
Abstract
Background:
It is unclear how clinical and endoscopic factors affect the attainment of endoscopic remission (ER) in patients with small bowel Crohn’s disease (SB-CD) who are infliximab-naïve.
Objectives:
We aimed to identify the effect of different factors on attaining ER using double-balloon endoscopy (DBE) evaluation.
Design:
A single-center retrospective observational study was conducted from 1 January 2018 to 30 November 2022. Among 262 patients who were screened for isolated SB-CD by baseline DBE, 108 patients were assessed for effectiveness during maintenance infliximab therapy by a second DBE evaluation.
Methods:
DBE findings before and after infliximab therapy were compared. ER was defined as a simple endoscopic score for CD (SES-CD) below 3, and segmental ER as SES-CD activity of 0. Multivariate regression with calculations of odds ratios (OR) was used to determine the impact of different factors on attaining ER.
Results:
In all, 41 patients (38.0%) achieved ER. An elevated C-reactive protein at week 6 was independently associated with a decreased probability of ER [OR: 0.86, 95% confidence interval (CI) = 0.75–0.98, p = 0.03]. Segmental ER of the terminal ileum, rather than the proximal ileum, was associated with a higher rate of ER (60.9% versus 38.2%, p = 0.01). High baseline SES-CD (⩾16) was unrelated to overall ER. For patients with disease in the terminal ileum, those with moderate/severe disease were less likely to attain segmental ER than those with mild disease [adjusted odds ratios (aOR): 0.27, 95% CI: 0.09–0.83, p = 0.02]. A large ulcer in the terminal ileum was associated with a lower rate of segmental ER (aOR: 0.18, 95% CI: 0.06–0.56, p = 0.01).
Conclusion:
For infliximab-naïve patients with SB-CD, the overall severity of the endoscopic score was unrelated to attainment of ER. Patients were less likely to attain segmental ER if they had greater endoscopic inflammation or larger ulcers in the terminal ileum.
Introduction
Crohn’s disease (CD) is a chronic and progressive inflammatory disease that can affect the upper gastrointestinal tract, small bowel (SB), colon, and perianal region. The main therapeutic goal is deep remission. The standard definition of deep remission is the resolution of symptoms and endoscopic inflammation, including endoscopic remission (ER) and mucosal healing (MH). 1
About 30% of patients with CD have a disease confined to the SB. 2 For these patients, it is crucial to thoroughly examine the SB for the accurate assessment of ER. However, most examinations rely upon ileocolonoscopy, and this approach may miss SB lesions because the disease may not be present in the terminal ileum. 3 Balloon-assisted endoscopy (BAE), such as double-balloon endoscopy (DBE), provides direct examination of the SB, and DBE is therefore an important tool for evaluating the response to treatment in small bowel Crohn’s disease (SB-CD) patients. 4
Antitumor necrosis factor (anti-TNF) drugs, such as infliximab (IFX), are widely used as a first-line biologic therapy for CD patients with moderate-to-severe disease activity. 5 However, few studies have examined the effect of IFX treatment for patients with isolated SB-CD due to the complexity of SB endoscopy. Thus, there is little known about the factors associated with deep remission following IFX treatment of these patients. In particular, there is uncertainty regarding the association of achieving ER with specific baseline endoscopic features, such as the extent of endoscopy inflammation in different segments, ulcer location, and ulcer size.
Therefore, we compared the DBE findings of SB-CD patients before and after IFX treatment to assess the predictors of ER. Our general purpose was to identify the association of different endoscopic factors with ER, especially the location and severity of SB lesions.
Methods
Study population
This was a retrospective observational study of patients who were examined from 1 January 2018 to 30 November 2022 at the Center for Gastroenterology, The First Affiliated Hospital of Anhui Medical University (Hefei, China). The inclusion criteria were as follows: (i) isolated SB-CD, with diagnosis based on clinical, DBE, radiological, and histopathological evidence from our center; (ii) receipt of IFX treatment, either as a first-line treatment or after escalation of following failure of conventional treatment by a corticosteroid, 5-aminosalicylic acid, and/or immunomodulators; and (iii) receipt of two DBE procedures for endoscopic evaluation, one before and one during IFX maintenance therapy. The exclusion criteria were as follows: (i) age less than 14 years; (ii) receipt of colostomy or ileostomy; (iii) prior use of an anti-TNF agent or another biological agent; and (iv) unavailability of complete data.
