
Abstract
Background:
Vedolizumab is a gut-selective anti-lymphocyte trafficking agent used to treat ulcerative colitis (UC) and Crohn’s disease.
Objectives:
We aimed to evaluate the effectiveness, safety, and durability of the therapeutic effect of vedolizumab after treatment discontinuation in a real-world cohort of patients with UC treated in Poland.
Design:
This was a multicenter, prospective study involving patients with moderate to severely active UC from 12 centers in Poland who qualified for reimbursed treatment with vedolizumab between February and November 2019.
Methods:
The primary endpoints were clinical response (⩾2-point improvement from baseline on partial Mayo score) and clinical remission (partial Mayo score 0–1), including steroid-free remission, at week 54. Other outcomes included response durability at 26 weeks after treatment discontinuation, identification of predictors of response and remission, and safety assessment.
Results:
In all, 100 patients with UC were enrolled (55 biologic naïve and 45 biologic exposed). At baseline, 68% of patients were on corticosteroids and 45% on immunomodulators. Clinical response was observed in 62% of patients, clinical remission in 50%, and steroid-free remission in 42.6% at week 54. Within 26 weeks after treatment discontinuation, 37% of patients who maintained response by week 54 relapsed. The decreased number of liquid stools and rectal bleeding and endoscopic response at week 14 were predictive factors for response at week 54. Time from diagnosis ranging 2–5 years, decreased stool frequency, and non-concomitant use of corticosteroids at baseline and at week 14 were predictive factors for remission at week 54. Partial Mayo score < 3 with no subscale score > 1 at week 54 was a predictive factor for durable response after treatment discontinuation. The rate of serious adverse events related to treatment was 3.63 per 100 patient-years.
Conclusion:
Vedolizumab is effective and safe in UC treatment in Polish patients. However, the relapse rate after the treatment cessation was high.
Registration:
ENCePP (EUPAS34119).
Keywords
Introduction
Ulcerative colitis (UC), belonging to a group of chronic immune-mediated conditions known as inflammatory bowel diseases, is a disorder of poorly defined etiology. 1 Genetic susceptibility, environmental factors, aberrant host immune responses, and intestinal dysbiosis are implicated in the multifactorial pathogenesis of UC.2,3 In the last three decades, there has been an increase in the global prevalence of the disease, and this trend is expected to continue in future, along with the associated healthcare and societal costs. 4
UC exacerbation hinders the performance of everyday activities, which can significantly reduce the health-related quality of life in patients, not to mention anxieties about an increased risk of developing cancer and potential indications for hospitalization, surgical procedure, or an ostomy. 5 According to the latest STRIDE-II recommendations, the short-term goal of therapy for UC is symptomatic response (normal stool frequency and absence of rectal bleeding); intermediate targets are symptomatic remission, normalization of CRP, and reduction in calprotectin; and the long-term goals are endoscopic healing, restoration of quality of life, and absence of disability. 6 Treatment options for patients with UC vary according to the disease activity and severity and include mainly 5-aminosalicylates, corticosteroids, immunosuppressants (thiopurines or cyclosporine), biologics, and among others; monoclonal antibodies targeting tumor necrosis factor-α (TNF-α) or interleukin-12 and -23; and anti-integrin agents, as well as small-molecule drugs: Janus kinase inhibitors and sphingosine 1-phosphate receptor modulator. 7
In contrast to TNF-α antagonists, vedolizumab, a humanized monoclonal antibody which blocks binding of lymphocytes to the intestinal endothelium by inhibiting α4β7 integrin expressed on their surface, is not associated with an increased risk of serious infections or malignancy caused by the systemic immunosuppression due to its gut selectivity and a favorable safety profile. 8 Moreover, in view of the frequent primary non-response or secondary loss of response observed in patients receiving anti-TNF agents, there is a need for alternative therapeutic drugs with different targets to reduce inflammation. 9
Vedolizumab (Entyvio, Takeda Pharmaceutical Company Ltd, Tokyo, Japan) has been approved for the treatment of inflammatory bowel diseases, including both UC and Crohn’s disease, by the European Medicines Agency and United States Food and Drug Administration in 2014, based on the results of three pivotal clinical trials (GEMINI 1 conducted in UC patients, and GEMINI 2 and 3 in patients with Crohn’s disease). 9 The GEMINI 1, phase III study, established the efficacy and safety of this novel anti-integrin drug in patients with UC as both induction and maintenance therapies. 10 Clinical guidelines recommend vedolizumab as a first-line biological treatment for moderate-to-severe UC, along with other biologics, and as a second-line biological treatment in patients who are refractory to conventional or TNF-α antagonist therapy.7,11,12 At the time of conducting the POLONEZ study, vedolizumab was available, alongside with infliximab (TNF-α inhibitor) as a biologic therapy for UC reimbursed within the National Drug Program (NDP) in Poland, limited to 54 weeks of treatment. 13 Adalimumab and golimumab are not reimbursed for UC patients in Poland.
The aim of the POLONEZ study was to assess the real-world effectiveness and safety of vedolizumab for induction and maintenance therapies for UC in the scope of NDP in Poland as well as response durability at 26 weeks after treatment discontinuation. As detailed baseline characteristics of Polish patients showed, at the time of enrollment in the NDP, this population had a more severe disease activity, a higher percentage of biologic-naïve patients, and received the first dose of vedolizumab earlier after UC diagnosis than those described in other European real-world cohorts. 14 The obtained treatment results, which may be impacted by the abovementioned differences, complement the data of clinical trials in relation to a larger patient population and daily clinical practice.
