
Abstract
Background:
Limited research exists on colorectal cancer (CRC) patients with bladder invasion, with survival outcomes post-cystectomy underexplored and a debate between partial and total cystectomy ongoing.
Objective:
The study aimed to evaluate the effect of pathological bladder invasion on the long-term tumour prognosis of patients with clinically diagnosed bladder invasion in CRC after cystectomy.
Design:
Retrospective, cohort study.
Methods:
Our study involving 105 CRC patients with bladder invasion who had partial or total cystectomy from 2012 to 2020 collected surgical and pathological data. Groups were divided by pathological bladder invasion presence and compared for 3-year overall survival (OS) and recurrence-free survival (RFS) rates. Multiphoton imaging assessed collagen features in some samples.
Results:
Pathological bladder invasion was confirmed in 50 patients (48%). Of 94 who had partial cystectomy, 41 were in the bladder invasion (+) group. The 3-year OS and RFS rates were 62.97% and 57.35% for the bladder invasion (+) group, and 77.16% and 58.68% for the bladder invasion (−) group, with no significant differences in recurrence rates between groups (p > 0.05). There are also no significant differences in 3-year local recurrence and intravesical recurrence rates between the two groups (18.62% vs 25.83%, 7.73% vs 11.82%, p > 0.05). Distant metastasis was identified as an independent risk factor for OS and RFS by univariate and multivariate Cox regression analyses. Of the 24 samples that underwent multi-photon imaging, 142 collagen features extracted did not show statistical differences.
Conclusion:
Pathological bladder invasion impacts CRC patients’ post-cystectomy survival may be less than what clinical practice implies. Partial cystectomy in cases with pathological bladder invasion might offer similar survival rates to total cystectomy.
Trial registration:
ChiCTR2300077861.
Introduction
Colorectal cancer (CRC) is the third most prevalent cancer globally, 1 accounting for more than 1.8 million new cases and causing nearly 900,000 deaths annually. 2 In primary CRC, 5%–20% of cases show adjacent organ involvement, with the urinary system being affected in 10%–30% of these cases.3,4 The sigmoid colon and rectum are the most common primary tumour sites for bladder invasion. 4
Currently, comprehensive management of CRC with bladder invasion continues to revolve around surgical intervention. En bloc resection, aiming to eliminate residual cancer, is the gold standard for locally advanced CRC with bladder invasion.5,6 Fifteen studies involving patients with CRC with bladder invasion have yielded unfavourable outcomes: the 3-year overall survival (OS) rate ranged from 82% to 91%, the 5-year OS rate from 39% to 75% and the 5-year local recurrence (LR) rate from 11% to 37%.4,7–20 Nevertheless, the surgical method of bladder resection is a subject of ongoing debate in the management of CRC with bladder invasion. Due to the challenge of distinguishing whether the tumour is solely adhered to the bladder or actively invading it during the preoperative examination and intraoperative procedures, surgeons in the past have frequently opted for total cystectomy with urinary diversion. This strategy aimed to secure negative surgical margins and prevent bladder recurrence. Moreover, total cystectomy with urine diversion was frequently employed to secure a negative surgical margin and prevent bladder recurrence.15,16 However, the rate of concurrence between clinical and pathological infiltration in cases of bladder invasion was only approximately 40%–50%,4,7–11,13–19 and nearly half of patients can avoid surgical risks and complications associated with total cystectomy.
Although studies have reported an approximate LR rate of 10%–30% after cystectomy in CRC patients with bladder invasion, no significant difference in LR rates between total cystectomy and partial cystectomy has been documented.7–10 Considering the increased complication rates linked to total cystectomy and the absence of proven significant disparity in recurrence rates between the two types of cystectomy, the necessity of total cystectomy warrants further investigation. Resection of primary colon tumours combined with cystectomy followed by adjuvant systemic chemotherapy remains the current gold standard of care.3,7 Tsang and Lau 8 suggest that selecting between partial and total cystectomy involves balancing margin clearance, LR risk and patient’s quality of life. Total cystectomy is the standard procedure for muscle-invasive bladder cancer. 21 However, for CRC patients with bladder invasion, partial cystectomy may be incorporated into a comprehensive resection strategy. Partial cystectomy can safeguard urinary function, mitigate the surgical risks associated with urine diversion and decrease the occurrence of postoperative complications.7,9,10
The contrast between total cystectomy and partial cystectomy stems from the inherent risk of bladder recurrence associated with partial cystectomy.7–10 Indeed, intravesical recurrence rates have been utilized to assess the oncological efficacy of partial cystectomy for locally advanced CRC. In 2013, Lou et al. 17 demonstrated that pathological invasion of the bladder is an independent predictor of intravesical recurrence and distant metastasis after partial cystectomy. Nonetheless, the postoperative status and survival outcomes of partial cystectomy versus total cystectomy for CRC patients with bladder invasion remain uncertain, with limited studies addressing this topic. With the increasing desire of patients to preserve bladder function, it is necessary to explore the feasibility of partial cystectomy. This study focused on evaluating the effect of pathological bladder invasion on the long-term prognosis of CRC patients with clinically diagnosed bladder invasion after cystectomy, and further exploring the feasibility of partial cystectomy in cases with pathological bladder invasion.
