
Abstract
Faecal microbiota transplantation (FMT) is increasingly used for diseases associated with a disrupted intestinal microbiome, mainly Clostridioides difficile infection. Encapsulated FMT is a patient-friendly application method that improves accessibility and convenience. Capsule processing may be standardised, but validation protocols are warranted. This review aimed to describe published validation methods for encapsulated FMT. Original studies reporting using encapsulated faecal formulations were included, regardless of indication. Studies were excluded if they did not address processing and validation or used non-donor-derived content. We conducted a comprehensive scoping review, implementing a systematic search strategy in PubMed, Embase and Web of Science. Processing data and validation methods were registered during full-text analysis and combined to create an overview of approaches for assessing quality in encapsulated FMT processing. The searches identified 324 unique studies, of which 44 were included for data extraction and analysis. We identified eight validation covariables: donor selection, pre-processing, preservation, oxygen-sparing processing, microbial count, viability, engraftment and clinical effect outcomes, from which we constructed a model for quality assessment of encapsulated FMT that exhaustively categorised processing details and validation measures. Our model comprised three domains: (1) Processing (donor selection and processing protocol), (2) Content analysis (microbiota measures and dose measures) and (3) Clinical effect (engraftment and clinical outcomes). No studies presented a reproducible capsule protocol; their validation strategies were sparse and divergent. The validation of FMT capsules is heterogeneous, and processing requires relevant standardisation protocols, mainly focusing on capsule content. Future studies should report validation covariables to enable accurate comparative assessments of clinical effects.
Plain language summary
Faecal microbiota transplantation (FMT) is a life-saving therapy, based on the transfer of intestinal microbiota from a healthy donor to a patient to treat disease. Encapsulation of donor faeces eases the application of FMT, but methods to evaluate the quality of encapsulated FMT are not standardised. Based on a systematic literature review, we here provide a comprehensive overview of factors that may influence the quality of encapsulated FMT. We describe three main domains that together form a model for standardisation: 1. Processing (donor selection and processing protocol), 2. Content analysis (microbiota measures and dose measures) and 3. Clinical effect (engraftment and clinical outcomes). These domains may be addressed in future studies that report the use of encapsulated FMT.
Keywords
Introduction
Faecal microbiota transplantation (FMT) is the transfer of intestinal microbiota and metabolites from a healthy donor to a recipient suffering from diseases due to a compromised intestinal microbiome. 1
Intestinal microbiota modulation through FMT is an effective treatment against Clostridioides difficile infection (CDI). Since the first randomised trial demonstrated an extensive benefit of FMT over vancomycin monotherapy for recurrent CDI, 2 multiple randomised controlled trials,2–8 cohort studies9–13 and meta-analyses 14 have confirmed effect rates above 90% and superiority to standard antibiotic treatments. Despite this evidence, a European survey from 2021 found that less than 10% of patients with recurrent CDI received FMT, 15 indicating a significant underuse. The use of FMT is expanding rapidly due to emerging evidence of its benefit in treating ulcerative colitis (UC) 16 along with its potential in experimental indications such as Parkinson’s disease17,18 and graft-versus-host disease.19,20 The current underuse of FMT in CDI and its potential future demand for new indications necessitate improved access and standardised, clinically validated processing protocols.
Traditional FMT administrations involve direct infusion of liquid-suspension faecal material by nasoduodenal tube, colonoscopy or enema. Encapsulated FMT is a patient-friendly administration form with reduced invasiveness, 21 improved feasibility and decreased total costs; moreover, it confers effect rates comparable to those obtained with other application forms. 22 Accordingly, the use of encapsulated FMT has increased in recent years. Still, a standardised preparation protocol for encapsulated FMT has yet to be published, and there is currently no international consensus on the validation of FMT capsule preparations.
Validation of the processing methods is a pivotal first step in standardising encapsulated FMT components, requiring a multifaceted approach that comprehensively evaluates the entire FMT value chain from donor screening to faeces processing to clinical outcomes. While previous studies have focused on standardising donor selection23,24 and clinical outcomes, 22 further explorations are needed to analyse the contents of the FMT components, that is, encapsulated faeces or liquid faeces, during the faeces processing stage. Because encapsulated FMT preparations are more processed than traditional liquid suspensions, identifying which processing steps may influence the clinical outcomes is critical.
This study aimed to provide a comprehensive overview of the currently published validation methods for encapsulated FMT by reviewing the existing literature.
Methods
This study was reported to conform to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) statement 25 (Supplemental Table 1). We systematically searched the current literature on methods used to validate encapsulated formulations for FMT. The search strategy was made according to the PRISMA-ScR guideline and applied to PubMed, Embase and Web of Science databases on 26 April 2024.
The search thread was created using synonyms, including MeSH terms in PubMed and Emtree terms in Embase (the search terms are listed in Table 1). The synonyms were separated by the ‘OR’ operator, and synonym groups were combined by the ‘AND’ operator. The resulting records were imported and managed in Covidence (Covidence systematic review software; Veritas Health Innovation, Melbourne, Australia) to eliminate duplicates and facilitate title, abstract and full-text screening for eligibility plus data extraction.
