
Abstract
Background:
Morphological and functional cardiac involvement is rarely described in patients with inflammatory bowel disease (IBD) but there is evidence that they have an increased risk of cardiovascular (CV) events despite the lower prevalence of traditional CV risk factors.
Objectives:
Our systematic review and meta-analysis examined the relationship between IBD and cardiac function, namely the incidence of heart failure (HF) and subclinical echocardiographic changes.
Data sources and methods:
Two medical databases, PubMed and Scopus, were systematically searched up to September 2022 to identify all studies reporting HF and/or echocardiographic changes in IBD patients.
Results:
The qualitative analysis comprised a total of 18 studies (14 retrospective and 4 prospective studies) involving 59,838 patients. IBD was associated with subtle systolic and diastolic alterations, vascular dysfunction, increased risk for HF hospitalizations, and globally worse CV outcomes. Nine studies were included in the meta-analysis. In the IBD population, we found statistically significant reduced early to late diastolic transmitral flow (E/A), higher E to early diastolic mitral annular tissue velocity (E/e′), and decreased global longitudinal strain. Increased left atrial diameter and area were also present in IBD patients but no statistical significance was reached. Inter-atrial and right intra-atrial conduction delays were observed.
Conclusion:
The IBD population has an increased risk for left ventricular and atrial dysfunction, vascular changes, arrhythmias, and HF hospitalization. Screening with sensitive imaging like speckle tracking echocardiography could identify early subclinical changes. IBD is in fact a CV risk factor and tight inflammation control may reduce CV risk.
Plain language summary
Introduction
Inflammatory bowel disease (IBD) is a chronic immunomodulated disease of unknown etiology comprising Crohn’s disease (CD) and ulcerative colitis (UC). It is characterized by chronic relapsing and remitting inflammation of the gastrointestinal tract. While some extra-intestinal manifestations are common (mainly osteoarticular, cutaneous, and ocular), others, such as cardiac involvement, are rarely seen. 1
IBD patients are mainly represented by young otherwise healthy patients, at least in the first years after the diagnosis. Nevertheless, the risk of CV events is higher in IBD patients.2,3 The pathogenesis of cardiac involvement in IBD patients is not clearly understood, but there are several potential mechanisms described.
First, chronic inflammation plays a central role in all phases of the atherosclerotic process through direct impact on endothelial dysfunction, hypercoagulability, and indirect disturbance of regular lipid metabolism. 2 Furthermore, an inflammatory environment leads to collagen deposition which can occur at cardiac extracellular matrix proteins and endocardial fibers changing the morphological structure of the myocardium, and therefore its appropriate function. 4 On the other hand, the increased systemic immune response observed in these patients may cause myocarditis/pericarditis. 5 In fact, mediators, such as tumor necrosis factor (TNF-a), interleukin-1 (IL-1), and IL-6, that are increased in IBD patients even in the remission phase, may cause cytotoxic damage in myocytes. 6 Second, IBD patients are at higher risk of nutritional deficits in relation to chronic malabsorption which may compromise heart health. 7
In addition, there is a major risk of drug-related cardiotoxicity. In fact, corticosteroids, TNF-alpha inhibitors, some Janus kinase (JAK) inhibitors, and selective sphingosine 1-phosphate receptor modulators have undesired cardiac effects which can accelerate the CV pathological process.8–14 It is important to notice that, regarding anti-TNF-alpha therapy, initial studies aimed to determine whether infliximab could yield positive effects in non-IBD patients with moderate-to-severe heart failure (HF). However, these studies not only failed to show any favorable effects but also revealed an elevated risk of worsening HF. 15 In spite of that, recent studies have demonstrated a decreased risk of CV events in IBD patients exposed to anti-TNF-alpha therapy.16–21 Further research is required to determine whether this is linked to the management of disease activity or the underlying mechanism of the drug. As for ustekinumab, a monoclonal antibody targeting IL-12/23p40, 2-year follow-up data from CD and UC trials did not demonstrate an impact on CV events risk.22,23 Nevertheless, a recent epidemiological study reported a potential link between ustekinumab treatment and CV adverse events in patients with a high CV risk profile. 24 Further investigations are needed to clarify this association. In regard to anti-integrins, randomized controlled trials and real-world observational studies have not found an increase in CV events in IBD patients on vedolizumab.25–28 Despite this, data from long-term studies are lacking.
