
Abstract
Background:
Pre-procedural anxiety is known to impact the quality of upper gastrointestinal endoscopy (esophagogastroduodenoscopy, EGD), particularly in non-sedated patients. Elevated anxiety levels can cause discomfort and reduce procedural success.
Objectives:
This study aimed to evaluate the effect of pre-procedural anxiety, measured by the State-Trait Anxiety Inventory (STAI), on the quality of EGD and to determine whether anxiety levels can predict the need for sedation.
Design:
This was a prospective, cross-sectional study conducted at a tertiary care hospital.
Methods:
This study included 1344 non-sedated patients aged 18–90 years undergoing EGD at Ankara Etlik City Hospital (September 2023–March 2024). Anxiety levels were assessed using STAI before the procedure. Receiver operating characteristic (ROC) analysis determined the optimal STAI-I cutoff for predicting sedation needs. EGD quality was evaluated by examination thoroughness and biopsy adequacy. Logistic regression identified predictors of unsuccessful procedures.
Results:
The mean participant age was 50.6 years; 47.8% were male. The average STAI-I score was 42.14. ROC analysis identified an STAI-I cutoff of 36, above which unsuccessful procedures were more likely (area under the curve = 0.720, p < 0.001). Higher STAI-I and STAI-II scores were independent predictors of unsuccessful endoscopy, with each unit increase in STAI-I raising the odds by 3.8%.
Conclusion:
Pre-procedural anxiety, as measured by STAI, significantly affects non-sedated EGD quality. An STAI-I cutoff of 36 predicts the need for sedation. Routine anxiety assessment could enhance sedation strategies, patient satisfaction, and procedure quality.
Plain language summary
Keywords
Introduction
Esophagogastroduodenoscopy (EGD) is an essential procedure for diagnosing and treating many gastrointestinal conditions. Despite its benefits, EGD often causes significant anxiety in patients. 1
Anxiety can lead to various adverse outcomes during medical procedures by altering physiological responses and affecting patient comfort. For instance, increased sympathetic nervous activity can elevate heart rate and reduce heart rate variability, increasing the risk of sudden cardiac events.2,3 Furthermore, elevated anxiety levels result in a notable elevation in respiratory rate. 4 Anxiety affects respiratory patterns by reducing respiratory time and increasing the rate, leading to prolonged expiration and shortened post-expiratory pauses. 5 In addition, it can heighten pain perception and muscle tension, making cooperation difficult and often necessitating higher sedative doses. 6 These hemodynamic and respiratory changes can lead to complications during EGD. Anxiety-induced tachycardia and hypertension may hinder esophageal and stomach navigation, complicating the procedure. Elevated respiratory rates can cause excessive movement, impairing image quality and diagnostic accuracy. Anxiety-induced hyperventilation, with rapid and shallow breathing, may cause respiratory alkalosis, complicating patient management. Anxiety also increases discomfort and pain perception, making the procedure harder to tolerate.
Sedation practices vary significantly between countries and clinical settings. While some countries routinely use sedation during gastroscopy, others limit its use due to cost, safety concerns, and healthcare policies. 7 These differences create international variability in endoscopy practice, emphasizing the need for individualized sedation strategies based on patient-specific factors. While sedation is common in endoscopy, non-sedated procedures are frequent in some countries due to the cost and potential side effects of sedation, such as respiratory depression and cardiovascular complications. This raises the question of whether pre-procedural anxiety affects both patient experience and endoscopic quality.
The quality of EGD depends on factors like clear mucosal visualization, accurate lesion identification, adequate biopsy sampling, and efficient procedure time. Increased movement, hyperventilation, and discomfort in anxious patients may interfere with the thoroughness of the examination. Lack of patient cooperation may prolong the procedure, increasing the risk of complications or incomplete assessments.
Previous studies show a correlation between pre-procedural anxiety and adverse outcomes in non-sedated EGD patients. Anxiety is linked to increased discomfort, heightened pain perception, and reduced tolerance during the procedure.8 –10 In particular, women and younger patients report higher anxiety, leading to greater pain perception and the need for sedation. 11 However, no method currently exists to predict which patients should receive selective sedation.
The existing research on the effect of pre-procedural anxiety level on endoscopic imaging quality in non-sedated patients is limited. This study aims to elucidate the challenges that these patients may encounter during the procedure by examining the potential impact of pre-procedural anxiety and other potential risk factors on endoscopy quality in non-sedated patients. In addition, this study will assess the feasibility of utilizing anxiety levels prior to endoscopy in non-sedated patients to enhance patient satisfaction and procedural success during the endoscopic procedure.
Methods
Study design and patient population
This prospective, cross-sectional observational study was conducted in the Gastroenterology Clinic of Ankara Etlik City Hospital from September 2023 to March 2024. It included 1344 non-sedated patients aged 18–90 years and was designed in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 12 A study flow diagram (Figure 1) has been included to illustrate the study process, and the STROBE checklist has been provided as Supplemental Material 1. Patients were selected consecutively to ensure a systematic and unbiased inclusion process.
