
Abstract
Background
We performed a meta-analysis to compare the effects of high-dose (80 mg/day) versus low-dose (40 mg/day) proton pump inhibitors (PPIs) on gastrointestinal ulcer bleeding.
Methods
We retrieved studies of randomized controlled trials of PPIs administered according to different schedules for the treatment of gastrointestinal ulcer bleeding from Medline, Embase, Web of Science, Clinical Trials, and the Cochrane Database in April 2020.
Results
Nine randomized controlled trials including 2329 patients were included in this meta-analysis. There were no significant differences in the incidences of re-bleeding, operation intervention, postoperative mortality, and length of hospital stay between the low-dose and high-dose groups. However, the blood transfusion volume was significantly higher in the high-dose group.
Conclusion
Compared with low-does PPIs, high-dose PPIs had no effect on the incidence of re-bleeding, operation intervention, or postoperative mortality, and did not reduce hospital stay in patients treated with endoscopic hemostasis for gastrointestinal bleeding.
Keywords
Introduction
Gastrointestinal bleeding is a common clinical emergency caused by various factors, including gastrointestinal ulcers, tumors, stress, and trauma. Gastrointestinal ulcers are one of the most common causes of gastrointestinal bleeding, with digestive tract ulcers accounting for about 50% of cases.1,2 Endoscopic hemostasis is an effective method for treating bleeding caused by digestive tract ulcers, and has been shown to significantly reduce the rebleeding and mortality rates in patients.3–5 However, gastric acid can affect the formation of blood clots and increase the risk of rebleeding, 6 and controlling the formation of gastric acid after endoscopic hemostasis is a key factor in reducing the occurrence of rebleeding.
Proton pump inhibitors (PPIs) are commonly used to inhibit gastric acid secretion and increase gastric pH. They can inhibit basic gastric acid and histamine secretion, inhibit acid secretion stimulated by food, and block the final channel of gastric acid secretion.6,7 PPIs are benzimidazole drugs that combine irreversibly with and inactivate the proton pump, thus inhibiting its acid-secretion function. 8 However, PPIs only inhibit the activated proton pump in the acidic environment of secretory tubules and have no inhibitory effect on the static proton pump, and also depend on covalent binding to the H+-K+-ATPase, making their action relatively slow.9,10 Although these factors mean that high-dose PPI regimens are often used in the clinic, 11 some results have shown that high-dose PPIs may have a similar acid-inhibitory effect to low-dose PPIs. 11
In this study, we systematically evaluated the effects of high-dose (80 mg/day) versus low-dose (40 mg/day) PPIs on the prognosis of patients with gastrointestinal ulcer bleeding, to provide evidence to support the choice of PPI administration schedule in patients with gastrointestinal ulcer bleeding.
Methods
Search strategy
We performed a systematic review and meta-analysis, reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Supplementary table 1). Articles reporting randomized controlled trials (RCTs) of different administration schedules of PPIs for the treatment of gastrointestinal ulcer bleeding were retrieved from PubMed, Embase, Web of Science, Clinical Trials, and the Cochrane Database from the start of the database up to April 2020, using the keywords “Proton Pump Inhibitors” [MeSH] OR “PPI” [MeSH] OR “Esomeprazole” [MeSH] OR “Lansoprazole” [MeSH] OR “Omeprazole” [MeSH] OR “Pantoprazole” [MeSH] AND “Gastrointestinal bleeding” [MeSH] OR “Peptic Ulcer Bleeding” [MeSH] AND “Randomized Controlled Trial” [MeSH] OR “RCT”. The search strategy is shown in detail in Supplementary list 1.
This was a meta-analysis of previously published studies, and ethical approval and informed consent were therefore not required.
Inclusion and exclusion criteria
We included RCTs written in English, regardless of whether or not specific random allocation methods were mentioned and distribution scheme hiding and blinding methods, with no limits on the date of publication. We included studies of patients who received endoscopic hemostasis within 24 hours after admission and who were treated with PPIs for bleeding caused by digestive tract ulcers. Studies were not limited by age or sex. The observation group included patients treated with continuous high-dose PPIs, i.e. an initial dose of 80 mg followed by 8 mg/hour for 72 hours. Patients in the control group received a routine dose of PPIs by intermittent intravenous drip. No other drugs were used in either group. The main outcome indicator was the incidence of postoperative re-bleeding (including hematemesis or hematochezia), and secondary indicators included surgical intervention, re-transfusion, length of hospital stay, and postoperative mortality.
