
Abstract
Background:
Alkaline phosphatase (ALP) is a potential cancer biomarker. However, its prognostic value in patients with colorectal liver metastasis remains unclear.
Objectives:
This study aimed to investigate the association between ALP levels and mortality risk in patients with colorectal liver metastases (CRLM), providing insights for enhancing prognostic assessments.
Design:
Retrospective cohort study.
Methods:
This study included 195 patients with CRLM from a single centre in China. ALP level was the primary exposure variable, with demographic, clinical and pathological factors serving as covariates. Multivariate Cox regression analyses were used to evaluate the impact of ALP on mortality over a 4-year follow-up period. Covariates included the number of liver metastases, T stage, N stage, chemotherapy, tumour location, primary surgery, topical treatment, apolipoprotein A1, targeted therapy, tumour type, CA-199 levels, metastatic surgery, sex, Karnofsky Performance Status and age.
Results:
Of 195 enrolled patients, 134 (68.72%) were male, and 61 (31.28%) were female, with ages ranging from January 2008 to December 2019. A total of 147 patients (76.96%) were diagnosed with left hemicolon cancer and 44 (23.04%) with right hemicolon cancer. After adjusting for the covariates, elevated ALP levels were significantly associated with an increased risk of mortality (hazard ratio = 1.24, 95% confidence interval: 1.08–1.43, p = 0.0029). Sensitivity analyses confirmed the robustness of these findings, reinforcing the association across different analytical approaches.
Conclusion:
ALP level is a valuable prognostic indicator in patients with CRLM. Integrating ALP measurement into clinical practice may enhance risk stratification and patient management. Future research should explore the role of ALP in broader populations and explore its implications for treatment strategies.
Introduction
Colorectal cancer (CRC) is the third most common malignancy worldwide, with liver metastasis being the leading cause of mortality. 1 In 2020, approximately 1.9 million new CRC cases and 935,000 deaths were reported globally. 2 In China, the incidence and mortality rates are notably high, with approximately 555,000 new cases and 286,000 deaths in the same year. 3 Liver metastasis occurs in 20%–34% of patients at initial diagnosis, while 50%–60% develop metastases during disease progression. 4 The presence of liver metastases significantly reduces survival rates, with the 5-year survival rate for patients with unresectable disease being less than 5%. 5
Alkaline phosphatase (ALP), a hydrolase enzyme primarily produced by the liver, bones and placenta, is widely distributed in human tissues.6,7 Recent studies highlighted the potential use of ALP as a biomarker for various conditions. Its predictive value extends to non-malignant diseases such as cerebral haemorrhage, orthopaedic disorders and surgical complications.8–10 Notably, elevated ALP levels are correlated with poor prognosis in several malignancies, including lung, liver, prostate and penile cancers,11–14 making ALP an increasingly important tool in cancer prognostication.15–17 Research has also revealed a significant relationship between ALP and carcinoembryonic antigen, which influences the prognosis of liver metastases from CRC. Elevated ALP levels in cases of liver metastasis can signify liver damage caused by invasive tumour cells. 18 Previous single-centre retrospective studies have suggested that serum ALP levels are an independent predictor of overall survival in patients with stage I–IV CRC, excluding those with elevated ALP levels due to liver and kidney diseases. 19 This research gap highlights the need to further investigate the role of ALP in prognostic assessments of patients with CRC and liver metastasis, which may provide a more valuable basis for clinical practice.
Therefore, we conducted a retrospective cohort study to evaluate the association between ALP levels and mortality risk in Chinese patients with colorectal liver metastases (CRLM). Our study included 195 patients and considered multiple covariates to provide comprehensive and representative data for the Chinese population. These findings are expected to offer valuable insights for improving the prognostic assessment and personalised treatment strategies for patients with CRLM. The unique aspect of our study design lies in its comprehensive consideration of various clinical and biochemical indicators, aiming to more accurately assess the independent role of ALP in prognostic prediction.
