
Abstract
Objectives:
Stenting of the malignant hilar biliary obstruction (MHBO) area for bile drainage is challenging. Bilateral stenting techniques of stent-in-stent (SIS) and stent-by-stent (SBS) have shown promising results. This study evaluates the efficacy of different stenting methods for MHBO.
Design:
A meta-analysis was performed to determine the efficacy of SIS and SBS stenting strategies for MHBO.
Data sources and methods:
Medical databases such as PubMed, Web of Science, Embase, and Scopus, were searched up to August 2023. We selected eligible studies reporting the data on technical and clinical success, adverse events, and incidence of re-obstruction (RO) of SBS and SIS groups in MHBO patients. We compared the outcomes of SBS and SIS groups.
Results:
A total of 9 studies comparing the data of 545 patients (268 in the SBS group and 277 in the SIS stenting group) were analyzed. There was no significant difference (p > 0.05) in the odds ratio (OR) of Re-obstruction (RO) 0.87 (95% confidence interval (95% CI) 0.6–1.25), technical success 0.58 (95% CI 0.16–2.11), clinical success 1.13 (95% CI 0.62–2.07), and adverse events 1.53 (95% CI 0.88–2.64). The mean difference in procedure time was −12.25 min (95% CI −18.39, −6.12), and the hazard ratio of stent patency was 1.22 (95% CI 1.01–1.47), favoring SBS, with high heterogeneity (I2 = 94%). There was no significant difference in HR for survival 1.05 (95% CI 0.95–1.16) with high heterogeneity (I2 = 84%).
Conclusion:
Compared with SIS, SBS showed better stent patency with comparable technical and clinical success and adverse events.
Prospero registration:
The registration number for this study on PROSPERO is CRD42024523230.
Introduction
Patients with primary or metastatic hepatobiliary tumors, are at risk of developing malignant hilar biliary obstruction (MHBO).1–4 Palliative care is the primary therapeutic option for a majority of patients with MHBO, as approximately 80% of patients diagnosed with MHBO are not eligible for surgical interventions. 5 Effective biliary drainage is crucial for improving the quality of life of patients with MHBO.6,7 Endoscopic biliary drainage (EBD) and percutaneous drainage are the methods for restoring proper bile flow in advanced MHBO, but EBD is preferred because of better outcomes.8,9 In EBD, metal stent placement is preferred over plastic stents due to superior outcomes and increased safety.5,10–12
There are two methods of performing endoscopic bilateral metal stenting: stent-by-stent (SBS) and stent-in-stent (SIS).13–17 Although SIS is more complex than SBS, it enhances physiological drainage by inserting the second stent through the central wire mesh of the first stent. The bilateral insertion of two stents in parallel, known as SBS, is a simpler procedure compared to SIS. Numerous studies have demonstrated the efficacy of bilateral deployment methods using metal stents. 18 Some studies support SBS, while others support SIS. 19 So it is difficult to recommend a method with better outcomes. A meta-analysis is the most effective approach for comparing the safety and efficacy of two stent deployment methods in order to determine the optimal procedure for biliary drainage in MHBO. Previous meta-analyses have included single-arm studies or few limited studies.20–22 So there is need for meta-analysis with updated data. Using recent studies that compare the outcomes of SBS and SIS, we conducted this meta-analysis.
This meta-analysis compares the safety and efficacy of SBS and SIS bilateral metal stenting for bile drainage in MHBO patients.
Materials and methods
This study is conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.23,24
Search strategy
We performed an extensive search of medical databases, such as PubMed, Web of Science, Embase, and the Cochrane Library. The search terms used were “metal stent,” “stent-in-stent,” “stent-by-stent,” “cholangiocarcinoma,” and “malignant hilar obstruction” and their different combinations. The search was concluded in August 2023. The relevant studies were collected by two authors, and conflicts were resolved via discussion.
Studies selection
Studies were included and excluded according to the following criteria.
Inclusion criteria
(1) Studies comparing the efficacy of SBS to SIS bilateral metal stenting.
(2) Studies conducted on MHBO patients.
(3) Human studies published in English.
Exclusion criteria
(1) Letters, reviews, abstracts, single-arm studies, and case reports were not included.
