
Abstract
Background:
Acute gastrointestinal bleeding (GIB) is a life-threatening event. Around 20–30% of patients with GIB will develop hemodynamic instability (HI).
Objectives:
We aimed to quantify HI as a risk factor for the development of relevant end points in acute GIB.
Design:
A systematic search was conducted in three medical databases in October 2021.
Data sources and methods:
Studies of GIB patients detailing HI as a risk factor for the investigated outcomes were selected. For the overall results, pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated based on a random-effects model. Subgroups were formed based on the source of bleeding. The Quality of Prognostic Studies tool was used to assess the risk of bias.
Results:
A total of 62 studies were eligible, and 39 were included in the quantitative synthesis. HI was found to be a risk factor for both in-hospital (OR: 5.48; CI: 3.99–7.52) and 30-day mortality (OR: 3.99; CI: 3.08–5.17) in upper GIB (UGIB). HI was also associated with higher in-hospital (OR: 3.68; CI: 2.24–6.05) and 30-day rebleeding rates (OR: 4.12; 1.83–9.31) among patients with UGIB. The need for surgery was also more frequent in hemodynamically compromised UGIB patients (OR: 3.65; CI: 2.84–4.68). In the case of in-hospital mortality, the risk of bias was high for 1 (4%), medium for 13 (48%), and low for 13 (48%) of the 27 included studies.
Conclusion:
Hemodynamically compromised patients have increased odds of all relevant untoward end points in GIB. Therefore, to improve the outcomes, adequate emergency care is crucial in HI.
Registration:
PROSPERO registration number: CRD42021285727.
Introduction
Acute gastrointestinal bleeding (GIB) is a life-threatening event, often requiring emergency medical care. 1 The mortality rate ranges from 2% to 10%, varying between the countries, making it one of the acute gastrointestinal diseases with the most unfavorable prognosis.2,3
Current guidelines provide little to no information and recommendations on the optimal management and resuscitation of hemodynamically unstable GIB patients.4–6 The only randomized controlled trial (RCT) which investigated the early resuscitation of patients with upper GIB (UGIB) found that patients receiving early vasopressor treatment with more value-controlled fluid therapy reached hemodynamic stability significantly sooner. Moreover, these patients also had better laboratory values, developed fewer complications, and had an increased chance of survival. 7 These results suggest that the early detection and aggressive treatment of hemodynamic instability (HI) are crucial.
Approximately 20–30% of patients with acute GIB develop HI, which is thought to be associated with worse outcomes, including higher mortality and rebleeding rates than usual. Laursen et al. 8 found that hemodynamically unstable GIB patients had a mortality rate of 13%, compared to only 4% in stable patients. Several other identified studies suggested the same trend.9,10 However, these values have never been systematically reviewed and quantified before.
Our systematic review and meta-analysis aimed to quantify the magnitude of the risk of developing the most relevant end points in the presence of HI in acute GIB.
Methods
A systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement (see Supplemental Table S1) and the recommendations of the Cochrane Handbook.11,12 The review protocol was registered in advance on PROSPERO with the registration number CRD42021285727.
Systematic search
Three databases, MEDLINE (via PubMed), Embase, and Cochrane Central Register of Controlled Trials (CENTRAL), were systematically searched from inception until the 22nd of October 2021. We did not apply any filters or restrictions to our search. The main parts of the search query included terms in connection with HI/shock and GIB. For the detailed search strategy, see Supplemental Table S2. In addition, we manually searched for relevant articles and checked the bibliographic reference lists of studies selected for inclusion.
Eligibility criteria
The population–exposure–outcome (PEO) framework was used to identify eligible studies. 13 We included studies with a population (P) of adult patients (age >18 years) with GIB. Studies were eligible if they contained data on the investigated outcomes in the presence (E) of HI/shock at admission. The primary outcome (O) was mortality, and the secondary outcomes were rebleeding, need for surgery, need for transfusion, length of hospitalization (LOH), and need for rescue endoscopic therapy.
The end points were investigated in UGIB, lower GIB (LGIB) patients, and in populations with UGIB and LGIB patients separately. For defining HI/shock, the individual definitions of the included studies were used. Based on their definitions, HI and shock were considered synonyms, and the term HI was used for both.
