
Abstract
Background:
Barrett’s esophagus (BE) is a premalignant condition, caused principally by gastroesophageal reflux disease (GERD). Anti-reflux mucosectomy (ARMS) is an effective endoscopic treatment for GERD-related BE, utilizing scar tissue in the area of the esophagogastric junction, narrowing the gastric cardia. Thus, an anti-reflux barrier is formed, which obstructs the reflux of gastric contents into the esophagus.
Objectives:
Therefore, in this study, we investigated whether GERD-related BE improved post-ARMS by analyzing the changes in lower esophageal sphincter (LES) pressure, Hill’s classification for GERD, and GERD-related questionnaires.
Design:
In this retrospective study, we observed whether ARMS was superior to argon plasma coagulation (APC) in the management of GERD disease-related BE.
Methods:
Ninety-five patients were grouped into two cohorts, with 43 and 52 in the ARMS and APC cohorts, respectively. Four GERD-related questionnaires were administered. The anxiety self-rating scale (SAS) and depression self-rating scale (SDS) were used for the psychological evaluation of both cohorts. Endoscopic manifestations of BE were observed, and Hill’s classification for GERD was employed. Moreover, high-resolution esophageal manometry was performed to test esophageal motility. The follow-up period was 6 months post-treatment.
Results:
Greater statistically significant improvements in the four GERD-related questionnaires and SAS and SDS scores were observed post-ARMS than post-APC. Lesion residue was statistically significantly lower in the post-ARMS cohort. Six months post-treatment, proton pump inhibitor use was statistically significantly higher in the ARMS cohort. Moreover, Hill’s classification grades and the LES pressure improved statistically significantly post-ARMS after this time interval. The operation time and hospitalization duration were statistically significantly longer in the ARMS cohort than in the APC cohort. However, incidence rates of adverse events were similar.
Conclusion:
ARMS is more effective than APC as an endoscopic focal mucosal resection procedure for GERD-related BE and is an optional treatment for both BE excision and GERD improvement.
Plain language summary
Barrett’s esophagus (BE) is considered a precancerous lesion of esophageal cancer, and gastroesophageal reflux disease (GERD) is deemed the main reason of BE. The common treatments for BE are destructive and mainly care of endoscopic manifestation. Anti-reflux mucosectomy (ARMS) is reported of effective for GERD, with the similar operation of endoscopic submucosal dissection (ESD) for esophagogastric junction (EGJ), it may be an optional treatment for both BE and its main etiology of GERD simultaneously. This study retrospectively investigated the effect of ARMS for GERD related BE, High resolution esophageal manometry (HREM) and endoscopy was used to evaluate the effect objectively combined with subjective questionnaires. Many positive results demonstrated it is a effective option for GERD related BE.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is a common disease with an increasing prevalence. Long-term treatment, relapse, and severe complications are typical of GERD. 1 Acid reflux, heartburn, and eructation are characteristic esophageal symptoms that are frequently observed in patients. 2 Some atypical symptoms, such as globus pharyngeus and asthma, are considered non-esophageal symptoms 3 and are usually misdiagnosed as other diseases. 4 Endoscopy is the gold standard for both definitive and differential diagnoses. In addition, this diagnostic modality enables the detection of complications, severity grading, and performance of biopsies.5,6 Questionnaire surveys are another method of diagnosing GERD, particularly non-erosive reflux disease (NERD). 7 GERD-associated symptoms and severity can be quantified using surveys, and questionnaire scores can be statistically calculated for accurate diagnosis and treatment references. 8 High-resolution esophageal manometry (HREM) is an auxiliary yet effective diagnostic method for GERD that focuses on esophageal motility and anti-reflux valve function. 9 The combination of endoscopy, quantitative surveys, and HREM is a comprehensive diagnostic method for GERD and the complications thereof. 10
Barrett’s esophagus (BE) is a recognized premalignant esophageal lesion, characterized by columnar squamous epithelium. 11 Epidemiological studies have established that prolonged GERD is a major risk factor for BE and neoplastic changes. Other risk factors include increasing age, male sex, European race, abdominal obesity, cigarette smoking, and lack of infection with Helicobacter pylori.12 –14
Proton pump inhibitors (PPIs) are useful in the treatment of GERD; however, reversing BE remains challenging with the use thereof. Moreover, long-term medical management is essential for mucosal repair, 15 particularly involving the novel potassium-competitive acid inhibitor (P-CAB). 16 Surgery is not appropriate for the management of GERD, particularly in the absence of the risk of cancer. Many endoscopic modalities, such as argon plasma coagulation (APC), 17 radiofrequency ablation (RFA), 18 and photodynamic therapy (PDT), 19 are beneficial for curing or delaying the progression of BE.