Methods
Patient selection
We conducted a retrospective analysis of patients aged between 18 and 80 years who were clinically diagnosed with primary or recurrent CRC involving bladder invasion between December 2012 and April 2020 at our institute. Exclusion criteria were as follows: non-adenocarcinoma patients, other malignancies and no cystectomy. The clinical diagnosis of bladder invasion is defined by the preoperative imaging or intraoperative findings of tumour invasion into the bladder, while the definition of pathological bladder invasion is the confirmation of cancer cells in the bladder tissue after cystectomy under the microscope, and it is considered to be of CRC origin.
Management
The pathological staging of the tumour was performed in accordance with the eighth edition of the American Joint Committee on Cancer Staging Manual. 22 The diagnosis of all CRC patients is based on imaging studies, colonoscopy and pathological reports from biopsy specimens obtained during colonoscopy. Preoperative chemotherapy is tailored to the patient’s tumour location, size, bladder preservation wishes and metastatic status, all involving preoperative chemotherapy, with a minority of patients also getting radiotherapy or targeted treatments simultaneously. The main regimens for preoperative chemotherapy were FOLFOX or FOLFIRI. The Clavien–Dindo classification is utilized for grading the severity of postoperative complications. 23 Our study categorized patients into two groups based on the presence or absence of pathological bladder infiltration: the bladder invasion (+) group and the bladder invasion (−) group. Total cystectomy is indicated for tumour invading the trigone or dome of the bladder, difficulty in separating the tumour from the bladder, a small residual bladder capacity after resection or when partial cystectomy is not feasible. Partial cystectomy involves full-thickness and partial-thickness bladder wall resections, based on the tumour’s depth of invasion during surgery. Follow-up was performed according to our centre’s preference: for the initial 2 years, a physical examination every 3 months and a computed tomography (CT) scan every 6 months are recommended, followed by an annual procedure for the subsequent 5 years. OS was defined as the time from the discovery of CRC to death from any cause. Recurrence-free survival (RFS) was defined as the time interval between initial treatment and tumour recurrence. LR was defined as recurrence near the primary site of resection, and intravesical recurrence was defined as recurrence within or on the external surface of the bladder after partial cystectomy. The sites of bladder infiltration were divided according to the CT report into the parietal wall, the basal wall and the posterior wall. The primary outcome measure is OS, and the secondary outcome measures include RFS, LR and intravesical recurrence rate. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 24
Data collection
Evaluated parameters included age, sex, tumour location, presence or absence of pathological bladder infiltration, primary surgical method, partial versus total cystectomy, site of tumour invasion, estimated blood loss, surgery duration, length of stay, histological type, lymph node metastasis, distant metastasis and neoadjuvant and adjuvant therapy. Tumour invasion extent (T), regional lymph node metastasis (N) and tumour stage were evaluated following the TNM stage guidelines for CRC from the AJCC (8th edition).
Multiphoton image acquisition and collagen structural feature extraction
Researches have demonstrated that changes in the collagen composition of the tumour microenvironment are linked to the dissemination of cancer and overall prognostic outcomes.25–27 To further investigate the reasons for bladder recurrence in CRC patients with bladder invasion, we utilized multiphoton imaging to observe the collagen characteristics of the tumour microenvironment. The extraction of collagen features was performed automatically via Zeiss LSM 880 with Airyscan (Zeiss, Jena, Germany). 28 Collagen structural feature extraction was then performed using MATLAB software, version 2018B (MathWorks, Natick, MA, USA), from second harmonic generation (SHG) images. 29 Four types of collagen features were extracted in this study, including morphological features, histogram-based features, Gray Level Co-occurrence Matrix (GLCM)-based features and Gabor wavelet transform features. For morphological features, the SHG image was first segmented into collagen pixels and background pixels using the Gaussian mixture model method. 30 The collagen mask image was processed with a fibre network algorithm to trace fibres and identify cross-link points, quantifying collagen alignment using Fourier transform spectra.31,32 We used a histogram approach to extract features including mean, variation, skewness, kurtosis, energy and entropy from SHG pixel intensities and added 80 GLCM-based texture features. The contrast, correlation, energy and homogeneity were calculated from the GLCM with five different displacements of pixels at 1, 2, 3, 4 and 5 and four different directions at 0, 45, 90 and 135 degrees. In addition, 48 Gabor wavelet transform features were included for analysis. Finally, we computed Gabor wavelet features by convolving the SHG image with filters across four scales and six orientations, assessing mean and variation. These parameters informed the collagen feature extraction from multiphoton images.
Statistical analysis
Qualitative variables are presented as numbers (%) and were compared between groups using Pearson Chi-square tests or Fisher’s exact tests. Quantitative variables are reported as the mean ± standard deviation. Survival analysis employed the Kaplan–Meier method, and survival curves were compared using the log-rank test. Potential prognostic factors were evaluated via Cox proportional hazard regression models. Survival time was defined as the interval between intervention and event occurrence or last follow-up. Patients without events and alive at the study’s conclusion were reviewed. Factors with a p value < 0.15 in univariate analysis were included in multivariate models. Risk ratios are reported with 95% confidence intervals. All tests were two-sided and conducted using SPSS software version 25.0 and GraphPad Prism software version 8.0.
Results
Patients characteristics
The patient inclusion and exclusion flow chart is shown in Figure 1. In this study, a total of 125 patients with primary cancer and bladder involvement were included between December 2012 and April 2020, meeting the specified criteria. Among them, two patients with histologically diagnosed squamous cell carcinoma and two with different malignancies (one gastric cancer and one prostate cancer) were excluded. Additionally, 15 patients were excluded because cystectomy was not performed, comprising 6 who abandoned treatment, 4 under palliative care and 5 who experienced regression of the bladder invasion site post-neoadjuvant therapy. The final analysis focused on 105 patients who underwent bowel cancer combined with cystectomy for CRC. The study included 50 patients in the bladder invasion (+) group and 55 patients in the bladder invasion (−) group.