RCTs, case–control, cross-sectional, and cohort studies were eligible for the systematic review. Only cohort studies were included in the meta-analytical calculations. Full-text articles were considered eligible.
Study selection and data extraction
After the systematic search, the yielded articles were imported into a reference management program (EndNote X7.4, Clarivate Analytics, Philadelphia, PA, USA). After duplicate removal, two independent authors (ET and LF) screened the remaining publications first by title and abstract, and then by full text. Disagreements were resolved by consensus and the involvement of the senior review author (BE). Cohen’s kappa coefficient (κ) was calculated at both levels of selection to measure inter-reviewer reliability. 14 In the case of multiple publications from the same cohort, the study with the highest number of cases was selected.
Two investigators independently extracted data (ET and LF) and manually uploaded them into a purpose-designed Excel spreadsheet (Office 365, Microsoft, Redmond, WA, USA). Disagreements were solved by the senior review author (BE).
Data were collected on the first author, year of publication, study location, study design, period of enrollment, study population, number and age of the enrolled patients, source of bleeding, follow-up time, number of patients with and without HI/shock at admission, and on the definitions of HI/shock. For statistical analysis, raw data were extracted into two-by-two tables (outcome yes/no; HI/shock yes/no). Odds ratios (ORs) and hazard ratios (HRs) and their respective 95% confidence intervals (CIs) were also collected.
Statistical analysis
The statistical analysis was performed by a biostatistician (DSV) using the R programing language (R Core Team 2022, v4.2.1). Forest plots were used to display the results of the meta-analytical calculations. The minimum number needed to perform the meta-analytical calculation was three. In-hospital mortality and mortality in less than 7 days, as well as 6-week and 30-day mortality, were pooled. The same strategy was used for rebleeding. Pooled ORs with 95% confidence intervals were calculated using the random-effects model. I2 statistics by Thompson and Higgings 15 were used to describe between-study heterogeneity. Publication bias was assessed by funnel plots and Egger’s tests with additional analysis if a potential small study bias was suspected. 16 The leave-one-out method was used for sensitivity analyses. Subgroup analyses were performed for studies where the ‘subtype’ of bleeding was specified. Additional analyses were performed on articles with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for HI.
Risk of bias assessment
The risk of bias assessment was carried out at the study level and across studies independently by two investigators (ET and TS) using the Quality of Prognostic Studies (QUIPS) tool for each outcome. 17 Disagreements were resolved by the senior review author (BE).
Results
Search and selection
A total of 11,583 studies were identified through database searching. After the duplicate removal and careful selection by title and abstract, 218 articles were found eligible for full-text assessment. Three additional studies were identified through cross-referencing and manual database searching. Finally, our qualitative synthesis comprised 62 studies, and 39 were included in the quantitative synthesis. The details of the study selection process are summarized in the PRISMA flow chart in Figure 1.

Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 flowchart representing the study selection process.
Basic characteristics of included studies
The main characteristics of the included studies are summarized in Table 1. Eligible studies were reported between 1977 and 2021. The number of study participants ranged from 56 to 12,601. The majority of the identified studies were cohort studies, of which 22 were prospective,8,10,18–37 32 were retrospective,9,38–68 and two were ambidirectional analyses.69,70 One RCT, 71 one case–control, 72 and three cross-sectional studies58,73–75 were also included in the systematic review.
Basic characteristics of included studies.

HI, hemodynamic instability; HR, hazard ratio; LGIB, lower gastrointestinal bleeding; M-W, Mallory-Weiss; NA, not applicable; NVUGIB, non-variceal upper gastrointestinal bleeding; OR, odds ratio; PUB, peptic ulcer bleeding; UGIB, upper gastrointestinal bleeding; UK, United Kingdom; USA, United States of America; VUGIB, variceal upper gastrointestinal bleeding.