However, these common therapeutic modalities for BE are damaging and destroying the mucosal lesion only. Furthermore, GERD is ignored as a potentially important cause for the progression of BE into cancer. Consequently, BE is re-diagnosed with an endoscopic review. Endoscopic submucosal dissection (ESD) prevents BE recurrence20,21; nevertheless, the effect on GERD has not yet been elucidated. Anti-reflux mucosectomy (ARMS) is an effective endoscopic treatment for GERD, which utilizes scar tissue in the area of the esophagogastric junction (EGJ) post-ESD, narrowing the gastric cardia. Thus, an anti-reflux barrier is formed, which obstructs the reflux of gastric contents into the esophagus. 22 Therefore, in this study, we investigated whether GERD-related BE improved post-ARMS by analyzing the changes in lower esophageal sphincter (LES) pressure, Hill’s classification for GERD, and GERD-related questionnaires.
Materials and methods
Ethical approval and informed consent
This study was approved by the (Ethics Committee (EC)) of (Suining Central Hospital) on the (December 26, 2023), with the (EC) approval number: (LLSLH20220070). Moreover, this study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from the patients for the publication of their de-identified data and images.
Study design and population
This was a single-center, retrospective case–control study. Patients from the Suining Central Hospital were retrospectively selected from February 15, 2023 to December 26, 2023. The selection flow chart is presented in Figure 1. Ninety-five patients were grouped into two cohorts, with 43 and 52 in the ARMS and APC cohorts, respectively.