Furthermore, early cardiac death is increased in the IBD population, and the CV events go from myocarditis, pericarditis, cardiomyopathies, myocardial infarction, atrial fibrillation (AF), stroke, and HF. 29 The increased CV risk in these patients might be fundamentally dependent on chronic systemic inflammation rather than traditional risk factors such as hyperlipidemia, hypertension, obesity, smoking, and alcohol use. 2
Even though cardiac involvement and complications are rare, it is crucial to screen IBD patients to detect them early. 30 Previous studies suggested that some subclinical CV features such as abnormal echocardiographic parameters can predict and stratify patients who are at an increased risk of CV intercurrence.8,31,32 Diastolic dysfunction represents a combination of impaired left ventricular (LV) relaxation, restoration forces, myocyte lengthening load, and atrial function which leads to increased LV filling pressures.33,34 Early to late diastolic transmitral flow (E/A) is used to assess diastolic function and E to early diastolic mitral annular tissue velocity (E/e′) estimates LV filling pressures. To evaluate global LV function, left ventricular ejection fraction (LVEF) is the most widely used parameter. However, global longitudinal strain (GLS) is a more sensitive parameter, especially for detecting subclinical LV dysfunction when LVEF is within the normal range. GLS represents the percentage of myocardial fiber shortening in the longitudinal direction during systole, reflecting LV deformation, and more negative values are considered indicative of better systolic function. 35 Left atrial (LA) dimensions are correlated with systolic and diastolic function. Impaired LA function resulting in increased dimensions can be a marker of diastolic dysfunction when the left ventricle has decreased relaxing and filling properties. 36 Electrophysiological and electromechanical abnormalities originating from intra-atrial and inter-atrial conduction disturbances are associated with an increased risk of AF. 37 Moreover, an increase in atrial electromechanical delay (AEMD) duration was shown to be an independent variable for AF development. Supplemental Tables 1 and 2 present the most relevant echocardiographic parameters with the corresponding definition and interpretation.33–35,38–42
In the literature, we found seven systematic reviews underlying the topic of CV impact and IBD disease.2,3,8,43–46 However, to our knowledge, there are currently no systematic reviews on echocardiographic changes in IBD patients. This review aims to summarize the latest evidence of the association between IBD and heart function and structural abnormalities that can lead to HF. Our meta-analysis mainly adds up to the subclinical echocardiographic changes in patients with IBD. This work is the result of an ongoing collaboration between the gastroenterology and cardiology departments of our unit.
Materials and methods
Study design and data sources
We performed a systematic review and meta-analysis based on the guidelines dictated by PRISMA. Two medical databases, PubMed and Scopus, were systematically searched.
Search strategy
The article search was conducted independently by two authors until September 19, 2022. The following search queries were utilized in the “Advanced search” section of the PubMed and Scopus databases. From PubMed: ((“heart failure”) and (“inflammatory bowel disease”)), ((“heart failure”) AND (“ulcerative colitis”), (“heart failure”) AND (“Crohn’s disease”)), ((“inflammatory bowel disease”) AND (“echocardiography” OR “echocardiogram”)), ((“ulcerative colitis”) AND (“echocardiography” OR “echocardiogram”)), and ((“Crohn’s disease”) AND (“echocardiography” OR “echocardiogram”)). From Scopus: (ABS ( “HEART FAILURE”)) AND (ABS (“INFLAMMATORY BOWEL DISEASE”)), (ABS (“HEART FAILURE”) AND ABS (“CROHN’S DISEASE”)), (ABS (“HEART FAILURE”) AND ABS (“ULCERATIVE COLITIS”)), (ABS (“inflammatory bowel disease”) AND (“echocardiography” OR “echocardiogram”)), (ABS (“ulcerative colitis”) AND (“echocardiography” OR “echocardiogram”)), and (ABS (“Crohn’s disease”) AND (“echocardiography” OR “echocardiogram”)).
Eligibility criteria
We included randomized controlled trials, observational studies, case–control studies, and cohort studies comparing HF, and/or echocardiographic changes between IBD patients (UC and CD; age ⩾16 years old) and healthy individuals, with sufficient data to extract the effect estimates. Studies that evaluated electrocardiographic changes and other cardiac imaging modalities were also eligible. There were no restrictions regarding patients’ past medical history or the treatment approach employed for managing their disease. Only articles published in English were included. Case reports, as well as those detailing laboratory, in vitro, or animal studies, were excluded.