The Research Ethics Committee of the First Affiliated Hospital of Anhui Medical University approved this study (Protocol No.: ETIC Quick-PJ 2022-14-56). The written informed consent was obtained from all patients.
Schedule of IFX induction and maintenance therapy
All SB-CD patients received intravenous IFX as induction therapy (5 mg/kg on weeks 0, 2, and 6) and as maintenance therapy (5 mg/kg once every 8 weeks). Passive therapeutic drug monitoring was performed for patients with secondary loss of response (LOR) to optimize the treatment.
Data collection
Before the first DBE and the onset of IFX induction therapy, demographic and clinical characteristics were recorded, including age, gender, smoking habit, course of the disease, disease location, disease behavior (as defined in the Montreal classification), 6 fistulizing perianal lesions, use of combination therapy, and Crohn’s disease activity index (CDAI) score. Laboratory data, including C-reactive protein (CRP), white blood cells (WBC), hemoglobin (Hgb), platelets, and albumin (ALB), were also assessed at baseline. Laboratory biomarkers and the CDAI score were recorded after each IFX infusion. A total of 108 patients were enrolled, all of whom received two DBE evaluations (one before onset of IFX and one during IFX maintenance therapy) and were eligible for inclusion (Figure 1).

Disposition of SB-CD patients who received DBE screening (n = 262) and were excluded for various reasons (n = 154) or were examined to assess IFX effectiveness (n = 108).
DBE procedure and evaluation using the simple endoscopic score for CD
Data from the first DBE were used for baseline assessment, and data from the second DBE were used to evaluate the efficacy of IFX treatment. The second DBE was usually 12 months after the onset of treatment, although the exact time depended on the doctor’s discretion and the patient’s wishes. The DBE procedures were performed and evaluated by four experienced endoscopists using the Fujinon DBE (Fujinon EN-580T Inc, Saitama, Japan). An oral or anal approach was selected according to clinical presentation and radiology results. The longest distance from the endoscope to the ileocecal valve or pylorus was determined from the distance of each push–pull cycle. The depth of insertion, path (transoral, transanal, or both), and endoscopic findings (e.g. normal, erosions, ulcers, hyperplasia, stenosis, and bleeding) were recorded by the endoscopic system.
For data analysis, the SB was divided into three sections: (i) the terminal ileum, the region within 10 cm from the ileocecal valve; (ii) the proximal ileum, the region within 10–300 cm from the ileocecal valve; and (iii) the jejunum, the proximal region excluding the proximal ileum.7,8
The endoscopic operator and a single-blinded reviewer performed endoscopic scoring using the simple endoscopic score for CD (SES-CD). To determine this score, each of the three SB sections was assessed using four endoscopic variables, with each variable ranging from 0 to 3: (i) ulcer diameter (no ulcer: 0; <0.5 cm: 1; 0.5–2 cm: 2; and >2 cm: 3); (ii) percentage of ulcerated surface (no ulcer: 0; <10%: 1; 10–30%: 2; and >30%: 3); (iii) percentage of affected surface (unaffected: 0; <50%: 1; 50–70%: 2; and >70%: 3); and (iv) presence of stenosis (no stenosis: 0; a single stenosis that can be passed: 1; multiple stenoses that can be passed: 2; and stenosis that cannot be passed: 3).7,8 If the DBE could not a reach section, it was scored as ‘0’. Figure 2 shows representative imaging results of patients who had different SES-CD scores.