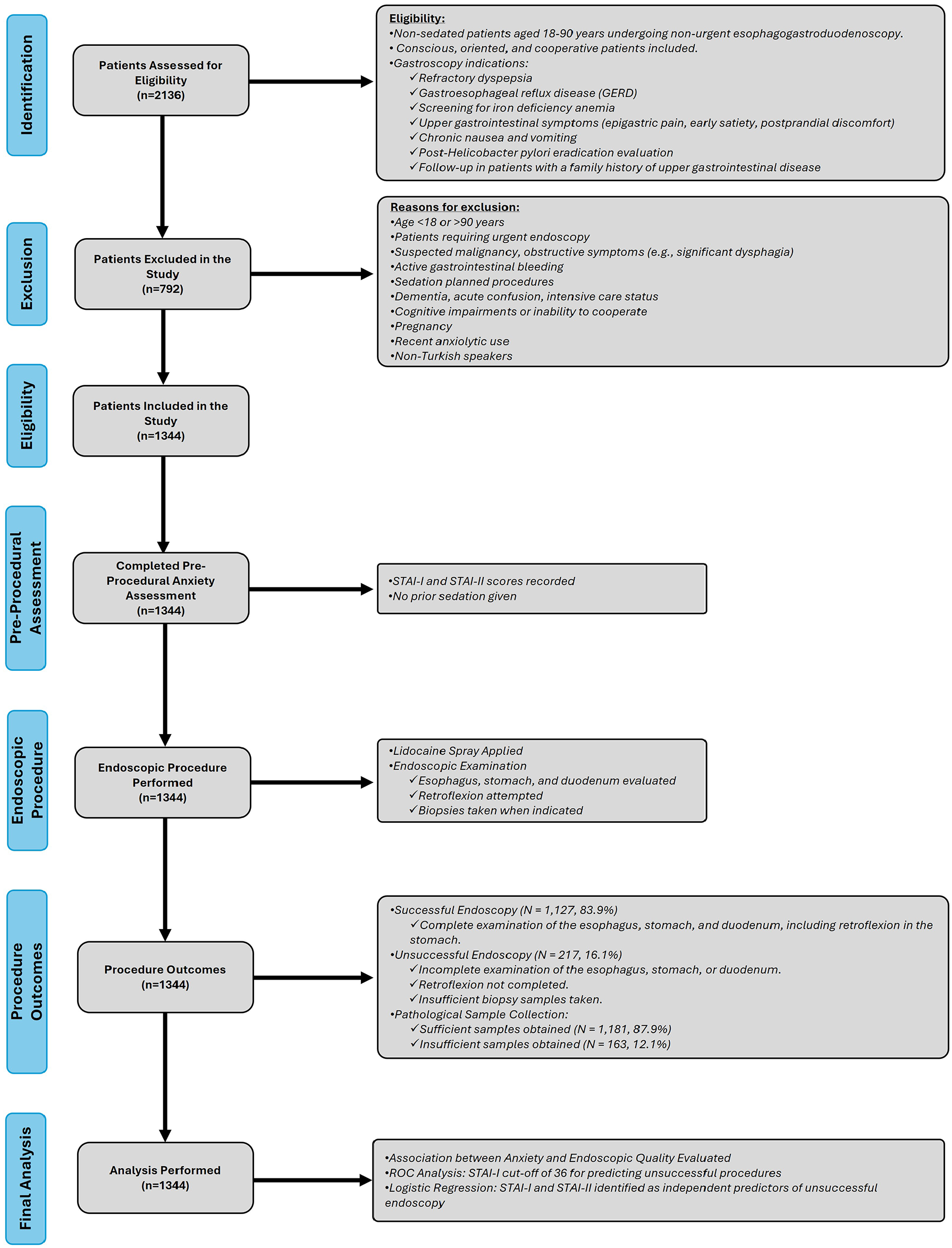
Study flow diagram.
Data collection and evaluation
Data were collected through face-to-face interviews with patients and endoscopists before and after the procedure. Demographic details, medical history, and past endoscopy experiences were documented. Anxiety levels were assessed using the Spielberger State-Trait Anxiety Inventory (STAI), comprising two subscales: STAI-I (state anxiety) and STAI-II (trait anxiety). Scores ranged from 20 to 80, with higher scores indicating elevated anxiety. Post-procedure data included discomfort levels and procedural quality (e.g., retroflexion and biopsy adequacy).
Anxiety measurement tools
The validated Turkish version of the STAI, assessing both state and trait anxiety, was administered prior to the endoscopy. 13 The STAI scale can be completed in approximately 10 min for both subscales (STAI-I and STAI-II). It is a practical tool that can be administered at the bedside and is feasible for routine clinical use. The original English version of the STAI questionnaire has been provided as Supplemental Material 2 for reference.
Inclusion and exclusion criteria
Participants were non-sedated patients between 18 and 90 years undergoing non-urgent EGD at the clinic, who were conscious, oriented, and cooperative. The indications for gastroscopy included refractory dyspepsia, gastroesophageal reflux disease (GERD), screening for iron deficiency anemia, upper gastrointestinal symptoms (e.g., epigastric pain, early satiety, postprandial discomfort), chronic nausea and vomiting, post-Helicobacter pylori eradication evaluation, and follow-up in patients with a family history of upper gastrointestinal disease.
Exclusion criteria included patients planned for sedated endoscopy, those with dementia, acute confusion, intensive care status, emergency procedures, cognitive impairments, refusal of consent, age under 18, pregnancy, non-Turkish speakers, and recent anxiolytic use. In addition, patients with suspected malignancy, those with obstructive symptoms (e.g., significant dysphagia), active gastrointestinal bleeding, and those requiring urgent endoscopy were excluded from the study.
Endoscopic procedure
Endoscopies were performed by experienced endoscopists, each conducting over 1000 procedures annually, ensuring consistent outcomes reflecting the true impact of anxiety. All patients received topical lidocaine spray before the procedure to improve tolerance and reduce discomfort. Endoscopy was initiated approximately 2–5 min after the application to allow sufficient anesthetic effect. To ensure an unbiased evaluation during the procedure, endoscopists did not have access to the patients’ STAI scores prior to endoscopy. This measure was taken to minimize the risk of observer bias.
Endoscopy quality assessment
The quality of endoscopic imaging was evaluated based on the number of biopsies obtained during the procedure, the clarity of images, and the reporting of pathological findings during endoscopy. A successful endoscopic procedure was defined as the ability to fully examine the esophagus, stomach, and duodenum, complete critical maneuvers such as retroflexion, and obtain adequate biopsies when necessary. Biopsies were taken at the discretion of the endoscopists, based on clinical judgment and observed mucosal pathologies; therefore, obtaining biopsies in all patients was not the primary aim. Biopsy adequacy was assessed based on the suitability of the samples for histopathological evaluation. A good biopsy was defined as a sample containing sufficient tissue and deemed diagnostically useful. Examination of the esophagus, stomach, and duodenum was assessed in terms of its thoroughness, along with the documentation of any observed lesions. In addition, parameters such as procedure duration and patient positioning were recorded.
Statistical analysis
The statistical methods used in this study are commonly employed for prospective, cross-sectional studies. Analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). The sample size was determined to be sufficient for generating statistically meaningful results. The normality of numerical variables was assessed with the Kolmogorov–Smirnov test. Normally distributed variables were reported as mean ± standard deviation, and comparisons were made using the independent samples t-test. Categorical variables were expressed as frequencies (percentages), with group comparisons conducted via the Chi-square or Fisher’s exact test. Logistic regression analysis was used to identify independent predictors of unsuccessful endoscopic procedures, beginning with univariate and followed by multivariate analysis. Receiver operating characteristic (ROC) curve analysis was employed to determine the optimal STAI-I cutoff score for predicting outcomes. A two-tailed p-value <0.05 was considered significant.
Results
The study included a total of 1344 patients, with an average age of 50.6 years (±20.54), and 47.8% of the participants were male. The mean body mass index of 25.2 kg/m² (±4.66). The participants’ systolic and diastolic blood pressure values averaged 126 mmHg (±21) and 65 mmHg (±15), respectively.
