
Abstract
Background:
Recently, several novel programmed cell death protein 1 (PD-1) inhibitors have been approved for second-line treating advanced or metastatic oesophageal squamous cell carcinoma (OSCC), including camrelizumab, nivolumab, pembrolizumab, sintilimab and tislelizumab. However, the optimal treatment regimen remained ambiguous.
Objectives:
The purpose of this study was to investigate the efficacy, safety and economy of available PD-1 inhibitors to determine the optimal treatment from the Chinese healthcare system perspective.
Design:
A systematic review and economic evaluation.
Data sources and methods:
A systematic review was undertaken utilizing PubMed, Web of Science, Cochrane Library, Embase and Scopus databases to identify eligible studies until 31 August 2023. Primary outcomes were progression-free survival (PFS), overall survival (OS) and adverse events (AEs). We also developed a partitioned survival model at 3-week intervals based on five clinical trials to predict long-term costs, quality-adjusted life-years (QALYs) and incremental cost-effectiveness ratios for various treatment options. Direct medical costs and utility values were obtained from public drug bidding databases, clinical trials or published literature. The parameter uncertainties within the model were determined via one-way and probabilistic sensitivity analyses.
Results:
Five randomized controlled trials involving 2837 patients were included in the analysis. Compared with other treatments examined, camrelizumab provided the best PFS benefits [hazard ratio (HR): 0.69, 95% confidence interval (CI): 0.56–0.86], and pembrolizumab provided the best OS benefits (HR: 0.55, 95% CI: 0.37–0.82). Nivolumab caused a relatively lower incidence of treatment-related AEs (HR: 0.10, 95% CI: 0.05–0.20) and grade 3–5 AEs (HR: 0.13, 95% CI: 0.08–0.21) than other immunotherapy regimens. In the economic evaluation, average 10-year costs ranged from $5,433.86 (chemotherapy) to $50,617.95 (nivolumab) and mean QALYs ranged from 0.55 (chemotherapy) to 0.82 (camrelizumab). Pembrolizumab was eliminated because of dominance. Of the remaining strategies, when the willingness-to-pay thresholds were 1, 2 and 3 times GDP per capita in 2022, sintilimab, tislelizumab and camrelizumab were the most cost-effective treatment options, respectively.
Conclusion:
Sintilimab might be the optimal treatment alternative for second-line therapy of advanced OSCC in China, followed by tislelizumab and camrelizumab.
Trial registration:
This study has been registered on the PROSPERO database with the registration number CRD42023495204.
Plain language summary
Background: The purpose of this study was to investigate the efficacy, safety and economy of available PD-1 inhibitors to determine the optimal treatment from the Chinese healthcare system perspective. Methods: A systematic review was undertaken utilizing PubMed, Web of Science, Cochrane Library, Embase, and Scopus databases to identify eligible studies until August 31, 2023. Primary outcomes were progression-free survival (PFS), overall survival (OS), and adverse events (AEs). We also developed a partitioned survival model at 3-week intervals based on 5 clinical trials to predict long-term costs, quality-adjusted life-years (QALYs) and incremental cost-effectiveness ratios (ICERs) for various treatment options. Direct medical costs and utility values were obtained from public drug bidding database, clinical trials or published literatures. The parameter uncertainties within the model were determined via one-way and probabilistic sensitivity analyses. Results: Compared with other treatments examined, camrelizumab provided the best PFS benefits (HR: 0.69, 95% CI: 0.56-0.86), and pembrolizumab provided the best OS benefits (HR: 0.55, 95% CI: 0.37-0.82). Nivolumab caused a relatively lower incidence of treatment-related AEs (HR: 0.10, 95% CI: 0.05-0.20) and grade 3-5 AEs (HR: 0.13, 95% CI: 0.08-0.21) than other immunotherapy regimens. In the economic evaluation, average 10-year costs ranged from $5,433.86 (chemotherapy) to $50,617.95 (nivolumab) and mean QALYs ranged from 0.55 (chemotherapy) to 0.82 (camrelizumab). Pembrolizumab was eliminated because of dominance. Of the remaining strategies, when the willingness-to-pay thresholds were 1, 2, and 3 times GDP per capita in 2022, sintilimab, tislelizumab, and camrelizumab were the most cost-effective treatment options, respectively. Conclusion: Sintilimab might be the optimal treatment alternative for second-line therapy of advanced ESCC in China, followed by tislelizumab and camrelizumab.