We entered the retrieved literature from the databases into EndNote and eliminated duplicate documents. We then read the titles and abstracts according to the PICOS principles for preliminary screening, and then read the full texts of the relevant articles. We excluded articles reporting reviews, case reports, letters, minutes of meetings, animal trials, patients without endoscopic hemostasis, and patients with gastrointestinal bleeding due to stress, hematopathy, and malignant neoplasms.
Data extraction and methodological quality evaluation
The data were extracted and evaluated by two staff members during the study period and any differences were resolved by negotiation. We extracted the following data: (1) title, name of first author, and date of publication; (2) numbers of cases in high-dose and low-dose groups, types and methods of drug administration, including dosage; (3) Incidences of primary outcome of postoperative rebleeding (including hematemesis or hematochezia), and secondary indicators including surgical intervention, re-transfusion, length of hospital stay, and postoperative mortality. The quality of the studies was evaluated using the Cochrane risk of bias (ROB 2.0) tools.
Statistical analysis
This meta-analysis was conducted using RevMan 5.3 software provided by the Cochrane Cooperative Network. The effects of continuous data were presented as mean difference (MD), the effects of binary data as odds ratios (ORs), and the combined effect was expressed by each effect amount with 95% confidence intervals (CIs). The validity of the fixed-effect model was assessed by study heterogeneity within each pairwise comparison. The degree of heterogeneity was quantified using Cochran’s Q and Higgin’s I2 statistic, before the combined data were subjected to meta-analysis. If there was no heterogeneity (P ≥ 0.05 or I2 ≤ 50%), the combined statistics were calculated using a fixed effect model. If there was significant heterogeneity among the groups (P < 0.05 or I2 > 50%), 12 the source of heterogeneity was analyzed and subgroup analysis of the factors causing the heterogeneity was carried out.
Results
Literature search results