In terms of education, the majority of participants had completed at least high school, with 28.8% having a high school diploma and 40.7% holding a license or higher education degree. Comorbidities included hypertension (9.3%), diabetes (8.4%), and depression (6.2%), while anxiety and panic disorder prevalence were 4.4% and 4.5%, respectively.
The anxiety levels of the participants were assessed using the STAI, where the mean STAI-I score was 42.14 (±12.91) and the mean STAI-II score was 41.82 (±10.45). The participants were categorized into low, moderate, and severe anxiety groups based on their STAI-I and STAI-II scores. STAI-I classification showed 37.7% in low anxiety, 17.7% in moderate, and 44.6% in severe. Similarly, for the STAI-II scores, 34.4% were low, 25.6% moderate, and 40.0% severe (Table 1).
Demographic characteristics and descriptive statistics of the study population.
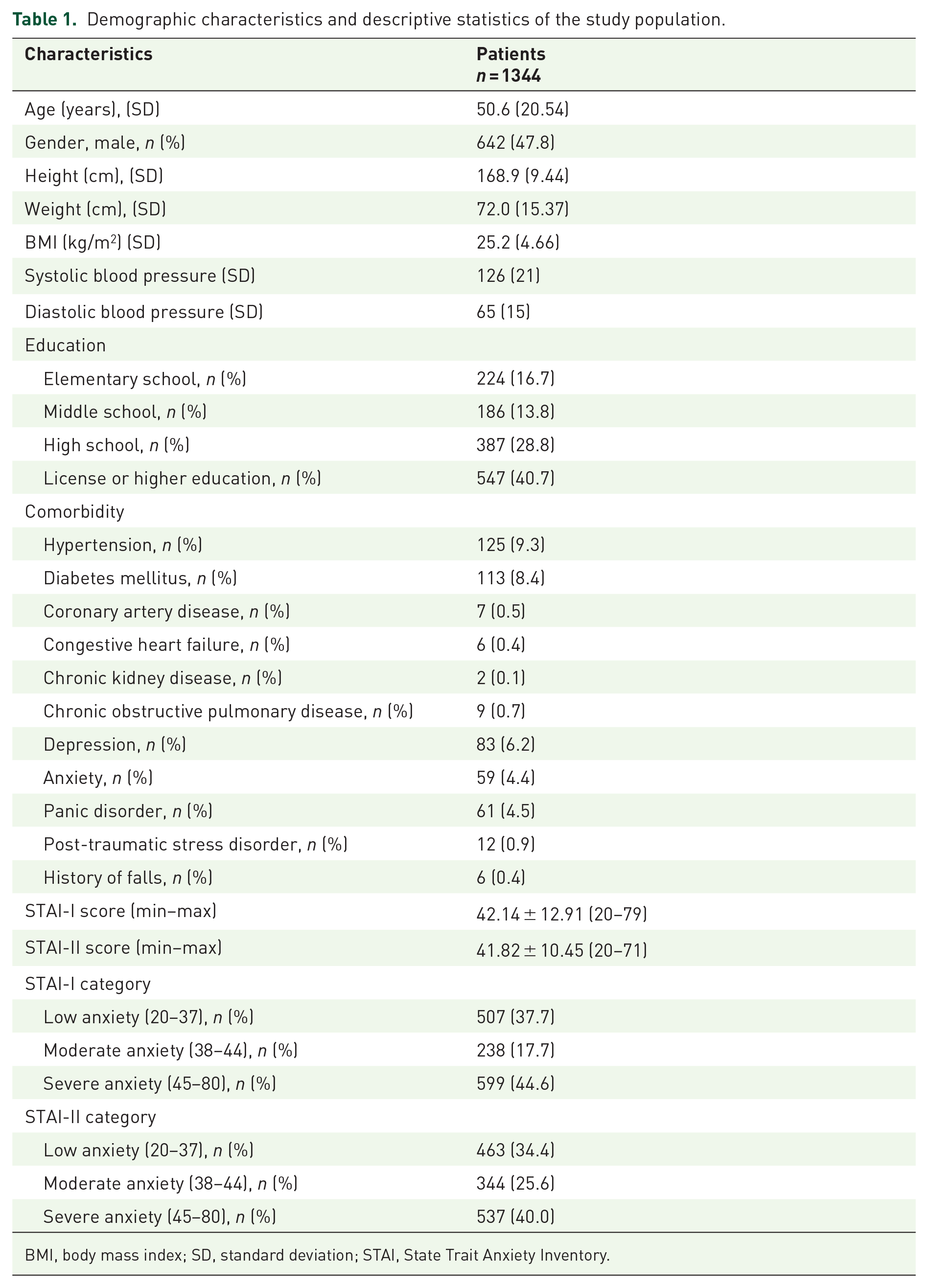
BMI, body mass index; SD, standard deviation; STAI, State Trait Anxiety Inventory.
The analysis shows a significant association between higher STAI scores and reduced thoroughness of endoscopic examinations, including retroflexion in the stomach (Table 2). Patients with severe anxiety (STAI-I) were less likely to undergo a thorough examination (66.4%) compared to those with low anxiety (11.1%). Similar trends were observed with STAI-II scores, where 63.1% of severely anxious patients had incomplete examinations compared to only 8.3% with low anxiety. Figures 2 and 3 illustrate that as anxiety levels increase, the likelihood of a thorough examination decreases, highlighting the impact of psychological factors on procedural quality. This suggests that higher anxiety levels are linked to less thorough endoscopic exams, potentially affecting procedural effectiveness and diagnostic outcomes.
Comparison of STAI scores based on the thoroughness of endoscopic examination.
