
Abstract
Upper gastrointestinal (UGI) endoscopy contributes a major clinical service with consistently growing demand around the world. Its utility corresponds to varying epidemiological issues throughout the globe, with cancer screening and surveillance being of the utmost priority. Despite high accuracy in neoplasia detection, UGI endoscopy remains a highly operator-dependent procedure, characterized by a substantial rate of missed pathology. Despite an overall lack of high-quality performance measures, there is an increased level of awareness about the need for quality control of this procedure, which is reflected in several guidelines and position statements published in recent years. It is widely recognized that quality assessment should go beyond mere technical aspects of the examination, and include both pre- and post-procedural factors. By this means, quality control encompasses the entire patient experience with the health care provider, from appropriate indication and physical assessment, through high-quality endoscopy service, to appropriate follow up and patient satisfaction. This article aims to review the available and emerging quality metrics for UGI endoscopy, taken mostly from Western endoscopy societies, with references to Asian recommendations where appropriate. The paper is limited solely to diagnostic UGI endoscopy and does not include performance measures for therapeutic procedures.
Introduction
Gastrointestinal endoscopy contributes a major clinical service, demand for which is consistently increasing. 1 Esophagogastroduodenoscopy (EGD), in particular, has become a key diagnostic procedure in the upper gastrointestinal (UGI) tract, principally for detection and surveillance of premalignant conditions and cancers. Data from the United States (US) have shown that, within the first decade of the new millennium, the use of endoscopy has increased by over 50%, 1 a trend that continues to today. In 2009 alone, for example, it was estimated that 6.9 million EGDs were performed in the US, contributing to a cost of $12.3 billion (in an outpatient setting only). 1 More recent data from the United Kingdom (UK) have shown that over 1.2 million EGDs (both therapeutic and diagnostic) were performed in the UK in 2016. 2
The utility of EGD corresponds to varying epidemiological issues throughout the globe. In high-risk regions for gastric cancer, such as Japan and South Korea, EGD has not only become an established alternative to X-ray photofluorography as a first-line screening modality but is gradually replacing it. 3 In the Western world, on the other hand, the dramatically increasing incidence of esophageal adenocarcinoma (EAC) has become an important epidemiological issue. 4 Since this malignancy has an endoscopically detectable (and potentially curable) precursor lesion – Barrett’s esophagus (BE) – implementation of endoscopic screening for high-risk individuals is being encouraged.5–7
Clearly, the utility of EGD is increasing on a worldwide scale, and, with growing demand, there is a need to ensure the highest quality standard. The importance of quality assessment in endoscopy has already been explored in the field of colonoscopy. Since its introduction as a screening test for colorectal cancer, a significant body of research has been dedicated to developing quality metrics. These are measurable parameters of individual performance usually related to the procedural diagnostic yield (e.g. positive correlation of colonoscopy withdrawal time with the rate of detected adenomas) and patient-oriented outcomes (e.g. the inverse association of adenoma detection rate and incidence of post-colonoscopy cancers).8–10
Despite a growing interest in the topic of quality metrics for EGD reflected in recently published guidelines and position statements,11–14 high-quality indicators for this procedure are still lacking. Most of the presented measures are based on poor evidence, and are rarely associated with patient-oriented outcomes.11–14 Given a substantial number of missed UGI cancers during endoscopy, namely 11.3%, according to a recent meta-analysis, 15 the topic of EGD quality control is of paramount importance.
This review aims to present established and emerging quality metrics for UGI endoscopy. It collates current recommendations, taken mostly from Western endoscopy societies with references to Asian recommendations where appropriate. The article focuses on diagnostic EGD and does not cover quality metrics for therapeutic procedures. The summary of key quality metrics discussed in the article is presented in Table 1.
Summary of key quality metrics in UGI endoscopy.

AE, adverse event; AGA, American Gastroenterological Association; BE, Barrett’s esophagus; BSG, British Society of Gastroenterology; EGD, esophagogastroduodenoscopy; ESGE, European Society of Gastrointestinal Endoscopy; GEJ, gastroesophageal junction; MAPS, management of precancerous conditions and lesions in the stomach; NBI, narrow-band imaging; UGI, upper gastrointestinal tract.
Pre-procedure quality indicators
Preparation
All individuals undergoing endoscopy should be accurately informed about the procedure, indications for it, the risks it will entail, and the management of potential complications. Preparation of the patient includes proper fasting instructions – a key performance measure according to the European Society of Gastrointestinal Endoscopy (ESGE). 12 Based on available data, ESGE defines the adequate time of fasting as at least 2 h for liquids and 6 h for solids. 12 Although not included in the guidelines, patients with known delayed gastric emptying (gastroparesis) may benefit from a longer duration of fasting (e.g. overnight fasting) on a case-by-case basis. 16 Before EGD, patients should receive an easily understandable take-home information sheet about the procedure, and, unless it is an emergency procedure, informed signed consent should always be obtained.
