
Abstract
Background:
Currently, no guidelines specifically recommend scoring systems and biomarkers for early evaluation of the severity and prognosis of acute pancreatitis in pregnancy (APIP).
Objectives:
This study aimed to explore the early predictive value of scoring systems and routine laboratory tests on APIP severity and maternofetal prognosis.
Design:
This study retrospectively analyzed 62 APIP cases in a 6-year period.
Methods:
The predictive value of scoring systems and routine laboratory tests that were collected 24 h and 48 h after admission, for APIP severity and fetal loss, were analyzed.
Results:
To detect severe acute pancreatitis (SAP), a 24-h Bedside Index for severity in acute pancreatitis (BISAP) achieved a higher area under the curve (AUC) value of 0.910 than the Acute Physiology and Chronic Health Evaluation II (AUC = 0.898) and Ranson score (AUC = 0.880). The combination of BISAP, glucose, neutrophil-to-lymphocyte ratio (NLR), hematocrit (Hct), and serum creatinine (Scr) provided an AUC value of 0.984, which had greater predictive power than BISAP (p = 0.015). 24-h BISAP and Hct were independent risk factors for predicting SAP of APIP. The cutoff values of Hct and blood urea nitrogen (BUN) to predict SAP were 35.60% and 3.75 mmol/l in the APIP. Furthermore, 24-h BISAP had the highest predictive power (AUC = 0.958) for fetal loss.
Conclusion:
BISAP is a convenient and reliable indicator for the early prediction of SAP and fetal loss in APIP. The combination of BISAP, glucose, NLR, Hct and Scr proved to be the optimal early markers for the prediction of SAP in APIP within 24 h after admission. In addition, Hct > 35.60% and BUN > 3.75 mmol/l may be suitable thresholds for predicting SAP in APIP.
Keywords
Introduction
Acute pancreatitis in pregnancy (APIP) is a rare serious disease which may result in pancreatic necrosis, abscess, and multiple organ dysfunction, leading to other adverse maternofetal outcomes. The high maternal–fetal mortality of APIP has recently decreased due to early diagnosis, recognition of acute pancreatitis (AP) severity, and improvements in maternal and neonatal intensive care. A recent meta-analysis demonstrated that the maternal mortality rate following APIP was reduced from 3.3% in 2010−2015 to 2.8% in 2016−2020 and the fetal mortality rate reduction was 12.6% from 13%. 1 Nonetheless, the fetal death rate secondary to APIP is still among the highest fetal mortality rates for surgical emergencies that may occur during pregnancy, compared to other pathologies, including 1.6% for simple appendicitis, 7% for non-operative management of cholecystitis, and 17% for small bowel obstruction.2–4 APIP is more harmful to the fetus than to pregnant women.
Early and rapid assessment of the severity of APIP, prediction of severe AP (SAP), and the occurrence of complications are very important to improve the outcomes of the mother and fetus. At present, several clinical scoring systems can help evaluate the severity of AP. The Acute Physiology and Chronic Health Evaluation II (APACHE II), Bedside Index for severity in acute pancreatitis (BISAP) score, and Ranson criteria are utilized in routine clinical practice worldwide. However, there are still certain limitations to their practical application, such as specific time constraints, many scores, and complex processes. 5 Therefore, novel and uncomplicated predictors are needed to complement these scoring systems.
Laboratory test markers, including C-reactive protein (CRP), blood urea nitrogen (BUN), serum creatinine (Scr), blood calcium, and procalcitonin (PCT) can reflect the severity of moderately SAP (MSAP) and SAP, and these are recommended to be monitored in Chinese guidelines for the management of AP. 6 Hematocrit (Hct), BUN, and 72-h CRP levels in laboratory tests are related to the severity of AP, but the accuracy is insufficient. 7 Studies have shown that neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are indicators that can reflect the inflammatory state and coagulation function of the body, and these indicators have been widely used in the prediction of the condition of many diseases in recent years.8,9 A study found that the PLR-NLR combination had similar prognostic significance to other scoring systems for evaluating the prognosis of AP. 10
However, AP during pregnancy is different from that in general patients. Are these scoring systems and laboratory indicators valuable for the evaluation of APIP severity and prognosis in the early stages? To date, scoring systems specially designed for APIP that consider the physiological conditions of pregnant patients are still lacking. Therefore, it is necessary to identify early predictors of SAP in patients with APIP.
Our study extracted and analyzed clinical data of previously admitted patients to explore the value of various scoring systems and routine laboratory tests to evaluate the severity and prognosis of APIP in the early stage of admission to help clinical medical staff quickly assess the severity of APIP and maternofetal prognosis and make a decision on the treatment of AP as soon as possible. Our study aimed to identify the optimal early predictors for the severity and prognosis of APIP and help reduce maternofetal mortality and morbidity.