Keywords
Introduction
Oesophageal cancer is the fifth most prevalent and the fourth deadliest digestive malignancy in China,1,2 where oesophageal squamous cell carcinoma (OSCC) accounts for approximately 85% of all cases. 3 Fluoropyrimidine or paclitaxel-based chemotherapy is considered the standard first-line treatment regime for advanced or metastatic OSCC patients. 4 However, effective treatment options were extremely limited for first-line resistant or progressive patients, although docetaxel and irinotecan have been applied extensively in clinical practice. 5 Patients were plagued by severe gastrointestinal, haematological and neurological toxicities and poor long-term survival. 6 Therefore, ground-breaking therapeutic options became an urgent priority.
In recent years, several studies have demonstrated that programmed cell death protein 1 (PD-1) or programmed death-ligand 1 (PD-L1) inhibitors exhibit promising anti-tumour activity and manageable safety profiles in the second-line treatment of patients with advanced OSCC.7,8 As a result, camrelizumab, nivolumab, pembrolizumab, sintilimab and tislelizumab were approved by the National Medical Products Administration and recommended by the Guidelines of the Chinese Society of Clinical Oncology (CSCO) 9 based on ESCORT, 10 ATTRACTION-3, 11 KEYNOTE-181, 12 ORIENT-2 13 and RATIONALE-302 14 clinical trials. Following successful government reimbursement negotiations in 2021, camrelizumab has achieved coverage on the National Reimbursement Drug List (NRDL) as the first PD-1 inhibitor for the treatment of locally advanced or metastatic OSCC with disease progression or intolerability after prior first-line chemotherapy. 15 The price reduction negotiated was an impressive 85.2%. Additionally, in 2023, tislelizumab was officially approved as the latest available health insurance-reimbursed medication for second-line treatment of patients with OSCC.
Despite the impressive survival rates associated with immunotherapy, the corresponding economic burden on patients and healthcare systems remains enormous. 16 Meanwhile, there are no structured head-to-head clinical trials simultaneously comparing the superiority of multiple treatment regimens, and no validated predictive molecular biomarkers to assist in choosing a relatively superior treatment option. 17 Accordingly, considering the extremely limited health budgets and rapidly growing pressures, decision-making based on health economic evaluations was warranted. 18 The available evidence suggested that toripalimab plus chemotherapy displayed the best overall survival (OS) advantages and camrelizumab plus chemotherapy showed the best progression-free survival (PFS) advantages in the first-line treatment of advanced OSCC. 19 Our previous economic evaluation revealed that toripalimab plus chemotherapy compared with other PD-1 inhibitors combined with chemotherapy represented the preferred first-line treatment option at current prices and willingness-to-pay (WTP) thresholds in China. 20 For second-line management, the intricate mechanisms of action for OSCC drugs have been extensively investigated in several previous studies.21,22 There is a scarcity of comprehensive economic assessments related to second-line treatment options, which are currently confined solely to comparisons between immunotherapy and chemotherapy.23–25 Consequently, conducting pertinent cost-effectiveness analyses is imperative to properly address the dilemmas of policy formulation and clinical practice. 26
Towards this end, the present study comprehensively evaluated the efficacy and safety of all available immunotherapies for the second-line treatment of advanced OSCC according to the systematic review and network meta-analysis and assessed the cost-effectiveness of treatment regimens from the perspective of the Chinese healthcare system. Our evidence would contribute to clinical management and policy decision-making.
Methods
Present network meta-analysis and economic evaluation were performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 27 and the Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) guideline, 28 respectively (Supplemental Materials). This study was based on systematic reviews and modelling techniques, and it was deemed exempt from institutional review board approval.
Systematic reviews
Study strategy
PubMed, Web of Science, Cochrane Library, Embase and Scopus were systematically searched from inception through 31 August 2023 for relevant randomized controlled trials (RCTs). The search terms were as follows: immunotherapy, immune checkpoint inhibitor, PD-1, PD-L1, chemotherapy, camrelizumab, nivolumab, pembrolizumab, sintilimab, tislelizumab, RCT, oesophageal squamous cell cancer. The detailed search strategy is represented in Supplemental Table S1. Furthermore, bibliographies of included studies and relevant reviews were also manually inspected to identify other eligible literature.