Preparation for the procedure also includes an assessment of the patient’s health status. The most common clinical issues requiring attention before endoscopy include management of diabetes, anticoagulation treatment, the need for prophylactic antibiotics, and sedation requirements. The American Society of Anaesthesiology (ASA) score is the most commonly used scoring system to categorize patients by their physiological status to predict the operative risk. 17 ASA scores classify patients into six categories (ASA 1–6), ranging from a normal healthy patient, through a patient with mild and severe systemic disease, up to moribund and brain-dead patient, as presented in Table 2.
ASA score. 15 Last approved by the ASA House of Delegates on 15 October 2014.

ASA, American Society of Anesthesiologists; BMI, body mass index; CHF, congestive heart failure; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DIC, disseminated intravascular coagulation; DM, diabetes mellitus; ESRD, end-stage renal disease; HTN, hypertension; MI, myocardial infarction; TIA, transient ischemic attack.
There is a growing body of evidence to suggest that surgical safety checklists can prevent errors and thus impact positively on patient morbidity and mortality. 18 Although there is no standardized checklist for the use of endoscopy, the British Society of Gastroenterology (BSG) defined basal domains that should be included in such a document: patient identifiers (name/hospital number/date of birth); allergies; medications and conditions that may preclude any interventions, such as use of anticoagulation or significant comorbidities; patient understanding of proposed test; completion of a consent form. 11
Although not used in routine practice, premedication with defoaming agents (e.g. simethicone) and mucolytics (e.g. pronase or N-acetylcysteine) to improve mucosal visualization during EGD are being increasingly discussed. In a recent multicenter randomized controlled trial (RCT) on 7200 screening EGDs, premedication with pronase and simethicone significantly increased mucosal visibility in the UGI tract, although this did not affect the rate of neoplasia detection. 19 Another RCT showed that a combination of N-acetylcysteine and simethicone ingested 20 min before EGD significantly improved mucosal visibility as compared with no intervention and a water preparation. 20 The Asian consensus on diagnostic standards for UGI endoscopy recommends the use of mucolytic and defoaming agents for the improvement of visual clarity during EGD. 14 Unlike in colonoscopy, there is no validated scale to assess the mucosal preparation of the UGI tract. Nevertheless, a dedicated scoring system for mucosal visibility was established for the purposes of previous studies. 21 This system can be used in everyday practice, and is based on a 4-tier scale of mucosal visibility ranging from 1 to 4 (1- no adherent mucus; 2- mild mucus, but not obscuring vision; 3- large amount of mucus obscuring vision; and 4- heavy adherent mucus). 21 ESGE recommends that EGD reports should include information on the contents of the stomach, such as food residues, blood, bile, or the presence of bubbles, along with information on whether a waterjet was used to improve mucosal visualization. 12
Indication appropriateness
Reviewing the endoscopy referral form along with the indications for the procedure remains a crucial task before performing any endoscopic examination. Endoscopists should be familiar with the standard indication list for EGD, and individually review every variation from it. Presenting the full list of indications goes beyond the scope of this article but may be found in previous documents, such as the American College of Gastroenterology (ACG) and American Society for Gastrointestinal Endoscopy (ASGE) quality recommendations.13,22 ACG/ASGE imply that indications for EGD must be documented, and be in line with the published standard list in at least 80% of cases. 23
Additionally, reviewing the indication and available clinical data provides an opportunity to identify patients at greater risk of UGI cancers. For such individuals, a lower threshold to biopsy suspicious lesions should be considered, and appropriate image-enhancing modalities prepared a priori. The Asian consensus emphasizes the need for patients’ risk stratification before every diagnostic EGD. 14 For example, patients of the male gender with a history of previous head and neck cancer and a known history of excessive alcohol intake or tobacco smoking are at increased risk of esophageal squamous cell carcinoma (ESCC). These patients should undergo a detailed inspection of the whole length of the esophagus, preferably with advanced imaging techniques (described further). On the other hand, obese men of Caucasian origin with a long-standing history of gastroesophageal reflux disease (GERD) are at increased risk of BE-related EAC, and require a meticulous inspection of the gastroesophageal junction (GEJ) and BE segment, if present. Figure 1 presents common high-risk clinical profiles and appropriate endoscopic management.

High-risk clinical profiles and endoscopic features.