Materials and methods
Participants
This retrospective cohort study was conducted at the First Affiliated Hospital of Guangzhou University of Chinese Medicine between January 2008 and December 2019, with follow-up until December 31, 2021. A total of 195 Chinese patients with CRLM were included. Inclusion criteria were as follows: (1) age ⩾18 years; (2) histologically confirmed CRC with liver metastases and no other distant metastases and (3) radiological evidence of liver metastases on contrast-enhanced computed tomography or magnetic resonance imaging. The exclusion criteria included the following: (1) evidence of other malignancies or severe non-malignant diseases; (2) survival of less than 6 months; (3) Karnofsky Performance Status (KPS) score <50 and (4) incomplete follow-up data. The index date was defined as the date of the initial diagnosis of liver-limited metastatic CRC. Data were independently extracted from the hospital’s electronic medical records system by two trained researchers and verified by a third researcher to ensure accuracy. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 20
Sources of selection of participants
The enrolled patients were guided according to the 2019 NCCN guidelines for clinical treatment decisions. During the study period, immunotherapy was not routinely recommended according to the NCCN guidelines for CRC treatment. Although a small number of patients may have received immunotherapy through clinical trials or off-label use, immunotherapy was not included as a variable in our analysis due to its limited application in this cohort.
We collected data on all treatment methods used for the enrolled patients, including whether the patient received primary surgery, targeted therapy, radiotherapy, local therapy for liver metastases or chemotherapy. The chemotherapy and targeted therapy regimens used included the following: oxaliplatin + leucovorin + fluorouracil (FOLFOX), oxaliplatin + capecitabine (CAPEOX), irinotecan + leucovorin + fluorouracil (FOLFIRI), irinotecan + leucovorin + fluorouracil + oxaliplatin (FOLFOXIRI), capecitabine, tegafur + gimeracil + oteracil (TS-1), oxaliplatin, bevacizumab and cetuximab. All treatment methods were recorded as binary variables for statistical analysis. Clinical doses were adjusted according to side effects, such as bone marrow suppression.
Follow-up methods
Since January 2020, we have regularly followed up on the survival time of enrolled patients. Data were acquired via the hospital’s electronic medical record system or telephone follow-ups 6-monthly. When the specific date of death could not be retrieved, the midpoint of the month in which the patient died was used. Survival time was calculated daily. Assessors were blinded to patient information to reduce assessment bias. All data were updated on December 31, 2021.
Variables
The exposure variable was ALP, measured using a Cobas 8000 automated biochemical analyser (Roche Diagnostics, Basel, Switzerland). Five millilitres of fasting venous blood was collected from all patients within 48 h of admission and placed in K2-EDTA anticoagulant tubes for testing. ALP levels were recorded as continuous variables in the database and later categorised based on clinical significance. The primary outcome was all-cause mortality, determined using hospital follow-up records and telephone interviews. Death events were recorded as binary variables (yes/no) in the database, along with the specific date of death. Two independent researchers were blinded to the ALP levels of the patients. Covariates included the number of liver metastases, lymph node metastasis, chemotherapy, primary tumour characteristics, tumour location, primary tumour surgery, local treatment, apolipoprotein A1 (Apoa-1)-targeted therapy, liver metastasis type, carbohydrate antigen 199, metastasectomy, sex, KPS score and age. These variables were selected based on previous literature and clinical expert opinions to control for potential confounding factors. All variables were obtained using standardised clinical assessments and laboratory tests. Missing data (<5%) were handled using multiple imputations to reduce bias and maintain the statistical power.
Measurement of ALP
Patients with CRLM were screened through routine blood tests, including the measurement of ALP levels, before starting drug therapy and at each treatment stage. However, only pre-therapy data were recorded in this study.
Statistical analysis
ALP levels were categorised into tertiles based on their distribution in the study population: low (⩽75 U/L, n = 63), middle (76–120 U/L, n = 67) and high (>120 U/L, n = 65). These cut-off values were determined based on the statistical distribution of our data and previous literature on liver function parameters. Tertile categorisation was used to ensure adequate sample sizes in each group while maintaining clinical relevance.
Continuous variables are presented as mean ± standard deviation for normally distributed data or as median (minimum and maximum) for skewed distributions. Categorical variables are expressed as frequencies or percentages. Differences between groups were assessed using the Chi-square test for categorical variables, the Student’s t-test for normally distributed continuous variables or the Mann–Whitney U test for non-normally distributed continuous variables. The association between ALP levels and mortality was analysed using the univariate and multivariate linear regression models. Three models were constructed: Model 1, with no covariate adjustment; Model 2, adjusted for sociodemographic data and Model 3, adjusted for Model 2 covariates and additional variables, as shown in Table 1. These models aimed to explore the trend of the effect of ALP under different adjustment strategies and assess the robustness of the results.