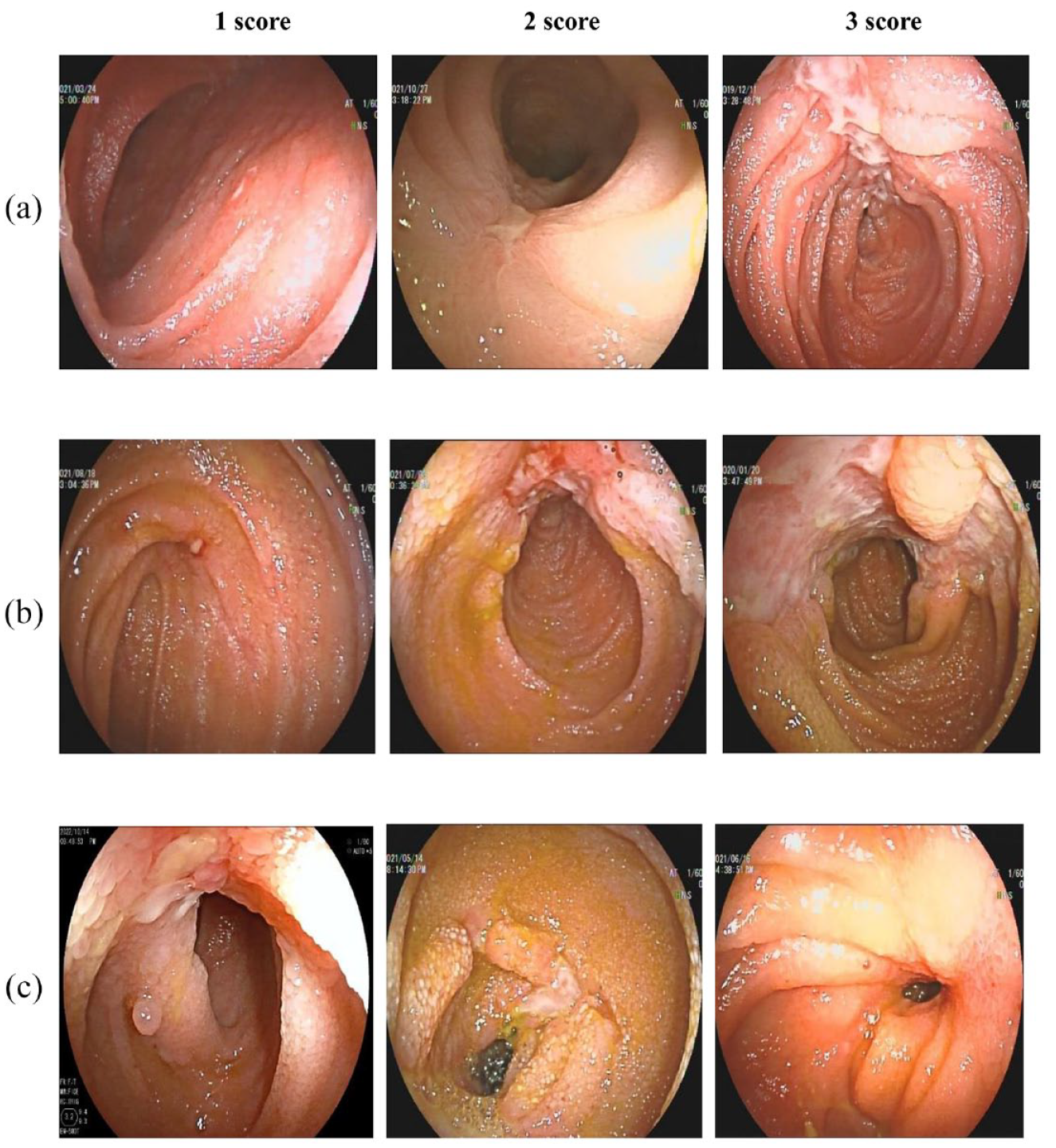
Representative DBE images with SES-CD scores of 1, 2, or 3 for ulcer diameter (a), ulcerated surface (b), and stenosis (c).
Variables, outcomes measures, and definitions
The sum of all variables for each SB section was defined as the total SES-CD. Then, SB-CD disease activity was classified as mild (SES-CD: 3–5), moderate (SES-CD: 6–15), or severe (SES-CD: ⩾16). Overall ER was defined as an SES-CD below 3, MH as an SES-CD of 0, endoscopic response as a 50% reduction in SES-CD from baseline, 9 clinical remission as a CDAI score below 150, and biological remission as normalization of serum CRP (<3 mg/L).