Methods
Study design and patient selection
This study retrospectively analyzed the clinical data of patients with AP from the First Affiliated Hospital of Anhui Medical University, Hefei, China, from January 2016 to December 2021. Patients with APIP were included in the study. The inclusion criterion was AP diagnosed during pregnancy. Male patients with AP, female patients with AP with no pregnancy, and patients with APIP with insufficient medical data records were excluded. This study conformed to the STROBE statement. 11
Diagnosis and definitions
According to the 2012 revised Atlanta Criteria for AP, 12 the diagnosis of AP requires two of the following three features: abdominal pain consistent with AP (acute onset of a persistent, severe, epigastric pain often radiating to the back); serum lipase level or serum amylase level (at least three times greater than the upper limit of the normal), and findings consistent with AP on imaging [contrast-enhanced CT, MRI, or abdominal ultrasound).
Hypertriglyceridemia-induced AP qualified the following criteria: serum triglyceride (TG) > 11.3 mmol/L or between 5.65 and 11.3 mmol/L but with a lipemic serum, and in the absence of biliary disease, alcohol, or medication abuse. 13 Acute biliary pancreatitis was defined as AP associated with gallstones or sludge in the biliary tree or the gallbladder. Alcoholic pancreatitis, pancreatitis associated with a high-fat diet, acute exacerbation of chronic pancreatitis, infectious pancreatitis, pancreatitis caused by sphincter of Oddi dysfunction, and pancreatitis of idiopathic etiology were classified under the category ‘other etiology’.
Outcomes
The primary outcome was the early predictive value of the scoring systems and routine laboratory tests for the severity of APIP. The second outcome was the early predictive value of the scoring systems and routine laboratory tests for fetal loss in APIP.
Patients were divided into three groups according to APIP severity. Mild AP (MAP) had no organ failure or local or systemic complications. MSAP was defined as the presence of transient organ failure within 48 h and/or local or systemic complications without persistent organ failure. SAP was defined as persistent organ failure (organ failure > 48 h). 12
In addition, according to fetal outcome, patients were divided into fetal loss and no fetal loss groups.
Fetal loss included abortion, fetal demise, and stillbirth. In China, abortion refers to the termination of pregnancy at less than 28 weeks and fetal weight less than 1000 g. 14 Fetal death in utero occurring after 20 weeks of gestation is classified as fetal demise or stillbirth. 15
Low birthweight infants refer to newborns weighing less than 2500 g within 1 h after birth. 16
Data collection
Demographic information, body mass index (BMI), complications, history of gestational diabetes, and gestational hypertension were collected from medical records. Initial routine laboratory tests and arterial blood gas analysis were performed 24 and 48 h after admission. Complete blood count was examined using an automatic analyser (SySMex XN9000, Sysmex Corporation, China). Biochemistry, including blood glucose, lipids, and electrolytes, was performed using an automatic biochemical analyser (Cobas 8000, Roche Limited, Switzerland). Arterial blood gas analysis was performed using an automatic analyser (i-STAT 300-G; Abbott Limited, USA).
The BISAP and APACHE II scores were evaluated in the first 24 h, and the Ranson score was calculated at 48 h after admission.
Statistical analysis
Continuous data were first examined for normal distribution using the Kolmogorov–Smirnov test. Non-normal data were represented as median and quartile; otherwise, mean and standard deviation were used. Discontinuous data are presented as numbers and percentages. The characteristics of pregnant women and their offspring were compared between groups with different severities of pancreatitis using one-way analysis of variance or Kruskal–Wallis tests. p Values of multiple comparisons between groups were corrected using the Bonferroni method. To assess the predictive power of the scoring systems and laboratory tests on the presence of SAP and fetal loss, receiver operating characteristic (ROC) curves were drawn to calculate the area under the curve (AUC) and determine the optimal cutoff value. Based on the optimal cutoff value, the sensitivity, specificity, and Youden index were calculated to assess the diagnostic value. For the significant predictors in ROC, logistic regression analyses with and without adjusting for confounding factors were also performed to examine the association between SAP and fetal loss which was represented by odds ratios (ORs) and 95% confidence intervals (95% CI). All analyses were performed using SPSS software version 24.0. All tests were two-sided, and p value < 0.05 represents statistical significance.
Results
In this study, 2985 patients with AP admitted to the First Affiliated Hospital of Anhui Medical University from January 2016 to December 2021, after excluding patients who met the exclusion criteria for patient selection, 62 patients with APIP were finally included (Figure 1), with an average age of 29.60 ± 5.16 years. Among them, 21 (33.9%) were diagnosed as MAP, 28 (45.1%) as MSAP, and 13 (21.0%) as SAP. During this period, 35,749 pregnant women were admitted to the same hospital, and APIP occurred in 64 women. The incidence of APIP was 17.9 cases per 10,000 pregnant women (64/35,749).