Lastly, identifying high-risk individuals provides an opportunity to prepare longer slots for examination during endoscopy lists. The BSG guidelines recommend that a standard diagnostic endoscopy should be allocated a slot of a minimum of 20 min, increasing as appropriate for surveillance of high-risk conditions. 11
Intra-procedure quality indicators
Competence
Assessing competence and granting permission for trainees to perform unsupervised EGDs remains challenging. It is debatable at which point UGI endoscopists become technically competent, and this is because, in most institutions, endoscopy training is personalized and rather informal. Previous studies on the EGD learning curve showed that at least 100 supervised procedures are necessary to achieve technical competence. 24 A more recent study analyzing 243,555 EGDs recorded at the Joint Advisory Group on GI endoscopy (JAG) database showed that it requires at least 200 procedures for most trainees (90%) to maintain a 95% procedural completion rate. 25 In this study, the rate of complete procedures was associated positively with previous experience in lower GI endoscopy and older trainee age. 25 Following this data, a minimum number of 200 complete unassisted procedures are required, in both the UK and Australia, to achieve competence in diagnostic EGD.26,27 Similarly, at least 150 procedures are required in Canada (including ⩾100 without assistance) and 130 procedures are required in the US.28,29 Interestingly, in South Korea, a minimum number of 1000 EGDs are recommended to achieve competency according to the Korean Society of Gastrointestinal Endoscopy (KSGE). 30
There is increasing evidence that structured training can improve the detection of superficial neoplasia. In recent years, several web-based video learning programs for detecting early disease became available. For example, the efficacy of an e-learning module for early gastric cancer recognition was evaluated in an international multicenter RCT on 332 endoscopists from 35 countries. 31 After a pre-test on 40 sets of endoscopic images, participants were allocated randomly to either e-learning or non-e-learning group, and, after 2 months, both groups received a post test. The study showed a mean improvement rate in recognizing early gastric cancers at a level of 1.4 (±0.26) and 1.0 (±0.16) for the e-learning and non-e-learning groups, respectively (p < .001). The Asian recommendations underline the benefits of structured training in improving the detection rate of UGI superficial neoplasia. 14
Rate of complete procedures
Currently, the rate of complete examinations, defined as the proportion of unassisted EGDs with successful intubation of the second part of the duodenum (D2), remains the main criterion in assessing competence in diagnostic UGI endoscopy. In the UK, for example, the JAG requires trainees to intubate the D2 and perform a J-manoeuvre (retroflection in the stomach) in ⩾95% of procedures. 26 In the US, the EGD completion rate is a key quality measure according to the Clinical Outcomes Research Initiative (CORI) – a central electronic database monitoring endoscopy outcomes. A target procedural completion rate of ⩾98% is recommended. 13
Procedure time
The procedure time is, so far, the most extensively studied quality parameter in diagnostic EGD. ESGE recommends that all endoscopy reports should routinely include procedure time (target: ⩾90% reports), 12 and the BSG require this at least for surveillance procedures in high-risk conditions, such as BE and premalignant stomach [atrophic gastritis (AG) and gastric intestinal metaplasia (GIM)]. 11 The definition of EGD procedure time, however, varies between studies. Some define it as the time from intubation to extubation of the patient, 32 while others consider only the time of withdrawal from D2 until extubation (the “inspection time”). 33 It also remains unclear whether to include the time spent on taking biopsies into the procedural time.
In a study by Gupta et al., it was shown that endoscopists who spent at least 1 min for every 1 cm of circumferential BE segment detect more suspicious lesions (54.2% versus 13.3%, p = 0.04), and tend to detect more foci of advanced neoplasia [high-grade dysplasia (HGD)/EAC], compared with endoscopists who spend <1 min on inspection (40.2% versus 6.7%, p = 0.06). 34 Following this study, ESGE included a recommendation of minimum 1-min inspection time per every 1 cm of BE as a minor performance measure. 12
A subsequent study from Singapore analyzed the association of time spent on routine EGD examination and the detection of precancerous lesions and cancers in the stomach. 32 The mean duration time of a “normal” EGD examination, defined as one that did not show any abnormalities and did not require biopsies, was 6.6 min (range 2–32 min). A rounded cut-off time of 7 min was used to show that “slow” endoscopists (>7 min procedure time) were more likely to detect high-risk lesions (AG/GIM, dysplasia and cancers) and neoplasia (cancer or dysplasia) as compared with “fast” endoscopists [odds ratios (OR) of 2.50; 95% confidence interval (CI), 1.52–4.12 and 3.42; 95%CI, 1.25–10.38, respectively]. 32
Lastly, a very recent retrospective study by Park et al. analyzed a large volume of screening EGDs in South Korea performed by 14 board-certified endoscopists. 33 Similarly, endoscopists were divided into two groups accordingly to inspection time (time upon withdrawal from the D2 after cleaning the mucosa of the stomach). A cut-off of 3 min was used in multivariable analysis to show that “slow” endoscopists were significantly more likely to detect gastric adenomas or cancers than “fast” endoscopists (OR 1.52; 95%CI, 1.17–1.97). 33
Following these studies, ESGE recommends a 7-min procedural time (from intubation to extubation) for a first diagnostic UGI endoscopy in every patient who has not undergone a previous EGD within the last 3 years. 12
Photo-documentation
Image documentation has become an integral part of EGD reporting and quality control. Although there is no data to support that photo-documentation increases EGD diagnostic efficacy, reports with an adequate number of photos may constitute a legal record of a full examination and provide information on mucosal visibility and the presence of any potential “blind spots.” Preferably, all pictures should be made after mucosal cleaning, keeping the center of the organ lumen in the center of the image. The stomach should be sufficiently insufflated so that the mucosal areas between the folds are clearly visible.