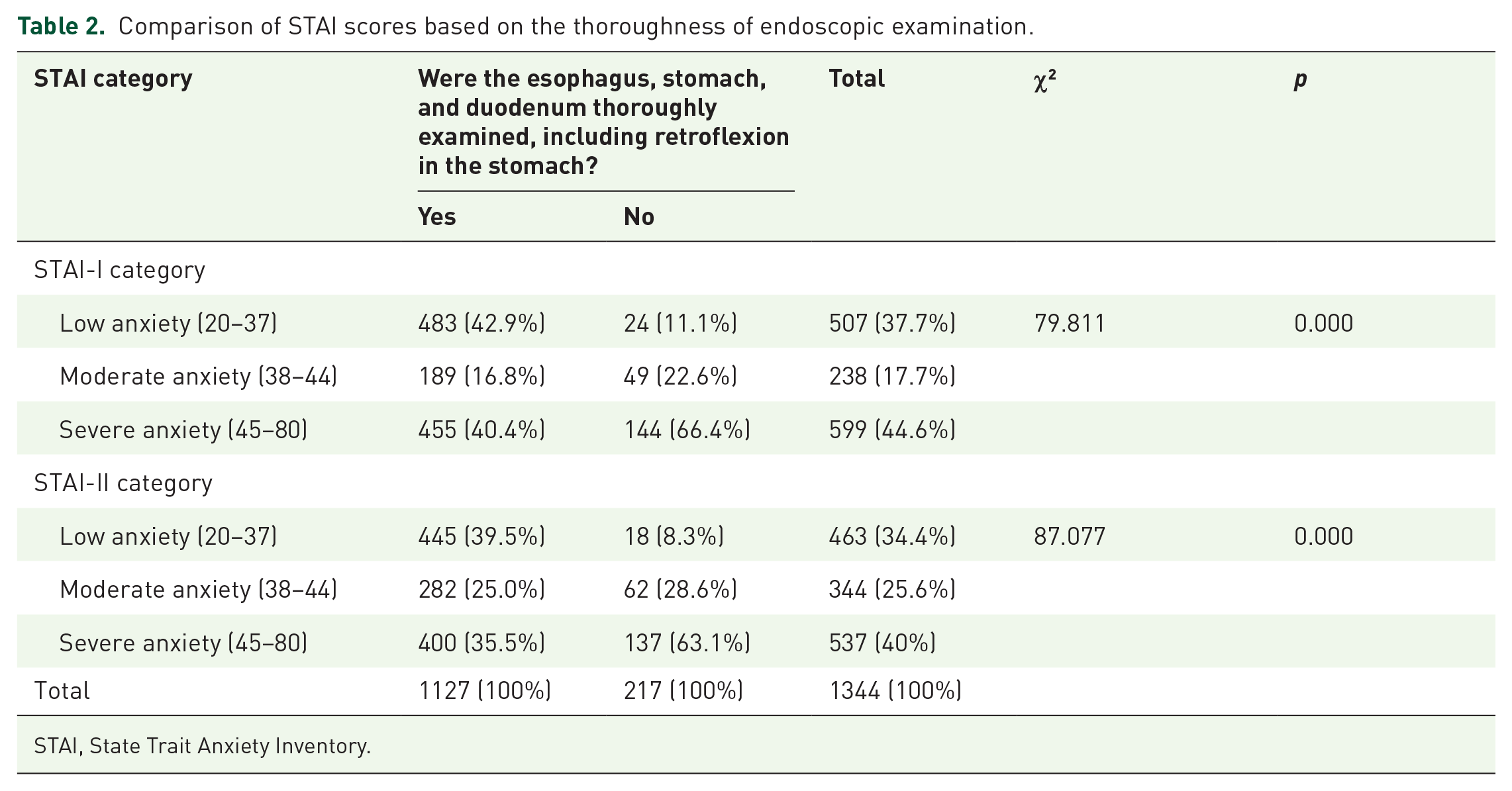
STAI, State Trait Anxiety Inventory.

Chi-square analysis of STAI-I categories and thoroughness of endoscopic examination.

Chi-square analysis of STAI-II categories and thoroughness of endoscopic examination.
In this study, 1344 patients underwent non-urgent upper gastrointestinal endoscopy. The primary indications for endoscopy included refractory dyspepsia (n = 367, 27.31%), GERD (n = 293, 21.79%), screening for iron deficiency anemia (n = 213, 15.85%), chronic nausea and vomiting (n = 159, 11.83%), post-H. pylori eradication evaluation (n = 118, 8.78%), and a family history of upper gastrointestinal disease (n = 74, 5.51%), while other less common indications accounted for 120 patients (8.93%).
To further investigate the potential impact of these indications on procedural success, a univariate analysis was performed to assess their association with unsuccessful endoscopy (i.e., incomplete visualization or inadequate biopsy collection). Patients undergoing endoscopy for GERD demonstrated a statistically significant increase in incomplete procedures (p = 0.027). Chronic nausea and vomiting showed a borderline association with procedure intolerance (p = 0.089). By contrast, refractory dyspepsia (p = 0.210) and screening for iron deficiency anemia (p = 0.477) did not appear to increase the likelihood of unsuccessful endoscopy. In addition, a family history of upper gastrointestinal disease was marginally associated with higher pre-procedural anxiety scores (p = 0.094), though this did not meet conventional statistical significance thresholds (p < 0.05).