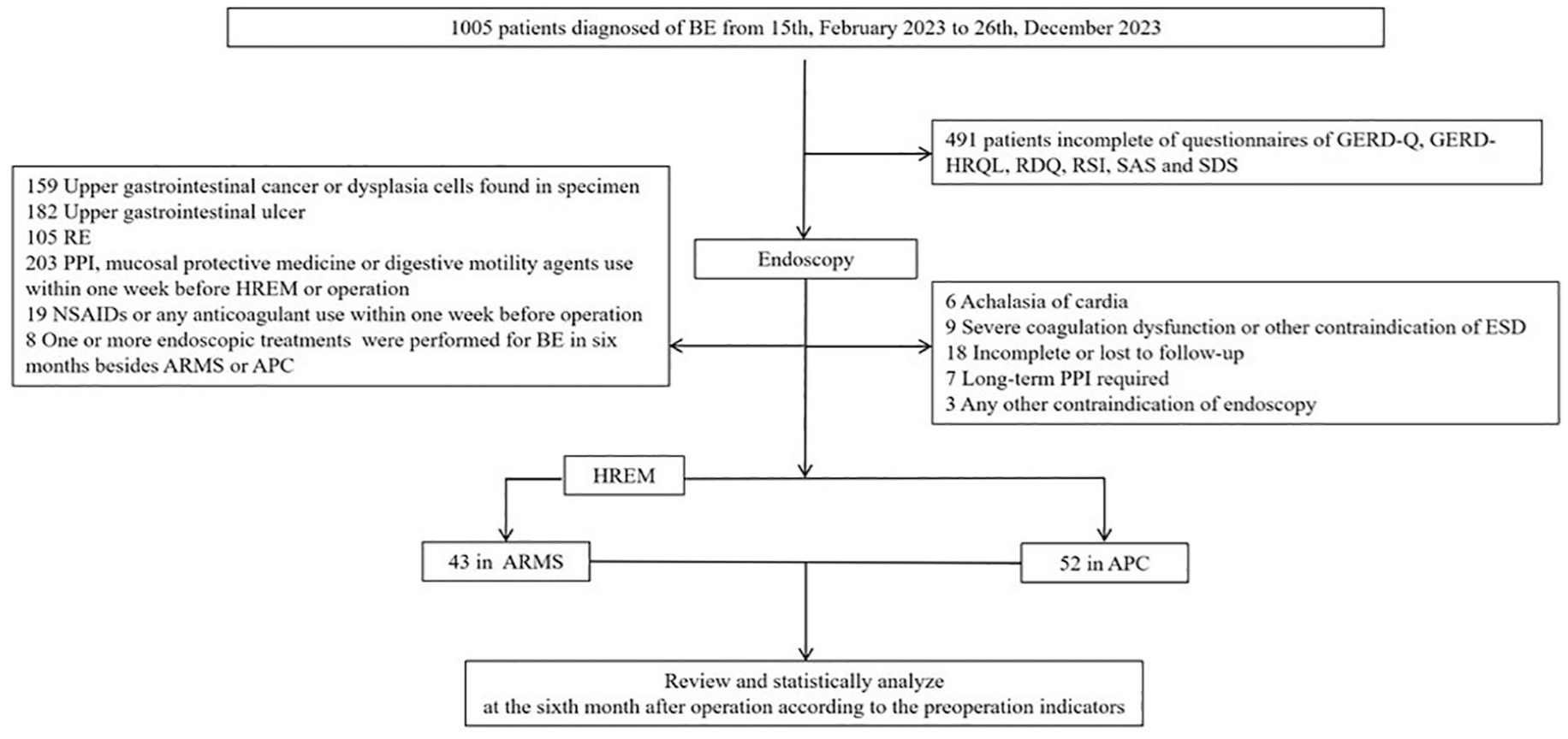
The selective flow chart of the study.
The inclusion criteria were as follows: (1) patients who had undergone endoscopic management for BE who had been surveyed using the Gastroesophageal Reflux Disease Questionnaire (GERD-Q), Gastroesophageal Reflux Disease Health-Related Quality of Life (GERD-HRQL) questionnaire, Reflux Disease Questionnaire (RDQ), and Reflux Symptom Index (RSI) to make a definitive diagnosis of GERD; (2) efficacy of PPIs was not satisfactory; (3) data from the anxiety self-rating scale (SAS) and depression self-rating scale (SDS) were available; (3) either ARMS or APC was accepted for BE endoscopic treatment after consensus; and (4) HREM had been performed to test the esophageal motility in the patients who consented to ARMS.
The exclusion criteria were as follows: (1) patients diagnosed with upper gastrointestinal cancer or severe dysplastic cells, as per the excised specimen; (2) patients with an upper gastrointestinal ulcer; (3) patients with endoscopically confirmed reflux esophagitis; (4) use of PPIs, mucosal protective medicines, or digestive motility agents at 1 week pre-HREM or preoperatively; (5) use of non-steroidal anti-inflammatory drugs or any anticoagulants 1 week preoperatively; (6) one or more endoscopic modalities apart from ARMS or APC performed for BE at 6 months preoperatively; (7) patients with achalasia of cardia; (8) patients with severe coagulopathies or other contraindications to ESD; (9) incomplete data or loss to follow-up; (10) patients with other serious conditions requiring long-term oral PPIs; and (11) patients with any other contraindications to endoscopies.