Characteristics of the study population by ALP tertiles.
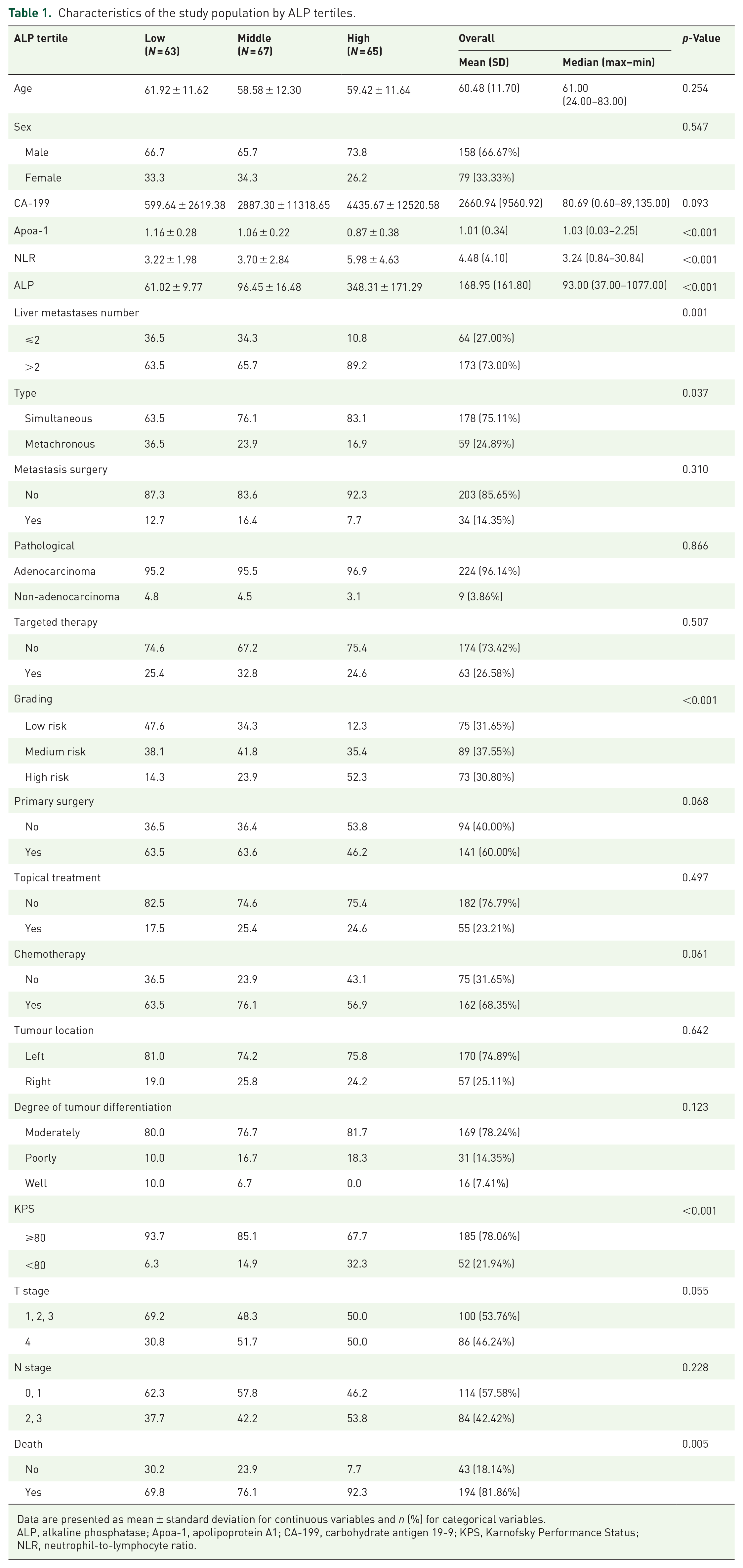
Data are presented as mean ± standard deviation for continuous variables and n (%) for categorical variables.
ALP, alkaline phosphatase; Apoa-1, apolipoprotein A1; CA-199, carbohydrate antigen 19-9; KPS, Karnofsky Performance Status; NLR, neutrophil-to-lymphocyte ratio.