The minimum requirements for photo-documentation are variable around the world and reflect the different burden of UGI cancers in different geographical regions. In the US, for example, where the incidence of gastric cancer is relatively low, the quality guidelines do not specify the minimum number of photos for EGD reports. 13 European requirements defined by ESGE, 12 similarly to BSG, 11 include a minimal number of 10 pictures for a normal endoscopic examination that should include: (1) proximal esophagus, (2) distal esophagus, (3) Z-line and diaphragm indentation, (4) cardia and fundus in inversion, (5) corpus in forward view including lesser curvature, (6) corpus, in retroflex-view including greater curvature, (7) angulus in partial inversion, (8) gastric antrum, (9) duodenal bulb (D1), and (10) D2, as presented in Figure 2. Of note, any additional abnormalities should be documented separately.

Photo-documentation.
Notably, in Japan, typically 20–40 endoscopic images are taken during screening EGDs. Yao et al. proposed a minimum required standard called “systematic screening protocol for the stomach” (SSS) that includes 22 images to illustrate the entire stomach. 35 This protocol is rarely followed in Western countries.
Recently, the ability to visualize the major papilla in the duodenum has been proposed as a quality indicator as it reflects a high performer’s proficiency and attention during the examination. A Korean study on 111, 962 asymptomatic patients undergoing EGD showed that the rate of ampulla photo-documentation correlated significantly with the detection of UGI neoplasms [coefficient of determination (R 2 ) = 0.57, p = 0.03). 36 The mean rate of ampulla photo-documentation was 49.0 % (range 13.7 – 78.1 %). ESGE suggests that the major duodenal papilla should be visualized and photographed in all EGDs (patients with normal anatomy when a full examination is intended). 12
Terminology and reporting systems
Standardized terminology is a hallmark of high-quality endoscopy reports. 12 Classification systems in endoscopy, in general, facilitate better communication between clinicians and researchers, and are especially important in cases of international collaboration. The use of standardized terminology is listed as a key performance measure by ESGE. 12
Moreover, classification systems may determine further management. For example, the Paris classification 37 used to characterize the morphology of superficial neoplastic lesions within the GI tract can provide an approximate assessment of the depth of infiltration (into the mucosa or beyond), and guide subsequent treatment (endoscopic therapy versus surgery). The Los Angeles (LA) erosive esophagitis grading system, 38 on the other hand, can inform about the need and timing of follow-up examination. Namely, patients with mild-to-moderate esophagitis (LA grades A and B) do not require a follow-up examination; however, those with severe esophagitis (LA grades C to D), and, hence, increased risk of developing BE, should undergo a follow-up endoscopy after 8 weeks of intensive anti-reflux treatment. 39 The Terminology Committee of the World Endoscopy Organization (WEO; formerly known as OMED) has been regularly publishing the “minimal standard terminology for gastrointestinal endoscopy”. 40 A list of the most commonly used endoscopic classification systems are presented in Table 3.