(2) Animal studies or published in other languages.
(3) Studies with incomplete outcomes or missing required outcomes.
(4) Studies with plastic stents.
Data extraction
Study inclusion and exclusion criteria were used to make decisions regarding the selection of studies. Two authors extracted data from the chosen studies. From each study, we retrieved data regarding the year of publication, the country, the study design, the patient count, the type of obstruction, the treatment method, the procedure approach, the technical and clinical success, stent dysfunction or obstruction, overall survival, stent patency, procedure time, and adverse events. Each study consists of two groups: the SBS group and the SIS group.
Outcome and definitions
The primary outcomes of our study include the odds ratio (OR) for stent re-obstruction (RO), which is defined as the number of cases of stent obstruction observed during the follow-up period. Secondary outcomes involve technical and clinical success, which are defined as follows: technical success refers to the successful deployment of the stents and drainage of bile, while clinical success is defined as a reduction in total bilirubin levels by up to 30%–50% within a period of 2–4 weeks following stenting. We also calculated the pooled hazard ratio (HR) for survival time, which includes the time to stenting and follow-up or death, as well as stent patency, which includes the time to stenting and obstruction or death. The pooled mean difference in procedure time refers to the duration required for the deployment of the stent. OR for the occurrence of adverse events, including cholangitis, cholecystitis, liver abscess, and pancreatitis, was also determined.
Statistical analyses
Statistical analysis was conducted using Review Manager (Rev Man 5.4, The Cochrane Collaboration, 2020). The Mantel–Haenszel methodology, using a random effect model, was used to calculate ORs and 95% confidence intervals (95% CIs) for dichotomous variables. As the included studies did not report the HR, we estimated the HR using Kaplan–Meier curves for time-to-event outcomes.25,26 The inverse variance method was employed to calculate the pooled HR for overall survival and stent patency using the random-effects model. The continuous variance method was used to calculate pooled mean differences. Statistical heterogeneity was assessed using Cochrane’s Chi-square (χ2) and I2 statistics. Values of 25%, 50%, and 75% correspond to low, moderate, and high levels of heterogeneity, respectively. 27 p-Value of less than 0.05 was considered a significant difference.
Risk of bias
We employed Cochrane risk of bias assessment tools to evaluate the risk of bias. 28 A study with a low risk of bias was given a grade of “low,” while a study with a moderate risk of bias or insufficient information resulted in a grade of “some concern.” A higher risk of bias was assigned a grade of “high.” 29 We used a funnel plot to detect publication bias. The data from the funnel plot exhibited a symmetrical distribution, suggesting the absence of any bias in the publication of research findings. 30 The impact of each study on the overall outcome was assessed by systematically removing each study and analyzing the resulting changes in the overall result.
Results
Characteristics of included studies
A total of 805 articles were retrieved from medical databases and other resources. After reviewing the topics and abstracts to eliminate duplicate and irrelevant studies, we assessed the eligibility of 152 articles for inclusion. Based on defined criteria for inclusion and exclusion, a total of nine studies were finally included in this meta-analysis (Figure 1). Among the nine studies included, eight were conducted retrospectively,4,8,12,31–35 while one was a randomized controlled trial (RCT). 5 Eight studies used the endoscopic method, while one study used the percutaneous method. A total of five studies were conducted in Japan, while two studies were conducted in Korea and there was one study conducted in both the USA and China. Among the 9 studies analyzed, 268 patients underwent bilateral SBS metal stenting, while 277 patients underwent SIS stenting. One study compared hybrid (combined SBS and SIS) 35 and SIS, but for our analysis, we consider hybrid as SBS outcomes. There were three studies that included patients with Bismuth type I–IV, three studies with patients having Bismuth type II–IV, two studies with patients having Bismuth type III–IV, and one study with patients having Bismuth type I–III. The tables present the raw data regarding the outcomes of the treatment (Tables 1 and 2). The RCT demonstrates a low risk of bias, while the other eight studies suggest a moderate risk of bias. The outcomes showed symmetrical funnel plots, which demonstrated that there was no publication bias and that no study had a greater study impact on the final outcome.