To address the potential nonlinearity between ALP and mortality, we used a generalised additive model (GAM) and smooth curve fitting using the penalised spline method. If nonlinearity was detected, the inflexion point was calculated using a recursive algorithm and a two-piecewise linear model was constructed on both sides of the inflexion point. Sensitivity analysis compared the standard linear regression model with the two-piecewise model using the log-likelihood ratio test to determine the most appropriate model for explaining the true association between ALP and mortality.
Subgroup analyses were performed using stratified linear regression models or GAMs. Continuous stratification variables were first converted into categorical variables according to clinical cut-off points or tertiles before interaction tests. Effect modification for subgroup indicators was assessed using the likelihood ratio test.
To further ensure the robustness of our analysis, we performed a sensitivity analysis by converting ALP into a categorical variable and calculating the P for the trend. This aimed to verify the results of ALP as a continuous variable and assess potential nonlinearity. All analyses were performed using R statistical software (version 3.4.3; http://www.R-project.org, The R Foundation, Vienna, Austria). Statistical significance was set at 0.05.
Results
In this study (Figure 1), 195 patients with CRLM were stratified into low, middle and high groups based on their ALP levels. The overall mean age was 60.48 years (standard deviation: 11.70 years), with a median age of 61 years (range: 24–83 years). For the CA-199 biomarker, the mean was 2660.94 U/mL (standard deviation: 9560.92 U/mL), with a median value of 80.69 U/mL (range: 0.60–89135.00 U/mL). The mean ApoaL1 level was 1.01 g/L (standard deviation: 0.34 g/L), and the median was 1.03 g/L (range: 0.03–2.25 g/L). The mean neutrophil-to-lymphocyte ratio (NLR) was 4.48 (standard deviation: 4.10), with a median value of 3.24 (range: 0.84–30.84). The mean ALP level was 168.95 U/L (standard deviation: 161.80 U/L), with a median of 93.00 U/L (range: 37.00–1077.00 U/L).

Flow chart of patient selection and analysis process.
The results showed that patients in the high ALP group had more unfavourable clinical characteristics and prognoses (Table 1). Higher ALP levels were significantly associated with a decrease in ApoaL1 level (p < 0.001) and an increase in NLR (p < 0.001). The high ALP group had a significantly higher proportion of patients with more than two liver metastases (89.2%) and simultaneous metastases (83.1%) compared to the other groups (p = 0.001 and p = 0.037, respectively). Furthermore, the high ALP group was characterised by a greater percentage of high-risk classifications (52.3%, p < 0.001), lower KPS scores (32.3% with KPS < 80, p < 0.001) and higher mortality rates (92.3%, p = 0.005). No significant differences among the three groups in terms of treatment modalities or other tumour characteristics were observed. These findings suggest that ALP levels may serve as crucial prognostic indicators in patients with CRLM.
Univariate analysis revealed several factors significantly associated with the mortality risk in patients with liver metastases from CRC (Table 2). Among biochemical indicators, a 100-unit increase in ALP was associated with a 13% increase in mortality risk (risk ratio (RR) = 1.13, 95% confidence interval (CI): 1.04–1.22, p = 0.0023). Conversely, each unit increase in ApoaL1 corresponded to a 43% decrease in mortality risk (RR = 0.57, 95% CI: 0.37–0.88, p = 0.0115). Regarding disease characteristics, higher mortality risks were associated with more than two liver metastases (RR = 2.12, 95% CI: 1.51–2.98, p < 0.0001), right-sided colon tumours (RR = 1.55, 95% CI: 1.12–2.15, p = 0.0081), T4 stage (RR = 1.58, 95% CI: 1.14–2.17, p = 0.0055) and N2–3 stage (RR = 1.61, 95% CI: 1.18–2.20, p = 0.0028). By contrast, metachronous metastases had a lower risk than synchronous metastases (RR = 0.52, 95% CI: 0.37–0.73, p = 0.0002). Treatment modalities significantly influenced prognosis, with metastasis surgery (RR = 0.52, 95% CI: 0.34–0.80, p = 0.0028), primary tumour surgery (RR = 0.43, 95% CI: 0.32–0.57, p < 0.0001), chemotherapy (RR = 0.54, 95% CI: 0.40–0.73, p < 0.0001) and local treatment (RR = 0.68, 95% CI: 0.49–0.95, p = 0.0236) all demonstrating protective effects. Additionally, patients with KPS < 80 had a 60% higher mortality risk compared to those with KPS ⩾80 (RR = 1.60, 95% CI: 1.15–2.23, p = 0.0053). These findings underscore the importance of early diagnosis and aggressive treatment, as well as the potential value of specific biochemical indicators and disease characteristics in the prognostic assessment of patients with CRLM.