Selection criteria
The study should meet the following inclusion criteria: (1) Patients were aged ⩾18 with histologically or cytologically confirmed advanced or metastatic OSCC, progressed on previous first-line systemic treatment. (2) Phase II/III RCTs comparing the efficacy and safety of immunotherapy versus chemotherapy regimens. (3) RCTs that reported PFS, OS and treatment-related adverse events (AEs). Exclusion criteria were as follows: (1) Abstracts, letters, case reports, reviews or meta-analyses. (2) Unavailability of data or full text.
Data extraction and quality assessment
Two reviewers separately (SL and LD) deleted duplicates, screened literature, extracted information and performed quality assessment. The primary information was extracted from each included publication: trial name, treatment regimens, patient characteristics and outcome indicators. Methodological quality was examined using the Cochrane Collaboration’s risk of bias assessment tool categorized as low, some concerns and high. 29
Statistical analysis
PFS and OS were presented as hazard ratios (HRs) along with 95% confidence intervals (CIs), while treatment-related AEs were expressed as odds ratios and 95% CIs. Heterogeneity across studies was calculated by Cochrane’s Q test and I2 statistic. I2 values >50% indicated substantial heterogeneity, the random-effect models were utilized; otherwise, the fixed-effect models were applied. We employed R software (version 4.2.2) (https://www.r-project.org/) gemtc package to conduct Bayesian network meta-analyses, comparing treatment regimens simultaneously. A two-sided p < 0.05 suggested statistically significant.
Economic evaluation
Model structure
Partitioned survival models have been extensively applied to reimbursement decisions for oncology drugs. 30 Therefore, we constructed a partitioned survival model in which advanced OSCC patients transitioned among three mutually independent health states, namely PFS, progression disease and death (Figure 1). The cycle length was defined as 3 weeks, with a 10-year time horizon, over which 99% of patients were predicted to die. We measured total costs, quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs) between any two treatment regiments. A half-cycle correction was enforced to adjust the head-tail bias of cycles in the analysis. Meanwhile, a 5% annual discount rate was implemented for both costs and health outcomes in line with the ‘China Guidelines for Pharmacoeconomic Evaluations 2020’. 31 All costs were adjusted to US dollars (2022 annual average exchange rate: $1 = ¥6.7261). Based on the recommendations of published studies, health interventions should be considered cost-effective if the ICERs were between 1 and 3 times the gross domestic product (GDP) per capita of that country.32–34 This threshold has been widely used in cost-effectiveness studies within global health. 35 In the present study, a range of WTP thresholds, ranging from $12,039.07 to $36,117.22, were employed to explore the probability that treatment alternatives would be the most cost-effective.

The structure of the partitioned survival model.
Clinical inputs
We assessed six treatment strategies: camrelizumab, nivolumab, pembrolizumab, sintilimab, tislelizumab and chemotherapy (Supplemental Materials). Patients received one of six treatment options until disease progression or unacceptable toxicity. After progression, third-line treatment will be initiated. The PFS and OS curves for patients administered with camrelizumab, nivolumab, pembrolizumab, sintilimab and tislelizumab were obtained directly from ESCORT, 10 ATTRACTION-3,11,36 KEYNOTE-181,12,37 ORIENT-2 13 and RATIONALE-302 14 trials, respectively. To determine survival data for chemotherapy, the average of the above-mentioned clinical trials was calculated. Because the original individual patient data were not available, GetData Graph Digitizer 2.26 (http://www.getdata-graph-digitizer.com/) was used to extract data points, and time-to-event data were obtained based on algorithms proposed by Guyot et al. 38 Subsequently, the best-fit parametric survival models for reconstructed data were selected among Exponential, Weibull, Log-logistic, Log-normal and Gompertz distributions, with clinical plausibility, visual inspection and statistical goodness-of-fit (Akaike information criterion and Bayesian information criterion). 39 More details concerning model fitting are presented in Supplemental Table 2 and Supplemental Figures 1 and 2.
Cost and utility inputs
We considered the costs of implementing each treatment from the perspective of the Chinese healthcare system, including drug acquisition costs, hospitalization expenses, laboratory testing costs, AEs management costs (for AEs ⩾3 grade and ⩾5% incidence), follow-up costs, best supportive care and end-of-life costs. Drug costs were derived from the average bid-winning price announced by YAOZH (www.yaozh.com) in 2023 40 (Supplemental Table 3). Other costs were estimated from published literature,20,25,41–44 and these costs were adjusted with the consumer price index related to health services. To calculate the dosages of chemotherapies, the default body weight of 65.0 kg and body surface area of 1.72 m2 were assumed for Chinese patients. 45 Health state utilities associated with OSCC were unavailable in the included trials; thus, we used those from the RAINBOW trial considering their comparability. 46 The disutility values incurred for treatment-related AEs were obtained from the literature.42,47,48 All model parameters are provided in Table 1.