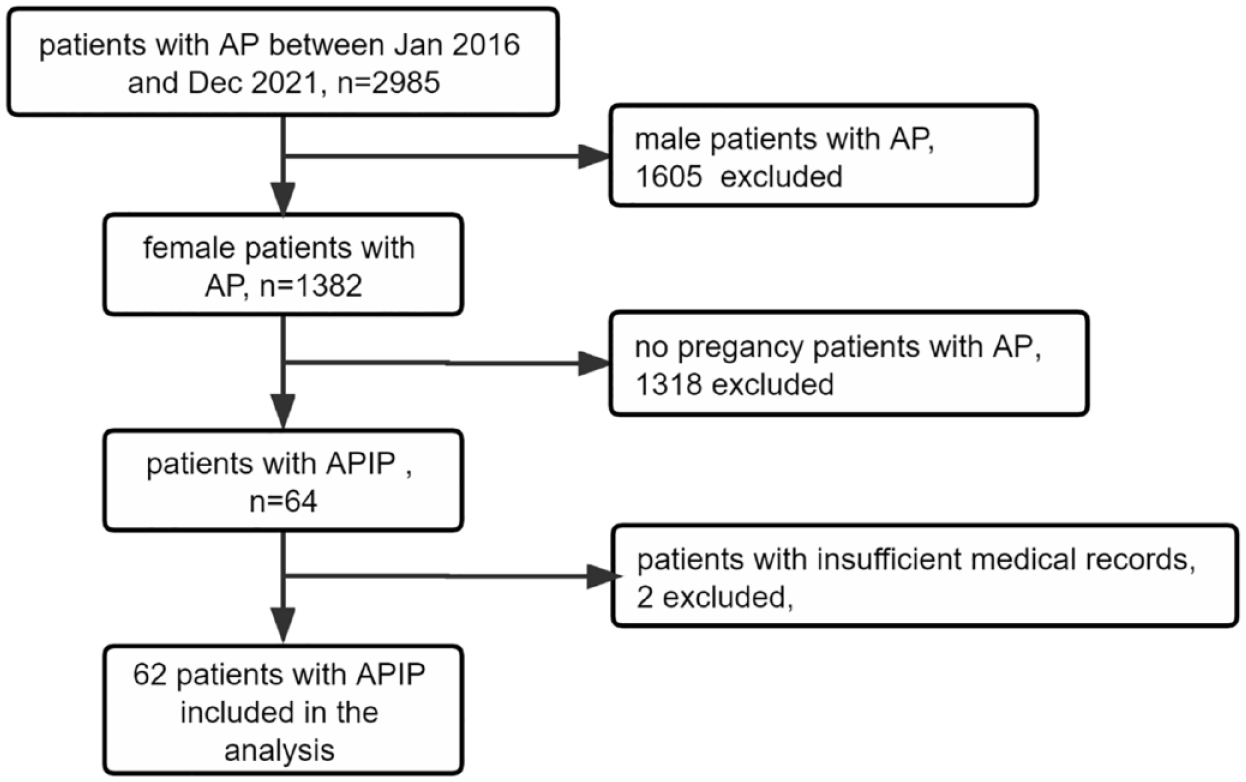
Study participant selection.
No patient with APIP died in this study. As shown in Table 1, there were significant differences in the 24-h APACHE-II score, 24-h BISAP score, 48-h Ranson score between the three groups, and patients with SAP showed higher scores. For laboratory tests, the levels of NLR, PLR, Albumin, TCH, and TG in 24 h after admission showed significant differences among the three groups. The 24-h Hct level of SAP group was significantly increased compared to MSAP group. The levels of 24-h glucose in SAP group and 72 h CRP in the MSAP group were both significantly higher than those in the MAP group.
Characteristic of patients with APIP.