Univariate analysis of death.

Table 2 presents the univariate analysis results of various factors in relation to the risk of mortality, including relative risk (with 95% CIs), and p-values. A risk ratio greater than 1 indicates a higher risk of mortality relative to the reference group, while a risk ratio less than 1 indicates a reduced risk. Results with p-values less than 0.05 are considered statistically significant.
ALP, alkaline phosphatase; Apoa-1, apolipoprotein A1; CA199, carbohydrate antigen 19-9; CI, confidence interval; KPS, Karnofsky Performance Status; NLR, neutrophil-to-lymphocyte ratio.
The Cox proportional hazards model analysis revealed a significant association between ALP levels and mortality risk in patients with CRLM (Table 3). In the unadjusted model, each 100-unit increase in ALP was associated with a 13% increase in mortality risk (hazard ratio (HR) = 1.13, 95% CI: 1.04–1.22, p = 0.0023). After adjusting for sex, age and KPS, the association remained significant (HR = 1.11, 95% CI: 1.02–1.21, p = 0.0209). In the fully adjusted model, which accounted for multiple additional clinical factors, the association strengthened with each 100-unit increase in ALP was associated with a 24% increase in mortality risk (HR = 1.24, 95% CI: 1.08–1.43, p = 0.0029). Across all models, the p-value was <0.05, demonstrating the statistical significance of this association. These results highlight the potential importance of ALP in predicting the prognosis for patients with CRLM while also emphasising the need to consider the broader clinical context when evaluating the association between ALP and mortality risk.
Association between ALP and mortality risk in patients with colorectal liver metastases.

Outcome: Death. Exposure: per 100 changes of ALP. Non-adjusted model adjusts for: None. Adjust I model adjusts for: sex, age and KPS. Adjust II model adjusts for: Liver metastases number, T stage, N stage, chemotherapy, tumour location, primary surgery, topical treatment, Apoa-1, targeted therapy, Type, CA-199, metastasis surgery, sex, KPS, age. Cox proportional hazard models were used with overall survival as the time variable. Data analysis was performed using R software (version 3.4.3) on August 18, 2024.
ALP, alkaline phosphatase; Apoa-1, apolipoprotein A1; CA199, carbohydrate antigen 19-9; CI, confidence interval; HR, hazard ratio; KPS, Karnofsky Performance Status.
In this retrospective cohort study of Chinese patients with CRC with liver metastases, we conducted subgroup analyses to evaluate the association between ALP levels and mortality risk across various clinical characteristics (Figure 2). Our findings revealed significant variations in this association among different subgroups: patients with moderately differentiated tumours showed an HR of 1.12 (95% CI: 1.03–1.22), while those with poorly differentiated tumours had an HR of 1.34 (95% CI: 0.99–1.81). The association was more pronounced in patients classified as low risk (HR = 1.47, 95% CI: 1.03–2.10). The relationship between ALP and mortality was most significant in patients with NLR < 3.24 (HR = 1.49, 95% CI: 1.22–1.83). Treatment modalities also influenced this association, with higher risks observed in patients receiving local treatment (HR = 1.39, 95% CI: 1.13–1.70), chemotherapy (HR = 1.21, 95% CI: 1.06–1.38) and primary tumour surgery (HR = 1.26, 95% CI: 1.10–1.45). The association was more evident in the N0–1 stage (HR = 1.35, 95% CI: 1.16–1.56) and patients with the T1–3 stage (HR = 1.34, 95% CI: 1.15–1.55). Additionally, patients with adenocarcinoma (HR = 1.14, 95% CI: 1.05–1.23), male patients (HR = 1.16, 95% CI: 1.06–1.26) and those with more than two liver metastases (HR = 1.09, 95% CI: 1.01–1.19) demonstrated higher risks. These findings provide valuable insights for identifying high-risk patients and optimising individualised treatment strategies. However, given the retrospective nature of this study, prospective investigations are necessary to validate these results and explore potential interactions between ALP and other prognostic factors.