A systematic literature search using predefined search terms was applied to the databases PubMed, Embase and Web of Science on 26 April 2024.

Relevant references not found by the search strategy were identified through other sources, including reference lists, PubMed searches on ‘similar articles’, a Web of Science search with citation ranging and recommended articles. Only the references that met the inclusion criteria were included in data extraction.
Inclusion and exclusion criteria were defined according to the PICOS (Population, Intervention, Comparison, Outcome, Study design) criteria 26 and they are listed in Table 2. Inclusion criteria were studies using donor-derived encapsulated FMT applications on human targets, regardless of indication. Only peer-reviewed records with original data and a capsule processing or validation description were included. Exclusion criteria were studies with FMT administrations other than capsules (e.g. tube or colonoscopy), studies without human targets and studies that did not address the donor selection, faeces processing or validation of the encapsulated formulations. Studies without original data and grey literature were excluded.
Inclusion and exclusion criteria were defined based on the PICOS criteria. 27

FMT, faecal microbiota transplantation; PICOS, Population, Intervention, Comparison, Outcome, Study design.
Study details, capsule processing details, validation methods and covariables were thoroughly registered during full-text data extraction. In addition to presenting the data in relevant tables, the study data were implemented in the EPPI Reviewer software 28 to provide an interactive Evidence Gap Map. 29
Results
Study inclusion
We identified 549 records (PRISMA-ScR flowchart in Figure 1). The records were imported into the systematic review software Covidence, and 225 duplicates were removed, leaving 324 unique records. Title and abstract screening excluded 236 records for reasons listed in Figure 1. The remaining 88 records were subjected to full-text screening for eligibility, and after the exclusion of 47 records, 41 records passed the inclusion and exclusion criteria (see Table 2). An additional 3 records were identified through other sources, resulting in 44 records for data extraction and analysis in this review.

PRISMA-ScR flow diagram detailing searches for PubMed, Embase and Web of Science, title/abstract screening, full-text screening for eligibility and data retrieval.
Study characteristics
This scoping review included 44 studies, all presented in Table 3. The most frequent study sites were the United States (n = 20, 46%), Canada (n = 5, 11%), China (n = 4, 9%), Denmark (n = 3, 7%) and Israel (n = 3, 7%). Of the included studies, the majority were prospective cohort studies (n = 21, 48%), randomised controlled trials (n = 15, 34%) or retrospective cohort studies (n = 3, 7%). The size of the study populations ranged from 5 to 185 patients (median 30) in whom encapsulated FMT was used for 13 different indications. The studied indications were CDI (n = 21, 48%), obesity (n = 5, 11%), UC (n = 4, 9%), graft-versus-host disease (n = 3, 7%), irritable bowel syndrome (n = 2, 5%), allogeneic haematopoietic cell transplantation (n = 2, 5%), dementia (n = 1, 2%), depression or anxiety (n = 1, 2%), hepatic encephalopathy (n = 1, 2%), human immunodeficiency virus (n = 1, 2%), Crohn’s disease (n = 1, 2%), systemic lupus erythematosus (n = 1, 2%) and antibiotics-associated dysbiosis (n = 1, 2%).
Studies included in this review listed by indication.

The given size of the study population can include a group of patients receiving other treatments than encapsulated FMT, such as placebo capsules or non-encapsulated FMT.
CDI, Clostridioides difficile infection; FMT, faecal microbiota transplantation.
Validation measures
Validation methods could be divided into three exclusive domains, each comprising two categories:
Processing domain, divided into donor selection and processing protocol.
Content analysis domain, divided into microbiota measures and dose measures.
Clinical effect domain, divided into engraftment and clinical outcomes.
Domains and categories were combined to create a model, illustrated in Figure 2, that describes an exhaustive validation approach for quality control of encapsulated FMT.