Outcomes
The main outcome of interest in our systematic review was the association between IBD and the heart’s functional and structural abnormalities that can lead to HF. Other outcomes included the impact of disease activity, duration, and treatment (mainly corticosteroids and TNF-alpha inhibitors) on cardiac health.
In the meta-analysis, the main focus resided on quantifying subclinical echocardiographic changes in IBD patients compared to healthy individuals. The cardiac changes were divided into their structural and electrical components, and echocardiographic parameters were selected by their clinical and practical relevance.
Data extraction
Two independent reviewers performed the data selection and extraction process using the pre-established form. The information extracted from each eligible study included the following: author(s), year of publication, study design, sample size, participant characteristics (age, sex, type of IBD), details of the IBD treatment approach used, echocardiographic, electrocardiographic, and other cardiac imaging parameters, main outcomes, and key findings.
Any discrepancies between the two reviewers were resolved through discussion and, when necessary, consultation with a third reviewer. It is important to note that not all variables outlined in the data extraction process were covered in each study included in our review. Missing data were objectively reported through the number of studies that provided information on specific variables. This was considered in the section “Discussion,” and the potential impact on overall findings is acknowledged.
Quality assessment
The methodological quality of each study was assessed using the validated CASP for cohort studies. This tool consists of three sections (“Are the results of the study valid?”—Section A; “What are the results?”—Section B; “Will the results help locally?”—Section C) and each question is answered based on “yes,” “no,” and “can’t tell.” Then an overall appreciation is obtained. 47
Statistical analysis
Data analysis was conducted using the Cochrane Review Manager Software (Review Manager (RevMan). Version 5.4. The Cochrane Collaboration, 2020). For individual measures of interest, a meta-analysis was performed if studies reported continuous variables as means and standard deviations. Data were then meta-analyzed using a random-effects model for overall effect size and assessed through standardized mean difference at a 95% level of confidence. Statistical significance was evaluated at p < 0.05. Heterogeneity was assessed using I-square test (I2). An I2 above 50% was defined as the cutoff for moderate heterogeneity, and low heterogeneity was determined above 25%. High heterogeneity was defined by I2 above 75%. 48
A sensitivity analysis for each meta-analysis with at least three studies was conducted. Within each meta-analysis, each study was taken out one at a time and recalculated the pooled effect size and I2 to assess the influence of each study.