Patient screening flow chart.
Table 1 comprehensively displays the patient characteristics. Of the 105 patients, 75 (71%) were male. The median age was 59 years (range: 46–68 years). Preoperatively, 24 patients (23%) exhibited urinary tract symptoms, including urinary tract irritation (10 cases), faecal urine (8 cases) and haematuria (6 cases). Colovesical fistula was identified in 28 patients (27%) before or during surgery. All patients showed suspected bladder invasion (clinical T4) or clinical symptoms in the preoperative assessment. Cystoscopy was performed before surgery in 30 patients (29%), 94 (90%) patients underwent CT scans, 57 (54%) underwent pelvic MRI and 14 (13%) had PET-CT scans. Fifty-two patients underwent both CT and MRI scans, 6 underwent both CT and PET-CT scans and 2 underwent both MRI and PET-CT scans. Among the 35 patients (33%) who received preoperative chemotherapy, 12 had stage IV disease, 9 had tumours invading the bladder mucosal layer detected by preoperative cystoscopy and received preoperative chemotherapy to preserve the bladder organ, 6 were mid to lower rectal cancer combined with lymph node metastasis and the remaining 8 patients had tumours that were too large to be resected directly. Two patients also receiving radiotherapy and three patients using PD-1 inhibitors.
Characteristics of CRC patients with bladder invasion.
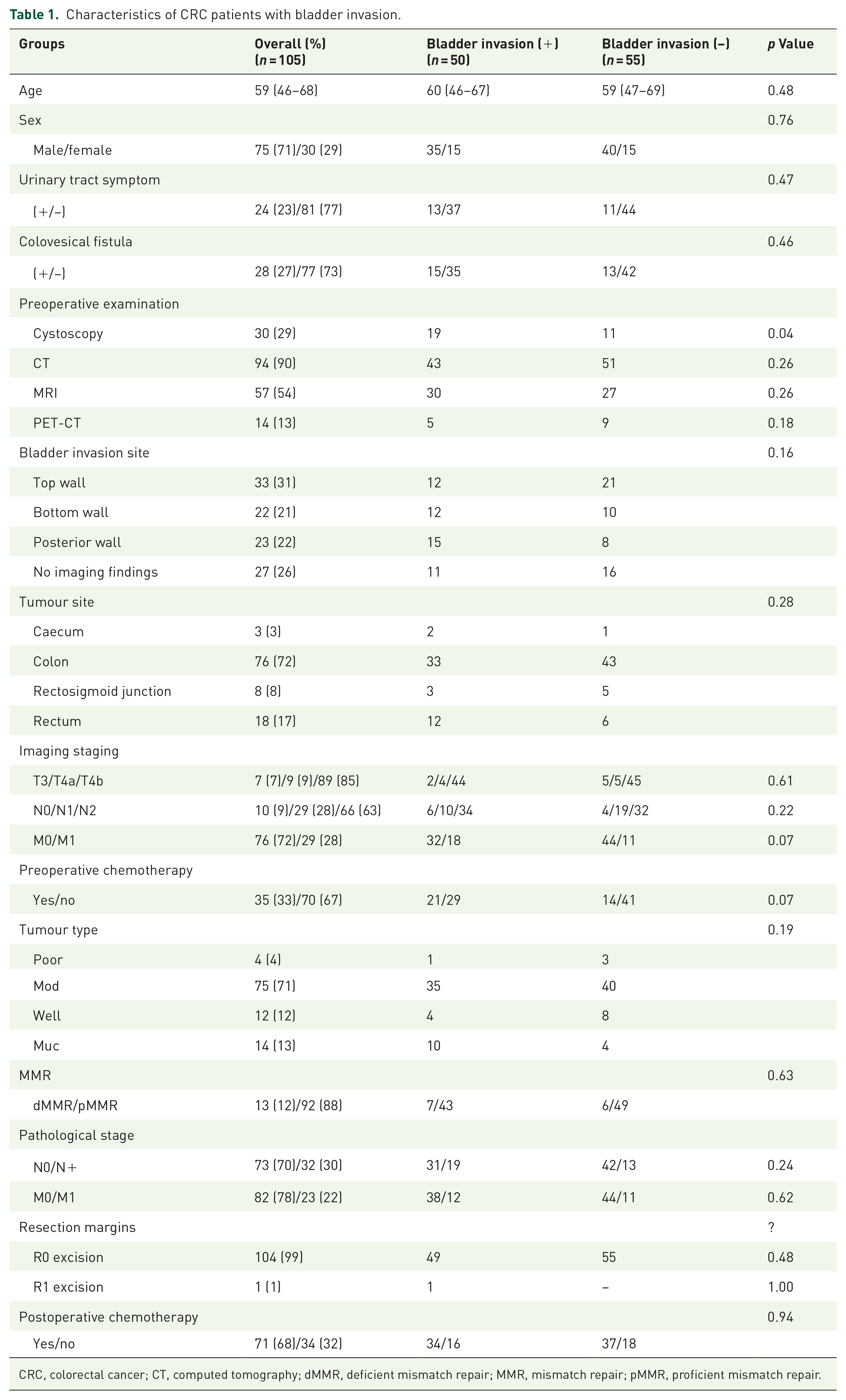
CRC, colorectal cancer; CT, computed tomography; dMMR, deficient mismatch repair; MMR, mismatch repair; pMMR, proficient mismatch repair.