The rate of HI/shock ranged between 1.2% and 68.3% of the eligible studies. The source of bleeding was UGIB in 54 of the included studies,8–10,18–34,36,37,39–45,47–50,52–55,58–60,63–76 and LGIB in 7.35,38,46,51,57,61,62 One study detailed a population including both UGIB and LGIB patients. 56
In terms of outcomes, 44 studies reported mortality,8–10,18,20–30,32–37,39,41–43,47–49,52–55,58,63–66,68–71,73–75 27 rebleeding,8,19,20,22,25,29–31,34,35,38–40,43,45,46,50,51,55–57,60,68,70,72,75,76 and 5 the need for surgery.38,44,59,61,67 Two studies detailed the need for transfusion,30,60 and another two the LOH.38,62
For the definitions in the included studies for HI/shock, see Supplemental Table S3.
Mortality
We identified 27 studies investigating in-hospital mortality in the presence and absence of HI in UGIB; 22 could be pooled and included in the meta-analytical calculation (see Figure 2). Our results suggested considerably increased odds of in-hospital mortality in patients with HI (OR: 5.48; CI: 3.99–7.52; I2: 74%) (see Figure 2). Subgroup analyses were made in the cases of UGIB, non-variceal UGIB (NVUGIB), and peptic ulcer bleeding (PUB). In studies containing information about patients suffering from all types of UGIB, the odds were higher (6.18; CI: 4.11–9.28), compared to the studies only with PUB patients (4.79; CI: 2.62–8.97). In the case of NVUGIB, the results were not statistically significant (OR: 6.52; CI: 0.29–144.21). The influential analysis detected no outlier study (see Supplemental Figure S1).

Forest plot representing the odds of in-hospital mortality in UGIB.
In the analysis of studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for HI, smaller, but still significantly increased odds were observed for in-hospital mortality (OR: 4.14; CI: 2.47–6.94; I2: 67%) (see Figure 3).
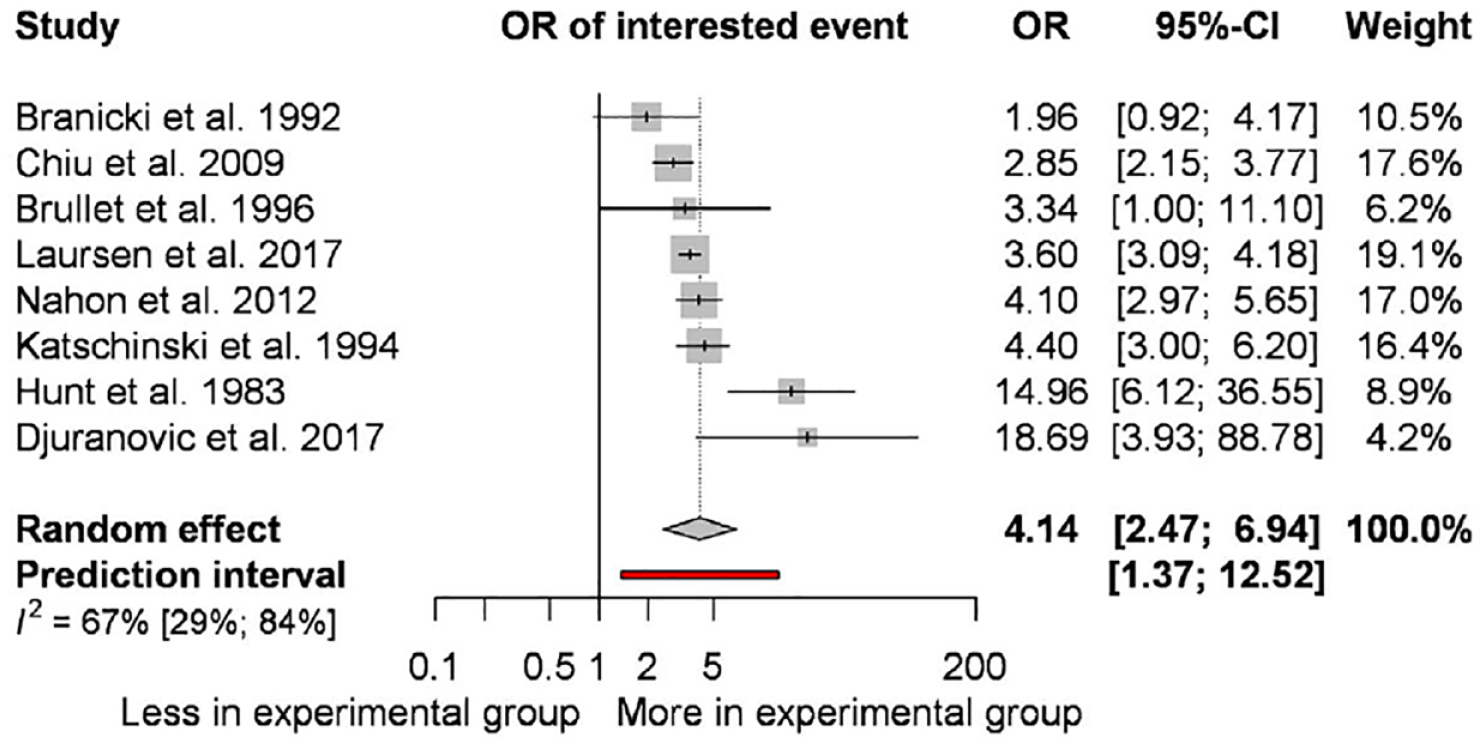
Forest plot representing the odds of in-hospital mortality in upper gastrointestinal bleeding in studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for hemodynamic instability (HI).