Questionnaires and surveys
Questionnaires have been widely used to diagnose GERD, particularly when NERD is diagnosed post-endoscopy; each questionnaire focuses on different concerns. Conditions can present within the esophagus and can involve systems external to the esophagus, 23 such as in the case of reflux pharyngitis, asthma, and sleep apnea. A combination of surveys is effective in diagnosing GERD, manifesting in different systemic symptoms. To decrease the risk of misdiagnosis, four different questionnaire scores were used to ensure an accurate diagnosis and to include all symptoms as completely as possible. Moreover, BE is a widely regarded precancerous lesion that may aggravate anxiety and depressive symptoms. To further encompass all symptoms, SAS and SDS scores were additionally applied in this study. Many studies have shown that the patients’ psychological scores are correlated with GERD-related manifestations. 24 The SAS and SDS scores are usually used to evaluate for potential diseases, and an initial checkup of patients’ psychological conditions and GERD-like symptoms could help screen for latent disorders in outpatients. 25
Hill’s classification
This study used Hill’s classification, as described by Hill et al. 26 as follows: Grade I, the tissue edge ridge is obvious and tightly encases the endoscope along the lesser curvature; Grade II, the edge ridge is not as obvious as that in Grade I, but occasionally opens with respiration and closes rapidly; Grade III, the edge ridge is almost nonexistent and cannot tightly encase the endoscope; Grade IV, there is no ridge at all, the gastroesophageal area is open, and the esophageal squamous epithelium is readily visible in the reversed view (Figure 2).

The Hill classification gradient. (a) The endoscopy manifestation of Grade I. (b) The endoscopy manifestation of Grade II. (c) The endoscopy manifestation of Grade III. (d) The endoscopy manifestation of Grade IV.
Surgical and medical interventions
The endoscopic cardiac sphincter valve gradient was first recorded, and ESD was performed to dissect the BE and phase-continuous half-circle tissues around the dental line in the ARMS cohort. APC was performed to damage the BE lesions in the APC cohort (Figure 3). Two experienced gastroenterologists performed the ARMS and APC procedures. PPIs, such as esomeprazole sodium, were administered for 4 weeks postoperatively to prevent wound bleeding. Further PPIs were administered as required, for relief of symptoms.

The endoscopy and treatments. (a) BE before ARMS. (b) Cardia valve before ARMS. (c) The wound from esophageal vision. (d) The wound from gastric vision (red arrow: mucosa in ARMS; yellow arrow: the wound of ARMS). (e) Endoscopy review of cardia valve. (f) Endoscopy review of BE healing after ARMS. (g) The vitro mucosa after ARMS. (h) BE before APC. (i) Cardia valve before APC. (j) The wound of APC. (k) The cardia valve after APC. (l) Endoscopy review of BE healing after APC.
Data collection and definitions
Six months post-treatment, questionnaires involving symptom scores were administered. Moreover, endoscopic reviews were performed to evaluate wound healing, using Hill’s classification. Regarding the ARMS cohort, HREM was reviewed to compare motility data. Lesion residue was defined as the presence of BE at the same location during the endoscopic review at the 6-month interval, post-ARMS, or post-APC, regardless of any changes in size.
Statistical analysis
Measurement data with normal distributions were expressed as (
Results
Clinical baseline characteristics
The baseline clinical characteristics revealed no statistically significant differences between the two cohorts regarding sex, age, symptom questionnaire scores, and endoscopic manifestations (Table 1).
The baseline of clinical characteristics.

APC, argon plasma coagulation; ARMS, anti-reflux mucosectomy; BMI, body mass index; CBE, circle Barrett’s esophagus; GERD-Q, Gastroesophageal Reflux Disease Questionnaire; GERD-HRQL, Gastroesophageal Reflux Disease Health-Related Quality of Life; LSBE, long segment Barrett’s esophagus; RDQ, Reflux Disease Questionnaire; RSI, Reflux Symptom Index; SAS, anxiety self-rating scale; SDS, depression self-rating scale; SSBE, short segment Barrett’s esophagus.
