
Abstract
Background:
Recently, the ENDOANGEL (EN) system, a computer-assisted detection technique, and water exchange (WE) assisted colonoscopy have both been shown to increase the colorectal adenoma detection rate (ADR).
Objectives:
The aim of this study was to compare the ADR between EN- and WE-assisted colonoscopy.
Design:
This was a retrospective study.
Methods:
Data from patients who underwent either EN- or WE-assisted colonoscopy between October 2021 and August 2022 were analysed consecutively. The primary outcome measure was the ADR.
Results:
The ADR was found to be similar between the EN and WE groups, with 80 out of 199 (40.2%) patients in the EN group compared to 78 out of 174 (44.8%) patients in the WE group [1.21; 95% confidence interval (CI), 0.80–1.83]. In the analysis using stabilized inverse probability treatment weighting after adjustment for confounding factors, both colonoscopy methods had similar performance in terms of ADR (1.41; 95% CI, 0.88–2.27).
Conclusion:
EN was found to be comparable to WE in terms of ADR during colonoscopy, and both methods may be effectively used in clinical practice.
Introduction
Effective colonoscopy plays a vital role in detecting colorectal adenomas and substantially reducing colorectal cancer incidence and mortality.1,2 Miss rates for colorectal adenomas during colonoscopy range from 6% to 27%, depending on adenoma and operator characteristics. 3 As endoscopic technology has significantly improved, more attention has been paid to improving the quality of colonoscopy by utilizing new endoscopic strategies, including technical and cognitive aspects.4,5
In recent years, computer-aided detection (CADe) systems based on artificial intelligence (AI) have been used in colonoscopy.6,7 Deep learning CADe systems have proved to be effective in real-time detection and differentiation of colorectal lesions.6,8 A large population-based prospective study showed that a real-time CADe system-assisted colonoscopy significantly elevated the adenoma detection rate (ADR) to 29.1%. 9 One of the currently developed CADe systems is ENDOANGEL (EN), which can detect lesions in real time and has been widely used for the detection and diagnosis of gastrointestinal diseases, including early gastric cancer, gastric neoplasms and gastroesophageal variceal bleeding.10–12 Zhou et al. 13 confirmed that EN can accurately assess bowel preparation status and can be reliably used in clinical settings. A recent study showed that the yield of colorectal adenomas was significantly improved by EN, which can monitor the adenoma in real time, synchronized with colonoscopy. 4
The water exchange (WE) method of colonoscopy is one of the water-assisted colonoscopies and is characterized by the airless introduction, infusion and aspiration of water, residual air pockets and faeces to achieve maximum cleanliness and minimum insertion pain during colonoscope insertion into the cecum. 14 Previous studies have shown that WE significantly improves ADR from 38% to 57.1%, particularly in the detection of diminutive lesions in the proximal colon, ranging from 28.3% to 41.8%.14–16 A multicentre prospective trial showed that WE could significantly improve ADR compared to air insufflation in screening patients aged over 50 years. 17
Although both EN and WE can improve ADR, there is currently no report on which colonoscopy method is superior in ADR. Thus, we aimed to compare the ADR in patients undergoing colonoscopy using the EN and WE methods.
Methods
Patients
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 18 A retrospective study was conducted at Yijishan Hospital of Wannan Medical College between October 2021 and August 2022. Consecutive patients aged 18 years and above who underwent colonoscopy screening, surveillance and diagnosis assisted with either EN (EN group) or WE (WE group) were included in this study. Exclusion criteria were as follows: polyposis syndrome, inflammatory bowel disease, colorectal cancer, history of colorectal resection, known or suspected intestinal obstruction or perforation, total Boston Bowel Preparation Scale (BBPS) score less than six points or any segment with a score less than two points. All patient details have been de-identified.