For individual SB segments, the endoscopic SES-CD activity (SES-CDa) was determined. 8 This score excluded the item ‘stenosis’ because it results from intestinal injury, not active inflammation. Thus, the ER of each intestinal segment was classified as having no disease (SES-CDa = 0); mild disease (1 ⩽ SES-CDa < 5); or moderate-to-severe disease (SES-CDa ⩾ 5). 10 Based on the ulcer diameter in the SES-CD, an ulcer was defined as large (>2 cm), medium (0.5–2 cm), or small (<0.5 cm). 11
The global assessments of physicians at 14 weeks after the first IFX infusion were also recorded. A primary nonresponse was defined as no clinical improvement for patients with luminal disease and a lack of reduction of at least 50% in the number of drainage fistulas for patients with perianal fistulas. 12 Secondary LOR was defined as an initial clinical improvement at week 14 of IFX therapy, followed by a relapse of disease. 13
Statistical analysis
The baseline and follow-up characteristics of patients were described. Mean and standard deviation (SD) were utilized to describe data with normal distributions, and median and interquartile range (IQR) were utilized to describe data with skewed distributions. Categorical variables were presented as numbers and percentages. The differences in clinical features at baseline and after IFX treatment were examined by the paired t-test (normally distributed data) or the Wilcoxon rank-sum test (non-normally distributed data). The differences between ER and endoscopic response among SB segments were tested by the chi-square test. Fisher’s exact probability test was used if the expected frequency was less than 1. The evolution of endoscopic ulcer size from baseline to after IFX treatment was assessed by a Sankey diagram. Spearman’s rank correlation test was used to determine the correlations of different endoscopy results with CRP level and CDAI score.
Univariate and multivariate logistic regression analyses were conducted to assess the effect of IFX on ER from SB-CD. First, baseline characteristics and clinical status were regressed on ER after IFX treatment to identify potential factors affecting ER after IFX treatment. Variables with p values <0.05 in the univariate regression were further incorporated into the multivariate logistic regression model. Second, the endoscopic characteristics at baseline (including overall inflammation, inflammation of individual segments, and ulcer size) were regressed on ER after IFX treatment in the univariate and multivariate logistic regression analyses. Based on prior knowledge and literature review,11,14 the multivariate logistic regression analysis adjusted for disease duration, receipt of concomitant medication, and time between DBE procedures. These results were expressed as odds ratios (OR) with 95% confidence intervals (CIs). All statistical tests were two-sided, and significance was set at p < 0.05. All analyses were conducted in IBM SPSS software version 23.0 (IBM Corporation, Armonk, NY, USA) and R software version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 15
Results
Baseline characteristics of patients
We examined 108 eligible patients with isolated SB-CD who received no prior IFX treatment (Table 1). There were 28 females (25.9%) and 80 males (74.1%), the median age was 33 years (IQR: 25–40), and the median disease duration was 38 months (IQR: 24–59). Analysis of disease behavior using the Montreal criteria indicated that 64 patients (59.3%) had B1 (non-stricturing, non-penetrating), 29 patients (26.9%) had B2 (stricturing), and 15 patients (13.9%) had B3 (penetrating). In addition, 29 patients (26.9%) had fistulizing perianal lesions and 10 patients (9.3%) had jejunal involvement. In all, 30 patients (27.8%) received different combination treatments, most of which included azathioprine.
Baseline and follow-up characteristics of patients (n = 108).

ALB, albumin; B1, non-stricturing and non-penetrating; B2, stricturing; B3, penetrating; CDAI, Crohn’s disease activity index CD; CRP, C-reactive protein; DBE, double-balloon endoscopy; Hgb, hemoglobin; IQR, interquartile range; L1, ileal; L4, proximal disease including upper gastrointestinal or jejunum; PLT, platelet; SD, standard deviation; SES-CD, simple endoscopic CD score; WBC, white blood cell.
Changes in clinical, laboratory, and endoscopy results from baseline to the second DBE
At baseline, 97 patients received transanal DBE, 5 received transoral DBE, and 6 received both. The median insertion length into the SB was 100 cm (IQR: 80–150), the mean total SES-CD was 12.1 ± 3.6, and the mean ± SD scores of each factor in the SES-CD were as follows: ulcer diameter (4.0 ± 1.4); percentage of ulcer surface (3.7 ± 1.3); percentage of affected surface (3.2 ± 1.2); and presence of stenosis (1.2 ± 1.4) (Table 1). The median time from the onset of IFX induction therapy to the second DBE procedure was 43 weeks (IQR: 36–55). In all, 75 patients (69.4%) achieved an endoscopic response; among them, ER was achieved in 41 patients (38.0%) and 30 patients (27.8%) achieved MH. Endoscopic nonresponse occurred in the other 33 patients (30.6%).