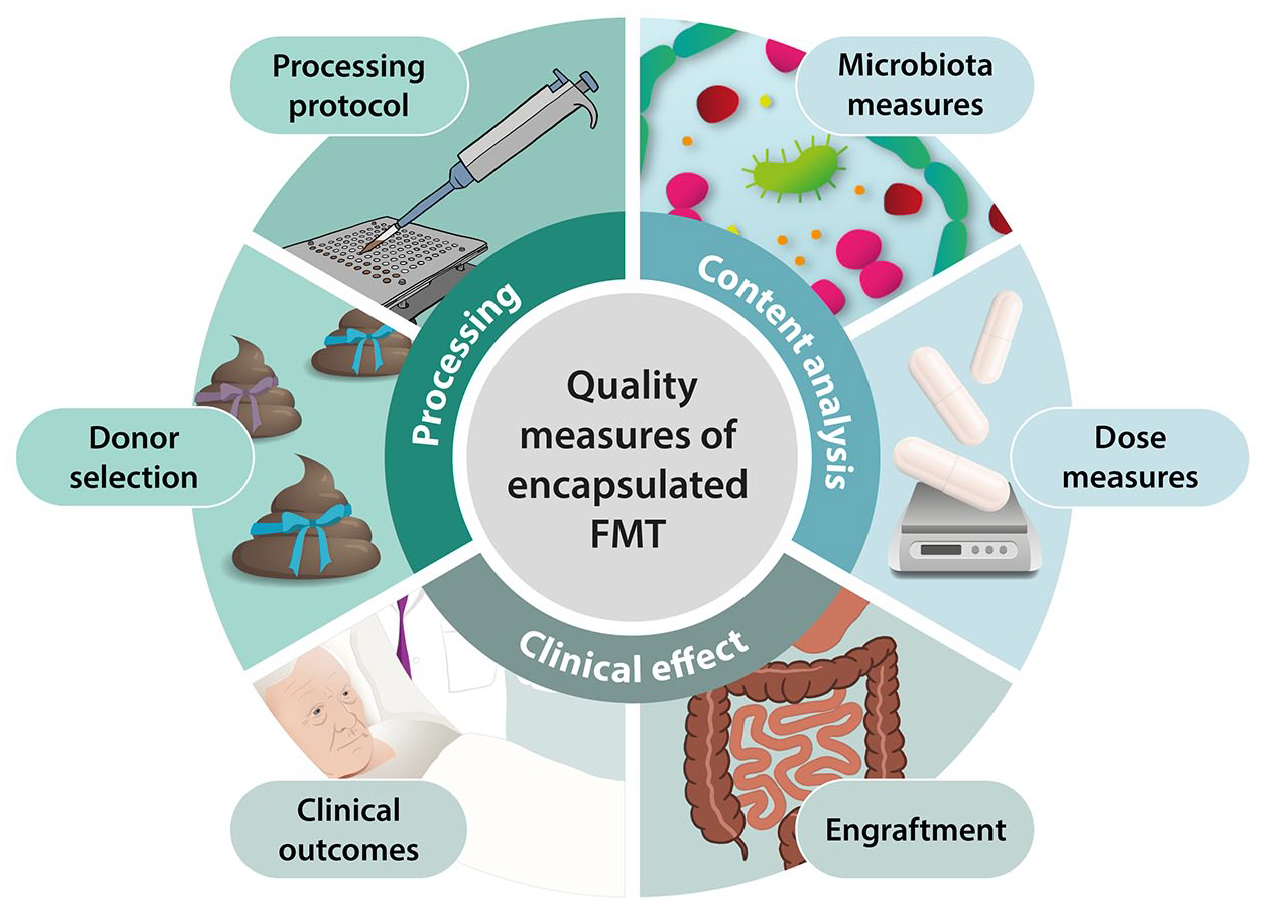
Validation model for quality measures of encapsulated FMT. The model comprises three exclusive domains (Processing, Content analysis and Clinical effect), each containing two categories. All categories combined are exhaustive for validating FMT quality.
Our quality assessment registered various covariables influencing the validation process that fell under the different domain categories in our model. The covariables were external factors that could reflect the quality of the FMT component and influence the validation process. The covariables could therefore be used as control parameters to monitor and standardise the preparation of FMT capsules, ensuring a consistent and high-quality formulation. Seven covariables for capsule validation and analysis methods were identified during data extraction, which are presented in Table 5. The identified validation covariables were four variables in the Processing domain: donor selection, pre-processing, preservation and oxygen-sparing processing – two variables in the Content Analysis domain: microbial quantification and viability measures – and one variable in the Clinical Effect domain: engraftment.
In an Evidence Gap Map, accessible at our institutional website (https://cefta.au.dk/about-fmt/efmt), we organised the study details according to the applied validation methods under the three validation domains. The interactive function of the map allows columns and rows to be folded or unfolded to enable analysis of the quantity and type of evidence related to the various validation variables.
Clinical outcomes are currently the primary measure of FMT quality as they directly reflect efficacy.
Processing domain
Donor selection
Donor selection was the most frequently registered validation covariable of all covariables. This covariable was addressed in 42 (95%) of 44 studies. Three studies used autologous FMT, and two treatments only relied on one screened donor. The remaining 37 studies screened donors by referring to different screening guidelines that were strictly defined and followed, including screening of donor health and pathogens in donor stool and blood. Donor selection mainly relies on safety parameters; still, a comparison of donor selection protocols revealed disagreements on exclusion parameters and pathogen analysis.
Processing protocol
Encapsulated FMT preparation methods were important validation targets and belonged in the processing domain for FMT quality (Figure 2). The defined covariables for this category were pre-processing, preservation and oxygen-sparing processing.
Of the 44 studies analysed, 37 (84%) utilised non-commercialised FMT preparations. The remaining seven (16%) studies incorporated manipulated, encapsulated microbiota formulations from North American companies (listed in Table 4) that we did not define as FMT preparations.
Faeces-to-capsule processing methods.