Effects of ARMS and APC
Greater statistically significant improvements in GERD-Q (p = 0.02), GERD-HRQL questionnaire (p = 0.03), RDQ (p = 0.002), RSI (p = 0.04), SAS (p = 0.003), and SDS (p = 0.01) scores were observed post-ARMS than post-APC. Complete and partial symptomatic relief were observed more post-ARMS than post-APC (p = 0.002), with a higher rate of PPI-use post-ARMS (p = 0.01). The endoscopic lesion residue was statistically significantly lower than that with APC (p < 0.001; Table 2).
The effects between ARMS and APC.

APC, argon plasma coagulation; ARMS, anti-reflux mucosectomy; GERD-HRQL, Gastroesophageal Reflux Disease Health-Related Quality of Life; GERD-Q, Gastroesophageal Reflux Disease Questionnaire; PPI, proton pump inhibitors; RDQ, Reflux Disease Questionnaire; RSI, Reflux Symptom Index; SAS, anxiety self-rating scale; SDS, depression self-rating scale.
Questionnaires and outcomes of ARMS
Six months post-ARMS, statistically significant changes were observed in the GERD-Q, GERD-HRQL questionnaire, RDQ, RSI, SAS, and SDS scores (Figure 4). Moreover, HREM and endoscopy were reviewed at the 6-month interval. The HREM review revealed a statistically significant increase in the LES pressure post-ARMS and a statistically significant decrease in the upper esophageal sphincter (UES) pressure and relaxation percentage. An endoscopic review showed a superior improvement in the Hill classification grades post-ARMS but not post-APC (Figure 5).
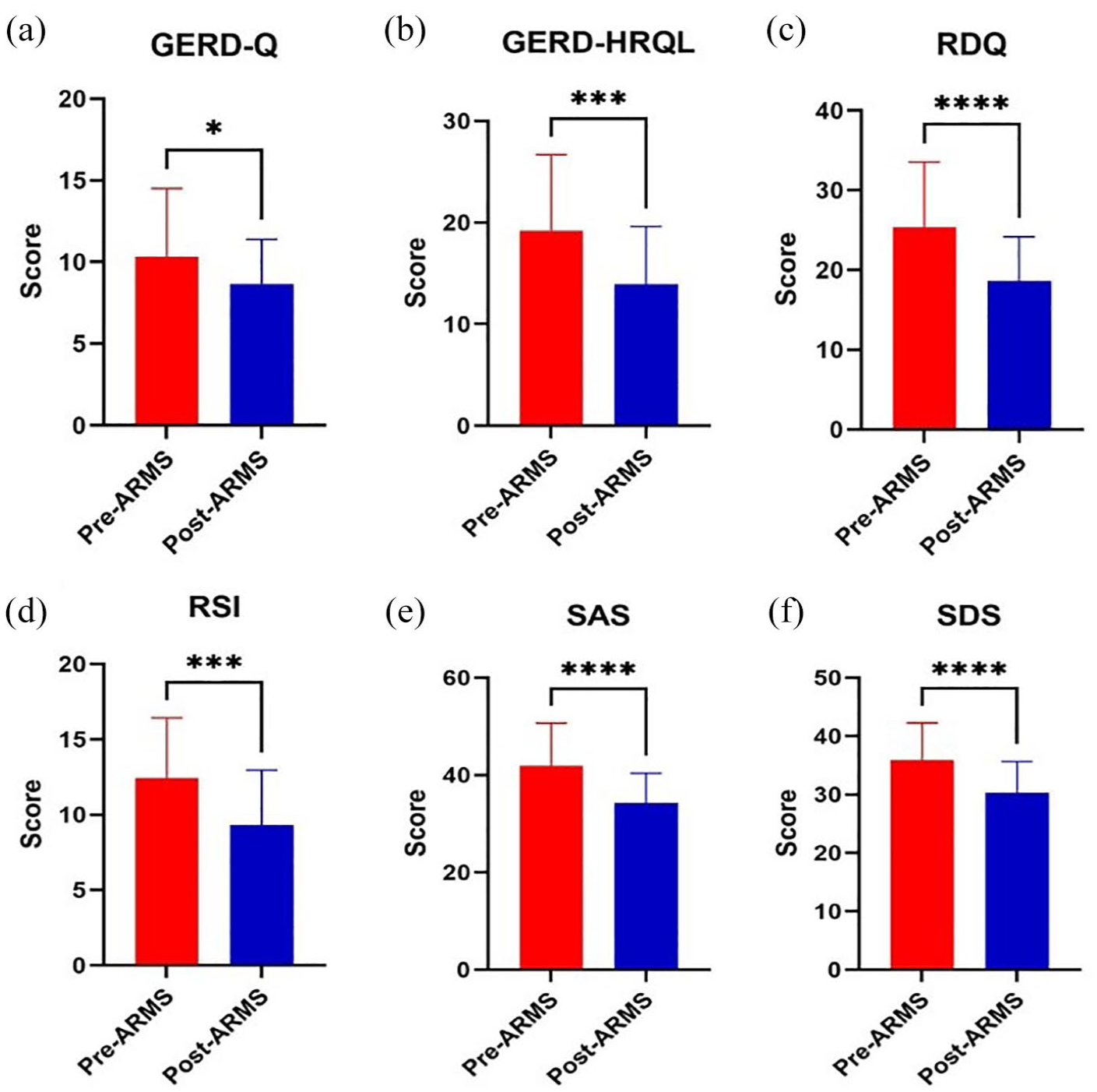
The questionnaires change after ARMS. (a) The GERD-Q score changes after ARMS. (b) The GERD-HRQL score changes after ARMS. (c) The RDQ score changes after ARMS. (d) The RSI score changes after ARMS. (e) The SAS score changes after ARMS. (f) The SDS score changes after ARMS.