Endoscopic classification systems.
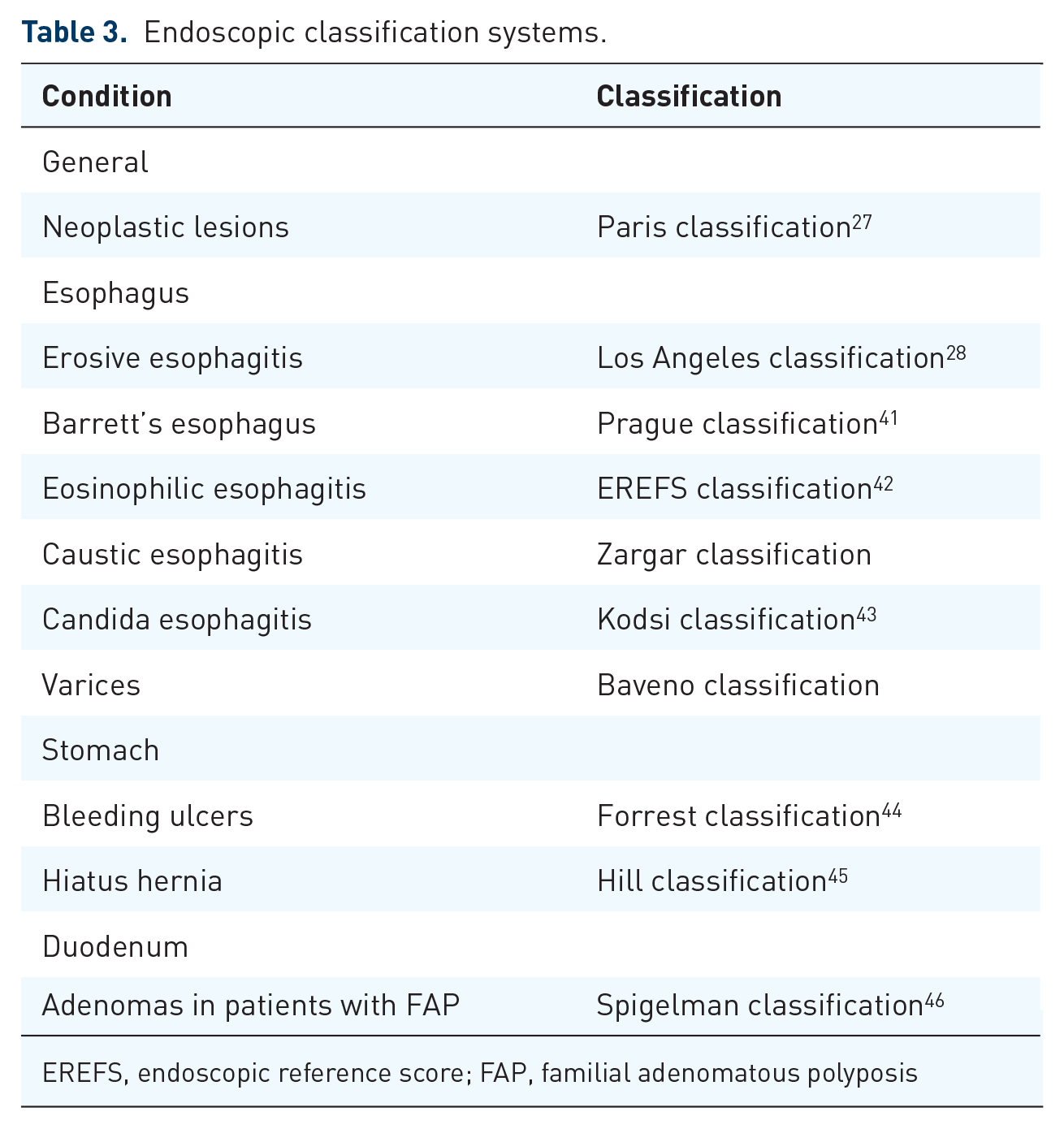
EREFS, endoscopic reference score; FAP, familial adenomatous polyposis
ESGE separately reviews the requirements of reporting systems. 47 According to these guidelines, high-quality endoscopy reporting systems must be electronic and integrated into hospital patient record systems. The patient identifiers should be easily available to facilitate data linkage. Moreover, the reports should be based on structured data entry with the use of free text entry restricted to a minimum. Lastly, endoscopy reporting systems should include histopathology data and outcomes, such as patient satisfaction, adverse events, and surveillance recommendations. 47
Advanced imaging techniques
Although EGD is considered a technically less demanding procedure than colonoscopy, the spectrum of mucosal changes encountered during EGD is much wider as it involves the assessment of three different organs and epithelia within a single examination. Advanced imaging techniques have been emerging in recent years, intending to improve mucosal visualization and enhance fine structural and microvascular architecture. 48
The current spectrum of established image-enhancing (IE) techniques include conventional chromoendoscopy, narrowed-spectrum endoscopy, such as narrow-band imaging (NBI; Olympus Medical Systems, Tokyo, Japan) and blue laser imaging (BLI; Fujifilm, Tokyo, Japan), but also several other systems, such as linked color imaging (LCI; Fujifilm, Tokyo, Japan), i-Scan digital contrast (I-SCAN; Pentax, Tokyo, Japan), autofluorescence imaging (AFI), and confocal laser endomicroscopy (CLE). These technologies are at a different level of clinical application and will not be thoroughly discussed within this article; however, few of them have an established role in routine practice and characterize a high-quality procedure. 48
In the esophagus, both Lugol staining and narrowed-spectrum endoscopy have been shown to improve detection and characterization of squamous neoplasia.49–51 Lugol reacts with glycogen, which is abundant in normal squamous epithelium, but significantly reduced or absent in dysplastic tissue. Thus, normal areas are being intensely stained by the Lugol dye to a brown color, whereas dysplastic areas have reduced or completely absent staining. In NBI imaging, on the other hand, squamous neoplasia appears as dark brown patches on the esophageal mucosa. NBI, coupled with magnification, can be extremely helpful in determining the likely depth of invasion by assessing the morphology of intrapapillary capillary loops (IPCLs). 52 Both BSG and ESGE recommend the use of Lugol’s chromoendoscopy if squamous neoplasia is suspected,11,12 which refers mostly to patients previously treated with curative intent for a primary head and neck cancer.