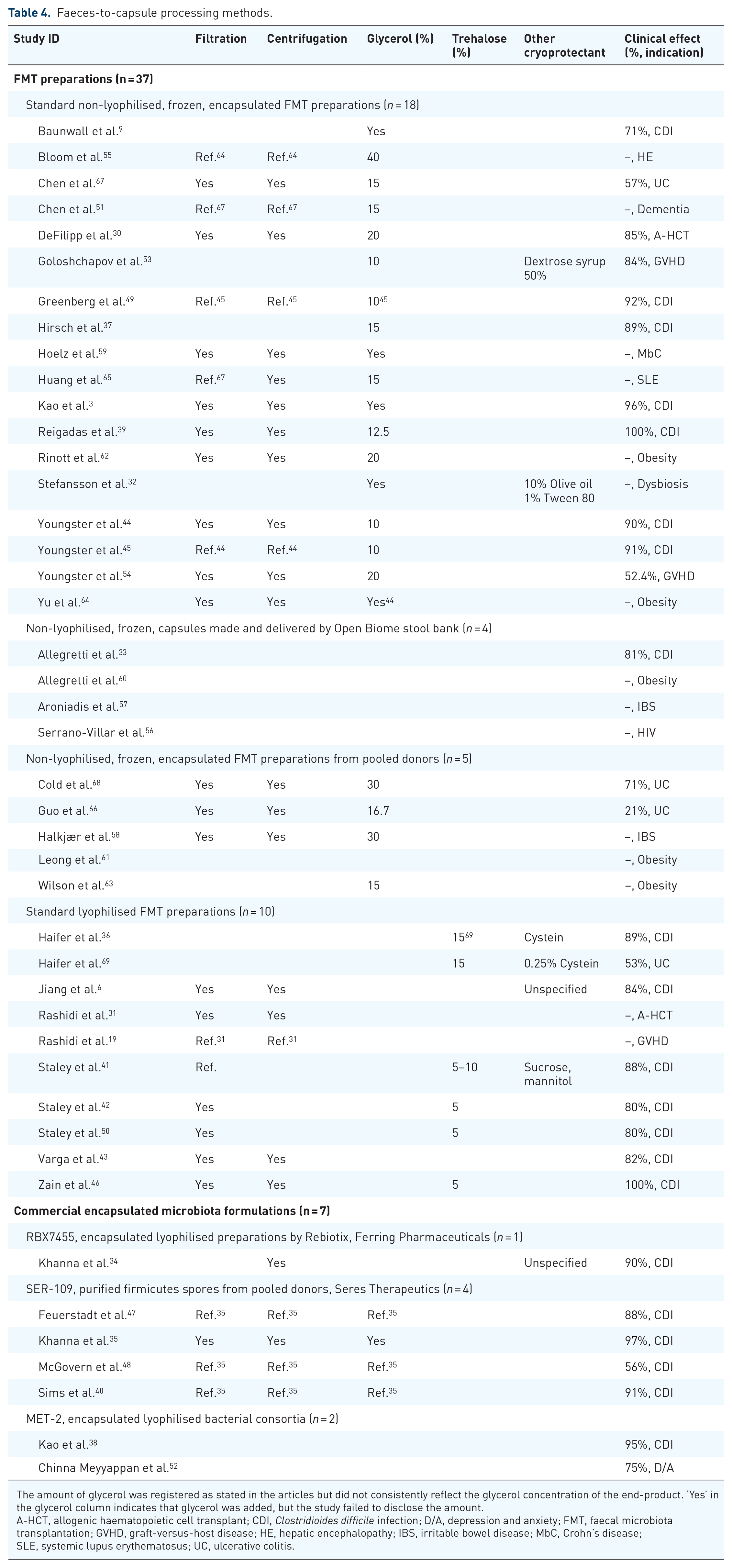
The amount of glycerol was registered as stated in the articles but did not consistently reflect the glycerol concentration of the end-product. ‘Yes’ in the glycerol column indicates that glycerol was added, but the study failed to disclose the amount.
A-HCT, allogenic haematopoietic cell transplant; CDI, Clostridioides difficile infection; D/A, depression and anxiety; FMT, faecal microbiota transplantation; GVHD, graft-versus-host disease; HE, hepatic encephalopathy; IBS, irritable bowel disease; MbC, Crohn’s disease; SLE, systemic lupus erythematosus; UC, ulcerative colitis.
The non-commercial FMT preparations were either non-lyophilised frozen preparations (n = 27, 73%) or lyophilised preparations (n = 10, 27%). The encapsulated FMT formulations were directly traceable to a single donor except for five non-lyophilised preparations58,61,63,66,68 that used pooled donations from multiple donors. Most FMT preparations were reportedly processed at the study sites, but four studies used non-lyophilised, frozen capsules provided by the Boston-based stool bank OpenBiome and did not report its processing details.
The processing details given by the studies are registered in Table 4. Most studies eliminate fibres in the first part of the protocol by filtration (n = 29, 66%) with varying pore sizes and/or centrifugation (n = 30, 68%) at varying speeds. Preservatives, including glycerol, trehalose and other cryoprotectants, were used in 34 (77%) of 44 studies. All studies with non-lyophilised FMT capsules contained glycerol as a cryoprotectant. Some studies mentioned the end-preparation glycerol concentration, while others stated the concentration before a centrifugation step, which did not reflect the end-preparation concentration. Therefore, the glycerol concentrations could not be compared across the studies.