Key model inputs.

PD, progressed disease; PFS, progression-free survival.
Sensitivity analyses
One-way and probabilistic sensitivity analyses were performed to ascertain the robustness of the model. One-way sensitivity analyses, presented as tornado diagrams, were conducted for all parameters separately, with a variation range of 95% CI or ±20% of the base-case value, to assess the influence of each parameter on ICER. To account for parametric uncertainty within the model, a second-order Monte Carlo simulation with 10,000 iterations was generated by simultaneously random sampling from prespecified statistical distributions. Gamma distributions were used for costs, and beta distributions were used for probabilities, proportions and health state utilities. 49 The results were represented by cost-effectiveness acceptability curves (CEAC).
Results
Network meta-analysis
A total of 654 documents were accessed through database searches. After primary and secondary screening, 7 articles with 2837 trial participants from 5 RCTs were included for further analyses (Supplemental Figure 3 and Supplemental Table 4). The methodologic quality of the included RCTs was provided in Supplemental Figure 4. All RCTs exhibited a high risk of bias in terms of performance but the overall risk of bias remained within an acceptable range. The findings revealed a significant reduction in the risk of mortality with PD-1 inhibitors, while only camrelizumab exhibited superior PFS (HR: 0.69, 95% CI: 0.56–0.86) compared to chemotherapy in patients with OSCC (Figure 2). In terms of safety, compared with chemotherapy, nivolumab, pembrolizumab, sintilimab and tislelizumab significantly reduced treatment-related AEs and grade 3–5 treatment-related AEs (Figure 3).

Hazard ratios and 95% CIs for progression-free survival (green) and overall survival (blue) of the Bayesian network meta-analyses.
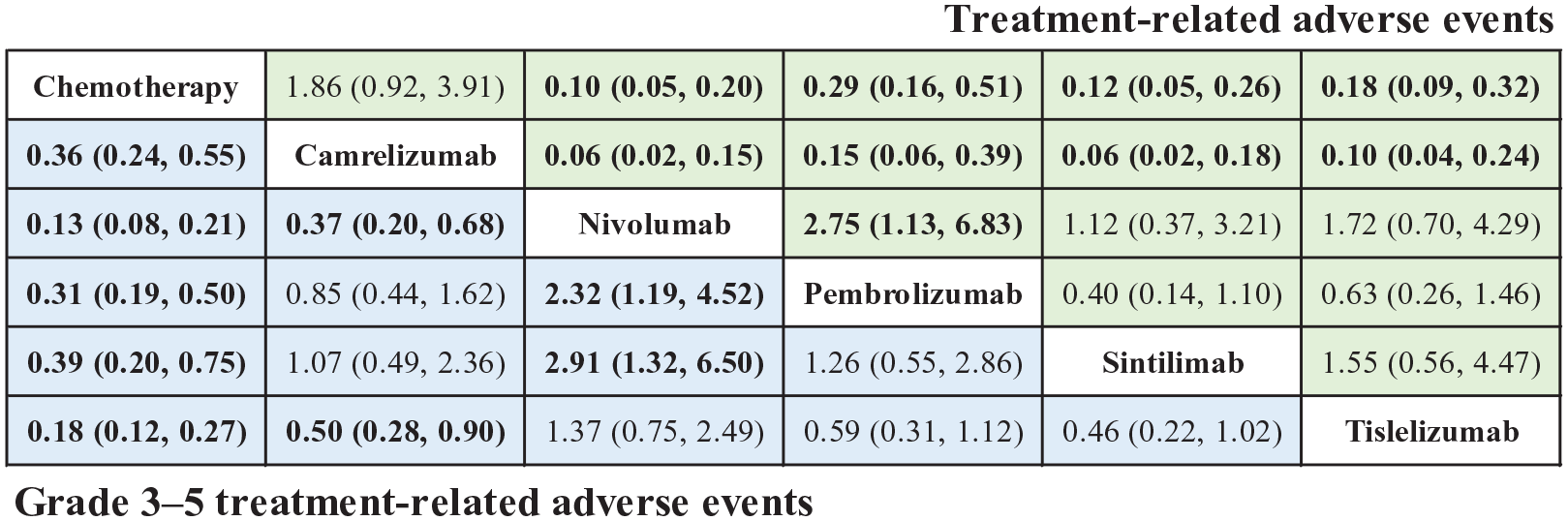
Odds ratios and 95% CIs for treatment-related adverse events (TRAEs) (green) and grade 3–5 TRAEs (blue) of the Bayesian network meta-analyses.