As per CT reports, 33 cases (31%) involved the parietal wall, 22 (21%) involved the basal wall, 23 (22%) involved the posterior wall and no infiltration was detected in 27 cases (26%). All patients received combined radical bowel cancer and cystectomy. Cystectomy techniques varied based on the surgeon’s decision. The main tumour sites were the sigmoid colon (76 cases, 72%) and rectum (18 cases, 17%). Radiographic TNM staging indicated T4b in 89 patients (85%) and distant metastases (M1) in 29 (28%). Patients were then categorized into bladder invasion (−) (n = 55) and bladder invasion (+) (n = 50) groups.
Pathological findings revealed 4 cases of poorly differentiated adenocarcinoma, 75 cases of moderately differentiated adenocarcinoma, 12 cases of highly differentiated adenocarcinoma and 14 cases of mucous adenocarcinoma. Immunohistochemistry results showed 13 cases of dMMR and 92 cases of pMMR. Pathological TNM staging showed lymph node metastasis as positive (N+) in 32 cases and negative (N−) in 73 cases, with confirmed distant metastasis in 23 cases (M1). Pathological bladder invasion was evident in 9 cases (82%) during total cystectomy and 41 cases (43.6%) during partial cystectomy. Table 1 reveals distinctions in cystoscopy between groups (p = 0.04); no significant differences were found for other reference variables, such as preoperative urinary tract symptoms, colovesical fistula, bladder infiltration site, tumour primary site, imaging TNM stage, tumour type, pathological TNM stage, R0 excision and postoperative chemotherapy (all p > 0.05).
Surgical outcomes of total cystectomy and partial cystectomy in two groups
As indicated in Table 2, among the 105 patients, 11 (10.5%) underwent total cystectomy with a well-defined ileal catheter constructed, and 94 underwent partial cystectomy. Laparoscopic resection was carried out in 41 patients (39%), with open surgery midway occurring in 19 (18%). The median operative time was 293 (range: 228–339) min, with 630 (range: 361–731) min for total cystectomy and 269 (range: 211–344) min for partial cystectomy. The median intraoperative blood loss was 200 (range: 100–300) ml, and the median postoperative hospital stay was 14 (range: 10–19) days. Among the patients, 4 who underwent total cystectomy had a total pelvic resection, 12 underwent partial cystectomy and vesicostomy and 10 underwent ureteral bladder replantation. Postoperative complications occurred in 38 patients (36%), encompassing anastomotic fistula (8 patients, 7.6%) and infections (20 patients, 19%), including urinary tract (7 cases), pulmonary (4 cases), abdominal cavity (5 cases) and wound (4 cases) complications. The shock occurred in four patients (3.8%), six other complications including intestinal obstruction, multiple organ failure, deep vein thrombosis, atrial fibrillation, hypoproteinaemia and subcutaneous emphysema (1 case each, 0.95%). With 19 cases of Clavien–Dindo ⩾3a complications, 5 cases for total cystectomy and 14 for partial cystectomy. Within 30 days after partial cystectomy, one patient (0.95%) died due to multiple organ failure. In the bladder invasion (+) group, partial cystectomy had significantly less operating time, blood loss during surgery, surgical complications and Clavien–Dindo grade III complications compared to the total cystectomy subgroup (p < 0.05).
Surgical outcomes of total cystectomy and partial cystectomy.

C-D ⩾ 3a, Clavien–Dindo 3a; LOS, length of hospital day; TPR, total pelvic resection; UBR, ureteral bladder replantation.
Total cystectomy versus partial cystectomy
Partial and total cystectomy decisions rely on preoperative CT, magnetic resonance imaging results and cystoscopy. A review of 11 total cystectomy cases revealed that 7 patients (64%) had peritoneal metastasis, 6 patients (55%) had recurrence after completing curative-intent chemoradiotherapy for rectal cancer and 3 patients (27%) showed no initial bladder invasion despite recurrence. Four patients (36%) developed urinary tract symptoms before surgery. A total cystectomy is an option for recurrent CRC with bladder invasion, other pelvic organ involvement and severe urinary tract symptoms. The complexity of partial resection in these areas and its impact on urinary system function guides this choice.
Follow-up and recurrence
The mean follow-up duration was 36 ± 9.5 months. The median relapse time was 15 months (interquartile range (IQR) = 8.5–20). Five patients were lost during follow-up, yielding an overall mortality rate of 29% (29 patients). In the bladder invasion (+) group, 3-year OS and RFS rates were 62.97% and 57.35%, respectively, with 3-year LR and intravesical recurrence rates of 18.62% and 7.73% (Figure 2(a)–(d)). The bladder invasion (−) group exhibited 3-year OS and RFS rates of 77.16% and 58.68%, respectively, with 3-year LR and intravesical recurrence rates of 25.83% and 11.82%, respectively (Figure 2(a)–(d)). There were no significant differences in 3-year OS and RFS rates between the bladder invasion (+) and bladder invasion (−) groups (p > 0.05) or in 3-year LR and intravesical recurrence rates (p > 0.05). In the bladder invasion (+) group, the 3-year OS rate for partial cystectomy was 70.17%, and total cystectomy was 33.33% (p = 0.054); the 3-year disease-free survival rate for partial cystectomy was 62.16%, and total cystectomy was 25.93% (p = 0.13) (Figure 3(a) and (b)).