In 10 studies with lyophilised faeces,6,19,31,36,41–43,46,50,69 6 (60%)36,41,42,46,50,69 used trehalose as the lyoprotectant, while Haifer et al.36,69 additionally added 0.25% cysteine. Staley et al. 41 tested trehalose at different concentrations with combinations of sucrose or mannitol and found that 5% trehalose alone was the optimal preservation method evaluated on preset goals for content requirements, stability and microbiota quality. One study used an unspecified lyoprotectant, 6 and two studies with lyophilised capsules did not report the use of lyoprotectants.31,43 Lyophilised capsules were mainly used in small studies (Figure 3).
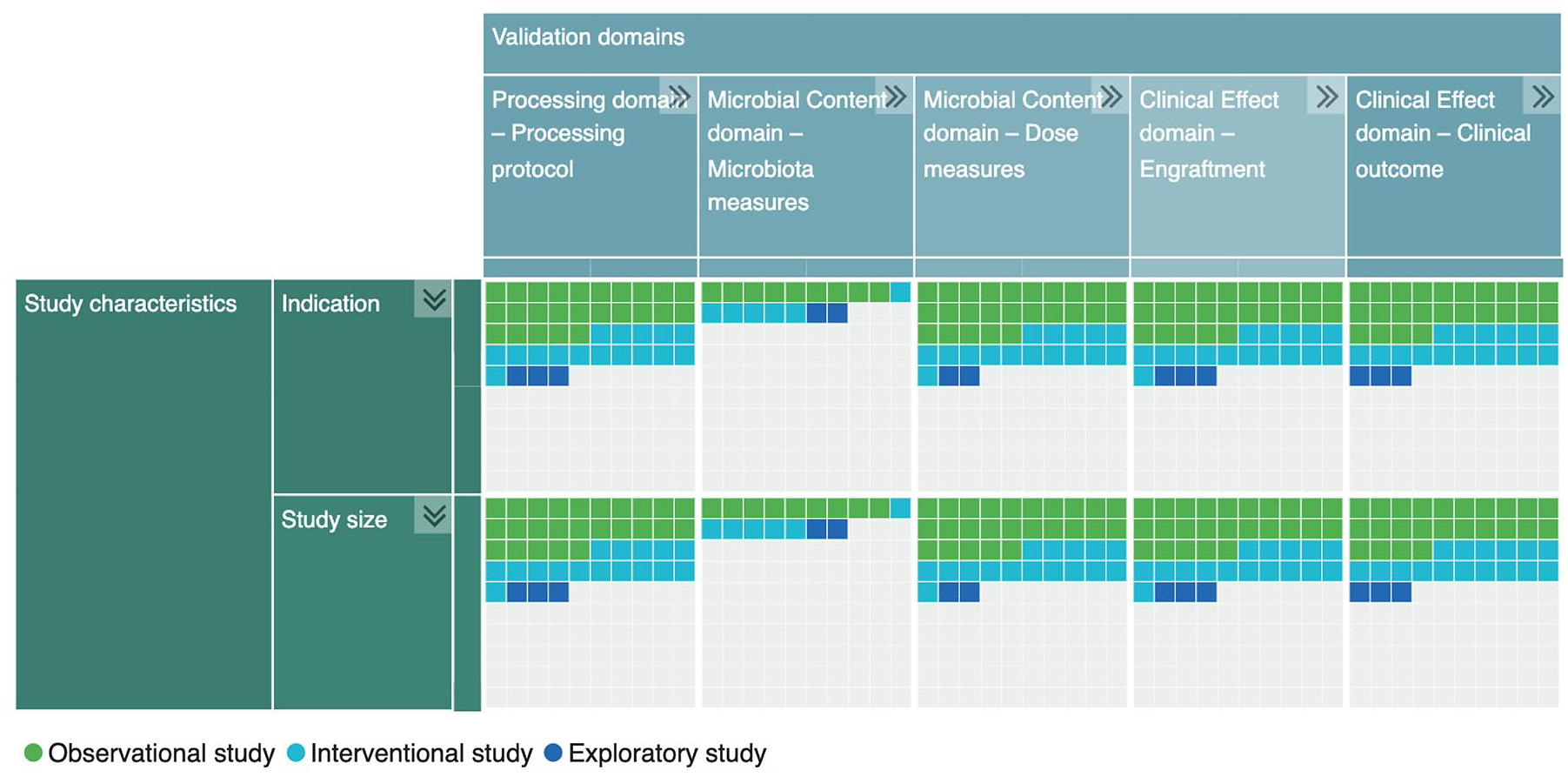
Evidence Gap Map, preview. Follow this link to access the interactive version: https://cefta.au.dk/about-fmt/efmt. Here, study details and quality assessment domains can be folded or unfolded to sort and visualise the present evidence of this review. The map is generated using v.2.3.0 of the EPPI-Mapper 29 software powered by EPPI Reviewer. 28 Observational studies covered prospective, retrospective and comparative cohort studies. Interventional studies covered randomised clinical trials and active comparator studies. Exploratory studies covered feasibility and descending dose studies.