Cost-effectiveness analysis
Base-case results
The base-case results are outlined in Table 2. Compared with chemotherapy, sintilimab, tislelizumab, camrelizumab, pembrolizumab and nivolumab as second-line therapy for OSCC provided incremental costs of $505.46, $1937.58, $3616.87, $35,252.58 and $45,184.09, with additional QALYs of 0.11, 0.22, 0.27, 0.13 and 0.26, respectively, resulting in ICERs of 4724.46$/QALY, 8913.28$/QALY, 13,549.69$/QALY, 269,654.18$/QALY and 170,710.46$/QALY. In pairwise comparisons, sintilimab, tislelizumab and camrelizumab were considered as high-value treatment options when the WTP thresholds were 1, 2 and 3 times GDP per capita, respectively.
Base-case results.
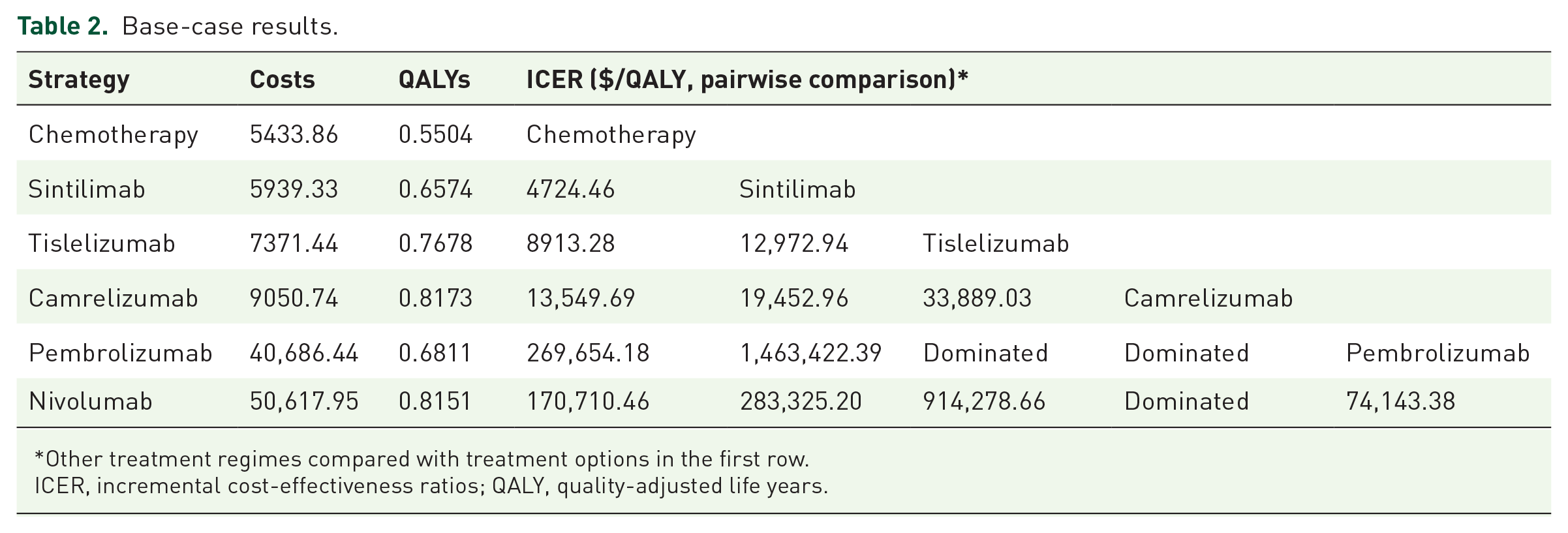
Other treatment regimes compared with treatment options in the first row.
ICER, incremental cost-effectiveness ratios; QALY, quality-adjusted life years.