Two certified endoscopists with more than 100 colonoscopies of experience in WE and 2500 in EN performed the colonoscopies,4,17 using an Olympus Optical colonoscope (GIF-H290; Olympus, Tokyo, Japan). All patients underwent bowel preparation with polyethylene glycol-electrolyte split dose following instructions. Basic demographic information and a history of abdominal or pelvis surgery were collected. Patients were sedated using propofol or midazolam and fentanyl. 19
In the WE group, the air pump was turned off before the colonoscopy started. Pre-warmed normal saline (between 25°C and 37°C) was infused using flushing pumps, and the opaque water as well as the residual air pockets and faeces were suctioned during the insertion phase.20,21 In the EN group, colonoscopy was performed as usual with air insufflation to distend the lumen as required, with lesions monitored in real time using the EN. 4 Visualization of the appendiceal orifice and ileocaecal valve indicated caecal intubation. 22 Insertion and withdrawal times were recorded. The BBPS score was used to evaluate the quality of the bowel preparation during withdrawal. 23 Diminutive polyps were removed directly for pathological examination during withdrawal after obtaining informed consent from the patients, otherwise polyps were removed on admission.
Confounders and study endpoints
Confounders were as follows: age, sex (male/female), body mass index (BMI), withdrawal time, BBPS score and sedation status (no/yes). The primary outcome was the ADR, defined as the proportion of subjects with at least one adenoma of any size. 17 Serrated lesions were classified into the adenoma group, while non-adenomatous polyps were defined as the hyperplastic group. 24 The secondary outcomes were the number of adenomas per colonoscopy (APC) 25 and the total (excluding intervention times) time of colonoscopy.
Statistical analysis
Categorical data were analysed using chi-square or Fisher’s exact test, as appropriate, and continuous data using Student’s t-test or Mann–Whitney U test. Multivariable logistic regression was employed to assess the performance of both methods on ADR (primary analysis). In addition, we used the propensity-score method to reduce the effect of confounding. The individual propensities to receive WE were assessed using a multivariable logistic model with covariates of age, sex, BMI, withdrawal time, insertion time, sedation status (no/yes) and history of previous abdominal or pelvis surgery (no/yes). In the inverse-probability-weighted analysis, the predicted probabilities from the propensity-score model were used to calculate the stabilized inverse probability treatment weighting (sIPTW) weight. 26 Subgroup analyses were conducted in the cohort with a BBPS score of ⩾7 or withdrawal time of ⩾6 min. Statistical analysis was performed using SPSS 26.0 software (SPSS Inc., Chicago, IL, USA) and R version 4.0.2 (The R Foundation for Statistical Computing, Vienna, Austria) with significance set at p < 0.05.