Six studies (14%) used pre-processing and prepared the donations for freezer storage before capsule processing to optimise the processing flow. None of these studies validated the method.
Oxygen-sparing processing methods were applied in five studies (11%) across two sites to protect the anaerobic microbes. One processing site delivered capsules for all three Staley et al. studies41,42,50 in Minneapolis, MN, to treat CDI and used N2 gas during homogenisation. No increased clinical effect was observed compared to similar studies for CDI using oxygen-exposed capsule processing. Another processing site delivered capsules to two studies from Copenhagen, Denmark, treating irritable bowel syndrome 58 and UC. 68 Here, they strove to minimise oxygen exposure by covering the donor stool with oxygen-reduced saline immediately after donation and processed the samples in a headspace flushing with argon gas. The study by Cold et al. 68 used oxygen-sparing processed capsules to treat UC and demonstrated an increased clinical effect treated compared to other UC studies. Still, the study was small and had other substantial processing and dosing variations compared to the other studies on UC.
The protocols behind the commercial preparations with encapsulated microbiota formulations were proprietary due to commercial interests. Very few processing details of these preparations were shared, illustrating a lack of transparency. Information on filtration, centrifugation and glycerol use in processing the commercial product SER-109, now marketed as Vowst® (Seres Therapeutics, Boston, MA, USA), was shared in one study 35 ; yet, without detailed information. The SER-109 product had clinical effects comparable to those obtained with non-commercialised products, except in the study from McGovern et al. 48 who reported a lower effect rate.
None of the included studies described a processing protocol for encapsulated FMT with sufficient detail and accuracy to replicate any capsule processing. Most often, the overall methods, such as filtration and centrifugation, were named without further user instructions. Details such as filtration pore size, centrifugal force and time, preparation registration, traceability, standardisation and quality assessment were missing from the provided information.
Content analysis domain
Microbiota measures
The microbial content was assessed in 17 (39%) of 44 studies by any method suited for validation in the microbiota and dose measures categories. The capsule content was examined for viability in 15 (34%) studies or for quantification of the microbes in 15 (34%) studies (Table 5). The methods used for this were cultivation (n = 6, 14%), flow cytometry (n = 5, 11%) and microscopy (n = , 9%). Cultivation was used for bacterial viability assays and dose quantification by colony-forming units. Flow cytometry and microscopy were used to count microbes as surrogates of dosages and assess viability. In general, more data are needed on the accuracy and validity of the methods used across the studies to make them directly comparable.
Validation covariables were recorded from the 44 included studies.

Donor selection was documented if a description or reference to any donor screening programme was provided. Pre-processing was identified as the preparation of donations for storage in a freezer before a later capsule processing. Preservation required any use of cryo- or lyoprotectants. Bacterial count, viability and engraftment analysis were registered regardless of the method used. Method was registered by technique or marked with ‘Yes’ if the method used was not named. 16S: bacterial identification by 16S ribosomal RNA sequencing; CFUs counted by cultivation on agarose; ITS: fungal identification by nuclear ribosomal ITS region sequencing.
Autologous donation.
Derived from one screened donor.
CFU, colony-forming units; FC, flow cytometry for counting; ITS, internal transcribed spacer; M, microscopy for counting, viability or visualisation; MGS, metagenomic sequencing; qPCR with PMA, quick polymerase chain reaction with propidium monoazide for viability assay; WGS, whole-genome sequencing.
Two studies (5%) analysed the capsule content using liquid chromatography-mass spectrometry to identify metabolites.
Microbial quantification was performed to determine the dose, but no relation between microbial number and clinical outcome was investigated. No studies compared viability with clinical outcomes.
As revealed by the Evidence Gap Map (Figure 3), the microbiota measures category in the Content analysis domain receives substantially less attention than the other categories in the quality assessment model.
Dose measures
Dose measures play a pivotal role in standardising FMT treatments. No consensus on a standardised dose measure was identified, and no general definition of FMT dose was found. Dose comparisons were challenging due to variations in the segregation methods, that is filtration and centrifugation. These variations caused differences in the materials discarded during processing, resulting in varying FMT contents across the studies.
Doses were registered using different measures across the articles (Table 6). The dose was reported as faecal weight (crude or processed, n = 30, 68%), capsule count (n = 37, 84%), microbial count (n = 10, 23%), viability (n = 5, 11%) or spore count (5, 11%).
Comparison of validation methods in each of the three domains, central to FMT and stratified by indication for its use.

Reported as weight before processing (crude faeces).
Reported as weight after processing.
CDI, Clostridioides difficile infection; FMT, faecal microbiota transplantation; ITS, internal transcribed spacer; MGS, metagenomic sequencing; WGS, whole-genome sequencing.