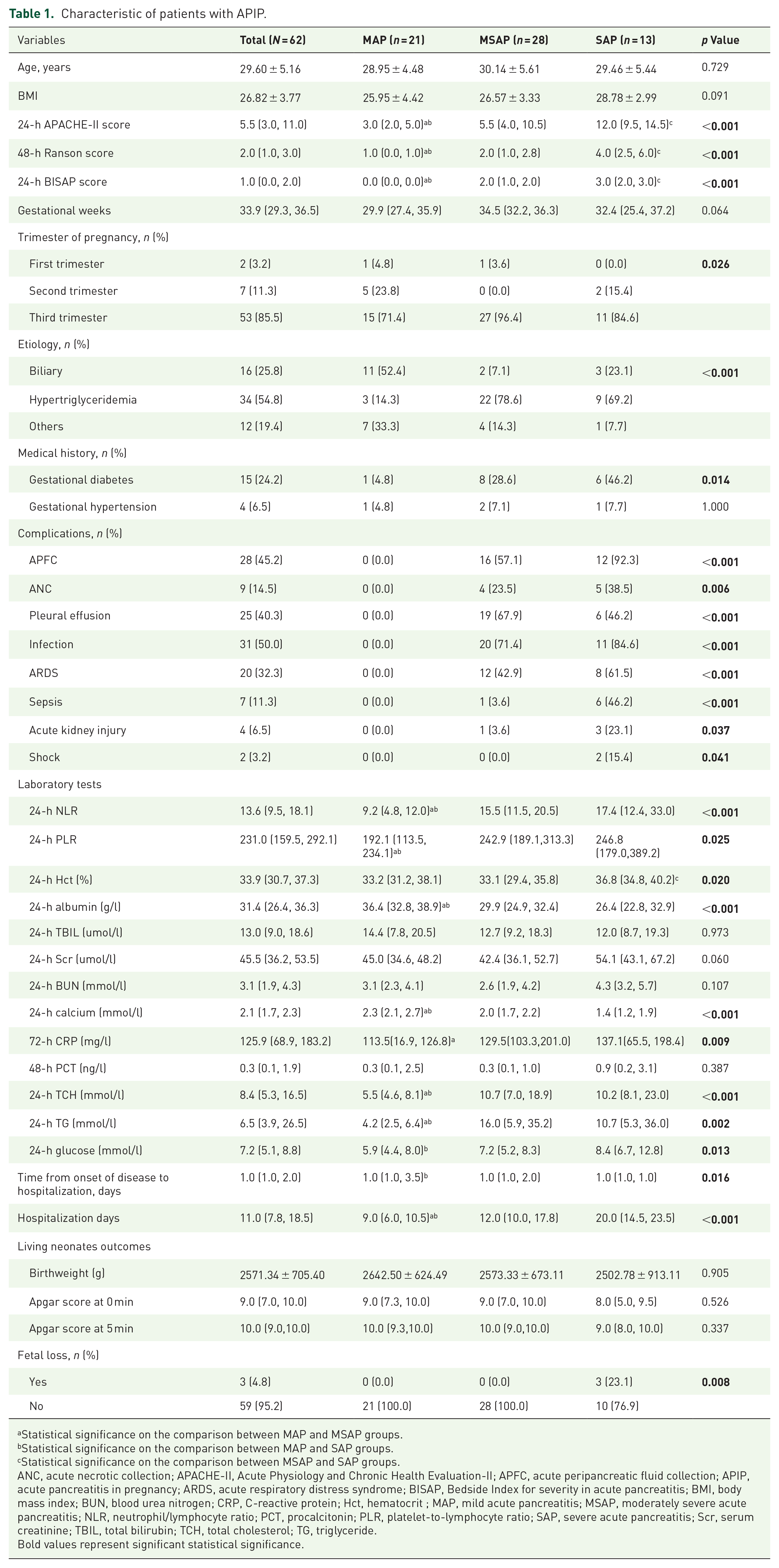
Statistical significance on the comparison between MAP and MSAP groups.
Statistical significance on the comparison between MAP and SAP groups.
Statistical significance on the comparison between MSAP and SAP groups.
ANC, acute necrotic collection; APACHE-II, Acute Physiology and Chronic Health Evaluation-II; APFC, acute peripancreatic fluid collection; APIP, acute pancreatitis in pregnancy; ARDS, acute respiratory distress syndrome; BISAP, Bedside Index for severity in acute pancreatitis; BMI, body mass index; BUN, blood urea nitrogen; CRP, C-reactive protein; Hct, hematocrit ; MAP, mild acute pancreatitis; MSAP, moderately severe acute pancreatitis; NLR, neutrophil/lymphocyte ratio; PCT, procalcitonin; PLR, platelet-to-lymphocyte ratio; SAP, severe acute pancreatitis; Scr, serum creatinine; TBIL, total bilirubin; TCH, total cholesterol; TG, triglyceride.Bold values represent significant statistical significance.
For the fetal outcome, a total of three patients in the SAP group had fetal loss and the other patients had no fetal loss. One fetal loss with a gestational age of 33 weeks occurred prior to admission, and the other two fetal demises occurred after admission with a gestational age of 22.9 and 31 weeks, respectively. The comparison between patients with and without fetal loss showed that patients with fetal loss had higher BMI, 24-h APACHE-II score, 24-h BISAP score, and higher prevalence of acute respiratory distress syndrome, sepsis, acute kidney injury, and shock. However, only 24-h Calcium and PCT levels showed significant differences between patients with and without fetal loss in laboratory tests (Table 2).