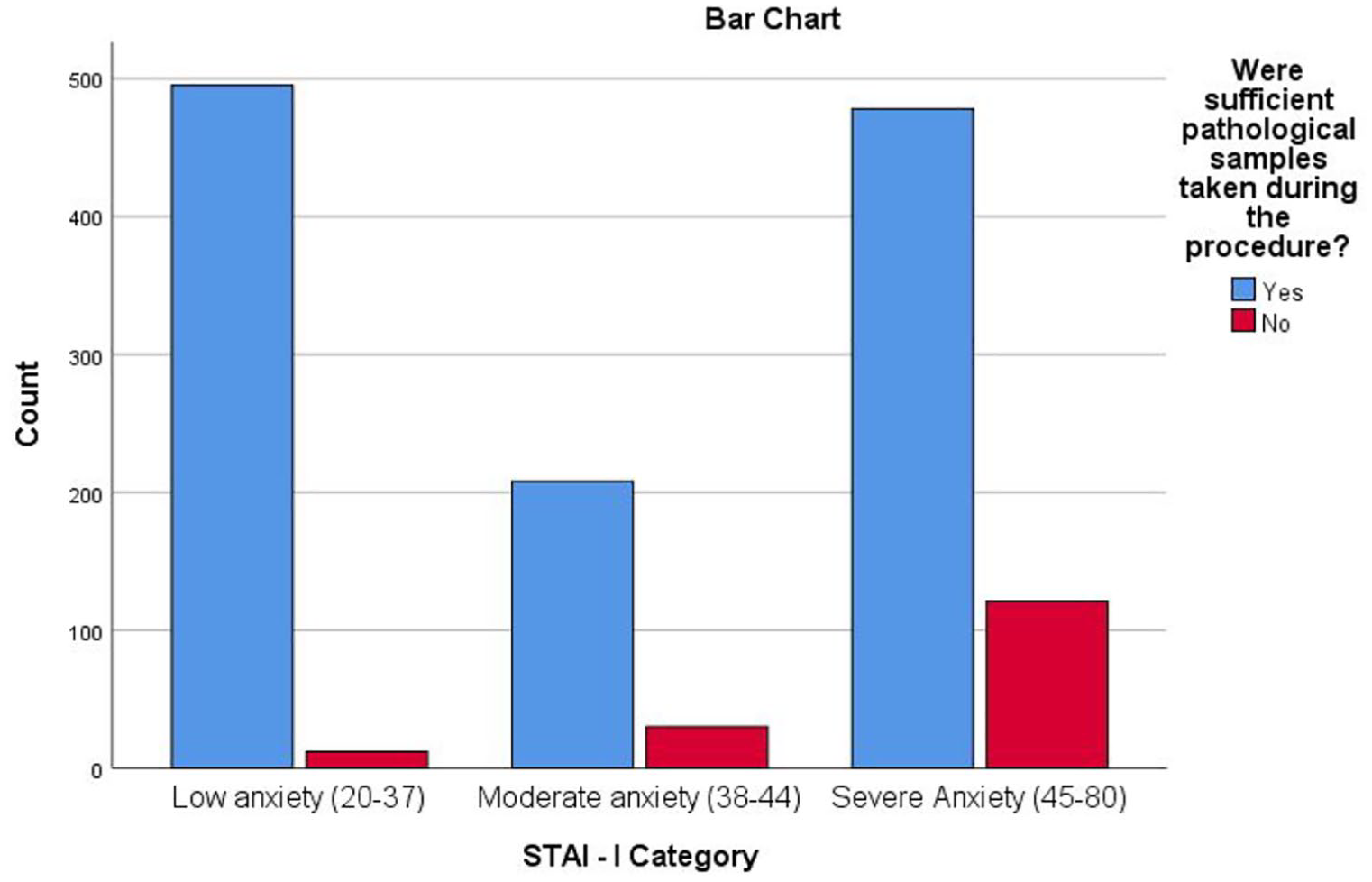
The relationship between anxiety levels and the adequacy of pathological samples, as shown in Table 3, reveals a significant correlation between higher anxiety and inadequate sample collection. Among patients with severe anxiety (STAI-I), 74.2% lacked sufficient samples, compared to 7.4% with low anxiety. A similar pattern is observed for STAI-II, where 73.0% of patients with severe anxiety had inadequate samples versus 8.0% in the low anxiety group. As illustrated in Figures 4 and 5, rising anxiety levels markedly decrease sample adequacy, emphasizing the need to manage anxiety for thorough examinations and proper sampling.
Comparison of STAI scores based on the adequacy of pathological samples collected.

STAI, State Trait Anxiety Inventory.
Chi-square analysis of STAI-I categories and adequacy of pathological samples collected.

Chi-square analysis of STAI-II categories and adequacy of pathological samples collected.
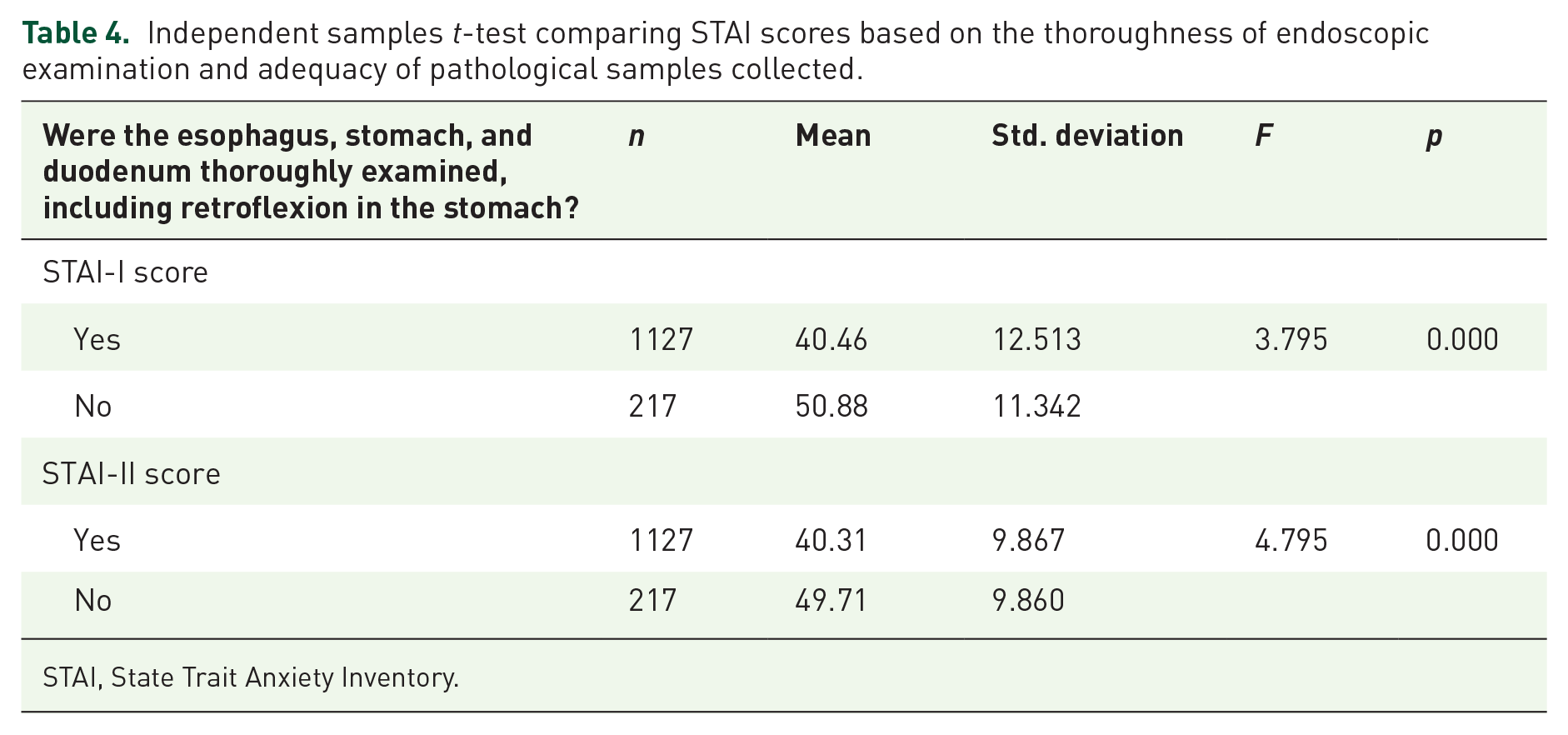
Table 4 presents the results of the independent samples t-test comparing STAI scores based on whether the esophagus, stomach, and duodenum were thoroughly examined and whether sufficient pathological samples were collected. Patients with complete examinations had significantly lower STAI-I scores (mean = 40.46 ± 12.51) compared to those without (mean = 50.88 ± 11.34, p < 0.001). Similarly, STAI-II scores were lower in the thorough examination group (mean = 40.31 ± 9.87) compared to the incomplete group (mean = 49.71 ± 9.86, p < 0.001). Regarding the adequacy of pathological samples, patients from whom sufficient samples were collected had significantly lower STAI-I scores (mean = 40.46 ± 12.51) compared to those from whom samples were inadequate (mean = 50.88 ± 11.34, p < 0.001). The STAI-II scores followed a similar pattern, with lower anxiety scores associated with adequate sample collection. These results further confirm the strong association between higher anxiety levels and both the thoroughness of the examination and the adequacy of sample collection, reinforcing the need to address patient anxiety to improve endoscopic outcomes.