Besides all other studies, four cohorts, and one cross-sectional, which were not included in the meta-analytical calculation, also suggested higher odds of in-hospital mortality in the presence of HI in UGIB.24,35,43,52,75
One of the identified studies detailed in-hospital mortality in a population both with UGIB and LGIB patients, also indicating increased odds among hemodynamically unstable patients (OR: 5.07; CI: 2.54–10.11). 56
In total, 19 studies investigated follow-up mortality, all for UGIB. Among the 19 studies, 16 included information on 30- to 42-day mortality, of which 10 were included in the meta-analysis. The odds of mortality during the follow-up period were 3.99 (CI: 3.08–5.17; I2: 52%) (see Figure 4). The influential analysis detected no outlier study (see Supplemental Figure S2).
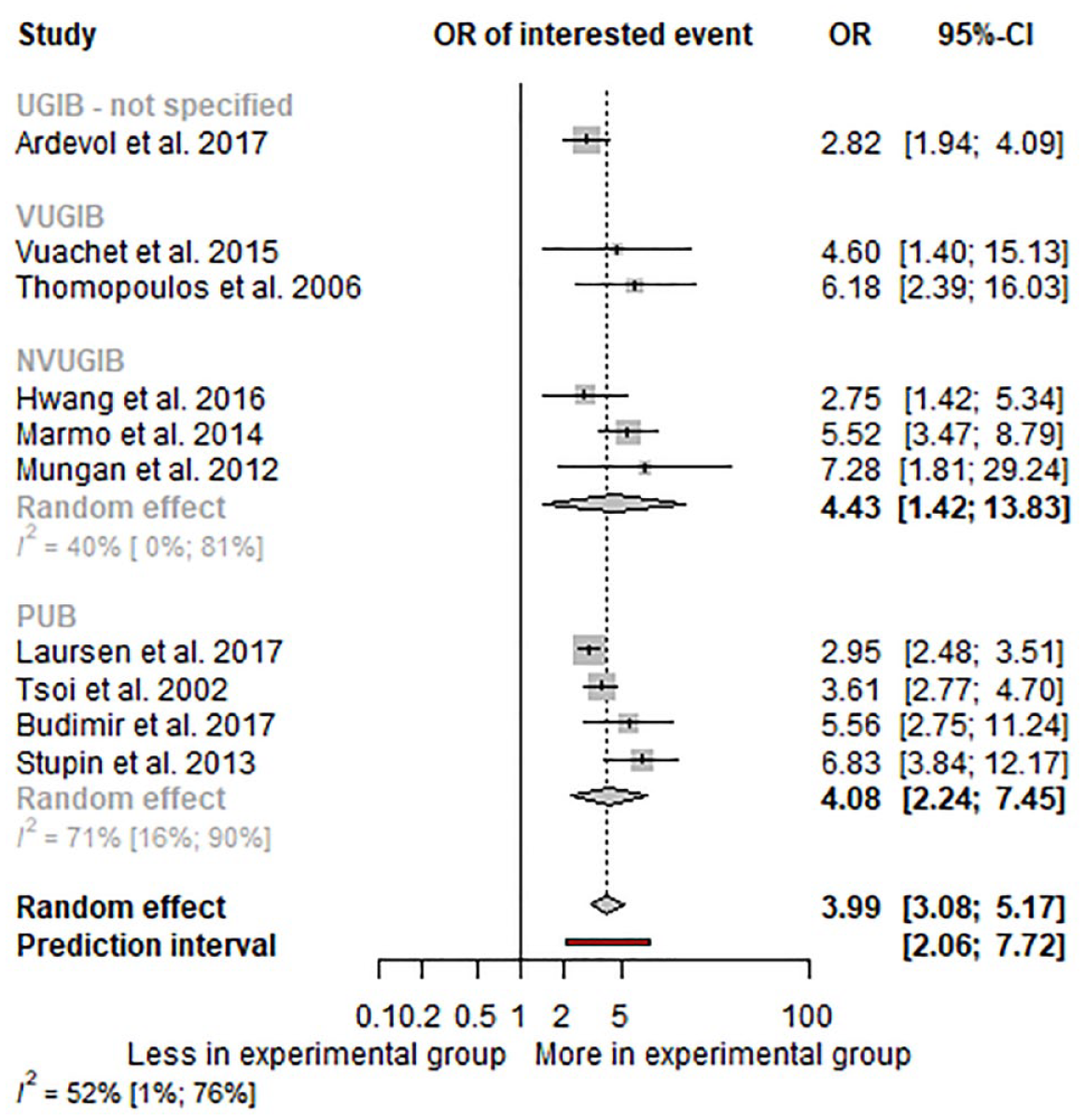
Forest plot representing the odds of 30- to 42-day mortality in UGIB.
In the analysis of studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for HI, the odds of 30- to 42-day mortality were also significant (OR: 4.03; CI: 2.68–6.05; I2: 58%) (see Supplemental Figure S3).
In addition, the other six eligible articles, five cohort studies, and one RCT suggested increased mortality in HI.36,42,43,49,53,71 Two studies investigated 2-week mortality, one in PUB and one in VUGIB. In VUGIB patients, HI was associated with 2-week mortality (OR: 4.08; CI: 1.52–10.96), in contrast with PUB, where the results were not statistically significant (OR: 1.67; CI: 0.26–10.74). Lohse et al. 32 reported increased 90-day mortality in PUB (OR: 2.03; CI: 1.69–2.43).
Rebleeding
In all, 17 studies examined the association between in-hospital rebleeding and HI, 16 in UGIB, and 2 in LGIB. Of the 15 studies with UGIB as the source of bleeding, 11 were included in the meta-analysis (see Figure 5). Our results showed increased odds of in-hospital rebleeding in the presence of HI in UGIB (OR: 3.68; CI: 2.24–6.50; I2: 91%) (see Figure 5). Subgroup analyses were made in the cases of NVUGIB and PUB, where the odds were higher in the case of PUB patients, compared to NVUGIB patients (OR: 2.55; CI. 1.44–4.50 versus OR: 4.95; CI: 1.70–14.44). The influential analysis detected Budimir et al. as an outlier study; however, no clinical cause could be identified behind it.