We examined changes in the clinical, laboratory, and endoscopy results from the first DBE assessment (baseline) to the second DBE assessment (Figure 3). Among all patients, the SES-CD decreased from 12 to 5, the CDAI score decreased from 215.4 to 169.5, and the CRP level decreased from 4.06 to 1.80 mg/L (all p < 0.01). After IFX treatment, 30 patients (27.8%) experienced clinical remission, and 66 patients (61.6%) experienced biological remission. The correlation between the SES-CD and CDAI score was 0.123 at baseline (p = 0.21) and 0.209 at the second DBE (p = 0.03). The correlation between the SES-CD and CRP levels was 0.311 (p < 0.001) at baseline and 0.536 (p < 0.001) at the second DBE.

Changes of SES-CD, CDAI score, and CRP (mg/L) from before (baseline) to after IFX treatment.
Predictors of IFX-induced ER
We performed univariate and multivariate analyses of all 108 patients to identify predictors of ER (Table 2). The univariate analysis indicated ER was significantly associated with age (OR = 0.96, p = 0.03), fistulizing perianal disease (OR = 0.38, p = 0.03), B2/B3 disease behavior (OR = 0.38, p = 0.02), CRP at week 6 (OR = 0.85, p = 0.01), Hgb at week 14 (OR = 1.02, p = 0.03), and CRP at week 14 (OR = 0.85, p = 0.03). The multivariable analysis indicated that CRP at week 6 (OR = 0.86, 95% CI: 0.75–0.98, p = 0.03) was the only factor independently and significantly associated with ER.
Univariate and multivariate analyses of factors associated with IFX-induced ER (n = 108).

ALB, albumin; B1, non-stricturing, non-penetrating; B2, stricturing; B3, penetrating; CD, Crohn’s disease; CDAI, CD activity index; CI, confidence interval; CRP, C-reactive protein; ER, endoscopic remission; Hgb, hemoglobin; IFX, infliximab; OR, odds ratio; PLT, platelets; SB, small bowel; SES-CD, simple endoscopic score for CD; WBC, white blood cells.
Segmental responses based on lesion location
At baseline, the 108 patients had 181 involved intestinal segments, including 69 (63.9%) terminal ileum segments, 102 (94.4%) proximal ileum segments, and 10 (9.3%) jejunum segments.
Segmental ER occurred in 42 of 69 (60.9%) terminal ileum segments, 39 of 102 (38.2%) proximal ileum segments, and 3 of 10 (30.0%) jejunum segments (Figure 4). The rate of ER was significantly higher in the terminal ileum than in the proximal ileum (p = 0.01) but the ER rate was not significantly different in the terminal ileum and jejunum (p = 0.07).

Endoscopic remission (left) and endoscopic response (right) in different small bowel segments.
Segmental endoscopic response occurred in 50 of 69 (72.5%) terminal ileum segments, 56 of 102 (54.9%) proximal ileum segments, and 6 of 10 (60.0%) jejunum segments (Figure 4). The rate of endoscopic response was significantly higher in the terminal ileum than in the proximal ileum (p = 0.02) but the endoscopic response rate was not significantly different in the terminal ileum and jejunum (p > 0.1).
Association of baseline endoscopy results with ER
We then estimated the relationship between the baseline SES-CD and overall ER (Table 3). In all, 22 patients (20.4%) had severe disease (SES-CD ⩾ 16) and 86 patients (79.6%) had moderate disease (SES-CD = 6–15). This difference was not significant in the multivariable-adjusted analysis (aOR = 0.97, 95% CI = 0.35–2.68, p = 0.95).
Impact of overall SES-CD and segmental SES-CDa at baseline on achieving ER after IFX treatment.

SES-CD severe: ⩾16; SES-CD moderate: ⩾6 and <16; SES-CDa moderate/severe: ⩾5; SES-CDa mild: ⩾1 and <5.
CD, Crohn’s disease; CI, confidence interval; ER, endoscopic remission; IFX, infliximab; OR, odds ratio; SES-CD, simple endoscopic CD score; SES-CDa, simple endoscopic CD activity score.