Flow chart of studies selection for this meta-analysis.
Characteristics of included studies.
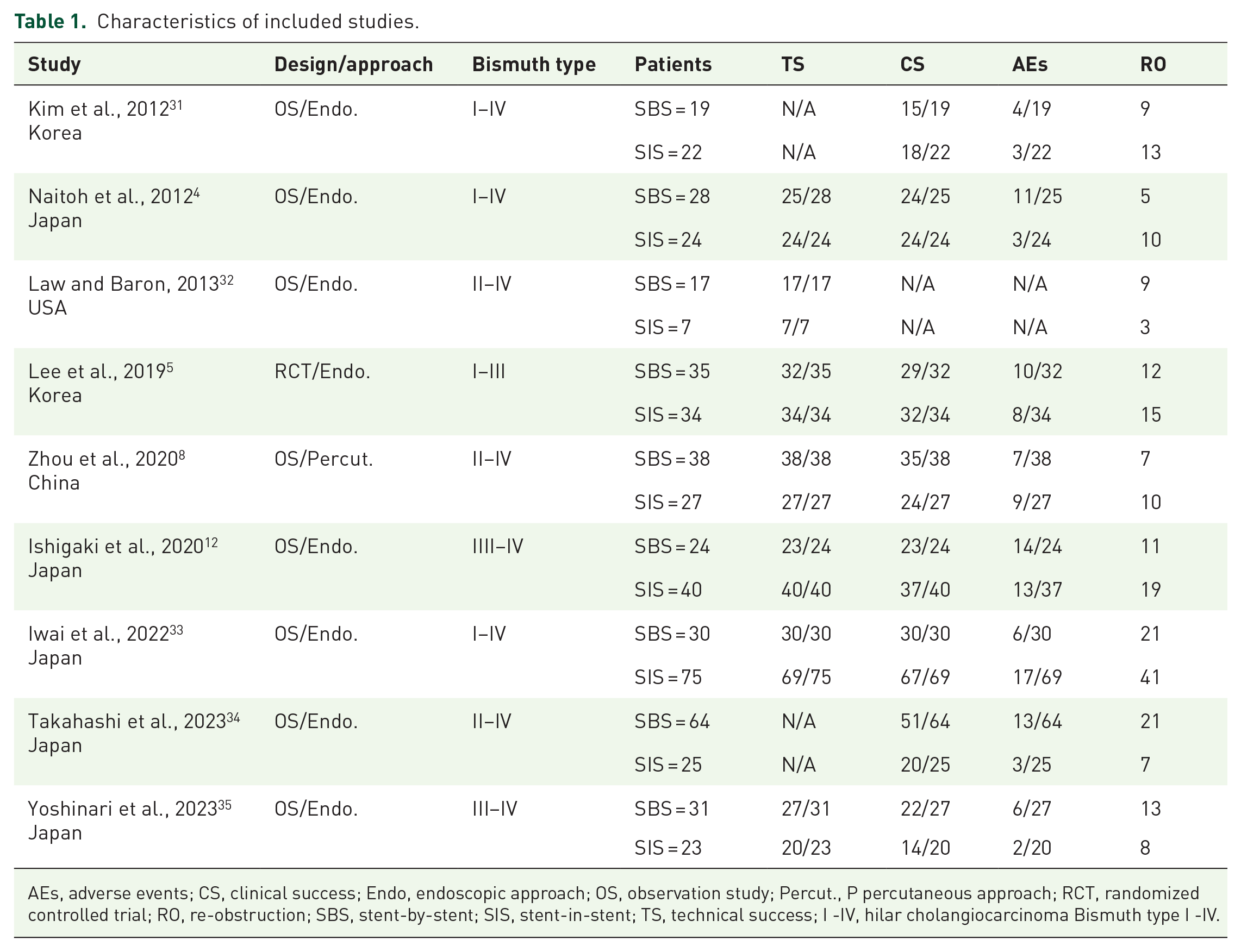
AEs, adverse events; CS, clinical success; Endo, endoscopic approach; OS, observation study; Percut., P percutaneous approach; RCT, randomized controlled trial; RO, re-obstruction; SBS, stent-by-stent; SIS, stent-in-stent; TS, technical success; I -IV, hilar cholangiocarcinoma Bismuth type I -IV.