IE techniques are used widely in the surveillance of BE, although (so far) none of them have been shown convincingly to be superior to standard high-definition white-light endoscopy (WLE).5–7,53 Acetic acid (AA) is a commonly used dye that induces the “acetowhitening” effect on BE mucosa, highlighting its surface. One retrospective study showed an improved neoplasia detection rate with AA-guided biopsies when compared with conventional protocol-guided mapping biopsies. 54 A randomized cross-over trial comparing AA-guided biopsies versus non-targeted biopsies as per Seattle protocol is underway (the ABBA study), and the results may provide more definitive evidence to promote this technique over current standard of care.55,56
For NBI, a simple validated system to identify dysplasia and EAC within BE segments has been developed [Barrett's international NBI group (BING) criteria]. 57 This classification is based on a simple evaluation of the BE surface and vascular patterns (regular versus irregular). The BING criteria had an overall accuracy of 85% in identifying patients with dysplasia, which increased to 92% with high confidence predictions. 57
In the stomach, virtual chromoendoscopy has been applied widely in the surveillance of premalignant conditions. NBI, in particular, can be helpful in highlighting AG and discrete areas of GIM. The updated ESGE guidelines on the management of epithelial precancerous conditions and lesions in the stomach (MAPS II) recommend that virtual chromoendoscopy (±magnification) should be used for the diagnosis of the premalignant stomach by guiding biopsy for staging atrophic and metaplastic changes and by helping target neoplastic lesions. 58
LCI, on the other hand, is an emerging imaging modality with growing utility in the UGI tract. LCI differentiates the red color spectrum, and increases the contrast between inflamed and normal areas; LCI is helpful in accurate detection and delineation of neoplastic lesions, particularly within gastric mucosa. In a recent study, LCI was shown more effective for recognition of early gastric cancer compared with WLE. 59 Moreover, previous studies have shown that LCI can be helpful in the real-time diagnosis of active Helicobacter pylori infection. 60
Computer-aided detection
In recent years, we have witnessed enormous progress in the field of artificial intelligence and computer-aided detection (CAD) systems, which may play a great role in improving the quality of UGI endoscopy worldwide. 61 This area of research focuses mostly on automated identification of early neoplasia within the UGI tract providing on-site decision support. CAD relies on algorithms that, after the process of machine learning (e.g. deep neural network learning), can automatically recognize complex image patterns, such as irregular vascular patterns or subtle changes of the mucosal surface. Recently, CAD technology has been introduced for the detection of esophageal neoplasms of both squamous and glandular origin achieving a sensitivity of 97.8% and 95.0%, and a specificity of 85.4% and 85.0%, respectively.62,63 It has to be emphasized, however, that most of these studies rely on good-quality images and the accuracy of these systems may significantly drop when adopted into general endoscopy practice (“preselection bias”).
Moreover, CAD could serve as a quality control system that could automatically recognize and document the mucosal preparation, percentage of the visualized mucosal surface, and assess the completeness of procedure. A novel real-time quality-improvement system called WISENSE has been developed by investigators from China to monitor blind spots during EGD, record the procedure time, and automatically record images during the procedure. 64 Recent RCT showed that WISENSE could significantly reduce the amount of blind spots during EGD (−15.39%) as compared with controls. 64 The authors suggested that WISENSE could be used to improve the performance of EGD. 64
Biopsy sampling
Despite evolving technology and increasing experience in optical recognition of UGI lesions, tissue acquisition and analysis remain the gold standard in diagnosing UGI pathology. Histological assessment, on one hand, provides a valid confirmation of endoscopically (or clinically) suspected condition, on the other hand, is related to a financial burden.
Recent studies demonstrate a high variability in the rate of obtaining biopsies between endoscopists during routine diagnostic and screening EGDs.33,64 In a study by Park et al., 33 the variability in the biopsy rate ranged between 6.9% and 27.8% among operators, and it correlated significantly with the UGI neoplasm detection rate (R 2 = 0.76; p = 0.015). 33 In a more recent multi-center study, the biopsy rate varied between 22.0% to 65.8% among operators. The endoscopists’ biopsy rate (EBR), defined as the proportion of EGDs with at least one biopsy to all examinations performed by a single physician, was shown to be correlated positively with the detection of premalignant conditions [Spearman’s rank correlation (rs) = 0.835, p < 0.001] and inversely associated with the rate of missed gastric cancers. EBR, therefore, was proposed as a novel EGD quality indicator. 64 As expected, the increasing EBR was related to the growing rate of “negative biopsies” that showed no abnormality in the microscopic assessment, hence carrying no clinical implications but increasing the costs. 64 The most accurate biopsy rate, compromising the highest diagnostic yield and the lowest financial burden, remains to be defined. 64
This high variability in biopsy rates indicates that the decision to biopsy remains subjective, and is based mostly on clinical judgment. Biopsy protocols have been introduced to maximize the diagnostic efficacy and apply uniform high-risk conditions surveillance. They represent a minimum standard of care in several defined conditions, and should be followed to maintain high-quality endoscopy service.