Funnel plot was the method used to assess the potential of publication bias.
Results
Search results
The total number of records identified through our search was 1287. We proceeded to duplicate elimination using the Rayyan online tool, obtaining a total of 658 articles. Subsequently, the remaining studies were screened by manually reviewing their titles and abstracts, and at this phase, 562 articles were excluded. In all, 96 full-text articles were assessed for eligibility. A total of 18 were considered eligible for qualitative synthesis. From the selected studies, nine were included for meta-analysis. Figure 1 shows the PRISMA flowchart depicting the search and selection process (Supplemental Table 3). The exclusion explanation step by step is presented as Supplemental Material (Supplemental Table 4).
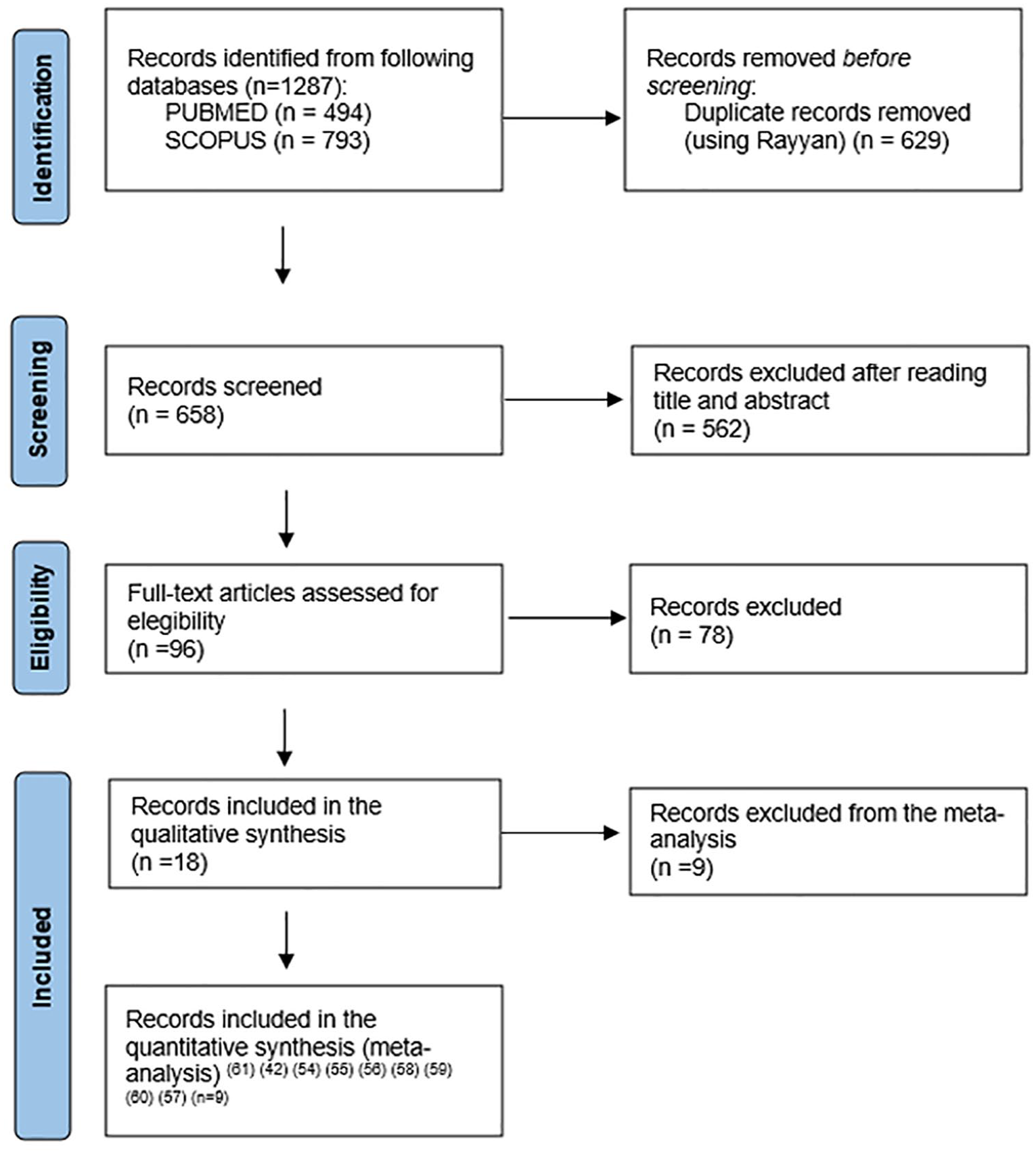
PRISMA flowchart depicting the search and selection process.
Quality assessment
The evaluation obtained through CASP Checklists showed that all included studies clearly stated the issue evaluated (Supplemental Table 5). On the other hand, most of them addressed the most relevant confounding factors.
Characteristics of included studies
All included studies were cohorts, and the majority were retrospective. Nine studies included both CD and UC patients, four included only CD patients and three UC patients only. The detailed characteristics and outcomes of the eligible studies are presented in Table 1. A total of 59,838 patients with IBD from the 18 studies were included in this review. Two articles included IBD patients without specified subtypes. Six studies analyzed IBD patients according to disease activity. Age, disease duration, disease activity, localization, and/or behavior were considered in 10. The impact of medical therapy was descriptively analyzed in 11 studies.
Individual study characteristics and the outcomes analyzed in each study.

AEMD, atrial electromechanical delay; aHR, adjusted hazard ratio; AMI, acute myocardial infarction; AS, ankylosing spondilitis; AZA, azathioprine; CD, Crohn’s disease; CDAI, Crohn’s Disease Activity Indez; CFR, coronary flow reserve; CI, confidence interval; CV, cardiovascular; 2D-STE, two-dimensional speckle tracking echocardiography; E/A, early to late diastolic transmitral flow; ECG, electrocardiography; ECHO, echocardiography; ESR, erythrocyte sedimentation rate; GLS, global longitudinal strain; GLSR, global longitudinal strain rate; HF, heart failure; IBD, inflammatory bowel disease; IQR, interquartile range; LV, left ventricular; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NA, not applicable; PALS, peak atrial longitudinal strain; RA, rheumatoid arthritis; TDI, tissue Doppler imaging; TNF-α, tumor necrosis factor-alpha; TWAS: Truelove and Witts Severity; UC, ulcerative colitis.