Characteristics of included studies.

Cholang., cholangitis; Cholecys., cholecystitis; Liver abs., liver abscess; NA, not available; OS, overall survival; Pancreat., pancreatitis; Pro. Time, procedure time; SBS, stent-by-stent; SIS, stent-in-stent; SP, stent patency.
Primary outcome
Re-obstruction
All nine studies included in the meta-analysis reported incidents of RO. The OR for RO was 0.87 (95% CI 0.6–1.25, p = 0.44), indicating no statistically significant difference between the two groups. Additionally, there was no heterogeneity observed between the groups (I2 = 0%) (Figure 2(a)).
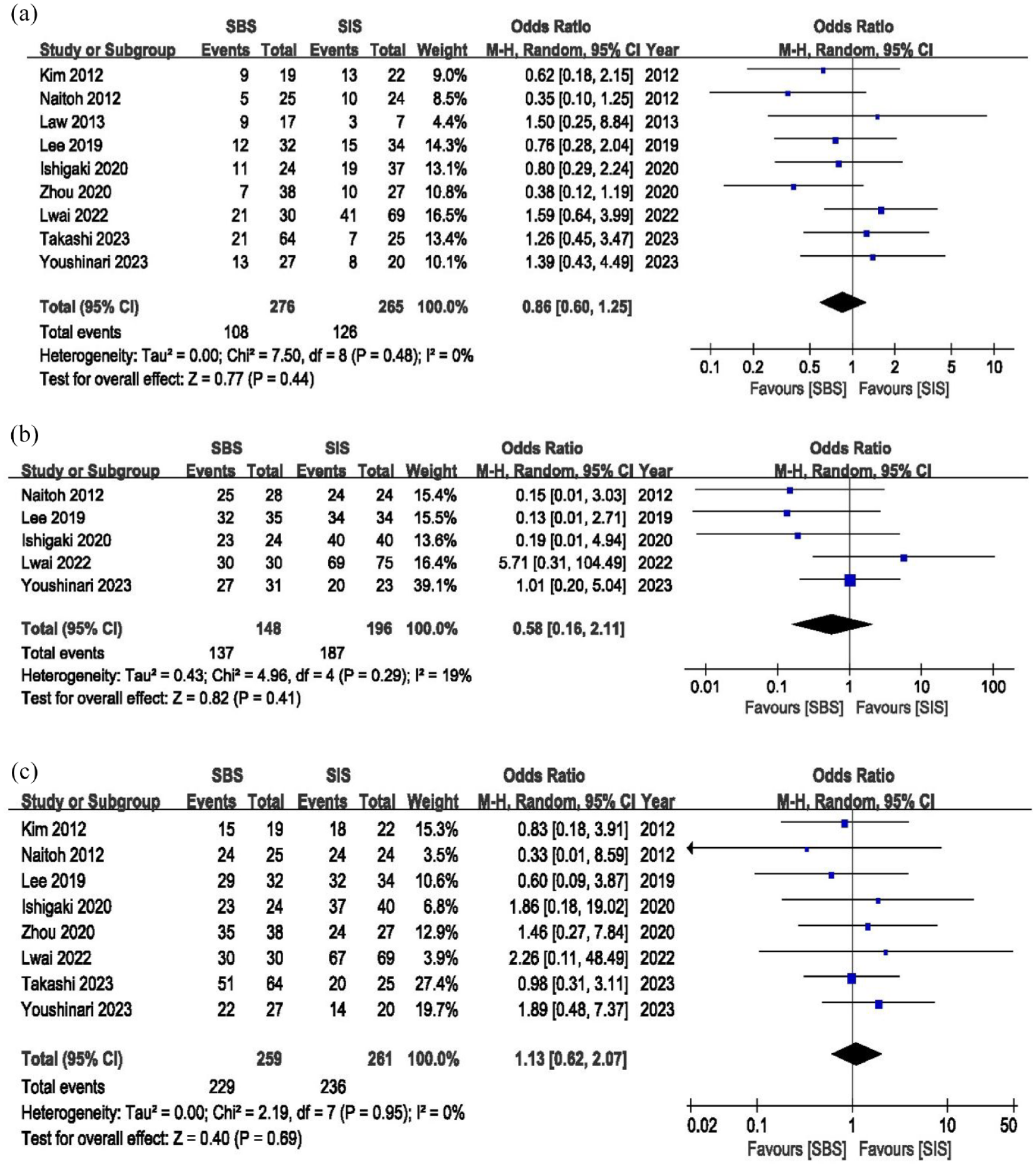
Forest plot of (a) re-obstruction; (b) technical success; and (c) clinical success.