Independent samples t-test comparing STAI scores based on the thoroughness of endoscopic examination and adequacy of pathological samples collected.
STAI, State Trait Anxiety Inventory.
The logistic regression analysis results are presented in Table 5. Initially, a univariate logistic regression analysis was conducted to identify significant predictors of unsuccessful endoscopic procedures. The factors found to be significant in the univariate analysis were then included in a multivariate logistic regression model to determine their independent effects. In the univariate logistic regression examining predictors of unsuccessful endoscopy, neither age nor gender reached statistical significance. The odds ratio (OR) for age was 1.005 (95% confidence interval (CI): 0.997–1.013, p = 0.21), indicating no clinically meaningful increase in the risk of incomplete examination per additional year. Female gender demonstrated a borderline association with unsuccessful procedures (OR = 1.228, 95% CI: 0.982–1.538, p = 0.07), but this did not meet the conventional threshold for statistical significance (p < 0.05). Therefore, neither variable was included in the subsequent multivariate model.
Multivariate logistic regression analysis of factors predicting unsuccessful endoscopic procedures.

Variable(s) entered on step 1: Do you have any concerns or anxieties about the endoscopy procedure? STAI-I Score, STAI-II Score.
CI, confidence interval; STAI, State Trait Anxiety Inventory.
The multivariate analysis revealed that higher STAI-I and STAI-II scores were significant independent predictors of unsuccessful endoscopic procedures. Specifically, for each unit increase in the STAI-I score, the odds of an unsuccessful procedure increased by 3.8% (OR = 1.038, 95% CI: 1.023–1.054, p < 0.001). Similarly, each unit increase in the STAI-II score was associated with a 7.4% increase in the odds of an unsuccessful procedure (OR = 1.074, 95% CI: 1.055–1.093, p < 0.001). In addition, patients who reported concerns or anxieties about the procedure were more than twice as likely to experience an unsuccessful endoscopic outcome (OR = 2.008, 95% CI: 1.403–2.874, p < 0.001). These findings suggest that anxiety, as measured by both STAI-I and STAI-II scores, is a significant independent predictor of endoscopic procedural failure. Managing patient anxiety could therefore be crucial in improving the success rates of these procedures. In the univariate analysis, the relationship between age, gender, anxiety levels, and endoscopic success was evaluated. However, in the multivariate analysis, age and gender were not found to be independent predictors and therefore were not included in the model. As shown in Tables 4 and 5, STAI-I and STAI-II scores were identified as independent predictors of unsuccessful endoscopic procedures.
The ROC curve analysis is detailed in Table 6 and visually represented in Figure 6. This analysis was conducted to determine the optimal cutoff value for the STAI-I score in predicting unsuccessful endoscopic procedures. The ROC curve for the STAI-I score revealed an area under the curve (AUC) of 0.720 (95% CI: 0.687–0.754, p < 0.001), indicating moderate discriminative ability. The analysis identified a cutoff value of 36 for the STAI-I score, above which the likelihood of an unsuccessful procedure significantly increased. This cutoff value was chosen based on its balance between sensitivity and specificity in predicting the outcome. The findings from the ROC analysis suggest that an STAI-I score higher than 36 is a strong indicator of potential procedural failure, reinforcing the importance of addressing anxiety levels before conducting endoscopic procedures.
ROC curve.

The test result variable(s): STAI-I score has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased.
Under the nonparametric assumption.
Null hypothesis: true area = 0.5.
STAI, State Trait Anxiety Inventory.

ROC curve analysis for STAI-I score.
Discussion
The primary objective of this study was to investigate the impact of pre-procedural anxiety levels on the quality of EGD in non-sedated patients. Our primary finding was that elevated anxiety levels, as indicated by a STAI-I score of 36 or above, as determined by ROC analysis, were significantly associated with a reduction in the quality of the endoscopic procedure. Logistic regression analysis further confirmed that higher STAI-I and STAI-II scores were independent predictors of unsuccessful endoscopic procedures, with each unit increase in STAI-I and STAI-II scores significantly increasing the odds of an unsuccessful procedure. In patients with an STAI-I score above 36, it was found that the endoscopic examination could not be performed in a comprehensive manner, critical maneuvers such as retroflexion could not be completed, and adequate biopsy collection was difficult. In these patients, the incidence of procedure failure was significantly elevated, and the quality of the endoscopic examination was diminished. This finding demonstrates the direct impact of anxiety on the success of endoscopy and emphasizes the necessity of proactively planning sedation in patients with high anxiety levels.
Our secondary findings demonstrated that elevated anxiety levels had a detrimental impact on both the quality of the endoscopy and the adequacy of the pathological specimens obtained during the procedure. A considerable proportion of patients with high STAI scores had inadequate biopsy specimens, which hindered the diagnostic process. Furthermore, the majority of patients who experienced discomfort during the procedure exhibited high levels of anxiety and expressed low levels of satisfaction post-procedure.
The efficacy of topical anesthetic sprays in improving patient comfort during gastroscopy remains controversial. Some studies suggest that lidocaine spray may enhance tolerance, particularly in younger and first-time patients, 14 while others report limited effectiveness. 15 Despite the use of lidocaine spray in all patients in our study, those with high STAI scores had significantly higher rates of unsuccessful procedures. This finding suggests that factors beyond the gag reflex, such as intra-abdominal pressure changes, air distension, and pain, may exacerbate anxiety during the procedure. Lidocaine spray alone may not be sufficient for highly anxious patients, and sedation should be considered in this subset of individuals.