A flow chart of the literature search is shown in Figure 1. After removing 21 duplicate studies, we identified 876 studies using the above search strategy. A further 838 were excluded as case reports, editorials, letters, meeting abstracts, review articles, and non-human studies through screening of the titles and abstracts. The full texts of the remaining 38 citations were assessed in more detail to determine their eligibility. Among these, 16 studies were excluded because they were not RCTs, two were excluded as guidelines or recommendations, five were excluded due to a lack of available data, five were excluded as citations or news releases, and three were excluded as meta-analyses. The remaining nine studies were included in the final data synthesis.13–21 The characteristics of the included studies are shown in Table 1.
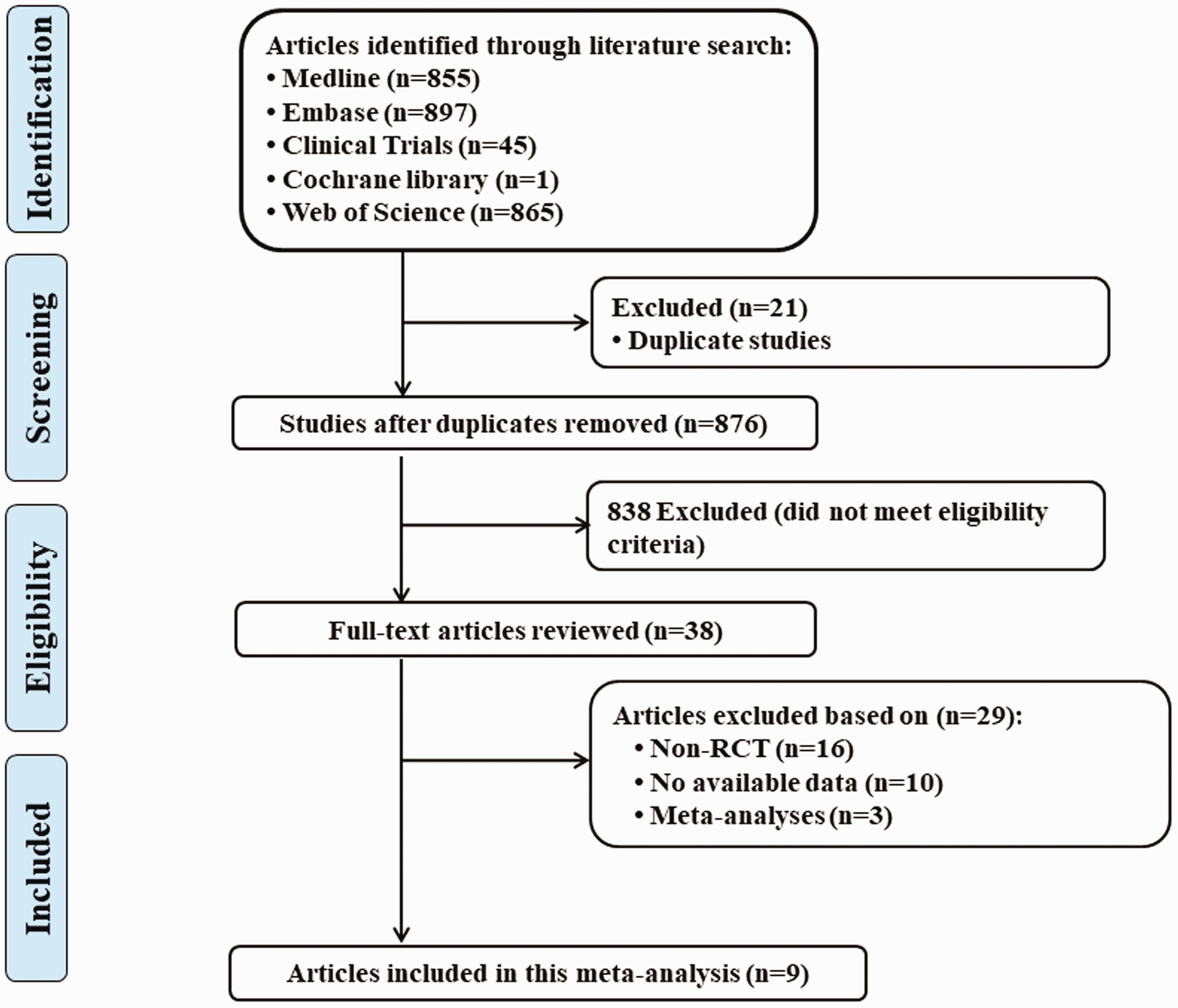
Flow diagram of the study selection process.
Characteristics of included studies.

Incidences of 1) re-bleeding; 2) operation intervention; 3) blood transfusion; 4) hospital stay; 5) postoperative mortality.
Study quality and risk bias
We evaluated the risk of bias for each study using Cochrane RevMan 5.3 software (Figure 2). Most studies showed a low risk of bias. We found no risk of bias.
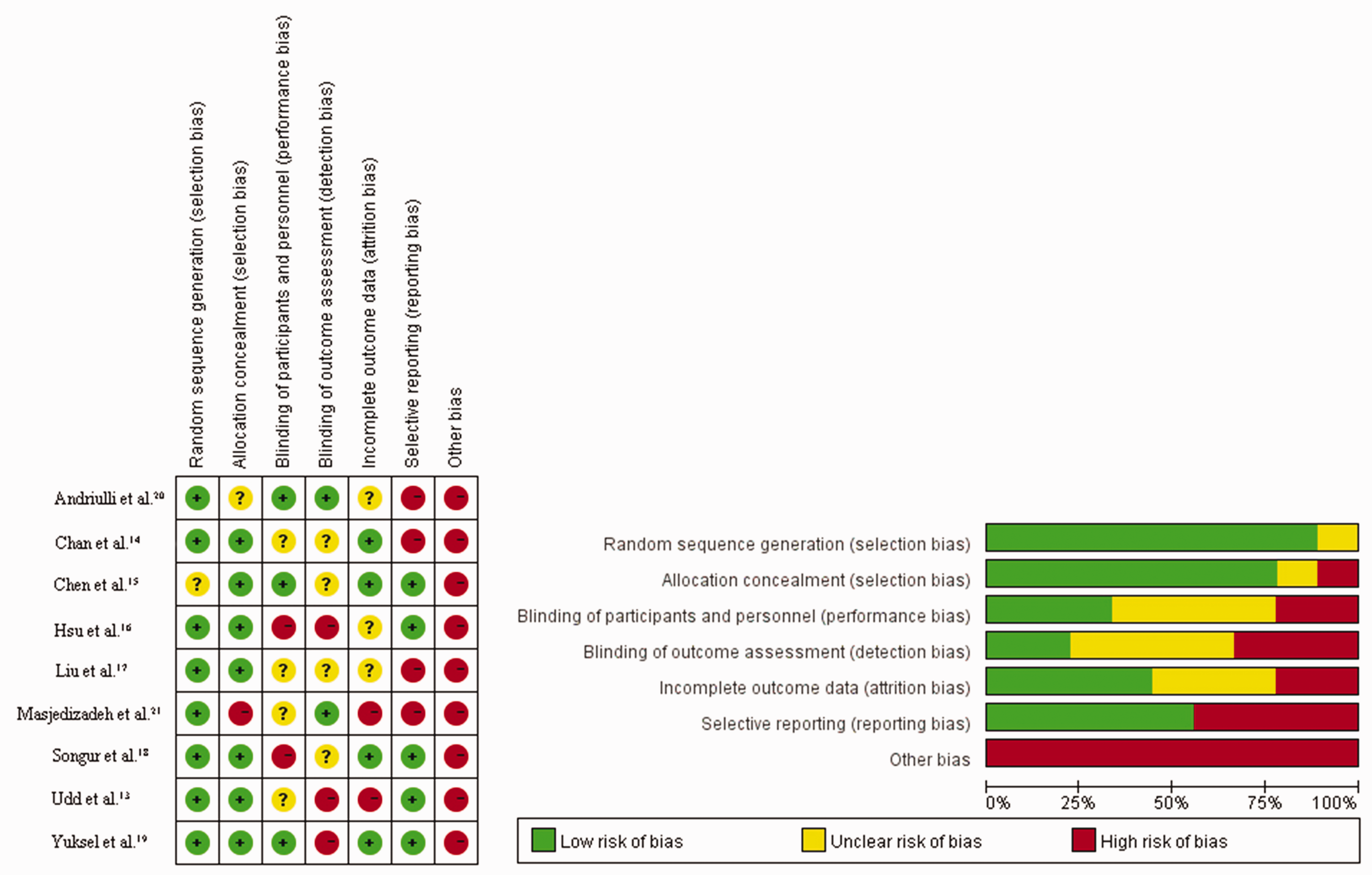
Risk of bias of the included randomized controlled trials.
Primary outcome: rebleeding
The incidences of rebleeding in patients treated with high-dose compared with low-dose PPIs for gastrointestinal ulcer bleeding are shown in Figure 3a. The incidence of re-bleeding was reported in all nine included articles, including 2321 patients. The results of heterogeneity testing showed no significant heterogeneity among the studies (P = 0.13, I2 = 36%), and there was no significant difference in the incidence of re-bleeding between the two groups (OR = 0.87, 95% CI = 0.65 to 1.15).

Forest plots of meta-analysis comparing intensive versus standard proton pump inhibitor regimens. (a) Re-bleeding; (b) operation intervention; (c) postoperative mortality; (d) hospital stays; (e) blood transfusion volume.
Secondary outcomes
