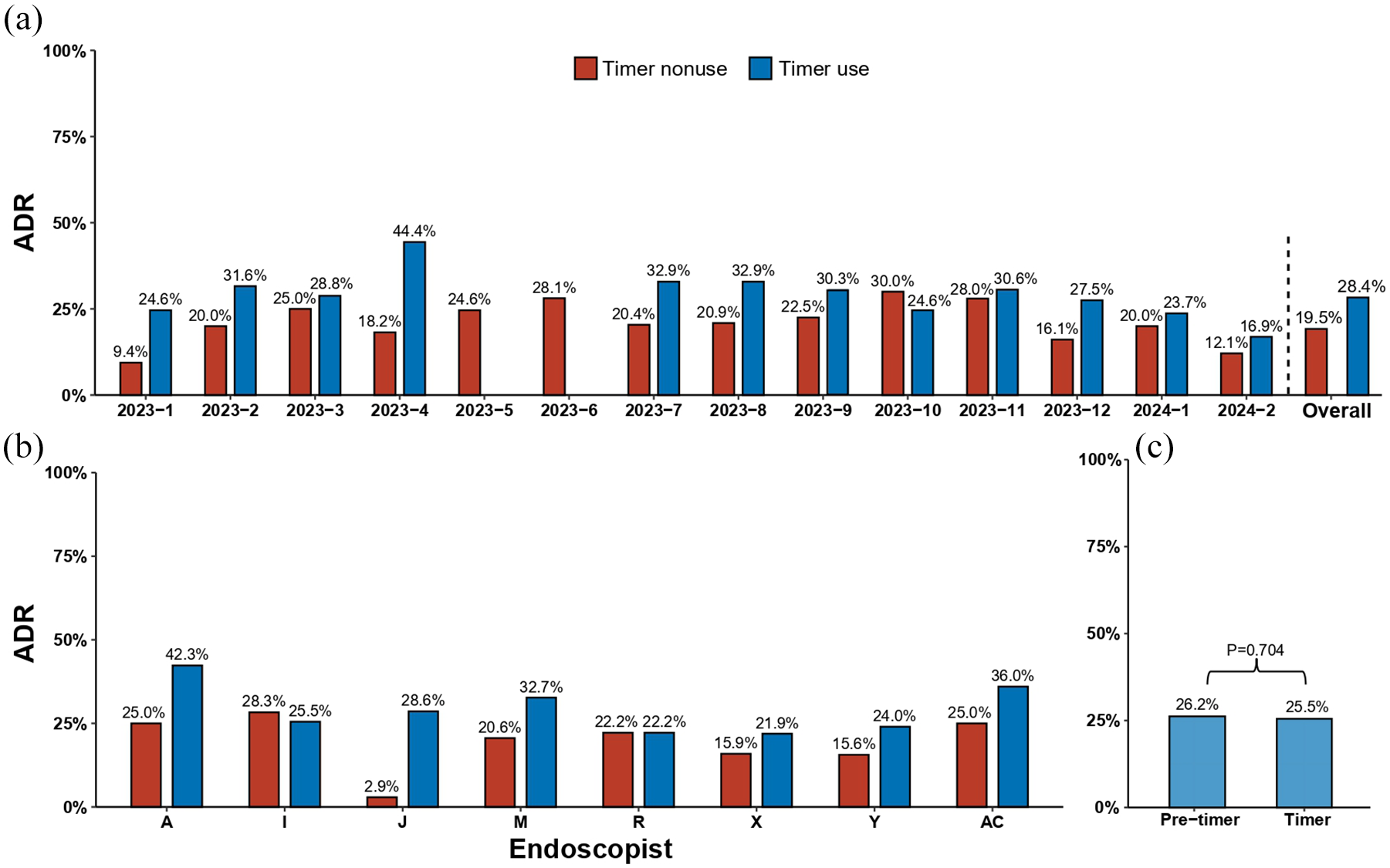
Changes in the ADR with the cecal withdrawal timer. (a) The ADR of colonoscopies performed with and without the cecal withdrawal timer during the period after its introduction. (b) The ADR of different endoscopists with and without the cecal withdrawal timer during the period after its introduction. Only endoscopists who performed at least 15 colonoscopies with and 15 colonoscopies without the cecal withdrawal timer during this period were included. (c) The overall ADR of the department before and after the introduction of the cecal withdrawal timer.