In addition to anxiety levels, the indication for endoscopy may also contribute to procedural success. Our results demonstrated that patients undergoing endoscopy for GERD exhibited a higher rate of incomplete procedures, while those with chronic nausea and vomiting showed a borderline association with unsuccessful endoscopy. These findings suggest that patient-specific factors beyond anxiety, such as esophageal motility disorders or functional dyspepsia, may influence procedural difficulty and tolerability. Previous research indicates that GERD is frequently associated with heightened esophageal sensitivity, particularly in patients with non-erosive reflux disease and overlapping functional esophageal disorders. 16 Patients with reflux hypersensitivity or functional heartburn often exhibit abnormal pain perception and increased visceral sensitivity, which may contribute to discomfort and intolerance during endoscopy. 17 In addition, the overlap of GERD with other functional gastrointestinal disorders has been linked to increased symptom burden and impaired quality of life. 18 While our study was not designed to assess the underlying pathophysiological mechanisms, it is plausible that altered esophageal sensitivity in these patients may reduce their tolerance to endoscopic procedures. Future studies integrating esophageal sensitivity testing, pH-impedance monitoring, and high-resolution manometry could provide further insight into how esophageal hypersensitivity affects procedural success in non-sedated endoscopy.
In a study conducted by Jones et al., 94 patients with STAI results obtained prior to endoscopy were evaluated. The findings demonstrated that anxiety levels were elevated irrespective of age and gender variables. 19 Furthermore, this study demonstrated that physicians attempted to gauge patients’ anxiety levels through the analysis of resting heart and respiratory rates, as well as the use of a visual analog scale. However, the subjective assessments provided by physicians proved inadequate for accurately determining the actual anxiety levels, particularly in comparison to the results obtained from the STAI. These findings indicate that comprehensive psychological assessments based on STAI measurements may more accurately predict pre-procedural anxiety levels and that other subjective and physiologic measurements may be inadequate. The objective of our study was to ascertain the actual anxiety levels of the patients and to interpret the effects of anxiety in the most accurate way using STAI measurements rather than subjective evaluations. Our findings also demonstrate that STAI measurements are a reliable method and that a cutoff value of 36 can be a critical indicator in determining the necessity for sedation. Pontone et al. 10 demonstrated that elevated pre-procedural anxiety levels were associated with reduced EGD tolerance in a study that examined the impact of pre-procedural waiting times on anxiety and included 105 patients. The findings of this study may not be generalizable due to several limitations. First, the anxiety scale used to assess patients was a simple numerical scale ranging from 0 to 10, which may not have fully captured the complexity of anxiety experienced by patients. Second, the variability in waiting time before endoscopy may have introduced confounding factors. Third, the small patient group examined may have limited the generalizability of the findings. Pontone et al. limited their study to a small sample, whereas our study used a larger sample and ROC analysis to demonstrate this relationship in a more comprehensive manner. In a study by Campo et al. 9 that included 509 patients who underwent EGD without sedation, the presence of a gag reflex, fear, young age, and high anxiety levels were identified as factors that could indicate poor tolerance of the procedure and the need for sedation. However, in this study, unlike our study, patients were divided only into low and high anxiety groups, detailed STAI score result analysis was not performed, and a cutoff value was not specified according to the measurement scores.
The management of patients with high anxiety levels represents a notable area of inquiry within the existing literature. In a study by Behrouzian et al., the efficacy of psychological preparation techniques in patients undergoing EGD was investigated. The study included 98 patients and demonstrated a notable reduction in STAI score measurements when psychological preparation techniques were employed for patients with elevated anxiety levels, as indicated by STAI score measurements prior to the procedure. 20 Nevertheless, the impact of this reduction in anxiety levels achieved through psychological preparation techniques rather than sedation on the quality of the procedure remains unexamined. Consequently, it is not possible to ascertain whether patients with elevated anxiety levels can be sufficiently sedated to enable the performance of a procedure of satisfactory quality without sedation. In a study conducted by Trevisani et al., 226 patients were randomly assigned to receive either non-pharmacological cognitive interventions or conscious sedation. The investigators sought to evaluate the impact of these two approaches on anxiety levels prior to undergoing an EGD. Their findings indicated that conscious sedation was more effective in reducing anxiety and improving tolerance during the procedure. 21 In a recent study by Choi et al. 22 in a pediatric patient population, it was demonstrated that higher doses of sedative drugs should be administered to patients with high anxiety levels. Furthermore, a study by Erdal et al. comprising 723 patients demonstrated that anxiety levels influence an individual’s preference for anesthesia. Patients with elevated anxiety levels exhibited a proclivity for undergoing the procedure under sedation, as evidenced by the STAI score results. 23 The aforementioned studies demonstrate that non-pharmacological methods are inadequate for enhancing EGD tolerance. Patients exhibiting elevated anxiety levels may necessitate sedation, and even higher doses of sedative drugs may be required. In this context, the accurate identification of patients who require sedation is of great importance. The findings from these studies suggest various strategies for the management of anxiety before endoscopy, and our study supports this literature. Our findings suggest that STAI score measurements are a reliable method, and the cutoff value determined in our study can play a critical role in determining the need for sedation. In our study, only topical lidocaine spray was used, and no sedative drugs were administered. However, different sedation methods are available in the literature. Deep sedation with propofol is known to eliminate anxiety completely, whereas the efficacy of midazolam alone remains uncertain. Further studies are needed to determine the appropriate sedation method and its indication in specific patient groups.
In a study conducted by Ünal et al., which included 233 patients, it was proposed that anxiety levels prior to EGD did not influence tolerance of the procedure. This finding challenges the prevailing assumption in the literature and our own study. 24 However, in this study, the Beck Anxiety Inventory (BAI) was employed to ascertain the level of anxiety experienced by the patients. The BAI is designed to assess the physical manifestations of anxiety. Such symptoms encompass physical manifestations such as cardiac palpitations, tremors, perspiration, and dyspnea. The BAI is less concerned with the cognitive dimensions of anxiety and is therefore more suitable for patients presenting with physical symptoms. By contrast, the STAI score assesses both emotional and cognitive aspects of anxiety, without being constrained by the presence of physical symptoms. The BAI’s exclusive focus on physical symptoms makes it challenging to comprehensively assess the cognitive and emotional dimensions of anxiety prior to EGD. However, the fact that the STAI score measures both state and trait anxiety allows for a more comprehensive understanding of the cognitive and emotional effects of anxiety on processing quality. Consequently, it is a more suitable instrument for assessing the effects of anxiety on an individual’s general mood and thinking. The cognitive and emotional effects of anxiety can directly impact patient experience and cooperation during EGD. The STAI is a more commonly used scale to measure anxiety before medical procedures and its impact on the procedures.