Results
Baseline characteristics
We collected information on a total of 442 patients who underwent EN- or WE-assisted colonoscopy. Ultimately, 373 eligible patients were included in our study (Figure 1). The distribution of baseline patient characteristics by colonoscopy method is shown in Table 1. In the unmatched cohort, there were significant differences in sex, age, BMI, insertion time, BBPS and previous abdominal or pelvis surgery. Patients who underwent WE had significantly longer mean insertion time and higher BBPS scores than the EN group (p < 0.001). The propensity-score model’s C-statistic for sIPTW analysis was 0.813. After sIPTW, in the matched cohort, there was no significant difference in all covariates (except BBPS) between the two groups.

Flow chart of the patient selection process.
Characteristics of patients receiving EN or WE, before and after stabilized inverse probability of treatment weight matching.
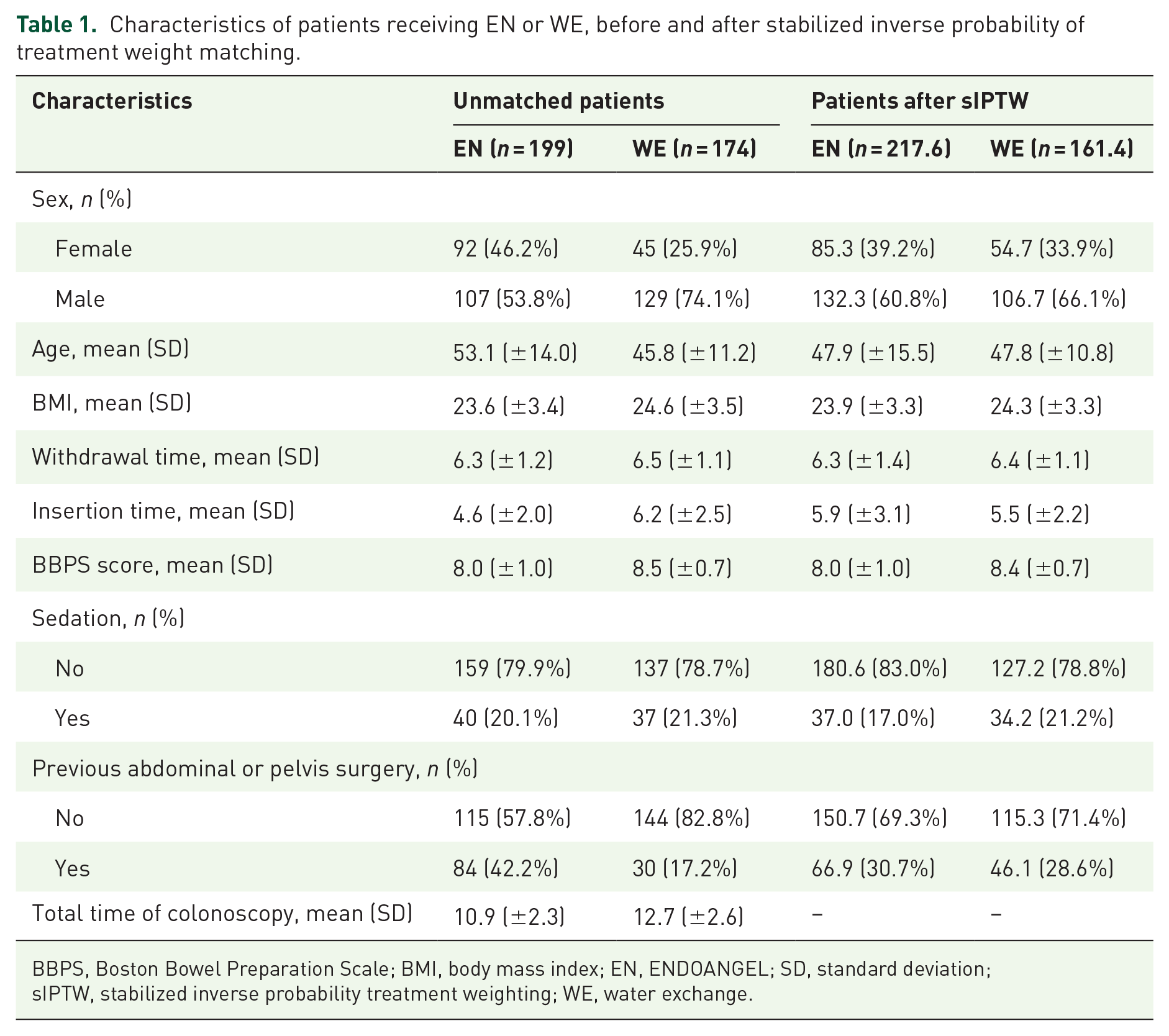
BBPS, Boston Bowel Preparation Scale; BMI, body mass index; EN, ENDOANGEL; SD, standard deviation; sIPTW, stabilized inverse probability treatment weighting; WE, water exchange.
Outcomes
In terms of primary outcome, the overall ADR was 40.2% for EN and 44.8% for WE (p = 0.37). The ADR was not significantly different between the two groups stratified by age, sex, sedation status and withdrawal time (Table 2). In the crude analysis, there was no significant association between ADR and patients who received the two different methods of colonoscopy [odds ratio (OR), 1.21, 95% confidence interval (CI), 0.80–1.83]. In the propensity score analysis with sIPTW, after adjusting for confounders, both colonoscopy methods showed similar performance in terms of ADR (OR, 1.41; 95% CI, 0.88–2.27) (Table 3). In terms of secondary outcomes, patients who underwent WE had a significantly longer mean total time of colonoscopy compared to the EN group (p < 0.001). However, there was no significant difference in APC between the two groups.
Comparison of ADR in patients in the EN and WE groups.

The ADR was calculated as the proportion of subjects with at least one adenoma.
ADR, adenoma detection rate; APC, adenomas per colonoscopy; EN, ENDOANGEL; WE, water exchange.
Associations of two different colonoscopy methods with adenoma detection in crude, multivariable and propensity score analyses.

Shown is the odds ratio from the multivariable logistic model, adjusting for confounding factors (age, sex, BMI, withdrawal time, BBPS and sedation status) with inverse probability weighting according to the propensity score. The analysis included all patients.
Shown is the odds ratio from the multivariable logistic model, adjustment for confounding factors (age, sex, BMI, withdrawal time, BBPS and sedation status). The analysis included 355 patients.