In the post-CWVT period, age, sex, bowel preparation quality, and endoscopist experience were distributed similarly between procedures with and without activated CWVT, while after-hours procedures were more prevalent among procedures without CWVT activation (32.7% vs 47.6%, respectively, p < 0.001; Supplemental Table 3). During the post-CWVT period, the ADR of procedures using the CWVT was 28.4% compared to 19.5% in those who did not (p < 0.001). When stratifying by months, the ADR of procedures with activated CWVT was higher in 11 out of 12 months included in the analysis, compared to procedures in which the system was not activated (Figure 3(a)). To assess for potential confounders of different CWVT usage by endoscopists with high and low detection rates, we calculated the correlation between baseline ADR (i.e., pre-CWVT) and CWVT usage frequency during the post-CWVT period and found it to be nonsignificant (p = 0.59; Supplemental Figure 1). The association between colonoscopy timing and ADR was also examined as a potential confounder and found to be nonsignificant (p = 0.21).
Of 627 colonoscopies in which adenomas were detected, 559 (89.2%) tests detected only adenomas smaller than 10 mm, 57 (9.1%) detected at least 1 adenoma larger than 10 mm, while data were unavailable in 11 (1.7%) tests. The detection rate of adenomas smaller than 10 mm was 25.7% for CWVT users compared to 17.5% among non-users (p = 0.001). The detection rate of adenomas larger than 10 mm was 2.2% for CWVT users compared to 1.8% among non-users (p = 0.79), suggesting that ADR improvement with CWVT usage was mainly driven by the detection of smaller adenomas.
We further analyzed the ADR of different endoscopists. For this purpose, we included endoscopists who performed at least 15 colonoscopies with and 15 without the CWVT during the post-CWVT period, resulting in 8 endoscopists. Six of these eight endoscopists improved their ADR with CWVT activation, and one had a stable ADR (Figure 3(b)). Notably, the single endoscopist who did not improve his ADR had the highest baseline ADR (28%). Lastly, we calculated the ADR among procedures with activated CWVT stratified by withdrawal time quartile. The ADR was 14.2% for the lowest quartile of withdrawal time length, progressively increasing to 17.4%, 34.1%, and 47.3% in the subsequent quartiles.
Discussion
Given that longer withdrawal time in screening colonoscopies is associated with higher ADR, we developed the CWVT to improve compliance with the recommended minimal withdrawal time and thereby potentially enhance adenoma detection.9,12 However, in this retrospective study of a high-volume medical center, the overall ADR of the gastroenterology department did not improve following the introduction of the CWVT compared to the previous year. Notwithstanding, in the post-CWVT period, the ADR was higher in procedures with CWVT being activated, compared to those in which it was not, particularly for the detection of adenomas smaller than 10 mm. The improvement was consistent across 11 out of 12 months included in this period and among six out of eight different physicians. While overall ADR improvement was not achieved following the CWVT introduction, the observed ADR improvements upon CWVT activation warrant further prospective study.
In this study, the primary endpoint of improving the Unit’s collective ADR from the pre-CWVT to the post-CWVT period was not met. Since the withdrawal time is not available for procedures without the CWVT, we cannot conclude whether it successfully prolonged the mean withdrawal time or eliminated overtly short withdrawal habits. Previous studies of potential interventions have also shown that improving mean ADR might be challenging. Enhanced visualization tools, such as magnification endoscopy and chromoendoscopy, demonstrated only a modest increase in ADR compared with high-definition colonoscopy.13,14 Likewise, most of the studies of novel endoscopes, such as wide-angle colonoscopes, did not find a significant ADR improvement with their use.14,15 More recently, studies assessing the efficacy of computer-aided diagnosis systems mostly reported performance enhancement, but some yielded mixed results.16–18 However, previous interventions directed at prolonging the withdrawal time by monitoring withdrawal time, increasing endoscopists’ awareness, and implementing a mandatory minimal withdrawal duration mostly report an ADR improvement following the intervention and inspired us to develop this new tool.8–10 Vavricka et al. 9 conducted a two-stage trial in which they monitored withdrawal time by a nurse, first without and then with the endoscopist’s awareness. They found a significant increase in withdrawal time when endoscopists were aware of being monitored, accompanied by a significant improvement in the ADR from 21.4% to 36.0%. By contrast, the CWVT tool is activated by a vocal command of the endoscopist without reliance on nurse assistance. In addition, it not only measures withdrawal time with endoscopist awareness but also displays the elapsed time from cecal intubation and announces each minute. This further enhances monitoring consciousness and facilitates real-time adjustments to the withdrawal pace.