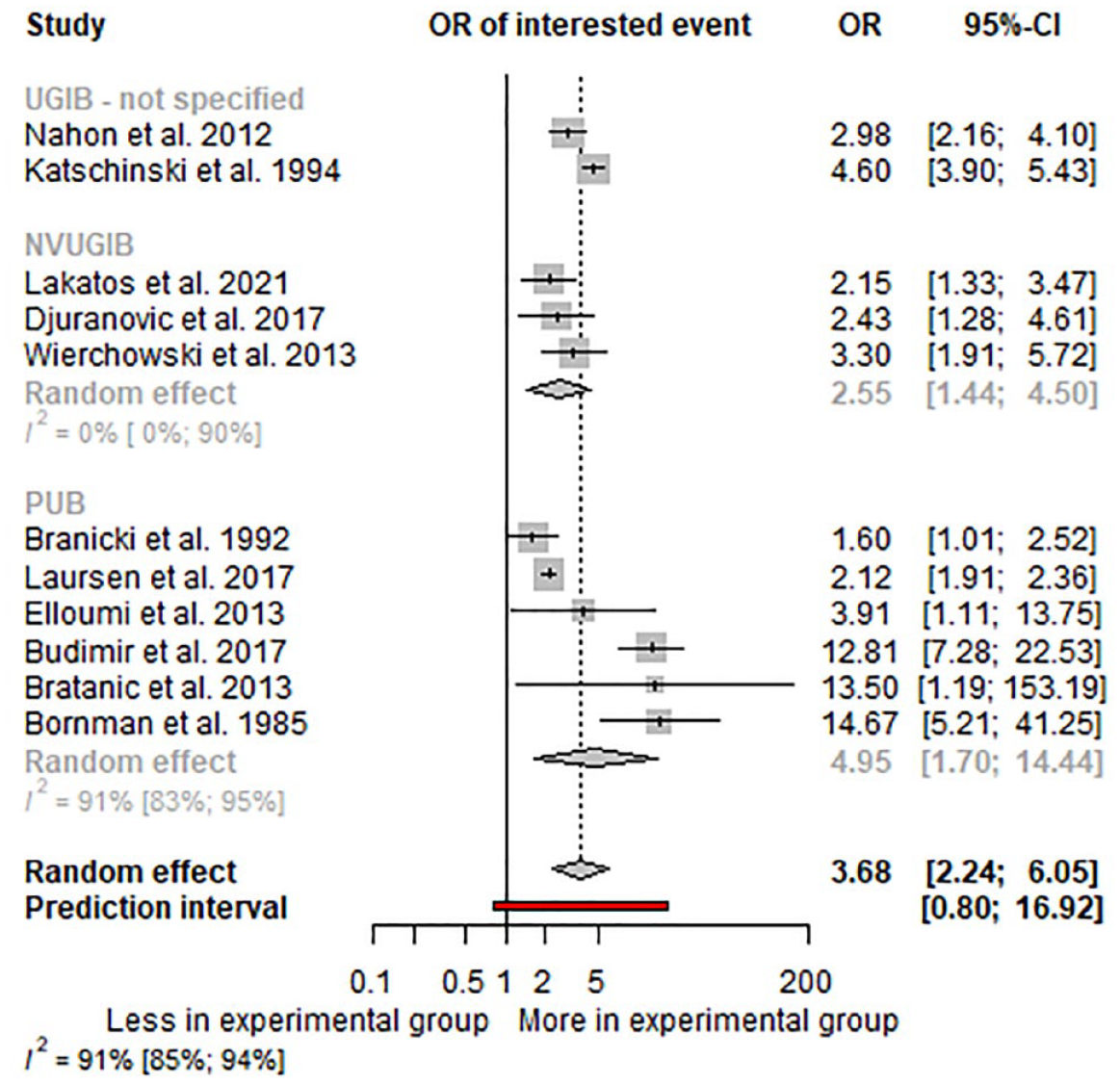
Forest plot representing the odds of in-hospital rebleeding in UGIB.
In the analysis of studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for HI, significant, but lower odds of in-hospital rebleeding in hemodynamically unstable patients (OR: 3.92; CI: 1.80–8.55; I2: 94%) (see Figure 6).

Forest plot representing the odds of in-hospital rebleeding in upper gastrointestinal bleeding in studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for hemodynamic instability (HI).
Moreover, the other four studies, which were not included in the meta-analytical calculation, reported increased odds of in-hospital rebleeding.43,60,75 Two studies investigating in-hospital rebleeding in hemodynamically unstable LGIB patients also reported increased odds (HR: 3.78; CI: 1.06–13.7; OR: 1.85; CI: 1.01–3.42).35,38
Nine studies detailed the odds of 30- to 42-day rebleeding in the presence of HI, eight in UGIB, and one in LGIB. Four studies of patients with UGIB were included in the meta-analysis, where the odds were 4.12 (CI: 1.83–9.31; I2: 39%) (see Figure 7). The leave-one-out analysis was limited due to the low number of studies (see Supplemental Figure S5).

Forest plot representing the odds of 30- to 42-day mortality in UGIB.