Comparison of survival curves between the bladder invasion (+) group and bladder invasion (−) group. (a) Comparison of the 3-year overall survival rates between the two groups. (b) Comparison of the 3-year recurrence free survival rates between the two groups. (c) Comparison of the 3-year local recurrence survival rates between the two groups. (d) Comparison of the 3-year intravesical recurrence survival rates between the two groups.

Comparison of survival curves between partial cystectomy and total cystectomy in the bladder invasion (+) group. (a) Comparison of the 3-year overall survival rates between the two groups. (b) Comparison of the 3-year recurrence free survival rates between the two groups.
During follow-up, 26 patients (26%) experienced LR, with 23 cases occurring after partial cystectomy and 3 following total cystectomy. Among the 96 stage cT4 patients completing follow-up, 34 received neoadjuvant therapy. LR incidence was not significantly affected by neoadjuvant therapy (36% vs 18%; p = 0.11) or adjuvant therapy (24% vs 27%; p = 0.52).
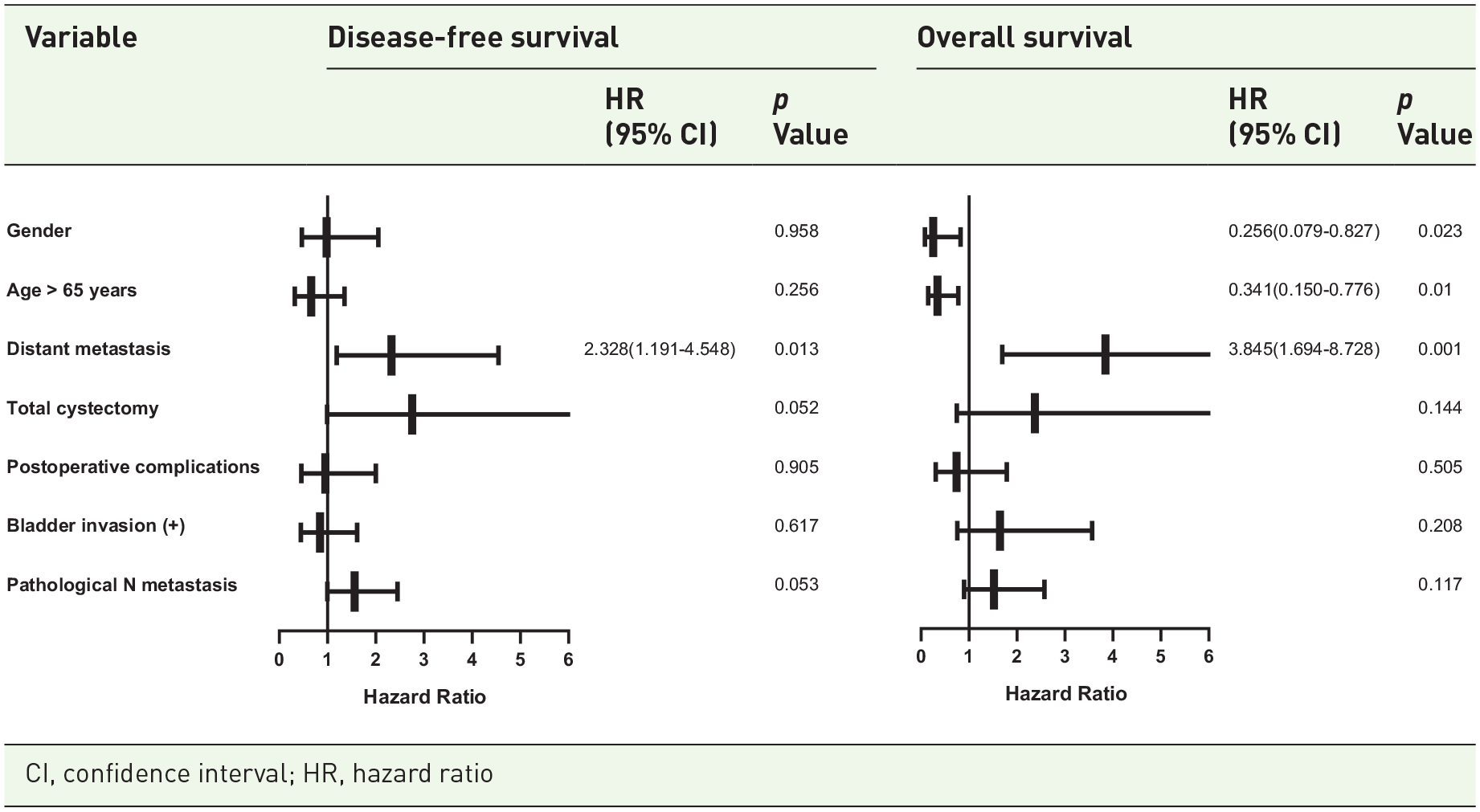
Univariate Cox regression analysis (Supplemental Figures 1 and 2) was used to examine factors including sex, age >65, neoadjuvant therapy, distant metastasis, total cystectomy, postoperative complications, bladder invasion (+), pathological lymph node metastasis and postoperative chemotherapy. Distant metastasis had a notable impact on both OS (hazard ratio (HR): 2.715; 95% confidence interval (CI): 1.458–5.056) and relapse-free survival (HR: 3.428; 95% CI: 1.650–7.122). Total cystectomy posed the highest risk for relapse-free survival (HR: 2.314; 95% CI: 1.063–5.037), and being female correlated with better OS (HR: 0.342; 95% CI: 0.119–0.984). Multivariate Cox regression analysis (Table 3) confirmed distant metastasis as significantly and independently linked to poorer relapse-free survival (HR: 2.328; 95% CI: 1.191–4.548) and OS (HR: 3.845; 95% CI: 1.694–8.728). In addition, Table 4 shows a literature review of all reports of CRC with bladder invasion, including detailed postoperative urinary complications, pathologic diagnosis rates and survival.