Forest plot of subgroup analyses.
To verify the robustness of our findings, we conducted sensitivity analyses using ALP as a categorical variable (see Supplemental Appendix). The results demonstrated that patients with high ALP levels had significantly higher mortality risk compared to those with low ALP levels. In the unadjusted model, the high ALP group showed twice the risk of death compared to the low ALP group (HR = 2.00, 95% CI: 1.45–2.77, p < 0.0001). This association remained significant after adjusting for demographic characteristics (sex, age and KPS score) (HR = 2.07, 95% CI: 1.47–2.92, p < 0.0001). In the fully adjusted model, which accounted for clinical factors including liver metastases number, lymph node status, chemotherapy and tumour characteristics, the significant association between high ALP levels and mortality risk persisted (HR = 1.68, 95% CI: 1.10–2.59, p = 0.0174). These findings further confirmed the independent association between ALP levels and prognosis in patients with CRLM.
Discussion
This study explored the association between ALP levels and the mortality risk in Chinese patients with CRLM. We conducted a retrospective cohort study involving 195 consecutive patients over a 4-year follow-up period, providing a reliable foundation for our findings with a moderate sample size and extended follow-up duration. The results revealed a significant positive correlation between ALP levels and mortality risk. After comprehensive adjustment for potential confounding factors, we found that for every 100 U/L increase in ALP, the risk of death increased by 24%. This finding underscores the potential importance of ALP as a prognostic biomarker in patients with CRLM.
The prognostic significance of ALP in malignancies with liver metastases has been well documented in recent studies. A comprehensive review by Jiang et al. 18 emphasised that elevated ALP levels are both diagnostic and prognostic indicators, particularly in patients with liver metastases. This prognostic role has been extended to various metastatic cancers. In patients with metastatic pancreatic cancer receiving nab-paclitaxel plus gemcitabine treatment, ALP levels above 260 U/L showed a significant association with poor survival outcomes, especially in patients with liver metastases. 21 Similarly, in patients with advanced HER2-negative gastric cancer undergoing immunotherapy, ALP levels exceeding 225 U/L predicted shorter progression-free survival. 22
Our findings align closely with those of Hung et al., 19 who conducted a retrospective cohort study on patients with stage I–IV CRC. Their research revealed a diminished 5-year overall survival rate in patients with ALP ⩾93 U/L. Although their study encompassed a broader patient population, our study specifically focused on 195 patients with CRLM, providing more targeted insights into this subgroup. Our methodological approach differed by treating ALP as a continuous variable, potentially offering a more nuanced risk assessment framework. While both studies employed multivariate Cox regression analyses, our inclusion of liver metastasis-specific factors provided a more comprehensive prognostic evaluation. Despite these methodological variations, both studies consistently underscored the potential value of ALP as a prognostic marker in CRC, supporting its integration into clinical decision-making and underscoring the need for further investigation into its prognostic role across various patient subgroups, particularly those with liver metastases.
The association between ALP and the prognosis of patients with CRC and liver metastases is complex. As an important indicator of liver function, elevated ALP levels are typically associated with liver cell injury and bile stasis. 23 In patients with liver metastasis, metastasis-induced liver cell damage and bile stasis can lead to increased ALP levels. 24 ALP may also directly participate in tumour growth and invasion. 25 In colon cancer cell lines, inhibition of ALP activity results in decreased cell proliferation, colony formation and expression of tumour suppressor genes.26,27 ALP may also suppress the function of the immune system, thereby weakening its ability to clear tumours. This suggests that changes in ALP levels may affect the efficacy of chemotherapeutic drugs, as the action of these drugs partially depends on the function of the immune system.28,29 Furthermore, elevated ALP levels may reflect the inflammatory state of the liver, 30 and chronic inflammation is an important factor that promotes tumour progression. 31 ALP is primarily produced in the liver and bones, and malnutrition can affect bone health and liver function. Therefore, changes in the ALP levels may indicate a patient’s overall nutritional status. Malnutrition is an important factor affecting cancer prognosis; therefore, there is a connection between ALP and tumour prognosis. 32 These mechanisms may interact with each other and collectively influence the prognosis of patients with CRC with liver metastases.