The wet weight of crude donor faeces used for a treatment ranged from 2.3 to 200 g per treatment.6,37 Water content is the primary factor influencing wet weight, but details on the variable stool characteristics, such as the Bristol Stool Scale, were not reported. The final processed weight ready for FMT depends on both crude faecal wet weight and the processing protocol. Most studies used capsule count to quantify the dose, with the total accumulated number of capsules per FMT treatment ranging from 4 to 1250 capsules.50,68
The microbe count used for dose measure ranged from 3.8 × 108 to 1 × 1013 microbes per treatment3,9 or 1 × 1011 to 5 × 1011 bacteria per treatment.31,50 Dose estimated by viability measures ranged from 3.2 × 105 to 3.2 × 1011 CFUs per treatment 52 derived from either spores or bacteria. Spore counts were only utilised to dose the SER-109 product.
Due to the heterogeneity of the dose measures and large variance in reported dosages, there is currently insufficient evidence to document firm associations between concrete dose and clinical effects.
Clinical effect domain
Engraftment
Microbial engraftment was categorised under the Clinical effect domain for clinical outcomes (Figure 2) and was also listed as a covariable. Engraftment was analysed in 33 studies (75%) by comparing donor and recipient microbiomes (Tables 5 and 6). In 26 of the 33 studies, engraftment was analysed by 16S sequencing of bacterial ribosomal RNA to identify bacteria on species and strain levels. Four studies used metagenomic sequencing for engraftment analysis, which provided more detailed information on the microbiome profile with a reference-free detection of bacteria, viruses, fungi, protozoa and archaea. Two studies analysed fungi engraftment using ITS region sequencing. No studies examined viral engraftment.
Microbial engraftment and clinical effect outcomes were not always concordant. Engraftment was measured in all seven negative FMT studies31,56–58,60,61,64 across various indications, raising questions about its role as an equivalent measure to clinical outcomes in evaluating FMT effectiveness.
Clinical outcomes
The studies included in the analysis focused on clinical effect, safety or feasibility as their main clinical outcomes (Table 3). Most studies used clinical effect as the primary outcome, while studies testing new indications for FMT often used safety and feasibility as the primary outcome and effect as the secondary outcome.
Of all indications listed in Table 3, clinical effects are established for two indications, that is CDI and UC. Using FMT for CDI, a consensus has emerged to define the primary outcome as a resolution of C. difficile-associated diarrhoea after 8 weeks. CDI had the best clinical evidence of all indications, with effect measures ranging from 71% to 100% (median 89%). In clinical trials investigating new treatments for UC, the primary outcome is often defined as clinical remission after 8 weeks. Two of four UC studies used this definition as their primary outcome.68,69 The four included UC studies showed disease remission in 21%–71% (median 55%) assessed after 8–13 weeks. No significant effect of FMT was established for obesity in larger randomised studies. One study describes the positive effect of a commercial product on depression and anxiety in a small phase I study. 52 Three small studies on graft versus host disease could indicate a potential effect of FMT. No evidence was found of FMT for other indications listed in Table 3.
All studies reported that encapsulated FMT was a safe and feasible treatment, but safety parameters and their relation to the safety of comparator treatments remain incompletely described.
Discussion
This scoping review identified 44 studies that address encapsulated FMT or faeces processing validation. The studies described different protocols for frozen or lyophilised FMT capsules with multiple differences in methods, highlighting a need for common standardised validation measures. We grouped validation measures into three domains that may be addressed in future studies: Processing, Content analysis and Clinical effect.
Standardisation of FMT has been addressed since its early modern use 10 and continues to be an important focus. The growing demand for FMT is partly driven by increased accessibility, ensured by capsule use due to their ease of use, cost and convenience to patients. This highlights the importance of developing standardised capsule processing protocols. Developing standardised, non-proprietary and operational protocols for capsule processing could accelerate the advancement and dissemination of capsule-based FMT. While efforts have focused on standardisation of donor selection and stool banking to ensure safety and traceability,23,70 the current processing protocols lack standardisation, partly due to a lack of evidence-based validation targets. The findings of this review underscore this issue. Validation of the entire FMT value chain is required to maintain high standards and achieve the best possible clinical outcomes of FMT. A consensus-based and validated dose definition, based on total microbial counts per volume and not merely crude faeces wet weight, would form an important part of such steps towards harmonising FMT.
Diverging definitions of FMT as either a tissue-like substance or a medicinal product complicates the development of international standards for processing, validation and quality control. Also, regulatory policies impact FMT development. 71 In the United States, FMT capsules are manufactured as biological medicinal products according to the Good Manufacturing Practice principles and require an Investigational New Drug application by the U.S. Food and Drug Administration (FDA).72,73 In the European Union, intestinal microbiota is considered a substance of human origin (SoHO), now embedded in the recently adopted SoHO regulation to replace the EU Tissues and Cells Directive by the European Commission. 74 When applied and regulated as a SoHO, FMT must be minimally processed and derived from a single donor. Selective processing, marketing or standardisation through, for example, pooling of faeces from several donors may render the product a faeces-derived medicinal product liable to regulation under the legal framework governing medicinal products for human use in the EU, similar to the FDA regulation. The European Directorate for the Quality of Medicines & HealthCare (EDQM) under the Council of Europe provides technical guidance for the quality and safety of tissues and cells. 75 The EDQM tissue guide now provides an updated and firm basis for handling intestinal microbiota according to the SoHO regulation by standardising the entire process from donor selection to processing, application and traceability. Together with published consensus-based guidelines, 23 this guide provides the best-described standardisation for FMT.