Sensitivity analysis results
The results of one-way sensitivity analyses indicated that drug costs, utility values, body surface area and discount rate were the most influential parameters within the model (Supplemental Figure 5). The parameters with the greatest impact on the economic evaluation were the prices of PD-1 inhibitors. The best-case ICERs for sintilimab, tislelizumab, camrelizumab, pembrolizumab and nivolumab compared with chemotherapy were 637.85$/QALY, 6112.83$/QALY, 10,016.38$/QALY, 214,131.98$/QALY and 135,855.13$/QALY, respectively; while the worst-case ICERs were 8,811.06$/QALY, 11,713.72$/QALY, 17,083.00$/QALY, 325,176.37$/QALY and 205,565.78$/QALY. Alterations in each parameter did not significantly alter conclusions. At the WTP thresholds of 1 and 3 times GDP per capita in China, the CEAC demonstrated approximately 0.22%, 60.17%, 39.35% and 0.26%, and 0.00%, 0.00%, 41.18% and 58.82% probabilities of chemotherapy, sintilimab, tislelizumab and camrelizumab being the most cost-effective options, respectively. Nevertheless, pembrolizumab and nivolumab might not be the preferred options (Figure 4).

Cost-effectiveness acceptability curves indicating the probability of each treatment regimen being cost-effective as second-line therapy for advanced oesophageal squamous cell carcinoma at various willingness-to-pay thresholds in China.
Discussion
Since 2020, substantial progress has been made in the second-line therapeutic landscape of advanced OSCC beginning with the publication of the ATTRACTION-3 trial. 11 Since then, immunotherapy has re-established a new standard of care for treating advanced OSCC after progression from first-line therapy. 9 This was the first study to synthetically appraise the efficacy, safety and economy of all available second-line PD-1 inhibitors in Chinese advanced OSCC patients. We adopted a healthcare system perspective in China and discovered that sintilimab emerged as the relatively superior treatment strategy, with the most optimal ICER in this trade-off. In addition, we also observed that at a WTP threshold of 1–3 times GDP per capita apart from sintilimab, other PD-1 inhibitors such as tislelizumab and camrelizumab could also be candidates for optimal cost-effective treatment regimes.
For efficacy and safety evaluations, the majority of existing studies have focused on the first-line treatment of advanced OSCC with PD-1 inhibitors in combination with chemotherapy, while comparatively less attention has been given to the second-line treatment. Neoadjuvant immune checkpoint inhibitors plus chemotherapy demonstrated promising efficacy and safety in treating resectable oesophageal cancer and OSCC.7,50,51 The best PFS was generated by sintilimab plus chemotherapy and camrelizumab plus chemotherapy, and the best OS was generated by toripalimab plus chemotherapy.19,52,53 The toxicity of first-line immunotherapy was manageable in OSCC patients.19,52,53 For second-line therapy, Gao et al. 52 found that camrelizumab exhibited optimal PFS, which was consistent with the present study. The present study utilized subgroup survival data specifically from Asian or Chinese populations, rendering the findings more applicable to the characteristics of Chinese patients.
For economic evaluations, compared with imported PD-1 inhibitors, the domestically produced agents (camrelizumab, sintilimab and tislelizumab) displayed relatively superior cost-effectiveness, which was similar to some extent from other published studies. Three studies constructed partitioned survival or Markov models to evaluate the cost-effectiveness of camrelizumab compared to second-line chemotherapy for advanced OSCC based on the ESCORT trial.24,54,55 These studies found that camrelizumab was cost-effective in China. Shi et al. 23 performed an economic evaluation of tislelizumab in second-line treatment for advanced OSCC from the Chinese healthcare payers’ perspective and estimated an ICER of $11,073.85 per QALY gained. These findings were consistent with our study, although the input parameters in these studies were slightly different from ours. Sintilimab was also a potentially valuable immunotherapy, while clinicians and policymakers were uncertain about its cost-effectiveness as a second-line treatment for advanced OSCC. 13 Our economic evaluation provides comprehensive evidence for future policy decision-making, particularly in scenarios where multiple treatment options are available and no biomarkers exist to guide the selection of the preferred option.