Multivariate Cox regression analysis of colorectal cancer with bladder invasion.

Reports on colorectal cancer with bladder invasion.

AL, anastomotic leak; AS, abdominal sepsis; CA, cerebrovascular accident; DFS, disease-free survival; IP, intestinal perforation; MOF, multiple organ failure; OS, overall survival; PE, pulmonary embolism; y, years.
As depicted in Supplemental Table 1, nine patients (10%) had intravesical recurrence after partial cystectomy at a median interval of 8 months (IQR = 6.5–13.5). Among these, six patients showed no histologically confirmed infiltration after partial cystectomy. The 3-year recurrence rate after partial cystectomy was 7.73% (n = 46) for patients with pathological bladder invasion, and patients without pathological bladder invasion had a 3-year recurrence rate of 11.82% (n = 54).
SHG imaging displays and collagen feature analysis
A total of 142 collagen features for all enrolled patients are extracted from multiphoton images. We included a total of 24 patients, consisting of 6 patients in the bladder invasion (+) group (3 with bladder recurrence and 3 without), and 18 patients in the bladder invasion (−) group (6 with bladder recurrence and 12 without). We selected SHG images from 4 representative patients (Green represents collagen), covering cases of bladder invasion positive/negative with and without bladder recurrence (Figure 4(a)). Figure 4(b) displays the expression of 142 collagen characteristics and clinical features of the 24 enrolled patients. However, we did not find statistically significant differences in collagen characteristics among these samples.
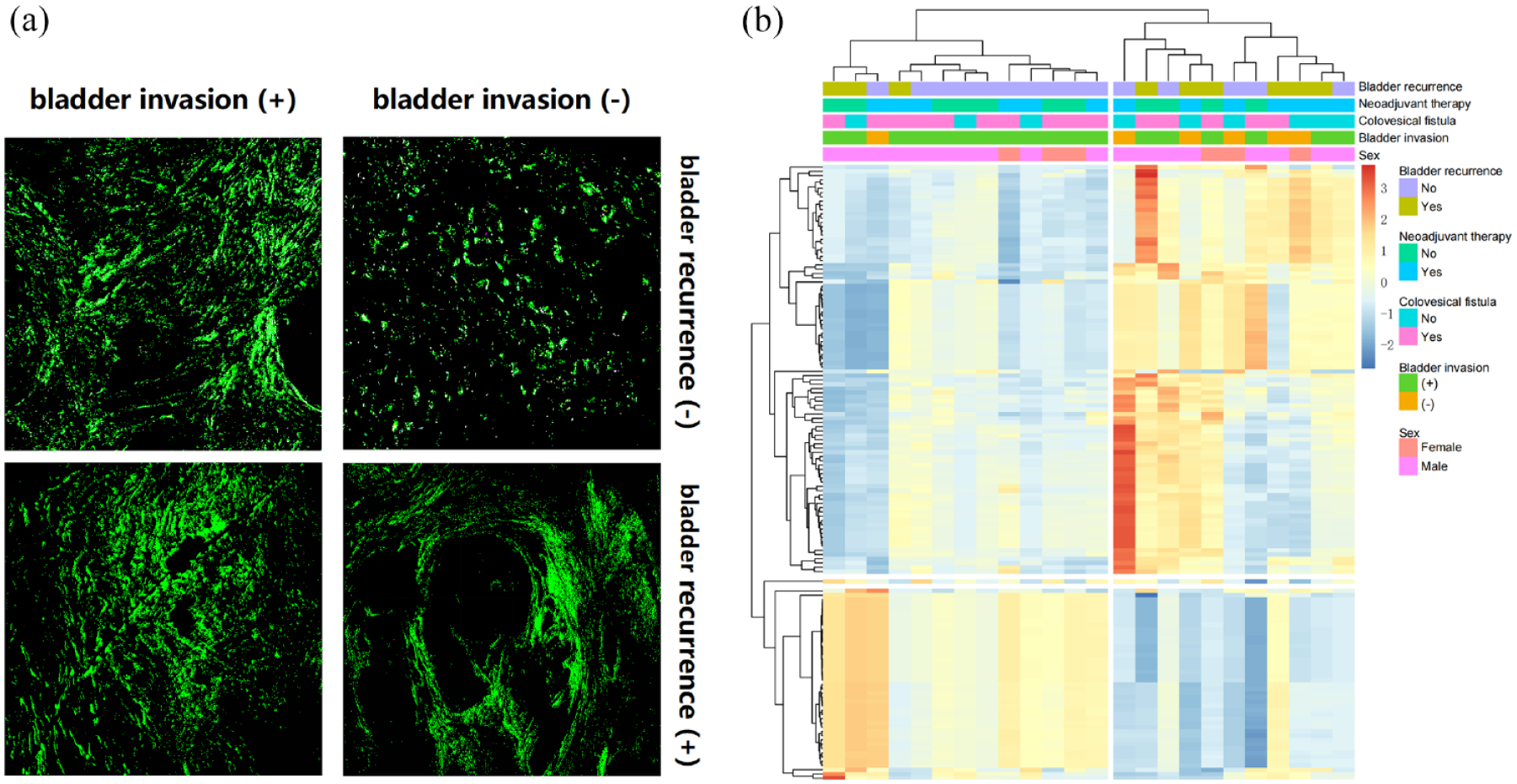
SHG imaging and collagen feature analysis of bladder-invasive CRC patients. (a) Corresponding SHG image (green represents collagen). (b) Clinical characteristic analysis of 24 samples and quantitative analysis of 142 collagen features.