The results of heterogeneity testing for operation intervention showed no significant heterogeneity among the studies (P = 0.74, I2 = 0%), and there was no significant difference in operation intervention between the two groups (OR = 0.86, 95% CI = 0.55 to 1.37) (Figure 3b).
The incidence of postoperative mortality was reported in all nine articles, including 2321 patients. Heterogeneity testing showed no significant heterogeneity among the studies (P = 0.59, I2 = 0%), and there was no significant difference in the incidence of postoperative mortality between the two groups (OR = 0.78, 95% CI = 0.43 to 1.40) (Figure 3c).
The length of hospital stay was reported in six articles. There was no significant heterogeneity among the studies according to heterogeneity testing (P = 0.39, I2 = 4%), and the results showed no significant difference in the incidence of re-bleeding between the two groups (MD = 0.33, 95% CI = −0.03 to 0.70) (Figure 3d).
Seven articles including 1326 patients reported the volume of blood transfusion. Heterogeneity testing showed no significant heterogeneity among the studies (P = 0.74, I2 = 0%). The results showed that the blood transfusion volume was significantly higher in the high-dose group (MD = 0.36, 95% CI = 0.11 to 0.61, P = 0.005) (Figure 3e).
Publication bias
There was no significant publication bias (Table 2).
Publication bias analysis of the meta-analysis.

CI, confidence interval.
Discussion
Endoscopic hemostasis is an effective treatment method for gastrointestinal ulcer bleeding. However, although it can reduce the incidence of re-bleeding and mortality to some extent, the continuous action of gastric acid may cause the clot to fall off, leading to re-bleeding. 22 Numerous studies have shown that decreasing the acidity and increasing the pH of gastric acid after surgery can significantly reduce the incidence of re-bleeding after endoscopic hemostasis.15,16,23 Gastric acid excretion in the stomach is proportional to the number of parietal cells, which also determines the number of active proton pumps. 24 Recent studies have shown that intravenous PPIs can significantly reduce the incidence of adverse events after surgery, but the optimal dosage and route of administration are still controversial.