Characteristic of APIP patients with different fetal outcomes.

ANC, acute necrotic collection; APACHE-II, Acute Physiology and Chronic Health Evaluation-II; APFC, acute peripancreatic fluid collection; APIP, acute pancreatitis in pregnancy; ARDS, acute respiratory distress syndrome; BISAP, Bedside Index for severity in acute pancreatitis; BMI, body mass index; BUN, blood urea nitrogen; CRP, C-reactive protein; Hct, hematocrit; na, not applicable; NLR, neutrophil/lymphocyte ratio; PCT, procalcitonin; PLR, platelet-to-lymphocyte ratio; Scr, serum creatinine; TBIL, total bilirubin; TCH, total cholesterol; TG, triglyceride.Bold values represent significant statistical significance.
For living neonates, there was no significant difference in the prevalence of premature delivery, low birthweight, Apgar score at 0 min, and Apgar score at 5 min in the different severity groups (Supplemental Table S1).
For the predictive power of the scoring systems, the ability of the 24-h BISAP score to predict SAP was the highest (AUC = 0.910, 95% CI: 0.834–0.986, p < 0.001), followed by the 24-h APACHE-II score (AUC = 0.898, 95% CI: 0.822–0.974, p < 0.001) and 48-h Ranson score (AUC = 0.880, 95% CI: 0.767–0.993, p < 0.001). For the predictive power of laboratory tests, 24-h glucose showed the highest predictive ability (AUC = 0.749, 95% CI: 0.600–0.898, p = 0.006) and moderate sensitivity (0.615) and specificity (0.776). Albumin had the highest sensitivity (1.000) and lowest specificity (0.02) (Table 3). Thus, the 24-h BISAP score is probably a suitable early predictive marker for SAP in APIP.
Variables for predicting SAP in the patients with APIP.

APACHE-II, Acute Physiology and Chronic Health Evaluation-II; APIP, acute pancreatitis in pregnancy; BISAP, Bedside Index for severity in acute pancreatitis; BUN, blood urea nitrogen; CRP, C-reactive protein; Hct, hematocrit; NLR, neutrophil/lymphocyte ratio; PCT, procalcitonin; PLR, platelet-to-lymphocyte ratio; SAP, severity in acute pancreatitis; Scr, serum creatinine; TBIL, total bilirubin; TCH, total cholesterol; TG, triglyceride.Bold values represent significant statistical significance.
In addition, among all 24-h laboratory test markers, the AUC of NLR, Hct, Scr, and glucose were all above 0.7. Therefore, we combined the BISAP score and these laboratory markers for SAP prediction, and the AUC for the combination curve was 0.984 (95% CI: 0.952–1.000, p < 0.001), which significantly increased the predictive power compared to the single BISAP score (p = 0.015) (Figure 2).

The ROC curve for the BISAP score and its combination with laboratory test biomarkers for SAP in APIP prediction.
For the predictive power of scoring systems for fetal loss, the ability of 24-h BISAP score was the highest (AUC = 0.958, 95% CI: 0.905–1.000, p = 0.008), followed by the 24-h APACHE-II score (AUC = 0.944, 95% CI: 0.864–1.000, p = 0.01) (Table 4). However, among all laboratory tests, only 24-h PCT showed good predictive power (AUC = 0.893, 95% CI: 0.713–1.000, p = 0.023) (Table 4).
Variables for predicting fetal loss in the patients with APIP.