For example, to accurately diagnose eosinophilic esophagitis (EoE), it is recommended to obtain a set of at least six biopsies from at least two distinct areas of the esophagus. 65 Usually, this includes taking three biopsies from the proximal and distal esophagus placed into separate containers. This recommendation was made given the patchy distribution of inflammatory changes throughout the esophagus and the fact that typical endoscopic characteristics of EoE, such as mucosal edema, rings (trachealisation), white plaques, longitudinal furrows, and strictures, are not always present. 65 The BSG guidelines recommend that such a set of biopsies should be obtained in >90% of patients presenting with dysphagia or food bolus obstruction where an alternative cause was not found. 11
Surveillance of BE is described by the Seattle protocol, which implies taking four quadrantic biopsies every 2 cm along the circumferential extent of the non-dysplastic BE segment. Targeted biopsies from any suspicious area within the BE segment should be taken separately. 55 Both ESGE and BSG acknowledge the Seattle protocol, which should be used in ⩾90% cases of BE surveillance.11,12
In the stomach, chronic AG and GIM are well-described precursor conditions for gastric adenocarcinoma. 66 The updated Sydney system is the most widely accepted protocol for the classification and grading of gastritis (including AG and GIM), 67 and recommends taking at least five biopsies: two from the antrum (from the greater and lesser curvature, ~3 cm from the pylorus); one from the incisura; and two from the gastric body (from the lesser curvature ~4 cm proximal to the incisura, and from the middle of the greater curvature). Such a set of biopsies provides information on the extent of AG/GIM in the stomach and enables risk-stratification of patients with histopathological staging systems, such as an operative link for gastritis assessment (OLGA), or, more commonly used, the operative link for gastric intestinal metaplasia (OLGIM). 68 Previous studies have shown that the separate biopsy taken from the incisura has a modest additional diagnostic value and, in some circumstances, can be avoided.58,69,70 ESGE recommend biopsies from at least two topographic sites (both the antrum and the corpus, at the lesser and greater curvature of each) for adequate staging of gastric precancerous conditions, especially when performed under advanced-imaging guidance by an experienced endoscopist. 58
A more rigorous Cambridge protocol is used for patients fulfilling the criteria of hereditary diffuse gastric cancer (HDGC) – a genetic form of gastric cancer related to a CDH1 germline mutation. 71 Although carriers of this mutation have a lifetime risk of gastric cancer reaching up to 80%, and are generally recommended to undergo prophylactic gastrectomy, endoscopic surveillance may be offered to those opting to postpone gastrectomy time, those with CDH1 mutation variants of uncertain significance, and those that fulfill HDGC clinical criteria without germline CDH1 mutations. 71 Such surveillance should be performed in experienced centers, with the use of high-definition endoscopes equipped with advanced imaging modalities within a dedicated session of at least 30 min. Target biopsies from suspicious areas (usually pale in appearance) and multiple random biopsies from each segment of the stomach (5 from each: pre-pyloric area, antrum, transitional zone, gastric body, fundus, and cardia) should be taken. 71
Lastly, biopsies from the duodenum are required for the diagnosis of celiac disease in adults, and in cases of suspicion of this disease (e.g. patients evaluated for anemia, iron deficiency without anemia, weight loss, and diarrhea) a minimum set of at least four biopsies from the duodenum are required. At least one biopsy from the duodenal bulb should be included in this set, as this may be the only site demonstrating villous atrophy.72,73
Figure 3 illustrates the biopsy protocols presented in this section.

Biopsy protocols.
Sedation
Sedation practices in endoscopy are highly diverse. There is no consensus on which procedures warrant sedation, who should administer it, and which sedatives should be used. These variations have a different source of origin, but relate mostly to different health care policies, cultural norms, and endoscopic training.
In recent years, the impact of sedation on the safety and quality of endoscopy has been increasingly discussed. Although no studies have directly analyzed the influence of sedation on EGD diagnostic performance, several reports have shown that sedation can significantly increase patient cooperation, satisfaction, and willingness to repeat the procedure. 74 The recent Asian consensus recommends the use of sedation to enhance the detection rate of superficial neoplasm of the esophagus and stomach. 14 In practical terms, the use of sedation should always be encouraged in high-risk patients who require longer and more complex examinations (e.g. a long segment of BE, premalignant stomach, genetic cancer syndromes). In general, there are three different levels of sedation, which, broadly, can vary from “light” through “deep” sedation, up to general anesthesia. The endoscopist should target the level of sedation accordingly to the planned procedure taking into consideration its complexity, invasiveness, and estimated time of the procedure. Light to moderate sedation (“conscious sedation”) is sufficient for most endoscopic procedures. Conscious sedation can usually be achieved with a combination of benzodiazepines and opioids or, propofol with or without adjunct of benzodiazepines. 75
Selected patients may be able to undergo endoscopic procedures without sedation. This decision should be carefully balanced, taking into consideration patient characteristics and local health care policies. A previous study analyzing patients’ attitudes towards diagnostic EGDs has shown that male gender and younger age were associated with a lower rate of sedation preference. Moreover, previous exposure to endoscopy reduced the level of discomfort during subsequent examinations. 76
To standardize the practice of sedation in endoscopy, ASGE released guidelines on sedation in endoscopy for non-anesthesiologists. 75 In general, light and moderate sedation can be delivered safely by endoscopists to patients who are ASA Class I, II, or III. Minimal patient monitoring includes an electronic assessment of blood pressure, heart rate, and pulse oximetry, and the visual assessment of ventilatory activity, level of consciousness, and discomfort. The American quality recommendations also advise that before administrating sedation and inserting the scope, a team pause should be made (and documented), during which the team makes clear that they have the correct patient and are performing the appropriate procedure. 13
Post-procedure quality indicators
Complications