Secondary outcomes
Technical success
Two of the studies did not report technical success, whereas the other two trials had 100% success. Therefore, five studies were included in the OR calculation, and the results showed that the OR was 0.58 (95% CI: 0.16–2.11). There was no significant heterogeneity (I2 = 19%), and there was no statistically significant difference between the two groups (p = 0.41) (Figure 2(b)).
Clinical success
Eight included studies reported data on clinical success. There was no significant difference in OR between the two groups (1.13, 95% CI: 0.62–2.07, p = 0.69). There was no heterogeneity in the results between the two groups (I2 = 0%) (Figure 2(c)).
Overall adverse events
Incidents of adverse events were reported in eight studies. We combined early and late complications as overall adverse events. The overall adverse events between the two groups had an OR of 1.53 (95% CI 0.88–2.64), with no significant difference and low heterogeneity (p = 0.13, I2 = 19%) (Figure 3(a)).

Forest plot of (a) overall adverse events; (b) pancreatitis; (c) cholangitis; and (d) cholecystitis.
Pancreatitis
Five studies reported incidents of pancreatitis after stenting. The OR for pancreatitis was 2.58 (95% CI 0.57–11.67), I2 = 34%, and p = 0.22. The results revealed moderate heterogeneity and no statistically significant difference in the incidence of pancreatitis between the SBS and SIS groups (Figure 3(b)).
Cholangitis
There were six studies that reported cases of cholangitis, and the OR between the SBS and SIS groups for cholangitis was 0.96 (95% CI: 0.41–2.25), I2 = 34%, and p = 0.92. This demonstrates that there is no significant difference in the number of cases of cholangitis between the two groups and a moderate degree of heterogeneity (Figure 3(c)).
Cholecystitis
Six studies presented cholecystitis data, and the OR between the SBS and SIS groups was 1.85 (95% CI 0.83–4.12), I2 = 0%, and p = 0.13. There is no significant difference in cholecystitis incidence between the two groups, and there is no heterogeneity (Figure 3(d)).
Liver abscess
For the purpose of estimating the OR of liver abscess between the two groups, data from seven studies was used. The findings revealed an OR of 0.75 (95% CI 0.27–2.06) with no heterogeneity and no statistically significant difference between the two groups (I2 = 05, p = 0.58) (Figure 4(a)).

Forest plot of (a) liver abscess; (b) procedure time; (c) stent patency; and (d) overall survival.
Procedure time
Only five studies reported the procedure time of the SBS and SIS stenting groups. A significant pooled mean difference of −12.25 min (95% CI −18.39, −6.12), I2 = 82%, and p = 0.00 was found between the two groups. The results indicated that SBS stenting required comparatively less time than SIS stenting. However, there was high heterogeneity in the results between the groups (Figure 4(b)).
Stent patency
Eight studies have reported the Kaplan–Meier graph of stent patency for SBS and SIS stenting. The pooled HR for stent patency was 1.22 (95% CI 1.01–1.47, p = 0.04), indicating a significant difference in favor of SIS stenting with improved stent patency. However, there is high heterogeneity (I2 = 94%). However, sensitivity analysis was not able to find the cause of this heterogeneity (Figure 4(c)).
Overall survival
Only five studies reported the Kaplan–Meier graph for overall survival time. The pooled HR for overall survival was 1.05 (95% CI 0.95–1.16, p = 0.33), demonstrating that there was no significant difference in overall survival time between the two groups. There was also a significant level of heterogeneity (I2 = 83%). However, the sensitivity analysis was unable to identify the factor that was responsible for this heterogeneity (Figure 4(d)).