In the analyses in studies with a definition of a blood pressure ⩽100 mmHg and/or a pulse rate ⩾100/min for HI, almost similar odds were observed (OR: 4.13; CI: 1.11–15.37; I2: 0%) (see Supplemental Figure S6).
The other five studies, four with UGIB and one with LGIB patients, also reported increased odds of 30- to 42-day rebleeding.43,46,57,68,72 Two studies were identified investigating 90-day rebleeding, one in LGIB and one in general GIB, both reporting increased odds of rebleeding in HI (OR: 0.59; CI: 0.17–2.06; OR: 2.90; CI: 1.10–7.70).32,51
Need for surgery
Five studies investigated the need for surgery in the presence of HI. For UGIB, there was an increased need for surgery among hemodynamically compromised UGIB patients (OR: 3.65; CI: 2.84–4.68) (see Figure 8).

Forest plot representing the odds of need for surgery in upper gastrointestinal bleeding.
Among patients with LGIB, the two identified studies also suggested an increased need for surgery in patients with HI (HR: 13.5; CI: 3.2–5.65; OR: 4.81; CI: 1.87–12.37).38,61
Need for transfusion
Two studies detailed the need for transfusion. In both studies, the source of bleeding was UGIB and indicated increased odds of transfusion in the presence of HI (OR: 3.57; CI: 2.6–5.0; OR: 3.42; CI: 2.73–4.28).
Length of hospitalization
Two studies were identified for LOH, both detailing LGIB patients. Abeldawi et al. 38 reported increased hospital stays among hemodynamically compromised patients (HR: 1.1; CI: 1.05–1.02). In contrast, the results of Schmulewitz et al. 62 (HR: 0.8; CI: 0.7–1.0) indicated a trend for shorter hospital stays under the same circumstances; however, their results were not statistically significant.
Need for endoscopic rescue therapy
We could not identify any studies reporting the need for endoscopic rescue therapy in hemodynamically unstable GIB patients.
Risk of bias and publication bias assessment
Of the 27 studies detailing in-hospital mortality, one (4%) had a high, 13 (48%) had a moderate, and 13 (48%) had a low risk of bias. For follow-up mortality, of the 19 studies, 2 (11%) were found to be high-, 8 (42%) moderate-, and 9 (47%) low-risk studies. Of the 17 studies detailing in-hospital rebleeding, 7 (42%) were considered moderate- and 10 (58%) low-risk studies. In the case of follow-up rebleeding, of the 11 studies, 3 (27%) were considered moderate-risk and 7 (73%) low-risk studies. As for the need for surgery, one of the five included studies had low risk (20%) and four had moderate risk (80%). The four studies detailing the need for transfusion and the LOH were found to have moderate risk. The assessment result was graphically demonstrated, as shown in Supplemental Figures S7–S13. The results of the publication bias assessment are shown in Supplemental Figures S14–S16.
Discussion
Our meta-analysis and systematic review found that HI was associated with a fourfold increase in both in-hospital and 30- to 42-day mortality and the risk of rebleeding in UGIB. In the presence of HI, the need for surgery was also more than three times higher. Moreover, all but one of the studies investigating the need for transfusion and LOH identified HI as a risk factor.
Hemorrhagic shock is a critical condition characterized by inadequate perfusion to vital organs leading to an imbalance in oxygen supply and demand. 77 It has several different consequences throughout various pathophysiological pathways. Hypovolemia results in decreased cardiac output, leading to reduced macro- and microcirculation, causing hypoxia. Hypoxia causes reduced oxygen delivery to vital organs to a certain point where it becomes impossible to meet the oxygen demand. 78 If there is a preexisting ischemic injury with compromised blood flow, the course and consequences of the disease can be even more severe. At a certain point in the progression of the disease, a switch from aerobic to anaerobic metabolism will occur, resulting in lactate acidosis. Moreover, current studies suggest that the initial lactate level could be associated with significantly worse patient outcomes. Shrestha et al. found that patients with elevated lactate levels (>2.0 mmol/l) on presentation were more likely to be admitted to ICU and receive red blood cell transfusion than patients with normal lactate levels, whereas Lee et al. found that at admission lactate level was associated with higher 30-day mortality.79,80
Many approaches are used in the literature to identify patients with HI/shock; however, almost all definitions were based on the initial low systolic blood pressure and/or high heart rate. These two parameters can be measured rapidly and noninvasively, without requiring any particular expertise or equipment. It can also be used in patients with impaired cognitive, mental, or critical status. Pre-endoscopic scoring, such as the Rockall or Glasgow-Blatchford scores, which are widely used in clinical practice to determine the severity of UGIB, also includes signs of HI, together with other risk factors.81,82 However, based on the results of our study, only the two parameters mentioned above at presentation can predict a fourfold increase in the odds of in-hospital mortality and rebleeding in acute GIB.