Microbiota measures in the Content analysis domain have received substantially less research attention than the two other domains (Figure 3). This may reflect a still limited understanding of the mechanism of action underlying the effects of FMT, which further complicates the microbial validation and poses challenges for establishing a standardised processing protocol. Due to the inherent heterogeneity of intestinal microbiota, two FMT preparations would never be identical, and striving towards a consistently homogeneous content may be unrealistic. Therefore, the standardisation of encapsulated FMT may focus on defining validated measures of clinically important constituents or properties rather than aiming for consistently uniform components. Maintained bacterial viability is often considered an essential requirement for FMT quality, 76 but no studies have demonstrated a firm association between microbiota viability and clinical effect. Although bacterial cultivation is regarded as the gold standard for assessing bacterial viability, it may not accurately reflect the viability of the FMT end-product. This is because the cultivation of certain species ex vivo varies according to the composition of the bacterial community. Oxygen-sparing processing could potentially increase viability as many intestinal bacteria are obligate anaerobes. Still, for recurrent CDI, the effect of FMT without specific anaerobic precautions is comparable to that of anaerobically processed donations.77,78 This suggests that ex vivo bacterial viability may not be essential for clinical effects or that obligate anaerobes are protected in the faecal medium during aerobic processing. Regardless, evaluating doses based solely on viability measures, as some studies advocate, may not be appropriate until studies have demonstrated an association between viability and clinical outcomes. In addition to viable bacteria, the effectiveness of FMT in treating CDI could also be attributed to the presence of other active constituents, such as metabolites or bacteriophages. 79 Future clinical studies should be designed to investigate all potential active factors in the content of FMT.
Bacterial engraftment was frequently used as a surrogate marker for the FMT effect, anticipating a pivotal role of donor bacteria colonisation for clinical effect. This is contrasted by limited evidence of a firm correlation between engraftment and clinical outcomes. In CDI, complete engraftment of donor bacteria may not necessarily be associated with disease resolution. 80 For other conditions, such as inflammatory bowel disease and irritable bowel syndrome, complete donor engraftment may occur without corresponding clinical benefits, or clinical improvement may occur without concomitant full bacterial engraftment.58,81 A significant limitation of these studies is their reliance on 16S rRNA analysis. Due to restricted identification and limited sequencing depth, 16S RNA analysis is not ideal for assessing the full impact of strain engraftment and its associated changes. 82 Nonetheless, engraftment analysis remains valuable for understanding the influence of FMT on the intestinal microbiota. Advances in untargeted metagenomic sequencing enable a more comprehensive characterisation of the metagenome, which includes microbial communities, including bacterial species, viruses, fungi and parasites, allowing a deeper portrayal of the microbiota and its engraftment. 83 A recent meta-analysis of metagenomes from various FMT studies found the importance of bacterial engraftment for clinical outcomes. 84 Coupled with quantitative analysis, metagenomic analysis shows great promise in elucidating the role of engraftment and identifying potential validation markers. Still, bioinformatic models used to evaluate the metagenome frequently yield inconsistent results, complicating a clear interpretation.85,86
The present study identified discrepancies in the validation methods used, highlighting the complexity of obtaining standardised microbiota preparations for human applications. Documents issued by international expert bodies, such as the EDQM tissue guide, 75 strive to describe uniform standards, but achieving this for FMT remains challenging. This is mainly due to the very limited number of studies comparing methods with clinical efficacy outcomes, which is essential for guiding future development. Lee et al. 87 initially assessed the impact of different processing methods on clinical outcomes, demonstrating no clinical difference between fresh and frozen preparations. To ensure that processing factors do not compromise the treatment effect, more studies comparing processing factors and clinical outcomes are warranted to advance FMT. Standardisation protocols require accessible validation approaches focusing on clinically relevant content measures, which future clinical research must identify. This is important for ensuring high-quality FMT formulations with stable clinical efficiency.
Our study has limitations. Because of data heterogeneity in the included studies, performing a meta-analysis was not possible, and the relations between validation covariables and clinical effects could not be summarised quantitatively. No systematic assessment of study quality was performed, and the results are presented as published. Still, interpretation bias could not be precluded.
Conclusion
This review identifies gaps in the assessment of FMT processing and quality. It provides an essential overview of how FMT capsules may be validated in the future, categorising them into three domains: Processing, Content analysis and Clinical effect. Advancing the validation of processing and content analysis is particularly necessary. Future clinical studies should explore the impact of validation covariables on the clinical effect of FMT.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848251314820 – Supplemental material for Validation methods for encapsulated faecal microbiota transplantation: a scoping review
Supplemental material, sj-pdf-1-tag-10.1177_17562848251314820 for Validation methods for encapsulated faecal microbiota transplantation: a scoping review by Nina Rågård, Simon Mark Dahl Baumwall, Sara Ellegaard Paaske, Mette Mejlby Hansen, Katrine Lundby Høyer, Susan Mikkelsen, Christian Erikstrup, Jens Frederik Dahlerup and Christian Lodberg Hvas in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.