Shown is the odds ratio from the multivariable logistic model, adjustment for confounding factors (age, sex, BMI, withdrawal time, BBPS and sedation status). The analysis included 293 patients.
BBPS, Boston Bowel Preparation Scale; BMI, body mass index; CI, confidence interval; EN, ENDOANGEL; WE, water exchange.
Subgroup analyses
Two subgroup analyses, including patients with a BBPS score of ⩾7 or withdrawal time of ⩾6 min, yielded similar results consistent with the sIPTW analysis (Table 3).
Discussion
ADR has been shown to be associated with the incidence of interval colorectal cancer and cancer-related deaths, 27 indicating that improvements in ADR can lead to a lower risk of both outcomes.28–30 This finding inspired us to develop novel methods to increase ADR. Studies have suggested that AI can help increase ADR and polyp detection rates.8,31,32 EN, an AI system, is effective in increasing ADR during colonoscopy. 4 In addition, the use of WE during colonoscopy has been found to significantly increase ADR.33–35 However, it is unclear which method is more effective for detecting ADR, and this was the focus of our study.
Our study showed that the ADR was similar for both the EN and WE groups (40.2% versus 44.8%; OR, 1.21; 95% CI, 0.80–1.83). A recent randomized trial demonstrated that AI-assisted colonoscopy can increase ADR to 54.8% compared to the control group (40.4%). 6 Another study found that AI-assisted colonoscopy increased the overall ADR by 7.5% compared to the control group (39.9% versus 32.4%). 36 AI has also been shown to decrease the miss rate of sessile serrated lesions and increase the number of APC. 8 As for WE, one study found that the ADR was significantly higher when using WE compared to traditional air insufflation (49.6% versus 39.5%). 37 In addition, WE has been found to significantly improve ADR in patients sedated with propofol. 38
Although we found no difference in ADR between the EN and WE groups, the way by which these two methods improve ADR is different. In the WE group, we found that the BBPS score (8.5 ± 0.7) was high, likely due to enhancing bowel cleanliness from using WE during insertion, making small flat lesions easier to detect. 24 In addition, the use of WE reduces multitasking and attention switching during withdrawal, allowing colonoscopists to better focus on finding lesions. 29 In the EN group, the high detection of ADR due to real-time lesion detection and withdrawal speed monitoring, reduced human error and increased the likelihood of detecting diminutive adenomas that may have been missed with visual inspection alone.36,39
Regarding EN, we found that the total examination time, especially the insertion time, was shorter than in the WE group. EN also helps to attenuate variations in the cognitive and technical abilities of endoscopists, improving reproducibility, fidelity and uniformity in bowel lesion detection.4,9,39 Furthermore, EN can monitor the withdrawal speed and time in real time, an important quality indicator for colonoscopy examinations. 4 However, the cost of EN may be prohibitive for some hospitals, particularly medium- and small-sized hospitals, limiting its applicability in clinical practice. By contrast, WE is a relatively low-cost method that requires no special equipment, making it a more feasible option for widespread use in clinical practice. In addition, WE-assisted colonoscopy has been found to improve caecal intubation rate and reduce patient pain scores in unsedated colonoscopy compared to air insufflation colonoscopy. 40 In terms of training costs, the EN system would show original colonoscopy videos as well as the insertion and withdrawal process when connected to the colonoscopy host. This system was easily understandable for experienced colonoscopists (more than 1500 prior experiences in general); thus, no additional training costs were required. 4 However, WE-assisted colonoscopy requires endoscopists with experience and proficiency in the technology. Additional training time may be necessary, although the learning curve for an experienced colonoscopist using the WE is not steep and the technology is relatively easy to learn.41,42
Our study has some limitations. Firstly, it was a retrospective study; therefore, selection bias is inevitable. Secondly, the ADR of WE was numerically higher than that of EN. The difference was not significantly likely because of the small sample size (type II error). Thirdly, our findings should be validated in future large-scale multicentre clinical trials. Fourthly, further research is needed to investigate whether combining WE with EN can improve ADR.
In conclusion, the EN group demonstrated comparably effective ADR compared to the WE group. Considering that EN and WE have specific advantages, we believe that both EN- and WE-assisted colonoscopies may be implemented in current clinical practice based on the specific situation of different hospitals.