Based on our result, initial resuscitation and stabilization of HI in acute GIB are crucial to prevent the development of the investigated outcomes. However, many questions about these patients’ initial care still need to be clarified. There is still uncertainty regarding the optimal rate of fluid resuscitation (aggressive versus restrictive), the use of vasopressors, and the optimal type of fluid therapy in the guidelines. Recent meta-analyses suggest that the availability and the use of different endoscopic techniques could also impact the outcomes of the bleeding episode.83,84 The European Society of Gastrointestinal Endoscopy (ESGE) Guideline recommends waiting at least 6 h after the development of UGIB before performing an endoscopy. 4 The recommendation is based on a prospective Danish cohort study that detected worse patient outcomes in case of too early endoscopy in hemodynamically unstable patients, such as higher in-hospital mortality rate. 8 One of the possible explanations for that could be the lack of the proper correction of the hemodynamic status in a shorter time.
All identified articles reported an increased risk for in-hospital mortality in the presence of HI. However, there were studies where the chance was extremely high. Bratanic et al. reported significantly higher odds of in-hospital mortality in PUB, OR: 29.00 (CI: 2.49–337.18). One of the possible explanations behind it could be that they only included patients with a high risk of bleeding, and the initial endoscopy was performed in 4 h. 39 Likewise, Chaabane et al. found higher odds of in-hospital mortality (OR: 19.70; CI: 6.43–60.32). Their patients also had an emergency gastroscopy, and the definition used for HI was stricter: a systolic blood pressure <90 mmHg. 41 On the other hand, Branicki et al. 20 and Ishikawa et al. 48 also reported a higher tendency for in-hospital mortality in the presence of HI (OR: 1.96; CI: 0.92–4.17 and OR: 11.93; CI: 0.65–219.99, respectively); however, their results were not significant. Branicki et al. used a less exact definition for GIB, that is, the presence of hematemesis or melena confirmed by the medical staff. Ishikawa et al. included patients only who underwent surgery for PUB, meaning a high-risk population.
Strengths of the study
This study is the first meta-analysis and systematic review quantifying HI as a risk factor for developing the most relevant adverse end points of GIB. A rigorous methodology was used to identify all relevant studies. We also investigated the major bleeding types separately, with subgroup analyses in the case of UGIB.
Limitations of the study
Despite all the strengths, this study had some limitations too. First, in certain analyses, there was considerable statistical heterogeneity. The reason behind it could be the clinical heterogeneity across studies, for example, the difference in defining HI or the source of bleeding. Second, some of the included cohort studies were retrospective analyses. Finally, in some of the included outcomes, the risk of bias was moderate or high.
Implications for practice and research
Based on our results, patients presenting with HI should be identified and treated as proactively as possible. A unified definition of HI/shock should be integrated into clinical practice. Moreover, high-quality RCTs are needed to investigate the initial resuscitation of these patients. Finally, further prospective cohort studies should investigate the risk for initial HI, looking for modifiable factors.
Conclusion
We can conclude that hemodynamically compromised patients have increased odds of the clinically most relevant end points of GIB, including a fourfold increase in in-hospital mortality. Therefore, early resuscitation and stabilization of these patients are crucial to improve survival.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231190970 – Supplemental material for At admission hemodynamic instability is associated with increased mortality and rebleeding rate in acute gastrointestinal bleeding: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848231190970 for At admission hemodynamic instability is associated with increased mortality and rebleeding rate in acute gastrointestinal bleeding: a systematic review and meta-analysis by Edina Tari, Levente Frim, Tünde Stolcz, Brigitta Teutsch, Dániel Sándor Veres, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.