Diagnostic UGI endoscopy is considered a remarkably safe procedure; however, it not completely devoid of complications. Previous studies have shown an overall adverse events (AE) rate for diagnostic EGD ranging between 1 in 200 to 1 in 10,000 procedures, and mortality rate ranging from none to 1 in 2000.41,77–80
The most common AEs in UGI endoscopy (up to 60%) are of cardiopulmonary origin. with an incidence rate ranging from 1 in 170 to 1 in 10,000 procedures.41,80 Typical examples of such complications include hypoxemia, aspiration pneumonia, hypo- and hypertension, vaso-vagal reactions, and arrhythmias. 42 Other procedure-related complications include perforation – a potentially life-threatening event – reported to be as low as 0.0009% to 0.05%,43,80 and mucosal bleeding, occurring mostly from mucosal lacerations and tears at the GEJ, which occur in less than 0.5% of diagnostic UGI endoscopies. 44
The occurrence of AEs should be closely monitored in endoscopy units and documented in the reporting system. BSG recommends that complications, both related to the procedure or associated with the use of sedation, should be audited annually with a recorded 8-day readmission and 30-day mortality rate after EGD. 11
Patient satisfaction
Patients satisfaction is an increasingly recognized quality indicator in endoscopy. In modern medicine, the performance measures are gradually shifting from the health providers’ perspective to the view of patient experience. Patient satisfaction facilitates higher willingness to return for a follow-up examination, 45 and some evidence from colonoscopy studies shows that better quality procedures are delivering better patient experience. 46
To date, a wide range of approaches have been developed to assess patients’ experience in endoscopy. Most of the available methods measure overall satisfaction with Likert scales, visual analog scales (VAS), and questionnaires. 81 Very rarely, these methods include practical aspects affecting patient experience such as preparation process, waiting time, and post-procedure issues, including communication of results. 81
A commonly used questionnaire for endoscopy is the modified Group Health Association of America-9 survey (mGHAA-9); however, this questionnaire is being criticized for not including pain control. 82 Recently, a Gastrointestinal Endoscopy Satisfaction Questionnaire (GESQ) was developed and validated. 83 This scoring system includes 21 questions categorized into four domains, including information before endoscopy, endoscopist skills, pain or discomfort during or after endoscopy, and information after endoscopy. Another common approach includes endoscopy nurses assessing patient comfort using the Modified Gloucester Scale (1 = no discomfort to 5 = severe discomfort).
Several measures can be undertaken to improve patient experience. A meta-analysis suggested that music may offer benefits for patients undergoing endoscopy, 84 and providing an information brochure on UGI endoscopy at least 1 day before the procedure has been shown to result in less anxiety and greater satisfaction after the procedure. 85
Missed UGI cancer rate
EGD is the gold standard for UGI cancer diagnosis; however, it remains a highly operator-dependent procedure with a significant rate of missed UGI neoplastic lesions. A recent meta-analysis showed that up to 11.3% of UGI cancers might be missed during this examination. 15 A commonly used definition for missed UGI cancer is cancer diagnosed within 3 years after an EGD with no evidence of neoplastic disease. The rate of missed UGI cancers is highly variable among reports, and this is most likely related to methodological and epidemiological variances among the studies. Most of the reports analyzing this issue of missed UGI cancers are single-institutional retrospective studies with limited cohorts. For example, an Australian study based on cross-linking EGD data with cancer registries showed a prevalence of missed UGI cancers on a level of 6.7%. 86 To compare, a Japanese report with a similar methodology showed a prevalence of 25.8% just for missed gastric cancers. 87 These differences can be explained by a higher prevalence of gastric cancer in the Asian populations, but also different histological criteria for gastric cancer in Japan.
The issue of missed GI cancers has already been highlighted in the field of colonoscopy. The rate of post-colonoscopy cancers is an established and important quality metric, strictly associated with other performance measures, such as the adenoma detection rate.9,10 In contrast to lower GI tract, UGI cancers represent a more heterogeneous group of diseases with different biology and incidence, which may hinder monitoring and drawing firm conclusions. Nevertheless, BSG recommends that endoscopy units should include audit rates of failing to diagnose cancer at UGI endoscopy up to 3 years before an esophagogastric cancer is diagnosed. 11
Conclusion
EGD remains a highly operator-dependent procedure, and the issue of quality in UGI endoscopy is increasingly discussed. Adherence to quality standards may facilitate a better experience for the patient and, potentially, reduce the number of pathologies missed during routine EGDs. A high-quality examination commences with adequate preparation of the patient, including proper fasting instructions, assessment of fitness, and tailoring sedation accordingly to the procedural requirements. Defoaming agents digested before the procedure can be considered, especially in patients undergoing surveillance for high-risk conditions. For the first diagnostic EGD, it is recommended to spend at least 7 min from intubation to extubation, and obtain a set of at least 10 pictures, including all anatomical landmarks. Any additional pathology should be adequately reported (e.g. with the use of Paris classification), photo-documented, and biopsied separately whenever appropriate. Advanced imaging techniques, including conventional and virtual chromoendoscopy, are increasingly available and characterize a high-quality procedure when used in the right setting by a properly trained endoscopist.
Lack of standardization remains a significant limitation of the EGD; therefore, biopsy protocols such as the Sydney protocol for chronic gastritis or Seattle protocol for BE surveillance have been introduced to uniform the management of high-risk UGI conditions and maximize the procedural diagnostic yield. These protocols, however, seem to be rarely followed in the community-based endoscopy setting. 88 Artificial intelligence might have a great impact on the standardization of UGI endoscopy; however, this technology seems to be still in the early stages of implementation and to require validation in rigorously designed trials to be fully accepted in everyday endoscopy practice.
Footnotes
Author contributions
Literature review (WJ), drafting of manuscript (WJ), critical revision of manuscript (WJ, MFK). Both authors approved the final version of the article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.