HF was the main direct outcome in four studies49,55,59,61; myocardial infarction in one 49 ; mitral valve prolapse in one 51 ; and pericardial effusion in one. 51
Twelve studies reported echocardiographic evaluation results, one reported cardiac MRI analysis, and one described non-invasive evaluation of the vascular endothelial function.
Four studies met the criteria to analyze E/A50,52,53,63 and two for E/e′,50,63 including in 295 and 144 IBD patients, respectively. Four studies, with a total of 218 IBD patients, were included to evaluate GLS.54,57,58,63 LA diameter was analyzed in six studies (340 IBD patients),42,50,52,58,60,63 and LA area in two (95 IBD patients).54,58
Electrocardiography was analyzed in three, but only the two that presented results as means and standard deviations were considered for meta-analysis, englobing 97 IBD patients.42,60 Five studies reported outcomes based only on medical records revision.49,55,59,61,62
Outcomes from a systematic review
Female patients with IBD have a higher risk of atherosclerotic cardiovascular (CV) disease compared to males and the risk is more pronounced in younger patients, despite the prevalence of traditional CV risk factors being lower. 49 After adjusting for age, sex, familial coronary disease, diabetes mellitus, hyperlipidemia, and hypertension, IBD (all subtypes) is associated with an increased risk of acute myocardial infarction (adjusted hazard ratio, aHR, 2.82; 95% confidence interval (CI), 1.98–4.04). 49 Furthermore, in a group of 68 patients with CD and 60 healthy subjects, CD patients had a statistically significant higher prevalence of mitral valvular prolapse and pericardial effusion, the last associated with high disease activity. 51 Vascular dysfunction was also objectified in patients with IBD, which presented with higher aortic stiffness and associated LV systolic and diastolic dysfunction, without known CV risk factors. 50 Furthermore, a significant impairment in coronary microvascular function in IBD patients was demonstrated which was correlated to disease activity and duration. 52
Regarding HF, a study involving 736 IBD patients (339 CD, 397 UC) compared to 1472 matched controls presented a twofold increased incidence of HF in IBD patients after adjusting for traditional CV risk factors (HR, 2.03; 95% CI, 1.36–3.03), and this risk was higher among UC, females, those with diagnosis after 40 years old, more extensive disease, and systemic steroids users.49,62 Besides that, these patients had a higher risk of first HF hospitalization, increasing to 2.5-fold risk in active stages. 59
In a small study involving 7 patients with CD, and 14 with UC, evaluating the acute and long-term effects of infliximab, there were no significant cardiac changes in 12 months follow-up. Despite that, plasma NT-proBNP mildly but significantly increased immediately after infliximab infusion. 64 Another study concluded that CD patients on anti-TNF therapy had a relative risk of HF of 1.2, but no statistical significance was reached. 55
Despite this, conflicting results are present in the literature as in an observation study involving electronic health records of 5078 IBD patients (subtype not mentioned) and there was no significant increase in incident HF in patients with IBD. 61
Echocardiographic parameters evaluating LV global function, such as GLS, show a significantly impaired function in UC and CD patients.54,57,58,63 This association was stronger in pancolitis patients and positively correlated to CDAI score.57,58 Diastolic dysfunction was consistently reported.50,60,63,65 Specific data on systolic parameters are not so widely discussed and Nar et al., 60 even outline no differences in these parameters between IBD and healthy patients. Cardiac MRI evaluations also demonstrated a reduction in right ventricular ejection fraction but no differences in LV assessment. 56
Electrical disturbances were also shown by increased AEMD duration which was correlated with disease duration and severity.42,53,60
Outcomes from meta-analysis
Effect of IBD on echocardiography and electrophysiological parameters
Functional and structural parameters
IBD and LV diastolic dysfunction parameters. There is a significant difference between controls and IBD patients showing a significant reduction in E/A ratio values for the IBD population (Std. MD −0.51, 95% CI −1.00 to −0.02; I2 = 87%), with an overall test effect of Z = 2.05 at p = 0.04 (Figure 2).

E/A values at IBD patients and controls.
Patients with IBD had significantly higher values of E/e′ ratios (Std. MD 1.46, 95% CI 0.86–2.07; I2 = 80%), with an overall test effect of Z = 4.73 at p < 0.00001 (Figure 3).

E/E′ values at IBD patients and controls.
IBD and LV global function. Overall IBD patients had a significant decrease in GLS absolute values (Std. MD 0.66, 95% CI 0.48–0.84; I2 = 0%), with an overall test effect of Z = 7.09 at p < 0.00001 (Figure 4) indicating worse GLS values.