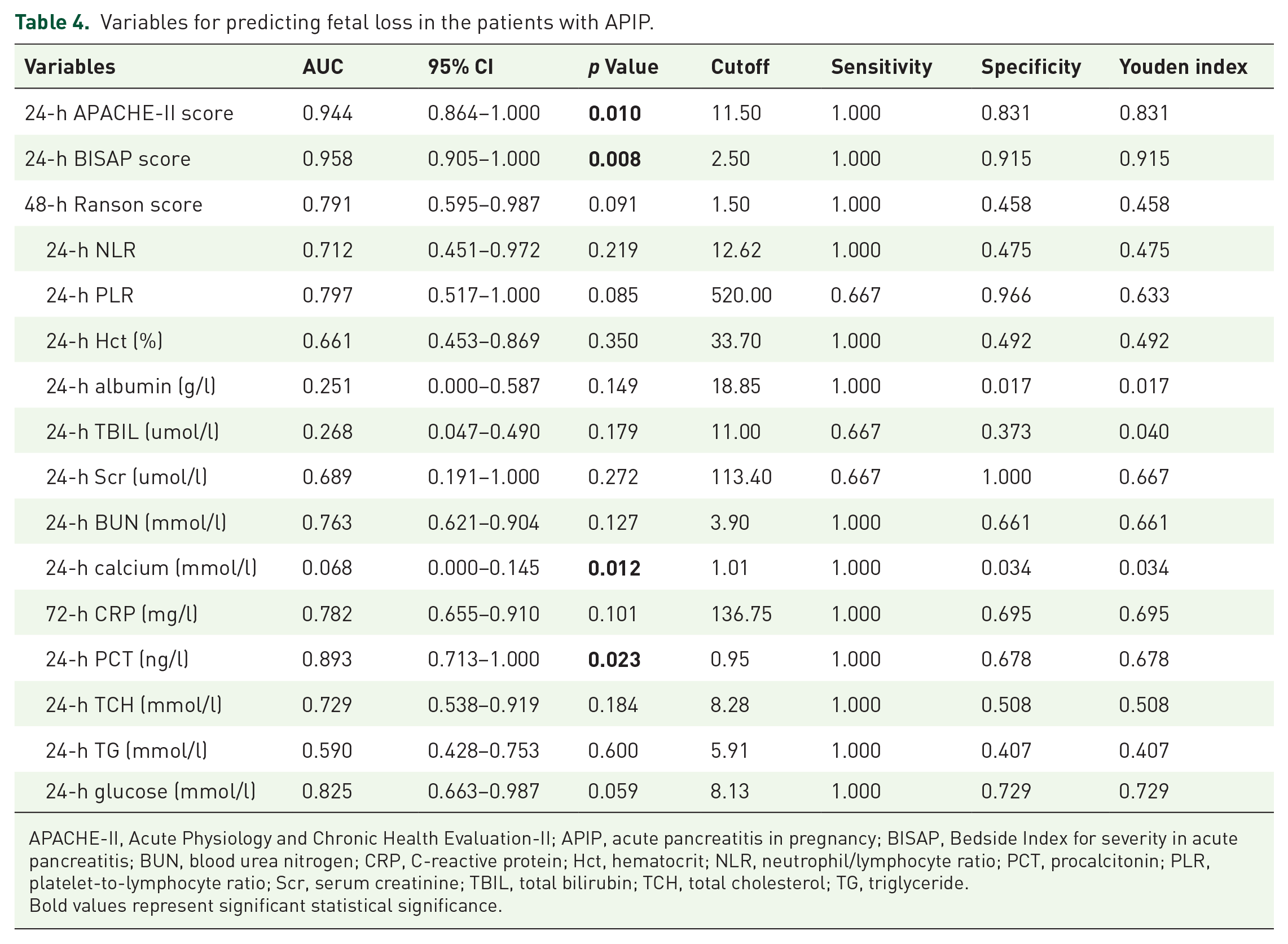
APACHE-II, Acute Physiology and Chronic Health Evaluation-II; APIP, acute pancreatitis in pregnancy; BISAP, Bedside Index for severity in acute pancreatitis; BUN, blood urea nitrogen; CRP, C-reactive protein; Hct, hematocrit; NLR, neutrophil/lymphocyte ratio; PCT, procalcitonin; PLR, platelet-to-lymphocyte ratio; Scr, serum creatinine; TBIL, total bilirubin; TCH, total cholesterol; TG, triglyceride.Bold values represent significant statistical significance.
All significant predictors of SAP, except 24-h BUN, were significantly associated with the risk of SAP in the univariate analysis (Table 5).
Results of logistic analysis on factors associated with SAP in the pregnant women.

Model 1 was unadjusted model.
Model 2 adjusted for age, BMI, gestational weeks, diabetes, hypertension.
APACHE-II, Acute Physiology and Chronic Health Evaluation-II; BISAP, Bedside Index for severity in acute pancreatitis; BUN, blood urea nitrogen; Hct, hematocrit; NLR, neutrophil/lymphocyte ratio; SAP, severity in acute pancreatitis; Scr, serum creatinine.Bold values represent significant statistical significance.
After adjusting for age, BMI, gestational weeks, diabetes, hypertension, 24-h APACHE-II score (OR = 1.47, 95% CI: 1.15–1.89, p = 0.002), 48-h Ranson score (OR = 7.15, 95% CI: 1.88–27.27, p = 0.004), and 24-h BISAP score (OR = 25.80, 95% CI: 2.07–321.92, p = 0.012) were positively associated with SAP (Table 5). However, among the laboratory markers, only 24 Hct (OR = 1.20, 95% CI: 1.00–1.44, p = 0.047) and 24-h calcium (OR = 0.03, 95% CI: 0.01–0.32, p = 0.003) were significantly associated with SAP (Table 5). In univariate analysis, 24-h APACHE-II score (OR = 1.41, 95% CI: 1.07–1.86, p = 0.014) and 24-h PCT (OR = 1.80, 95% CI: 1.02–3.17, p = 0.041) showed a positive association with fetal loss (Supplemental Table S2).