This study had several strengths. First, we employed a retrospective cohort design that included 195 Chinese patients with CRLM, providing valuable clinical data for this specific population. Second, we collected data on a wide range of clinical and biochemical indicators, including tumour characteristics, treatment regimens and functional status, allowing us to comprehensively control for potential confounding factors. We utilised multivariate regression models to thoroughly investigate the relationship between ALP and mortality risk. Furthermore, subgroup and sensitivity analyses were conducted to validate the robustness of the results. Notably, we analysed ALP as a continuous variable, potentially providing a more precise risk estimation than dichotomous methods. Finally, our study fills a significant knowledge gap regarding the relationship between ALP and the prognosis of CRLM in the Chinese population, making a unique contribution to this field of research.
However, this study had some limitations. We excluded patients with survival of less than 6 months and KPS scores below 50, meaning our findings may not apply to patients with an extremely poor prognosis or severely impaired physical status. As this was a single-centre study conducted in a tertiary hospital, our patient population may not fully represent broader clinical settings. The referral patterns specific to our institution may have led to a selection bias towards more complex cases. Additionally, the clinical practices, treatment protocols and available resources at our centre may differ from those of other institutions, potentially affecting patient management decisions. Furthermore, as a retrospective study, information bias may have occurred, with some potentially important confounders not being captured. Changes in diagnostic and treatment approaches over the study period (2008–2019) may have also influenced outcomes. Moreover, since our study primarily focused on the Chinese population, caution is necessary when extrapolating the results to other ethnicities. Being an observational study, we could only establish an association between ALP levels and mortality risk rather than prove causality. Despite adjusting for multiple known confounders, unmeasured confounding factors may have influenced the results. Future research should involve multicentre studies across different regions and healthcare settings, prospective trials with standardised data collection protocols, including more diverse patient populations, and account for institutional variations in treatment approaches to address these limitations and strengthen the validity of our findings. These efforts will help validate and expand upon our findings, highlighting the need for cautious interpretation while pointing towards directions for further research.
Conclusion
The findings of this study have significant implications for the clinical management of patients with CRLM. By demonstrating a strong association between ALP level and mortality risk, we provide clinicians with a simple, cost-effective and readily available tool for prognostic assessment. Based on our findings, we propose several practical clinical applications. Elevated ALP levels should prompt more intensive monitoring and potentially more aggressive treatment approaches, particularly for patients with multiple liver metastases. This biomarker can help identify high-risk patients who may benefit from early palliative care consultations and advanced care planning discussions. Regular monitoring of ALP levels can serve as a valuable tool for evaluating treatment responses and guiding the timing of surgical interventions. Furthermore, ALP levels could facilitate more informed discussions about prognosis with patients and their families, helping guide decisions regarding the frequency of follow-up visits and surveillance imaging. From a resource allocation perspective, patients with elevated ALP levels may require more frequent monitoring and earlier referral to supportive care services. Incorporating ALP monitoring into existing prognostic scoring systems can enhance risk stratification and treatment planning. Based on these findings, we recommend that ALP levels be included in the routine assessment of patients with CRLM and considered for integration into existing prognostic scoring systems. However, prospective studies are needed to validate the efficacy of ALP as a prognostic marker and to explore its potential role in guiding treatment decisions. Future research should focus on developing standardised ALP-based risk assessment tools, investigating the optimal timing and frequency of ALP monitoring, evaluating the cost-effectiveness of ALP-guided treatment strategies and examining the impact of ALP-based clinical decision-making on patient outcomes.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241311114 – Supplemental material for Association between alkaline phosphatase levels and mortality in Chinese patients with colorectal cancer with liver metastases: a retrospective cohort study
Supplemental material, sj-docx-1-tag-10.1177_17562848241311114 for Association between alkaline phosphatase levels and mortality in Chinese patients with colorectal cancer with liver metastases: a retrospective cohort study by ZhaoXi Liu, ZiQing Zhang, GuoFang Yu, MingJiang Mo, ChuanYu Xie, DangHan Xu, JieTao Lin, YuChen Zhang, Li Deng, YiChang Luo, YingFeng Huang and Cui Shao in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.