Discussion
This study investigates the impact of pathological bladder invasion on long-term tumour survival in CRC patients with clinically diagnosed bladder invasion after cystectomy. Our findings revealed no significant difference in the 3-year OS and RFS rates between the bladder invasion (−) and bladder invasion (+) groups. Additionally, there were no significant differences in the 3-year LR rate and intravesical recurrence rate. For CRC patients, mere pathological bladder invasion seems to have minimal impact on survival prognosis. This led us to delve into subgroup analysis. Upon further investigation, our data showed no significant differences in 3-year OS and RFS rates between total cystectomy and partial cystectomy in the bladder invasion (+) group, aligning with prior studies. Partial cystectomy is feasible for CRC patients with pathological bladder invasion, offering advantages such as shorter operation time, reduced surgical bleeding and fewer postoperative complications compared to total cystectomy.
Over time, numerous scholars have presented divergent perspectives on the selection between the two types of cystectomy. In 1999, Balbay et al. 11 suggested that partial cystectomy might be appropriate for female patients or male patients with solely localized bladder involvement. In 2001, Weinstein et al. 33 discovered that a significant portion of excised bladder specimens did not exhibit cancerous infiltration but instead dense fibrous adhesions. They recommended en bloc removal of the affected area during partial cystectomy rather than attempting forceful separation. 17 In 2014, Courtney et al. 34 found that a 2–3 cm negative incisal margin was crucial for successful resection of tumour-adherent portions on the bladder. In 2018, Nerli et al. 19 recommended determining cystectomy and ileal catheter urine diversion based on intraoperative surgeon judgement or frozen pathology of the incisal margin. In the same year, Diaconescu et al. 35 emphasized that the decision to preserve the bladder during surgery should be based on the potential to achieve R0 excision. In 2019, Yoshida et al. 9 suggested that confirming bladder invasion in CRC patients during surgery necessitates removing all layers of the bladder wall to achieve a gross surgical margin of at least 1 cm from the infiltrated area. They also recommended the insertion of a ureteral stent before or during surgery to prevent ureteral damage. 9 Currently, partial cystectomy is the favoured surgical approach. However, total cystectomy is advisable for intricate tumour resections, involvement of the bladder sphincter or triangle and an estimated bladder volume below 50 ml after partial cystectomy. This considers the challenge of balancing R0 excision and preserving bladder function.9,10 Nevertheless, given the short-term and long-term complications linked with total cystectomy, the option of minimally invasive surgery is also being explored. 10 Comparing the two procedures, partial cystectomy offers the advantage of no stoma but may require a temporary catheter or vesicostomy. Early research is limited, but Luo et al. 17 showed that bladder invasion confirmed by post-cystectomy pathology correlated with bladder recurrence and distant metastasis, impacting LR and long-term survival.
The decision between partial and total cystectomy should holistically consider achieving a clear margin, assessing LR risk and preserving bladder function. Given the low correlation between preoperative imaging and pathology, along with patient-centred concerns about oncologic efficacy and quality of life, partial cystectomy emerges as the favoured option for CRC not invading the bladder mucosal surface. 9 Recent studies affirm favourable outcomes with local R0 resection following partial cystectomy in patients without distant metastases.7–11,19,20,33–35
Furthermore, the primary distinction between partial cystectomy and total cystectomy on the oncologic front is with regard to the bladder recurrence risk.8,9 Yoshida et al. 9 demonstrated that the extent of bladder wall invasion impacts the intravesical recurrence risk following partial resection of colon cancer with bladder invasion. In cases in which a colon tumour infiltrates the bladder mucosa, vigilant monitoring for intravesical recurrence is crucial. Close CT and cystoscopy are recommended during the initial 2 years after partial cystectomy. They also speculated that intravesical irrigation with saline or chemotherapy agents after partial cystectomy can markedly decrease the risk of intravesical recurrence, offering novel treatment insights. In addition, intraoperative fluorescence guidance is valuable for precisely identifying and removing CRC, reducing damage to surrounding healthy tissues and potentially improving long-term outcomes. 36 Although there are no studies using fluorescent cystoscopy to assist in diagnosing bladder invasion in CRC patients, it has been proven in bladder cancer patients that the use of fluorescence cystoscopy and narrow-band imaging can increase tumour detection rates and reduce recurrence, particularly for non-muscle-invasive bladder cancer. 37
In our study, we identified nine cases of bladder recurrence following partial cystectomy, with six cases occurring in the bladder invasion (−) group, surpassing those in the bladder invasion (+) group. This distinct pattern prompted us to conduct an in-depth analysis of these nine patients experiencing bladder recurrence. Among them, moderately differentiated adenocarcinoma was found in pathological findings for the majority. However, it is noteworthy that four patients had preoperative or intraoperative diagnoses of colovesical fistula, suggesting the potential for incomplete sampling of postoperative pathology in such cases, which might lead to false negative outcomes. When a colovesical fistula is present in the absence of pathological bladder invasion, it is imperative to carefully assess the risk of bladder recurrence following partial cystectomy. Therefore, we selected 24 samples for multiphoton imaging and extracted 142 collagen features from each sample. Although the expression of collagen features varied across different groups, we did not find any statistically significant differences, which may be due to the small sample size. We also extensively reviewed all relevant literature concerning bladder invasion in CRC (Table 4). Based on the combined results of 15 studies, the 3-year OS rates ranged