The HREM and Hill gradient change after ARMS. (a) The LES position changes after ARMS. (b) The LES pressure changes after ARMS. (c) The UES pressure changes after ARMS. (d) The UES relaxation changes after ARMS. (e) The EGI-type changes after ARMS. (f) The Hill gradient changes after ARMS.
Surgical-associated events
Surgical-associated events showed statistically significantly longer operative times (p < 0.0001) and hospitalization stays (p < 0.0001) in the ARMS cohort than in the APC cohort. Delayed bleeding occurred 1 week post-discharge and was successfully treated using endoscopic electrocoagulation. Furthermore, cardiac stenosis occurred 2 months post-discharge, which improved post-balloon dilatation. No statistically significant adverse events were observed between the two cohorts (Table 3).
The operation-associated events.

APC, argon plasma coagulation; ARMS, anti-reflux mucosectomy.
Discussion
Symptomatic GERD manifesting either internally or externally of the esophagus affects the patient’s quality of life. Moreover, complications resulting from GERD lead to more severe outcomes. Thus, the timely diagnosis and treatment of these symptoms and complications play important roles in the prognosis of GERD. In this study, as per the administered questionnaires, GERD symptoms improved more in the ARMS cohort than in the APC cohort. Regarding Hill’s classification and lesion residue, endoscopic management and efficacy were superior in the ARMS cohort than in the APC cohort. Regarding HREM, improvement in the LES pressure was greater in the ARMS cohort than in the APC cohort. This may be accounted for by the more effective ARMS treatment for GERD-related BE.
A greater decrease was observed in the GERD scores post-ARM than post-APC, with greater complete and partial symptomatic relief post-ARMS. Moreover, SAS and SDS scores statistically significantly decreased post-ARMS.