Discussion
At present, there are no guidelines specifically recommending scoring systems and laboratory tests for early evaluation of the severity and prognosis of APIP. Scoring systems for APIP have not been widely reported. To the best of our knowledge, very few studies have compared the value of various scoring systems and routine laboratory tests in the evaluation of the severity and prognosis of APIP in the early stage of admission. The BISAP, APACHE II, and Ranson scores are recommended to evaluate the severity and prognosis of AP by the Chinese guideline. 17 Previous studies reported that BISAP was as good as APACHE II score and outperformed Ranson criteria in predicting the severity and death of AP.18,19 Chandra’s study demonstrated that BISAP had accurate performance for SAP across different patient populations and etiologies. 20 Our study reported that the ability of the 24-h BISAP score to predict SAP of APIP was better than 24-h APECHE II score and 48-h Ranson score. Furthermore, the combination of BISAP score, glucose, NLR, Hct, and Scr proved to be the optimal early marker for predicting SAP of APIP at a very early timepoint (24 h).
The Ranson score needs to be evaluated 48 h after admission to predict the severity; therefore, it has a certain delay in the evaluation of APIP. In addition, the APACHE II requires 12 variables that are not routinely obtained in patients who are not critically ill. It is complex and difficult to implement fully. Our study reported 24-h BISAP had a higher predictive power for SAP and was positively associated with SAP of APIP. However, we also observed that a variable in BISAP depending on age (⩾60 years) was not suitable for patients with APIP because of the normal age range for pregnancy (<50 years). Pregnant women cannot obtain score for this variable in BISAP. Furthermore, owing to the special physiological conditions of pregnant women, the BUN content of pregnant women is lower than that of the normal population. 21 The BISAP score calculated using the BUN value of APIP patients may have low scores, which affects the accuracy of the BISAP score in the evaluation of severity.
To overcome the limitations of most scoring systems and find a more effective marker for early prediction of APIP severity, we also compared the predictive values of routine laboratory tests at 24 h after admission. This study reported that a higher BUN level showed a predictive value for SAP, with a cutoff value of 3.75 mmol/l, which is much lower than that of BUN in the BISAP score (8.9 mmol/l). Similar to our study, a study of 100 cases of APIP revealed that an increase in BUN with a cutoff value of 4.1 mmol/l was related to SAP. 22 Therefore, we suggest that the variable of BUN level in scoring systems be modified according to the optimal threshold of BUN for SAP prediction in APIP. This study found BUN >3.75 mmol/l as a prediction threshold of SAP in APIP and a reference for improving APIP scoring systems in the future.
This study further indicated that the levels of NLR, Hct, albumin and glucose 24 h after admission showed significant differences between the three groups and predicted SAP in APIP. 24-h Hct and calcium levels were significantly associated with SAP and were independent risk factors for predicting SAP in APIP. A previous study of 1612 patients with AP showed that admission Hct ⩾ 44% and rise in BUN at 24 h may be the optimal predictive tools in clinical practice among existing laboratory parameters and scoring systems. 23 Chinese guidelines for the management of AP have recommended that Hct > 44% is an independent risk factor for predicting pancreatic necrosis. 6 However, our study reported that the cutoff value of Hct to predict SAP was 35.60% in APIP. A likely explanation for this finding is that the Hct of pregnant women is reduced under special physiological conditions, which may cause a low figure. Estimates based on Hct > 44% in the current guidelines for AP may underestimate APIP severity. We suggest that Hct > 35.60% may be the optimal threshold for predicting SAP in patients with APIP.
NLR integrates two opposite and complementary components of the immune pathway, representing the balance between inflammatory activator neutrophils and inflammatory regulator lymphocytes. 24 Recently study reported that NLR had a predictive value in evaluating the severity and prognosis of AP, similar to some scoring systems. The BISAP score and NLR can be used as early determinants of AP severity and mortality, and NLR has no lower prognostic value than the BISAP score. 25 Ilhan reported that NLR can be used as an early indicator to predict the severity of AP based on 14 patients with APIP without the severity classification. 26 Differently to previous studies, to explore the most accurate predictor, the 24-h NLR, Hct, Scr, glucose, and BISAP score were combined in this study and achieved the highest predictive ability of SAP in APIP. Since the combination is convenient, quick, and non-invasive to obtain in hospitals and emergency departments in many countries and regions within 24 h after admission, it is probably the optimal early marker for predicting the severity of APIP. We suggest that this combination be used in the early evaluation of SAP severity in APIP.