We also evaluated the relationship of baseline segmental SES-CDa with segmental ER (Table 3). In all, 42 patients (60.9%) had moderate/severe disease (SES-CDa ⩾ 5) and 27 patients (39.1%) had mild disease (1 ⩽ SES-CDa < 5) in the terminal ileum. After adjusting for known confounders, there was a significant difference in segmental ER for patients with moderate/severe disease rather than mild disease in the terminal ileum (aOR = 0.27, 95% CI = 0.09–0.83, p = 0.02). In all, 90 patients (88.2%) had moderate/severe disease and 12 patients (11.8%) had mild disease in the proximal ileum. However, the difference was not significant for those with moderate/severe disease rather than mild disease of the proximal ileum (aOR = 1.06, 95% CI = 0.29–3.92, p = 0.93). In addition, the number of affected segments (one versus two or more) was not associated with ER (aOR = 1.05, 95% CI = 0.45–2.46, p = 0.92; Table 4).
Impact of the number of involved small bowel segments on achieving ER after IFX treatment.

CI, confidence interval; ER, endoscopic remission; IFX, infliximab; OR, odds ratio.
Impact of baseline ulcer size on ER after IFX treatment
At baseline, there were 22 (31.9%) large ulcers (>2 cm), 27 (39.1%) medium ulcers (0.5–2 cm), and 20 (29.0%) small ulcers (<0.5 cm) in the terminal ileum segment. In addition, there were 71 (69.6%) large ulcers, 24 (23.5%) medium ulcers, and 7 (6.9%) small ulcers in the proximal ileum segment. We also analyzed the evolution of ulcer size in the terminal ileum and the proximal ileum after IFX treatment (Figure 5). In the terminal ileum, 18 of 22 patients (81.8%) with large ulcers were downgraded to small, medium, or no ulcers after treatment. In comparison, 49 of 71 patients (69.0%) with large ulcers in the proximal ileum were downgraded.

Sankey diagram of the evolution of the sizes of ulcers in the terminal ileum and proximal ileum after infliximab treatment.
Analysis of the relationship of ulcer size and ER indicated that ulcer size in the terminal ileum affected the probability of ER but ulcer size in other segments of the SB did not affect ER. In particular, patients with a large ulcer in the terminal ileum were significantly less likely to achieve ER than those with a small or medium ulcer in this segment (aOR = 0.18, 95% CI = 0.06–0.56, p = 0.01; Table 5). Ulcer size was unrelated to ER in three other comparisons (terminal ileum: medium/large versus small; proximal ileum: large versus medium/small; proximal ileum: medium/large versus small).
Impact of ulcer size in the terminal ileum and proximal ileum on achieving ER after IFX treatment. a

Ulcer size was defined as small (<0.5 cm), medium (0.5–2 cm), or large (>2 cm).
CI, confidence interval; ER, endoscopic remission; IFX, infliximab; OR, odds ratio.
Discussion
Very few trials of patients with CD evaluated treatment outcomes at different specific disease sites. Several cohort studies found that CD at an isolated ileal site led to poor response to treatment with an anti-TNFα drug.10,16 A meta-analysis, which examined data from the GEMINI trial and the CERTIFI and UNITI CD trial, concluded that patients with isolated ileal CD (rather than colonic CD) were significantly less likely to achieve response or remission after receiving a biological agent (29% versus 38%; relative risk = 0.70, 95% CI = 0.56–0.87).2,17 However, many other studies reported no correlation between disease location with response to IFX treatment. 18 It should be noted that the different designs of these studies limit the generalizability of the results. Especially, these studies did not use a consistent definition of effectiveness, and many of them measured the response to therapy using clinical parameters, even though there is a low correlation between clinical and endoscopic response.14,19 Our results also indicated that the CDAI score and CRP level did not fully reflect the severity of endoscopic lesions. In fact, ER and MH are currently the reference standards for therapeutic response because ER is associated with better outcomes, including a lower hospitalization rate and a reduced need for surgery. 1
A previous study that used ER as the reference standard for treatment response was a post hoc analysis of data from four clinical trials. 20 These researchers compared CD patients who received a biological agent on achievement of three outcomes: 1-year ER (SES-CD < 3), 1-year ileal ER, and 1-year colonic ER. Among IFX-naïve patients, the overall ER rate was 27.7% (39/141), the ER in the ileum was 36.7% (29/79), and the ER in the colon was 52.4% (55/105). Many studies used ileocolonoscopy to evaluate ER, 21 even though this method only provides observations of the terminal ileum of the SB, and about 30% of CD is limited to the SB, which may be beyond the scope of ileocolonoscopy. Our results indicated that the detection rate of endoscopic active lesions in the proximal ileal segment was higher than in the terminal ileal segment (94.4% versus 63.9%). There was no involvement of the terminal ileum in 39 of 108 patients (36.1%). In other words, nearly half of these patients had SB lesions that were not accessible by traditional ileocolonoscopy. CD with deep SB involvement predicts a poor prognosis and is associated with a higher risk of complications and surgery. 22 Therefore, the evaluation of deep SB lesions is a critical aspect of disease management. BAE is the only endoscopic method for obtaining supportive histological diagnosis and accurate assessment of ER on this portion of the gastrointestinal tract.