from 82% to 91%, the 5-year OS rates ranged from 39% to 75%, the 5-year LR rates ranged from 11% to 37% and the rates of pathological bladder invasion compliance ranged from 37% to 54% across most of the studies.4,7–20 In comparison with our study, the outcomes align closely with previous research findings. Notably, due to the limited availability of literature focusing on complications following cystectomy for bladder invasion in CRC, we conducted an extensive review encompassing all urinary system-related complications post-cystectomy. We found that urinary tract leakage and urinary system infections emerged as the most prevalent issues, followed by urinary retention and hydronephrosis. Notably, some studies lacked comprehensive recording of postoperative complications for total cystectomy and partial cystectomy, mainly due to constraints in grouping and relevant data. In recent years, Kondo 10 highlighted a substantial reduction in complications such as urinary leakage and anastomotic fistula following partial cystectomy when compared to total cystectomy (51.4% (n = 37) vs 94.4% (n = 17)). Their multivariate Cox regression analysis indicated that in comparison with the total cystectomy group, the partial cystectomy group exhibited a lower incidence of urinary retention, a decreased rate of LR and a higher OS rate. 10 Furthermore, our study’s findings revealed that partial cystectomy has significantly shorter operative times, lower blood loss and fewer postoperative complications than total cystectomy, consistent with findings from other studies.8–10 Van Kessel et al. 38 proposed that patients who undergo partial cystectomy often experience long-term urinary problems, and the quality of life outcomes for two types of cystectomy are similar, with significant improvements observed after surgery. Although we did not use specific scales for scoring, we observed that 37 patients who underwent partial cystectomy verbally expressed satisfaction with their urinary function and better quality of life. Only three patients who underwent total cystectomy had an improvement in quality of life. Despite experiencing symptoms such as urinary tract infections, patients recovered gradually with active postoperative management.
In our study, multivariate Cox regression analysis indicated that distant metastasis was an independent risk factor linked to reduced relapse-free survival and OS. The N stage did not show a significant difference in analysis, primarily likely due to the influence of distant metastasis. Interestingly, bladder invasion (+) did not emerge as a factor impacting relapse-free survival and OS. This finding reinforces the notion that straightforward pathological bladder invasion does not impact the long-term survival of these patients, aligning closely with previous study outcomes.10,15,16 Total cystectomy is an independent risk factor linked to diminished RFS. Our assessment of the preoperative status of 11 patients undergoing total cystectomy showed that more than half had recurrent CRC; in the remainder, tumours invaded the bladder triangle or involved other pelvic organs. Coupled with the pathological observation of a less than substantial concurrence rate of bladder invasion, advocating for partial cystectomy is noteworthy for primary CRC patients with bladder invasion. Given evolving treatment paradigms and patients’ inclination towards improved quality of life, the future use of total cystectomy warrants heightened prudence.
Limitations
Several limitations should be acknowledged in our study. First, our analysis was confined to a single-centre retrospective approach with a relatively modest sample size (n = 105), potentially limiting the robustness of our findings. Second, retrospective acquisition of patient data introduces selection bias that may influence outcomes. Additionally, due to funding and sampling limitations, the number of samples undergoing multiphoton detection is insufficient. Nonetheless, we remain optimistic about the possibility of future scientific and valuable research endeavours aimed at further exploring the feasibility of partial cystectomy in this patient population.
Conclusion
Pathological bladder invasion impacts CRC patients’ post-cystectomy survival may be less than what clinical practice implies, and factors for bladder recurrence require further assessment. Partial cystectomy in cases with pathological bladder invasion may offer the opportunity to achieve similar survival rates to total cystectomy, having a lower incidence of complications and better bladder organ preservation.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848241308387 – Supplemental material for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study
Supplemental material, sj-pdf-1-tag-10.1177_17562848241308387 for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study by Bing Lan, Rui Luo, Yang Li, Shijie Wang, Wei Jiang, Yun Zhong, Xuneng Zhang, Qingyang Zheng, Zichuan He, Bo Ma, Hui Wang, Keli Yang and Huaiming Wang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848241308387 – Supplemental material for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study
Supplemental material, sj-pdf-2-tag-10.1177_17562848241308387 for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study by Bing Lan, Rui Luo, Yang Li, Shijie Wang, Wei Jiang, Yun Zhong, Xuneng Zhang, Qingyang Zheng, Zichuan He, Bo Ma, Hui Wang, Keli Yang and Huaiming Wang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-3-tag-10.1177_17562848241308387 – Supplemental material for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study
Supplemental material, sj-pdf-3-tag-10.1177_17562848241308387 for Partial cystectomy as a surgical option for colorectal cancer patients with pathological bladder invasion: an original retrospective study by Bing Lan, Rui Luo, Yang Li, Shijie Wang, Wei Jiang, Yun Zhong, Xuneng Zhang, Qingyang Zheng, Zichuan He, Bo Ma, Hui Wang, Keli Yang and Huaiming Wang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
This study is supported by the National Key Clinical Discipline, and the authors thank the School of Science, Jimei University, Xiamen, Fujian, People’s Republic of China for providing the multi-photon technology platform.
Authors’ note
Meeting presentation: Our research abstract was accepted for ESMO GI 2024 and presented as a poster at the International Congress Center in Munich, Germany, on June 27.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.