Discussion
This meta-analysis of nine included studies compared the safety and efficacy of SIS and SBS for MHBO. Except for procedure time and stent patency, there was no significant difference in technical success, clinical success, total adverse events, and overall survival between the two groups (p > 0.05). Mean procedure time was significantly shorter for SBS stenting group and pooled HR of stent patency was also in the favor of SBS stenting group (p < 0.05). Out of eight studies reporting stent patency time, six studies reported comparatively higher stent patency time for the SBS group as compared to SIS group in the graph. Only two studies reported better stent patency for the SIS group.
Managing metal stenting in patients with MHBO is consistently difficult due to a lack of knowledge on the most effective draining technique. 1 Multiple meta-analyses have compared the effectiveness of unilateral and bilateral stenting for MHBO.2,3,36,37 These analyses have shown that unilateral stenting achieves similar functional success and long-term patency compared to bilateral stenting. In particular, unilateral stenting has been found to be more effective for patients with Bismuth III–IV MHBO. Performing bilateral stenting in patients with MHBO to drain at least 50% of the liver volume can significantly improve clinical outcomes. However, the existence of various technical challenges linked to bilateral stenting might limit its application. The overall success rate for SIS and SBS procedures can range from 73.3% to 100%.1,38,39 In the SBS technique, the procedure of placing two stents simultaneously using an endoscopic approach can be quite challenging. The SIS technique allows for the placement of a stent in either the left or right intrahepatic biliary system, followed by the placement of another stent in the opposite bile channel by passing through the mesh of the first stent. Selecting the process that would produce the best outcomes might be challenging because each has advantages and disadvantages of its own. To determine the optimal technique for biliary drainage in MHBO, a meta-analysis can be used to compare the safety and efficacy of two different stent placement strategies.
Previously published meta-analyses that used the data of only three studies to calculate OR have shown that OR for technical success was significantly in favor of the SIS group with no heterogeneity.20–22 Our meta-analysis, including data from five studies, revealed that there was no statistically significant difference in the OR of technical success, with low heterogeneity (p = 0.41, I2 = 19%). Among the nine studies included, two reported a 100% technical success rate for both groups. A recent meta-analysis of seven studies showed that there was significant difference in the OR of the complication rate between the two groups (p = 0.04) but our analysis of nine studies showed no difference in overall adverse events in the SIS and SBS groups. 21 The results of a previous meta-analysis demonstrated that the pooled HR of stent patency was considerably favorable to the SBS group (p = 0.01). Our research also discovered that the pooled HR for stent patency showed a significant difference in favor of SBS stenting with enhanced stent patency (p = 0.04). However, as previously published meta-analyses, there is a high degree of heterogeneity (I2 = 94%), and we were unable to determine the reason for this heterogeneity. Our analysis found that heterogeneity may arise from differences in the values of effects, the extent of overlap in CIs, as well as shifts in study weights. It is worth mentioning that out of all the research conducted, only two studies, Kim et al. and Youshinari et al., showed HRs that were less than 1. On the other hand, all the remaining studies found HRs above 1. After removing these two trials, the combined HR was 1.38 (95% CI 1.12–1.69). After removing studies with different results, there was an HR of 1.479 (95% CI 1.22–1.77) with 86% heterogeneity. After removing one study in the percutaneous approach, it showed an HR of 1.18 (95% CI 0.97–1.43) with 94% heterogeneity. Similarly, after removing studies with Bismuth type 3–4 MHBO, there was an HR of 1.33 (95% CI 1.04–1.69) with 94% heterogeneity, and after removing studies published before 2020, an HR of 1.17 (95% CI 0.90–1.52) with 91% heterogeneity was found. The pooled HR of the overall survival shows no significant difference between the groups. This may be related to the majority of patients in studies who underwent stenting as a postoperative anti-cancer treatment. Stenting has been found to alleviate jaundice, although it does not directly impact the primary tumor. Further anti-cancer treatments are necessary to significantly enhance patient survival and stent patency. Although SBS stent insertion provides dual drainage routes, and our study demonstrates its advantages of procedure time and stent patency, due to imbalances in the Bismuth classification, there is still need for more randomized trials to draw a definite conclusion with same type of hilar obstructions.