In this study, we used DBE to directly evaluate mucosal lesions in the SB and found the total rate of ER was 38.5%. Takenaka et al. 14 found that 41/114 patients (36%) had SB endoscopic healing during IFX maintenance therapy based on BAE evaluation. A subsequent study by Takenaka et al. 23 that also used BAE found that the SB-ER rate was 47% after treatment with biological agents (IFX, adalimumab, and ustekinumab). Han et al. 24 studied SB-CD patients and found that IFX led to deep remission in 42/91 (46.1%) patients based on capsule endoscopy. These rates of ER in the total SB are similar to our results. Our evaluation of the ER of different SB segments showed that segmental ER occurred in 42/69 (60.9%) terminal ileum segments, 39/102 (38.2%) proximal ileum segments, and 3/10 (30.0%) jejunum segments. Thus, the highest rate of ER was in the terminal ileum, and it appears to be more difficult to achieve ER in the deep SB. It is possible that deep SB lesions were more severe in our group of patients with isolated SB-CD. Thus, we suggest that future studies should stratify SB-CD patients according to lesion location and severity of inflammation when examining the effect of different treatments on ER.
Identification of the predictors of ER before treatment of CD patients may help to guide treatment strategies and provide more individualized treatments. For patients receiving anti-TNF drugs, most of the potential predictors had little or no usefulness. The few factors that may predict response were disease behavior, disease severity, CRP, ALB, serum cytokine expression, and previous anti-TNF treatment. 18 There is little known about the predictors of IFX-induced deep remission in patients with SB-CD. Han et al. 24 studied IFX-naïve SB-CD patients who received IFX and found that moderate-to-severe endoscopic activity and the presence of fibrosteatosis at baseline were associated with a reduced probability of deep remission. Takenaka et al. 14 found that failure to achieve endoscopic healing from SB-CD was significantly associated with the presence of stricturing or penetrating disease (p = 0.014), lack of concomitant treatment with an immunomodulator (p = 0.01), and previous treatment with an anti-TNF drug (p = 0.018). Our univariate analysis showed that age, perianal disease, B2/B3 disease behavior, CRP level at week 6, and Hgb and CRP at week 14 were associated with SB-ER but a high CRP level at week 6 was the only factor significantly associated with SB-ER failure in the multivariable analysis. A post hoc analysis of data from the ACCENT I trial (a 2012 prospective randomized controlled trial of CD patients that examined the effect of IFX) showed that normalization of CRP level at week 14 increased the probability of maintaining remission. 25 A post hoc analysis of data from the TAILORIX trial (a 2020 prospective randomized trial of CD patients that examined the effect of IFX and calprotectin) analyzed the correlation between biomarkers and endoscopic results and found that fecal calprotectin and CRP levels starting at week 6 were predictive of MH during maintenance treatment. 26 These results are consistent with our finding that the levels of inflammatory biomarkers at baseline were unrelated to overall ER. However, we found that a high CRP level after completion of IFX induction therapy (week 6) was negatively associated with ER during the maintenance period. This suggests that early response to treatment (based on CRP) may be a better predictor than disease severity at baseline.