The recommended high-dose PPI regimen is 80 mg + 8 mg/hour, i.e. an initial large dose (80 mg) of intravenous PPI followed by a continuous infusion of 8 mg/hour for 72 hours, which is referred to as the “808” treatment scheme. 25 In the treatment of peptic ulcer bleeding using this scheme, the stability of the PPI used for continuous intravenous drip is closely related to the pH of the drug solution, and the stability of the solution is also influenced by metal ions, light, temperature, and even the packing materials used in the infusion.26,27 The stability of the drug and its solution are therefore important considerations when high doses of PPIs are used, as in the “808” protocol, and the preparation requirements and storage conditions of the PPI must be understood. Continuous intravenous administration of PPIs also requires prolonged opening of the venous passage and nursing care by specialist nurses, and thus increases drug use and the risk of adverse drug reactions. After achieving the intended therapeutic purpose, it is therefore worth considering if the treatment can be reduced or provided on-demand.
PPI infusion therapy has been reported to be superior to placebo for the treatment of gastrointestinal ulcer bleeding.28–30 The aim of the current study was to compare high-dose versus low-dose PPIs in terms of the prognostic effects of the two methods on disease outcome and postoperative complications in patients with gastrointestinal ulcer bleeding. A meta-analysis of the available data found no significant differences between the two groups in terms of the incidence of postoperative re-bleeding, surgical intervention, postoperative mortality, and hospital stay, but the volume of blood transfusion differed significantly between the two groups. The volume of blood transfusion in the high-dose group was higher than that in the low-dose group, indicating that high-dose PPIs might not have a better effect on gastrointestinal ulcer bleeding than low-dose PPIs. This result differed from the results of RCTs published in 2010 and 2018, which found that low-dose PPI treatment was equally effective to high-dose PPI treatment following endoscopic arrest of bleeding.31,32 As shown by Wang et al., 33 the current analysis found that high-dose PPIs had no effects compared with low-dose PPIs on the incidences of re-bleeding, operation intervention, postoperative mortality, and hospital stay in patients treated with endoscopic hemostasis of gastrointestinal bleeding, 33 while another study also found no difference between intermittent and continuous PPI therapy in patients with high-risk bleeding ulcers. 34
This meta-analysis also had some limitations. The results of the PPI therapy statistical heterogeneity were limited in RCTs, and the limited evidence of a dose-dependent effect of PPI therapy shed some doubt on the reliability of the findings. Second, the included studies were all published papers and grey literature was not analyzed, leading to possible publication bias. Third, the type and administration method of the PPIs used in the studies were not completely consistent, which may have increased the clinical heterogeneity. Fourth, some data could not be extracted and included in the meta-analysis because of limitations in the original data. Further clinical research and evaluation are therefore needed to verify the current results and to evaluate the effects of the two administration schedules on the prevention of postoperative long-term complications.
The current findings indicate that there is no significant difference between high-dose PPI infusion therapy and low-dose PPI treatment in terms of re-bleeding, duration of hospitalization, need for surgery, and mortality among patients receiving endoscopic hemostasis for gastrointestinal bleeding. However, further studies with well-designed rigorous trial plans are needed to increase the sample size, and the results need to be verified by more high-quality clinical studies with long-term follow-up.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211067396 - Supplemental material for Effects of high-dose versus low-dose proton pump inhibitors for treatment of gastrointestinal ulcer bleeding: a meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-1-imr-10.1177_03000605211067396 for Effects of high-dose versus low-dose proton pump inhibitors for treatment of gastrointestinal ulcer bleeding: a meta-analysis of randomized controlled trials by Wei Zhu, Liang Chen, Jian Zhang and Pei Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211067396 - Supplemental material for Effects of high-dose versus low-dose proton pump inhibitors for treatment of gastrointestinal ulcer bleeding: a meta-analysis of randomized controlled trials
Supplemental material, sj-pdf-2-imr-10.1177_03000605211067396 for Effects of high-dose versus low-dose proton pump inhibitors for treatment of gastrointestinal ulcer bleeding: a meta-analysis of randomized controlled trials by Wei Zhu, Liang Chen, Jian Zhang and Pei Wang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
There are no conflicts of interest. This manuscript will be registered in PROSPERO in the future.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.