Currently, many treatments for GERD focus on the inhibition or prevention of gastric acid secretion, and anti-reflux barriers are mentioned only when surgery becomes necessary. LES plays an important role in GERD development. 27 As GERD severity increases, motor dysfunction of the LES and esophageal body gradually worsens. Decreased UES pressure plays an important role in the occurrence of extraesophageal symptoms, which are more noticeable in patients with globus pharyngeus. 28 BE, one of the most important complications, is usually ignored and disregarded as a superficial mucosal lesion isolated from GERD. 29 Furthermore, BE usually persists when endoscopy is reviewed despite the use of many treatments. With a deeper understanding of the development thereof, BE is an important endoscopic manifestation with the same reference value as Hill’s classification for GERD diagnosis. Moreover, BE is considered the result of GERD. The cancer risk and mechanism of BE remain unclear; however, thorough treatment thereof is necessary. Current therapies for BE include medical and endoscopic treatments. The focus of medical treatment is to decrease gastric acid secretion, which may not be sufficient for managing BE. 30 A high failure rate ensues, due to a lack of change of the LES. The long-term use of PPIs or P-CABs is required,31,32 and adherence becomes a challenge. In this study, patients who received PPIs and digestive motility agents pre-HREM were excluded, to ensure the accuracy of the LES test. PPIs were used for 4 weeks postoperatively, which was only for wound bleeding prevention and not for BE treatment.
Endoscopic treatment modalities are considered more useful for BE eradication. The typical destructive treatment is APC, which offers the advantages of speed, simplicity, safety, and effectiveness, particularly in the management of short-segment BE. 33 Moreover, RFA 34 and PDT 19 are also used for BE endoscopy, albeit less frequently than APC. Eradication therapies are commonly recommended, with the advantages of greater efficacy and lower recurrence rates. Endoscopic mucosal resection and ESD are both effective for BE eradication. ESD is believed to be more effective, particularly when intraepithelial neoplasia is complicated. 35 ARMS is reportedly effective for GERD, the mechanism of which is to improve the anti-reflux valve through scar hyperplasia repair post-ESD around the EGJ. 36 During the healing process, the exposed subcutaneous tissue and formed hypertrophic scars lead to the contraction of the LES. 37 In this study, BE lesions were included in the excision range, and the repair results demonstrated a lower recurrence rate for ARMS than for APC. Because of submucosal treatment involved in ARMS, LES pressure was increased by HREM review, and the anti-reflux valve was improved after endoscopy. In addition, UES relaxation improved, with fewer reflux events. The subjective and psychological scores of the GERD improved as a result of the above objective changes.
Adverse events included delayed bleeding at 1 week post-discharge and cardiac stenosis at 2 months post-discharge from the hospital. The delayed bleeding was successfully treated using endoscopic electrocoagulation; cardiac stenosis was treated by endoscopic balloon dilation, once endoscopy was reviewed. No other severe adverse effects were observed during follow-up.
Study limitations
This study had some limitations that require further refinement. First, fewer samples were included in this study, which may have led to the absence of some types of abnormal esophageal movement or statistical bias. Second, a 6-month follow-up period is insufficient for the evaluation of a potential cancerous disease. Third, HREM is not encompassed in APC, because APC is considered as a solely destructive method for managing precancerous lesions. Clinically, this may not be so necessarily deemed; however, this factor may be a flaw in the APC cohort. Other treatments for BE should be included in further research. Nevertheless, we have planned a prospective, multicenter, randomized controlled trial to evaluate whether this treatment offers greater benefits for GERD-related BE. The planned study will include HREM, gastric acid monitoring, other endoscopic treatments, and a long-term follow-up.
Conclusion
Definitively, ARMS may be a more effective endoscopic eradication approach than APC for treating GERD-related BE. In addition, HREM and Hill’s classification can serve as objective references alongside subjective questionnaire scores.
Footnotes
Acknowledgements
We would like to thank all the study participants for agreeing to participate in the medical research and all the staff of the Endoscopy Center and Pathology Department in Suining Central Hospital affiliated with Chongqing Medical University for the operation and for providing pathological specimens. We also would like to thank Xi Zheng for the paper structure suggestion from the Department of Gastroenterology, Chongqing University Cancer Hospital.