In recent years, China has witnessed a dedicated endeavour to enhance the availability and affordability of innovative cancer medications. 56 The National Medical Products Administration has introduced numerous favourable policies to accelerate the development, review and approval of promising anti-cancer drugs. 57 Based on rigorous cost-effectiveness and budget impact analyses, an increasing number of innovative medicines were successfully incorporated into the NRDL through meticulous price negotiations. 15 Drug prices have been reduced by half. 56 Camrelizumab, sintilimab and tislelizumab produced more favourable cost-effectiveness primarily attributed to price-negotiation mechanisms. 15 Considering imported PD-1 inhibitors, previous studies have shown that nivolumab and pembrolizumab might not exhibit cost-effectiveness relative to chemotherapy as second-line treatments for advanced OSCC patients from the perspective of Chinese society, aligning analogously to the findings of the current study.25,58 Nivolumab and pembrolizumab were also unaffordable in other countries, including the United States and Japan. 59 Kashiwa 47 developed a partitioned survival model from the Japanese National Health Insurance payer perspective to forecast costs and outcomes associated with first-line and second-line nivolumab therapy for advanced oesophageal cancer. This study found that nivolumab could be recommended as first-line treatment in combination with chemotherapy but not as second-line monotherapy. 47 Hu et al. 60 demonstrated that, from a third-party public healthcare payer perspective in the United States, pembrolizumab was not an economically advantageous scheme in patients with PD-L1 combined positive score (CPS) ⩽10 OSCC or oesophageal adenocarcinoma.
Tumour-cell PD-L1 expression was significantly enriched in OSCC, with approximately 50% of advanced disease patients exhibiting detectable expression levels of 1% or higher.61,62 Second-line treatment with PD-1 inhibitors exhibited longer OS in advanced OSCC patients with high PD-L1 expression in clinical trials.10–14 Published economic evaluations have also demonstrated that pembrolizumab resulted in superior cost-effectiveness in advance oesophageal carcinoma patients with a PD-L1 CPS ⩾ 10 compared to the total intention-to-treat population.58,60 The most extensively validated predictive biomarker for sensitivity to immune checkpoint inhibitors is PD-L1 expression, as measured by either the CPS or tumour proportion score. 17 Because substantial variations in the identification and definition of PD-L1-positive patients across clinical trials, and the corresponding Kaplan–Meier curves were not reported.10–14 On this basis, economic evaluations associated with different PD-L1 expression levels were not explored in the current study. Although our assessments suggested that sintilimab was the optimal regimen for all advanced OSCC, it might not be advisable to adopt a cost-effective drug for patients with varying levels of PD-L1 expression. 63 Therefore, subgroup analyses based on long-term follow-up or real-world data are needed to better tailor appropriate treatments with regard to individual patient characteristics.
There are some limitations in our study. First, we conducted efficacy and safety evaluations by Bayesian network meta-analyses due to the absence of head-to-head clinical trials. Considering survival data that violated the proportional hazard assumption, the economic evaluation was performed by incorporating naive indirect comparisons. Second, since the CSCO guidelines did not specifically recommend third-line treatment, we presumed that best supportive care predominantly constituted subsequent therapeutic interventions, potentially deviating from realistic diagnostic and therapeutic decision-making. Third, we primarily focused on the costs and disutility values associated with treatment-related AEs of grade ⩾3 and incidence ⩾5%, while inadvertently neglecting grade 1–2 AEs, which might underestimate the overall costs of each treatment option. Fourth, as health state utility values were not reported in the included clinical trials, we obtained the relevant baseline data from the RAINBOW trial; however, it should be noted that these data did not specifically pertain to Chinese populations. Future economic evaluations should be further carried out based on original data of Chinese patients, to provide more precise evidence for clinical and policy decision-making.
Conclusion
The findings of this Bayesian network meta-analyses and economic evaluations indicated that novel PD-1 inhibitors provided significant OS over chemotherapy alone as a second-line treatment of advanced OSCC patients. Among five immunotherapies, sintilimab was the optimal treatment option, followed by tislelizumab and camrelizumab from the Chinese healthcare system’s perspective.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848241233134 – Supplemental material for Immune checkpoint inhibitors versus chemotherapy as second-line therapy for advanced oesophageal squamous cell carcinoma: a systematic review and economic evaluation
Supplemental material, sj-pdf-1-tag-10.1177_17562848241233134 for Immune checkpoint inhibitors versus chemotherapy as second-line therapy for advanced oesophageal squamous cell carcinoma: a systematic review and economic evaluation by Shixian Liu, Lei Dou and Shunping Li in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.