In this study, a standardized waiting interval was adopted between the application of topical lidocaine spray and the initiation of endoscopy. Previous research suggests that topical lidocaine achieves optimal oropharyngeal anesthesia within approximately 3–5 min, potentially improving patient comfort during endoscopy.14,15 Therefore, we routinely waited 3 min following the application of lidocaine spray before starting the procedure to ensure sufficient mucosal anesthesia and minimize variability in patient tolerance. Since this standardized protocol was consistently applied to all patients, we did not consider it a limitation but rather an integral part of our routine practice.
The completeness and quality of endoscopic evaluation are not solely determined by biopsy adequacy and the immediate visualization of all anatomical segments. Another vital aspect is the frequency of missed diagnoses, particularly in the context of malignant or premalignant lesions. Although our study did not specifically quantify missed lesions during the follow-up period, the literature suggests that a small percentage of upper gastrointestinal pathologies can be initially overlooked despite thorough endoscopy.25,26 Establishing a consistent follow-up protocol or performing a second-look endoscopy under certain clinical indications (e.g., persistent symptoms, suspicious ulcer margins) can help mitigate this risk. 27 In our routine practice, patients with unremarkable findings but ongoing symptoms are re-evaluated within 3–6 months, and earlier repeat endoscopy may be warranted based on clinical judgment. Future multicenter studies that systematically track the incidence of missed diagnoses over longer follow-up intervals could provide a more robust assessment of endoscopic completeness and quality.
The single-center nature of our study limits the generalizability of the results to different clinical settings. In addition, the cross-sectional design prevents the establishment of causality between pre-procedural anxiety and unsuccessful endoscopic outcomes. Although we identified an STAI-I cutoff of 36, further validation in multicenter studies is required to confirm its predictive value across different populations and healthcare settings. Another limitation is that we did not assess the long-term impact of anxiety on patient outcomes, such as procedural tolerance in subsequent endoscopies. Furthermore, while we controlled for potential confounders, other psychological and physiological factors (e.g., baseline pain tolerance, previous negative medical experiences, and underlying psychiatric disorders) may have influenced patient anxiety and endoscopic outcomes. Lastly, although our study included a large sample size, future studies with diverse patient populations may further strengthen the external validity of our findings. As this study focused on non-urgent EGD cases and excluded patients with malignancy suspicion, obstructive symptoms, and active gastrointestinal bleeding, the potential impact of indications on endoscopic quality and biopsy rates is expected to be limited. However, future studies are needed to further evaluate the influence of specific indications on procedural outcomes. This study did not include a specific analysis of post-procedural complications. However, given that our study focused on non-sedated patients, the risk of major complications is considered low. All patients were monitored post-procedure, and no significant complications were reported. However, future studies may benefit from a more comprehensive evaluation of the relationship between pre-procedural anxiety and post-procedural complications. The study’s key strengths include the large sample size, the use of real-world data to address tangible clinical challenges, and the comprehensive statistical analyses, including ROC analyses, employed to evaluate the findings.
To the best of our knowledge, the findings of this study, which examined the effect of patients’ anxiety levels before EGD on procedure quality using reliable scales such as STAI and was conducted with one of the largest patient populations, suggest that routine assessment of anxiety levels before endoscopy in non-sedated patients may contribute to the development of more effective and personalized management strategies. In particular, patients with elevated anxiety levels can be readily identified through the administration of the STAI score assessment prior to the procedure. The cutoff value derived from the ROC analysis in this study may serve as a reliable indicator for predicting the necessity of sedation. It is recommended that routine STAI score assessment prior to endoscopy be more integrated into clinical decision-making processes. Consequently, patients exhibiting elevated anxiety levels can be effectively sedated in a proactive manner, thereby enhancing the quality of the procedure and patient satisfaction. This strategy also offers a cost-effective approach, to reduce the additional costs associated with unnecessary sedation and potential complications related to sedation. Therefore, a more precise identification of the necessity for sedation may enhance the safety and efficacy of clinical practice. Nevertheless, multicenter, prospective studies with greater enrollment are essential to substantiate this recommendation in a broader population. Such studies are crucial to ascertain the generalizability of the findings across diverse patient groups and to gain a deeper insight into the utilization of anxiety-based management strategies in routine clinical settings.
Conclusion
This prospective, cross-sectional study suggests that pre-procedural anxiety, as measured by the STAI-I score, may influence the quality of upper gastrointestinal endoscopy in non-sedated patients. An STAI-I score cutoff of 36, identified by ROC analysis, may help predict the likelihood of an unsuccessful procedure, emphasizing the potential importance of anxiety management in clinical practice. Logistic regression analysis indicated that higher STAI-I and STAI-II scores were associated with an increased likelihood of unsuccessful endoscopy. Routine assessment of anxiety levels before endoscopy may assist in sedation planning, potentially improving procedural outcomes, enhancing patient satisfaction, and minimizing unnecessary sedation-related complications. In addition, this approach could contribute to optimizing healthcare resources by reducing the overuse of sedation. However, due to the cross-sectional design of this study, causality cannot be established. Further multicenter studies with larger sample sizes are required to validate these findings and refine anxiety-based management strategies in endoscopic practice.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848251333025 – Supplemental material for The effect of pre-procedural anxiety level on the quality of upper GI endoscopy in non-sedated patients: “can the need for sedation be predicted?”
Supplemental material, sj-pdf-1-tag-10.1177_17562848251333025 for The effect of pre-procedural anxiety level on the quality of upper GI endoscopy in non-sedated patients: “can the need for sedation be predicted?” by Hulusi Can Karpuzcu, Görkem Yarbaş, Ramis Çatalbaş, Nur Aylin Atlı and Çağdaş Erdoğan in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848251333025 – Supplemental material for The effect of pre-procedural anxiety level on the quality of upper GI endoscopy in non-sedated patients: “can the need for sedation be predicted?”
Supplemental material, sj-pdf-2-tag-10.1177_17562848251333025 for The effect of pre-procedural anxiety level on the quality of upper GI endoscopy in non-sedated patients: “can the need for sedation be predicted?” by Hulusi Can Karpuzcu, Görkem Yarbaş, Ramis Çatalbaş, Nur Aylin Atlı and Çağdaş Erdoğan in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.