In addition to the assessment of clinical characteristics, we suggest that stratification using baseline endoscopic results should also be considered when attempting to predict patient outcomes. The significance of endoscopic disease severity scoring and ulcer size, as determined by the SES-CD, is presently unclear. Two previous studies used ileocolonoscopy to evaluate the impact of endoscopic characteristics on the outcome of CD patients who received IFX. The first study (a post hoc analysis of the SONIC study) showed that the overall severity of endoscopic lesions was unrelated to ER; however, a large ulcer (rather than a medium or small ulcer) in the ileum (OR = 0.31, p = 0.03) or rectum (OR = 0.26, p = 0.02) was associated with a reduced probability of achieving ER before week 26. 11 The second study (a post hoc analysis of the TAILORIX study) reported that disease severity at the baseline endoscopy was unrelated to ER and that the ER was similar for patients with very large and small ulcers at week 12 and week 54. 27 No previous study of patients with SB-CD used DBE to examine the association of baseline SB endoscopic characteristics with achieving SB-ER. Our study showed that overall endoscopic activity was unrelated to the achievement of SB-ER. However, our analysis of patients with lesions in the terminal ileum showed that patients with moderate/severe lesions (rather than mild lesions) had a lower probability of attaining ER (aOR = 0.27, 95% CI = 0.09–0.83, p = 0.02). Furthermore, we found that a larger ulcer in the terminal ileum was associated with a lower rate of segmental ER (aOR = 0.18, 95% CI = 0.06–0.56, p = 0.01). By contrast, disease severity based on endoscopy and ulcer size in the deep SB were unrelated to segmental ER. Thus, the overall severity of the disease based on the SES-CD score does not affect the likelihood of achieving ER. Patients with larger ulcers and moderate/severe lesions in the terminal ileum may have difficulty achieving segmental ER.
This study has some limitations. First, this was a single-center study and our sample size was relatively small. Second, the SES-CD score was initially developed for use with colonoscopy, and no current DBE scoring system for CD focuses on the SB. These studies previously demonstrated that the SES-CD and SES-CDa can be used to assess the deep SB.7,28 However, this scoring system is cumbersome. Moreover, because this system includes the percentage of ulcerative lesions, the score is likely to vary according to the insertion distance when the observation area of the deep SB was extensive. We consider it necessary to validate this scoring system in future work. Third, we used radiology evaluation to assess the major lesions of the SB and to determine the entry route for DBE and used a retrograde DBE approach in most patients. We did not perform total SB endoscopy examinations. Therefore, it is possible that we missed some jejunal lesions. Moreover, we only identified 10 patients (9.3%) with jejunum involvement, so a meaningful analysis of this group was not possible. Finally, the best time for evaluating ER in patients with SB-CD is not clear. A consensus statement concluded that this result should be evaluated using ileocolonic examination at 6–9 months after the onset of treatment. 1 However, our patients had different intervals between the first and second DBE, although this interval was close to 43 weeks (IQR: 36–56) in most patients.
Conclusion
In conclusion, we used DBE to evaluate ER in patients with SB-CD who received IFX treatment. Our three major results were as follows: (i) lesions in the terminal ileum had higher rates of ER than lesions in other deep SB segments (proximal ileum and jejunum); (ii) a higher CRP level at week 6 (after completion of IFX induction therapy) was associated with failure to achieve SB-ER; and (iii) the overall SES-CD at baseline was unrelated to achievement of total ER. Segmental ER may be more difficult to achieve in patients with SB-CD who have severe/moderate disease or larger ulcers in the terminal ileum. We suggest that clinicians should consider the risk factors identified here when adjusting therapeutic strategies and attempting to achieve deep remission in patients with SB-CD.
Supplemental Material
sj-doc-1-tag-10.1177_17562848231224842 – Supplemental material for Use of double-balloon endoscopy and an endoscopic scoring system to assess endoscopic remission in isolated small bowel Crohn’s disease after treatment with infliximab
Supplemental material, sj-doc-1-tag-10.1177_17562848231224842 for Use of double-balloon endoscopy and an endoscopic scoring system to assess endoscopic remission in isolated small bowel Crohn’s disease after treatment with infliximab by Wei Han, Jing Hu, Juan Wu, Peipei Zhang, Qiuyuan Liu, Naizhong Hu and Qiao Mei in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.