There was no significant difference in the OR of the RO in our study that is same as published by the prior studies.20,21 A recently published study involving 89 patients revealed that there was no statistically significant difference in the success ratio, complication rates, and rate of RO between the two groups. 34 Another study of 51 patients showed that SIS bilateral stenting of MHBO can be an efficient approach with better outcomes. 13 There was no statistically significant difference between the two groups in terms of technical and clinical efficacy, complications, or recurring biliary obstruction in the study of 105 patients. However, there was a big difference between the groups in the success rate of re-sending plastic stents through metal stents, with SBS stenting having greater success rates. 33 Both the hybrid (SBS + SIS) and the SIS stenting procedures were shown to have comparable results, with no significant differences between them, in a recent study that compared the two procedures involving 54 patients. 35
According to the findings of our analysis, the OR of adverse events did not demonstrate a significant difference between the two groups in terms of the incidence of pancreatitis, cholangitis, cholecystitis, or liver abscess (p > 0.05). According to the findings of a meta-analysis that included seven studies, the pooled early-complication rate was significantly lower for SBS groups than for SIS groups (p = 0.04). 21 In our study, we did not differentiate early or late adverse events and calculated them as overall adverse events. Other studies that were published in the past found that there was no significant difference in the number of incidences of adverse events that occurred between the SBS group and the SIS group.5,8,12,22,35 These adverse events can be prevented by employing sound expertise and taking appropriate precautions.
When it comes to dealing with advanced MHBO, the SIS technique and the SBS technique both have their own set of benefits and drawbacks that are unique to them. The preferences and levels of experience of the endoscopists may play a role in the decision on which type of deployment to use. According to the findings of this study, both methods had comparable levels of technical feasibility as well as rates of adverse events and RO. On the other hand, there aren’t enough patients to do comprehensive comparison studies due to the disease’s prevalence and poor prognosis. Recent RCTs have shown that both treatment options are equally effective in terms of technical as well as clinical success, stent patency, and the occurrence of adverse events. Even though these differences were not statistically significant, it is important to note that the SIS group displayed slightly higher rates of stent patency at both 3 and 6 months. 5 Another RCT also showed that there was no significant impact of additional radiofrequency ablation with stenting and stenting alone as an addition to SIS and SBS stenting for MHBO patients and both groups experienced same number of RO, clinical, and technical success rates. 40
Several limitations that indicate interesting directions for further research have been found in our meta-analysis. First, selection bias may have been introduced because most of the studies in our study were retrospective. Future RCTs are essential to offer more solid evidence. Second, the variations in stent implantation techniques may have an impact on the results. In the future, standardizing these processes can improve the evidence’s quality. Furthermore, certain outcomes exhibited heterogeneity in their results. It is important to keep this in mind when interpreting these findings. Finally, the fact that MHBO patients with different Bismuth types of MHBO were included in these studies may have limited the generality of our results. For a deeper understanding, more research is required to focus on particular Bismuth-type subtypes.
Conclusion
Although SBS and SIS stenting provided comparable outcomes in terms of technical and clinical success, adverse events, and survival time for bilateral stenting of MHBO, SBS achieved longer patency and shorter procedure duration.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241271962 – Supplemental material for Safety and efficacy of side-by-side versus stent-in-stent stenting for malignant hilar biliary obstruction: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848241271962 for Safety and efficacy of side-by-side versus stent-in-stent stenting for malignant hilar biliary obstruction: a systematic review and meta-analysis by Haibin Zhou, Hayat Khizar, Ashraf Ali and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848241271962 – Supplemental material for Safety and efficacy of side-by-side versus stent-in-stent stenting for malignant hilar biliary obstruction: a systematic review and meta-analysis
Supplemental material, sj-docx-2-tag-10.1177_17562848241271962 for Safety and efficacy of side-by-side versus stent-in-stent stenting for malignant hilar biliary obstruction: a systematic review and meta-analysis by Haibin Zhou, Hayat Khizar, Ashraf Ali and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.