Additional factors to consider when interpreting the primary endpoint analysis are submaximal CWVT usage and potential confounders. The CWVT was used in 67% of the procedures performed throughout the post-CWVT period, and, therefore, a potential benefit might have been diluted by submaximal usage. Notably, in the sensitivity analysis, the adjusted ADR also did not improve in either frequent or infrequent CWVT users. The incomplete adoption of novel tools by endoscopists should be considered in future implementation programs and study designs, and active measures should be taken to enhance their use by physicians. Furthermore, marked ADR variability between different months was noted irrespective of CWVT use. Therefore, the relatively higher ADR in the comparator group (i.e., during 2022) may mask potential improvement. Previous studies have identified a high level of ADR variability in the control groups of randomized colonoscopy trials as a possible source of bias. 19 Various causes have been suggested for this variability, including population characteristics, endoscopists’ skills, and possible operator-dependent bias.19,20 In our study, age and sex, which have been linked to ADR, did not significantly differ between the pre- and post-CWVT periods.21,22 However, morning colonoscopies were more common, and a higher proportion of procedures were performed by an experienced endoscopist before the CWVT introduction. While it has been suggested that ADR may be higher during the morning hours, 23 an ADR adjusted for colonoscopy timing was comparable to the crude measure.
Assessment of tests with and without the CWVT during the post-CWVT period revealed improved ADR with CWVT being activated. The improvement was mainly driven by increased detection of adenomas smaller than 10 mm, similar to previous studies that assessed the effect of longer withdrawal time on the ADR.6,10 Furthermore, ADR improvement was achieved by six out of eight physicians, while the single physician with an ADR reduction had the highest baseline ADR (28.3%). These findings are consistent with previous studies, which found that the primary utility of interventions to prolong withdrawal time may be in enhancing the performance of endoscopists with lower ADRs.2,10 Nevertheless, uncontrolled confounders should be considered when interpreting the results. The groups in this analysis were not randomly allocated but were instead formed due to the inactivation of the CWVT upon initiating colonoscopy. Although physicians were instructed to use the CWVT, it was not activated in 33% of procedures during the post-CWVT period, likely as part of an implementation and adjustment phase. However, other factors related to patient characteristics may have also influenced inactivation, potentially introducing confounding by indication. While these limitations should be considered, the observed ADR improvement in procedures using the CWVT during the post-CWVT period suggests its potential as a tool for enhancing adenoma detection and improving screening colonoscopy performance.
Limitations
Several limitations of our study should be acknowledged. First, the withdrawal time is not available for procedures without the CWVT, and, therefore, we cannot determine whether it successfully prolonged the mean withdrawal time. Hence, clinical endpoints were chosen for the study—namely adenoma detection. Second, submaximal usage of the CWVT during the post-CWVT period might have diluted potential benefits. Third, given the retrospective nature of the study, unaccounted-for confounders could affect the observed results. Marked ADR variability between different months was noted irrespective of CWVT use, supporting potential uncontrolled confounders. Differences in morning colonoscopy proportions and endoscopist experience between study groups may also have affected the results, although they remained consistent following adjustment with a regression model. Likewise, colonoscopies performed without activating the CWVT in the post-CWVT period are subjected to indication bias. While inactivation of CWVT in some of the colonoscopies is expected as part of the implementation phase, it may also be associated with certain patients or procedure characteristics.
Conclusion
The overall ADR of the gastroenterology department did not improve following the introduction of the CWVT. However, in the post-CWVT period, the ADR was higher in procedures with CWVT activation compared to those without, particularly in the detection of adenomas smaller than 10 mm. The improvement was observed consistently across most months of the study and among most endoscopists. Further prospective studies are required to assess the effectiveness of the CWVT in improving adherence to the withdrawal time recommendations, enhancing adenoma detection, and decreasing interval CRC.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251341752 – Supplemental material for Evaluation of the cecal withdrawal vocal timer in screening colonoscopies for optimizing withdrawal time and adenoma detection rate
Supplemental material, sj-docx-1-tag-10.1177_17562848251341752 for Evaluation of the cecal withdrawal vocal timer in screening colonoscopies for optimizing withdrawal time and adenoma detection rate by Adam Goldman, Alon Lang, Asaf Levartovsky, Idan Levy, Ido Laish, Shomron Ben-Horin and Uri Kopylov in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.