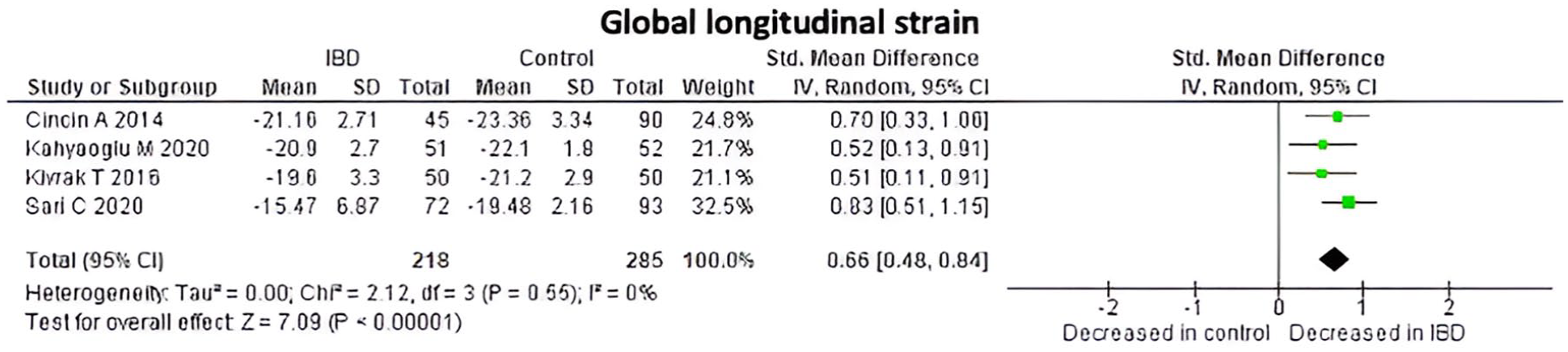
GLS values at IBD patients and controls.
IBD and LA dimensions. Overall IBD patients seem to have increased LA diameter, in millimeters (Std. MD 0.06, 95% CI −0.12 to 0.24; I2 = 20%), with an overall test effect of Z = 0.68 at p = 0.50. IBD patients had a numerically higher LA area when compared to healthy controls, but without a statistically significant difference (Std. MD 0.03, 95% CI −0.24 to 0.29; I2 = 0%; overall test effect of Z = 0.19 at p = 0.85) (Figures 5 and 6).

Left atrium diameter at IBD patients and controls.

Left atrium area at IBD patients and controls.
Electrical parameters
Inter-atrial electromechanical delay. A significant increase in inter-atrial electromechanical delay (IAEMD) was observed in IBD patients (Std. MD 0.88, 95% CI 0.45–1.31; I2 = 42%), with an overall test effect of Z = 4.02 at p < 0.0001 (Figure 7).

Inter-atrial EMD values at IBD patients and controls.
Intra-right and left AEMD (IAEMD). IBD patients had prolonged IAEMD either at right or left conduction systems. Std. MD for intra-right AEMD was 0.9, 95% CI 0.57–1.22 with an I2 = 0% and an overall test effect of Z = 5.42 at p < 0.00001 (Figure 8).

Intra-right EMD values at IBD patients and controls.
A prolonged intra-left AEMD was observed in IBD patients compared to healthy controls but without statistically significant differences (Std. MD 0.33, 95% CI −0.08 to 0.74; I2 = 41%; with an overall test effect of Z = 1.57 at p = 0.12) (Figure 9).

Intra-left EMD values at IBD patients and controls.
Discussion
This systematic review and meta-analysis examined the relationship between IBD and cardiac function, namely the incidence of HF and echocardiographic changes. The cumulative evidence derived from our study reveals a pattern of subtle, yet significant, cardiac changes among patients with IBD. We included studies with patients above 16 years to ensure the relevance of our findings to a primarily adult population. Besides that, we did not place any restrictions on the past medical history of the patients involved in these studies as we aimed to include a wide range of patients with diverse health backgrounds, which, in turn, would increase the generalizability of our findings.