In addition, our study based on 62 cases demonstrated that fetal loss was the highest in the SAP group and the 24-h BISAP score had the highest predictive value for fetal loss. 24-h Calcium and 24-h PCT also predicted the value of fetal loss in APIP. PCT is currently a sensitive marker for detecting pancreatic infection. 27 A previous study of 54 cases reported the incidence of fetal distress and fetal loss increased with the progression of severity of APIP. 28 Sun et al. 29 suggested the indications of termination of pregnancy include full-term gestation, severe pancreatitis, deteriorated condition after 24–48 h of treatment, no improvement of paralytic ileus, stillbirth, and fetal malformation. Since the complications of different stages of prematurity were targeted, this study further reported that 44 cases of APIP had termination of pregnancy and 41 neonates survived, and there was no significant difference in low birth weight and Apgar score among living neonates in different severity groups. The organs of premature infants are not well developed, the lower the gestational age, the lighter the weight. 30 Low birthweight in APIP may be caused by premature delivery in this study. The timing of pregnancy termination in patients with APIP is important for minimizing fetal loss. Therefore, the BISAP score, PCT, and calcium levels need to be monitored in the early stage of admission to evaluate the severity of APIP and take effective treatment measures as soon as possible to improve the prognosis of pregnant women and fetuses.
Moreover, our data confirmed that the incidence of APIP was 17.9 cases per 10,000 pregnant women which was higher than the 20.02/100,000 person-years reported in the study by Maruinghini A. 31 The most common cause of APIP was hypertriglyceridemia (54.8%), and the incidences of MSAP and SAP were higher than those of hypertriglyceridemic APIP. A previous study reported that the most common causes of APIP were gallstone (36.4%) and hypertriglyceridemia (32.2%), but hypertriglyceridemic APIP was correlated with a higher rate of local complication. 32 In addition, 24-h glucose showed the highest predictive ability, with moderate sensitivity and specificity of SAP in this study. In recent years, the incidence of hypertriglyceridemic APIP has increased significantly, which is related to the high-fat diet in pregnant women, leading to an increase in TG and cholesterol levels and pancreatic microcirculation disorders. Free fatty acids directly damage pancreatic acinar cells; furthermore, trypsinogen is activated, aggravating pancreatic self-digestion and damage.33,34 This may be related to the dietary habits of pregnant Chinese women. Pregnant Chinese women rarely drink alcohol but often consume a high-fat and high-calorie diet. Therefore, a healthy diet, less fat intake, and blood glucose levels should be strictly controlled during pregnancy, especially in pregnant women with hyperlipidemia and gestational diabetes. In this study, biliary APIP ranked second (25.8%); therefore, it was advisable to relieve the relevant risk factors before pregnancy for patients with previous biliary tract diseases.
Limitations
There are also limitations to the analysis. First, this was a single-center, retrospective study with a small sample size owing to the low incidence of APIP, which might limit the worldwide application of the study results. Second, not all patients underwent arterial gas blood analysis in the medical records to evaluate APACHE II and Ranson scores. This may affect the accuracy of the scoring systems. Third, the levels of BUN, Scr, Hct, and albumin in pregnant women are reduced under special physiological conditions. 21 The optimal threshold value of these biomarkers for the prediction of severity in APIP is different from that of general AP. These scoring systems may be affected by a lower number of laboratory tests, resulting in a lower score. These factors may lead to an inaccurate evaluation of APIP severity. Further studies concerning the optimal threshold value for these biomarkers are needed to improve the accuracy of the prediction of severity and outcome in APIP.
Conclusion
In conclusion, BISAP is a convenient and reliable indicator for the early prediction of SAP and fetal loss in APIP. In addition, the combination of BISAP, glucose, NLR, Hct, and Scr proved to be the optimal early prediction of SAP of APIP 24 h after admission. The predictive threshold of biomarkers in APIP is different from that of general AP, which may affect the accuracy of the scoring systems. High-quality prospective studies are required to provide a sound basis for prediction to improve outcomes in these critical and special populations.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231167277 – Supplemental material for Early predictive value of scoring systems and routine laboratory tests in severity and prognosis of acute pancreatitis in pregnancy
Supplemental material, sj-docx-1-tag-10.1177_17562848231167277 for Early predictive value of scoring systems and routine laboratory tests in severity and prognosis of acute pancreatitis in pregnancy by Yu Wang, Guangbo Qu, Zhangbi Wu, Dongmei Tian, Wenbei Yang, Hongye Li, Yu Lu, GuangJun Meng and Hong Zhang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
This study was supported by The First Affiliated Hospital of Anhui Medical University. We appreciated the patients with the acute pancreatitis in pregnancy and their relatives for their willingness to participate and cooperate with the present study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.