Evaluating LV diastolic function and estimation of LV filling pressure is complex, and no single parameter can be utilized to determine such impairment. The most used parameters in clinical practice are E and A wave velocities, E/A ratio, e′ velocity, E/e′ ratio, E wave deceleration time, isovolumetric relaxation time (IVRT), left atrium volume, tricuspid regurgitation maximum velocity, and pulmonary venous flow patterns. In our meta-analysis, we included E/A and E/e′ ratio parameters due to the availability of the data in the included studies. In a normal heart, ventricular filling occurs in two main stages, the passive LV filling (E wave) and the atrial contraction phase (A wave). The passive LV filling phase represents the major contributor to LV filling, with atrial contraction representing an important but proportionally smaller contribution. This means that in the healthy population, the E wave is larger than the A wave, resulting in an E/A ratio greater than 1. In the elderly, the E wave tends to be smaller than the A wave, and so the E/A ratio tends to be less than 1. The E/e′ ratio is an echocardiographic parameter that reflects the relationship between early diastolic filling (E) and myocardial relaxation velocity (e′) and is widely used to estimate LV filling pressures in conjunction with the abovementioned parameters. Normal diastolic function is characterized by an E/A ratio >0.8 and a normal E/e′ ratio. Impaired relaxation shows an E/A ratio <0.8 and normal E/e′. A pseudonormal pattern occurs when the E/A ratio appears normal but E/e′ is elevated, due to a decrease in e′ which represents impaired myocardial relaxation and consequently abnormal diastolic function. This represents an intermediate stage of diastolic dysfunction. In included studies, we observed a trend toward a lower E/A ratio in the IBD population, meeting statistical significance (p = 0.04). We also observed a trend toward higher values of E/e′ ratios (p < 0.00001), with values in the IBD population of 950 and 9.5. 63 A significant decrease in the E/A ratio in IBD patients likely reflects early-stage diastolic dysfunction (impaired relaxation). A significant increase in the E/e′ ratio in the studied IBD population may indicate impaired relaxation of the left ventricle. Of note, the larger the E wave and the higher the E/e′ ratio, the higher LV pressures and worse diastolic function. In the statistical analysis, we obtained high heterogeneity (87% for E/A and 80% for E/e′ analysis). This could be explained by differences in the study protocol, population characteristics, or other possible factors that can also influence the results and their interpretation.
Multiple studies demonstrated changes in LV diastolic function in IBD patients compared to healthy non-IBD patients, even in young patients and those without traditional CV risk factors. This was shown through echocardiographic parameters such as reduced E/A ratio, prolonged IVRT and deceleration time (DT), and increased E/e′ indicating impaired relaxation and increased filling pressures.50,52,57,65 Some evidence of subtle systolic dysfunction in IBD patients was also found when measured by more sensitive echocardiographic techniques like 2D speckle tracking strain imaging.54,57,58,63 Reduced GLS was commonly reported and correlated with disease activity scores in some studies.54,58 Though LV dysfunction was subclinical in most patients, even small changes in parameters like GLS are associated with worse outcomes like HF and mortality.65,66,67 Although statistically significant differences were observed between groups in these parameters, the data should be interpreted with consideration of multiple parameters. Most of the differences remained within the normal range.
Left atrium dimensions (diameter and area) were not statistically significantly different between the included studies in our meta-analysis. Of note, all mean values were within the normal range. Increased LA dimensions are associated with chronic elevated LV filling pressures and serve as a marker for diastolic dysfunction and atrial remodeling. Nowadays, the most accurate LA dimension parameter measured by echocardiogram is LA volume, acquired by disk summation algorithm. LA volume has a stronger association with CV outcomes. This measurement is also included in diastolic function algorithms. We may hypothesize that LA dilatation could be associated with chronic exposure to inflammation and uncontrolled IBD burden and so may be mitigated by appropriate disease activity control.
In the included studies in the systematic review, we have also explored the impact of vascular changes in IBD patients and its CV consequences. We observed that increased aortic stiffness was demonstrated to be associated with LV diastolic dysfunction, worse CV outcomes, and mortality. 68 Coronary microvascular dysfunction obtained by echocardiography measures of coronary flow reserve was validated over 30 years ago and is associated with a worse prognosis even in patients with non-obstructive coronary disease.69–71 Reduced coronary flow contributes to LV dysfunction and was positively associated with inflammation markers in some studies. These vascular changes may be due to endothelial dysfunction and low-grade inflammation from IBD. This may likely increase the risk for atherogenesis and coronary disease in the long term. 72
A few studies demonstrated increased AEMD in IBD patients, indicating impaired atrial conduction and this was also associated with inflammation. 42 Given this impaired conduction (prolonged intra- and inter-AEMD), it may indicate underlying electromechanical atrial dysfunction, a known risk factor for AF. Some studies propose that IBD may increase AF risk through inflammatory and structural atrial changes. One study found that IBD-associated inflammation had a stronger effect on AF development, even in younger patients and those without CV risk factors. 73
Large cohort studies consistently showed an increased risk of hospitalization for HF in IBD populations compared to the general population. The risk was higher during periods of active inflammation. In some studies, the overall HF risk was higher in UC patients compared to CD. Younger onset IBD and extensive colitis also had higher risks. The studies propose that uncontrolled inflammation is one factor contributing to a higher risk of HF. However, surveillance bias may also play a role.
One intriguing finding from our review was the transient rise in NT-proBNP levels following the administration of infliximab. This could suggest a possible acute deleterious effect of infliximab on cardiac function. Potential explanations range from the drug’s cytotoxic effects to induced volume overload. However, this study also found that long-term treatment with TNF-alpha blockers, including infliximab, did not seem to induce a lasting deterioration of cardiac function, hinting at a possible short-term impact rather than a prolonged adverse CV effect. This study, however, had a small sample size. Larger longitudinal studies are needed to clarify the relationship between IBD disease activity, inflammation levels, myocardial stress, and NT-proBNP kinetics. Despite this, anti-TNF therapy was not clearly linked with increased HF risk.
A few studies found that corticosteroid use increased the risk of HF in IBD patients, possibly due to effects on recovery from cardiac injury. Furthermore, some small interventional studies showed improvements in LV function or strain after treating inflammation with immunosuppression, suggesting a beneficial cardiac effect. The use of systemic corticotherapy, due to its mechanism of action, contributes to water and sodium retention, especially when in high doses, which can precipitate HF decompensation in susceptible individuals.3,74 Corticosteroid use is also associated with increased incidence of hypertension and dyslipidemia which are known risk factors for CV disease and specifically HF.75,76
These associations might be explained through the cumulative effect of inflammation, fibrosis, collagen deposition, endothelial dysfunction, toxicity from drug therapy, and malnutrition. There is a potential effect of vitamin deficit, mainly selenium, on cardiac health.
Importantly, these changes are detectable even in the absence of overt cardiac disease, implying that routine cardiac monitoring might be beneficial in this patient population, particularly those with long-standing or severe disease.
Limitations and strengths of the study
Some limitations of our study are the small sample size and observational nature of the studies which can introduce some selection biases. The lack of longitudinal follow-up in some of the included studies limits the ability to draw firm conclusions about the direction of causality and long-term outcomes. Heterogeneity was particularly high in the analysis of E/A and E/e′ measurements. The high heterogeneity in E/A meta-analysis (I2 = 87%) was not reduced by sensitivity analysis. The ability to thoroughly explore this degree of heterogeneity was limited by the small number of studies included in the pooled analysis. It could be attributed to intra- and inter-study heterogeneity, resulting from differences between patient groups’ characteristics. In addition, differences may exist in echocardiographic study protocols between centers as also as distinct echocardiography techniques and modes might have been used. These limitations may reduce the validity of the data. Furthermore, the absence of blinding in certain studies introduces the possibility of measurement bias.
Future studies should aim to investigate whether IBD contributes independently to cardiac dysfunction or acts through interactions with other CV risk factors.
The strengths of our article are the rigorous systematic review methodology, the evaluation of included articles bias using standardized tools, the evaluation of multiple topics on the relation between IBD and cardiac disease, and the inclusion of several studies with diverse patient populations.
In summary, from the findings of our systematic review and meta-analysis, there is significant evidence to conclude that the IBD population has an increased risk for mostly subclinical LV and atrial dysfunction, vascular changes, arrhythmias, and HF hospitalization. Screening with sensitive imaging like speckle tracking echocardiography could identify early subclinical changes. IBD is in fact a CV risk factor and tight inflammation control may reduce the risk.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241299534 – Supplemental material for Inflammatory bowel disease and cardiac function: a systematic review of literature with meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848241299534 for Inflammatory bowel disease and cardiac function: a systematic review of literature with meta-analysis by Caroline Almeida Soares, João Gouveia Fiuza, Cláudio André Melo Rodrigues, Nuno Craveiro, Júlio Gil Pereira, Paula Cristina Ribeiro Fernandes Sousa, Diana Catarina Pinto Martins, Eugénia Maria Cancela and Maria Paula Ministro dos Santos in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
None.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.