Patients and methods
Patients and measures
The POLONEZ is a non-interventional, real-world, prospective study conducted in 12 centers in Poland to evaluate the effectiveness and safety of a 54-week therapy with vedolizumab in patients with moderate to severe UC. In addition, durability of response to treatment was assessed at 26 weeks after treatment cessation in all patients. In all, 100 consecutive adult patients who met the NDP criteria for reimbursement of treatment with vedolizumab 13 and gave their consent were recruited between February and November 2019. These reimbursement criteria were as follows: moderately to severely active UC defined as a total Mayo score of > 6 points, contraindications to treatment with cyclosporine, and an inadequate response, intolerance, or other contraindications to conventional therapy with both corticosteroids and immunosuppressants. 13 The NDP excludes patients who present with any of the following conditions: hypersensitivity to vedolizumab or excipients; severe viral, fungal, or bacterial infections; chronic heart, renal, liver, or respiratory failure; unstable coronary artery disease; demyelinating disease; diagnosis of precancerous condition or malignancy within 5 years prior to study enrollment; alcoholism; and pregnancy or lactation. During the period in which the POLONEZ study was conducted, the maximum duration of vedolizumab therapy in accordance with NDP was 54 weeks. After this time, treatment with vedolizumab was discontinued and patients remained on non-biological concomitant treatment. 13
The data concerning sex, age, body mass index (BMI), disease duration, smoking status, comorbidities, presence and type of extraintestinal manifestations, status of previous biological therapy for UC, and concomitant medications (i.e. corticosteroids, immunomodulators, 5-aminosalicylic acid derivatives) were collected. The phenotype of UC was determined according to the Montreal classification. 15 The disease activity was measured with the total Mayo score (range: 0–12, with higher scores indicating more active disease) at weeks 0 and 14.14,16,17 Mucosal healing, defined by an endoscopic Mayo score of ⩽1, 17 was assessed at week 14. The partial Mayo score (range 0–9, total Mayo score without the endoscopic component) was used to assess the effectiveness of maintenance therapy at week 54. 18 Clinical response at week 54 was defined as an improvement of at least 2 points from baseline (week 0) on the partial Mayo score, with clinical remission as 0 or 1 on the partial Mayo score. Response durability was assessed by the physician at week 80 among patients who sustained response to treatment and then discontinued vedolizumab at week 54. The patient demographic and clinical characteristics at baseline have been published elsewhere. 14 Here, results during the visit at week 54 and response durability at 26 weeks after treatment discontinuation (week 80) are described.
Vedolizumab was administered according to the label, that is, induction with 300 mg intravenously at weeks 0, 2, and 6, and maintenance with 300 mg intravenously every 8 weeks, for 54 weeks, in accordance with the regulations of NDP. Shortening of dosing frequency to every 4 weeks due to lessening response to the treatment was also allowed. 19 Patients who did not respond to treatment or lost response during maintenance therapy were excluded from NDP, which was tantamount to stopping their follow-up in this study.
Outcomes
The primary outcome measures were clinical response and clinical remission (including steroid-free remission) rates at week 54, based on the partial Mayo score and as defined above. The secondary endpoints were as follows: response durability at 26 weeks after treatment discontinuation, identification of predictors of response and remission, and assessment of the real-world safety profile of vedolizumab. In addition, changes in the partial Mayo score, Mayo subscales score, and C-reactive protein (CRP) concentrations, as well as concomitant use of corticosteroids, the presence of extraintestinal symptoms, and the need to use dosing interval shortening due to lessening response to the treatment were assessed. Subgroup analysis included biologic-naïve, biologic-exposed, and biofailure patients.
Safety
All patients who received at least one dose of vedolizumab were included in the safety analysis. All adverse events (AEs) which occurred between the visit at week 0 and the visit at week 54 were recorded. The results were expressed according to the medical dictionary of regulatory activities (MedDRA) 23.0 terminology. 20
Statistical analysis
Data of all patients who received at least one dose of vedolizumab (full analysis set) were used for analysis. Continuous variables are shown as median and interquartile range (IQR) or range. For categorical variables, the number of observations and percentages are given. To compare the groups, the paired Wilcoxon test was used for quantitative variables (with Bonferroni corrections for multiple comparisons) and the chi-square test (or Fisher’s test) for qualitative variables, with the significance level set to 0.05. Multivariable logistic regressions were applied to identify independent predictors for the primary endpoint of clinical response and remission at week 54 as well as response durability at 26 weeks after treatment discontinuation (week 80). Akaike information criterion (AIC) was used to select the optimal model with the backward stepwise procedure. A two-tailed p value < 0.05 was considered statistically significant. All statistical analyses were performed using R version 3.6 (The R Foundation for Statistical Computing, c/o Institute for Statistics and Mathematics Wirtschaftsuniversität Wien, Vienna, Austria). 21
Results
Patient disposition and baseline characteristics
Among 100 UC patients enrolled in the POLONEZ study, 91 were evaluated on vedolizumab therapy during the visit at week 14, whereas 63 completed the 54-week maintenance treatment (Figure 1, the subgroups: Supplemental Figure S1A–C). Patients discontinued vedolizumab maintenance therapy mainly due to the loss of response to treatment. The basic demographic characteristics of the patients are listed in Table 1 (median age: 35 years, 49% female, 70% nonsmokers). The detailed baseline demographic and clinical profile of the study cohort was described previously. 15 The biologic-naïve patients constituted 55% of the study group. Most of the biologic-exposed patients received anti-TNF-α treatment previously, in particular infliximab and/or adalimumab. Prior anti-TNF therapy had failed in 25 individuals (biofailures), accounting for 56% of all patients exposed to anti-TNF-α. At baseline, almost half of the patients were taking immunosuppressants and 68% received concomitant systemic corticosteroids, with an average prednisone dose equivalent of 20 mg/day. Patients with extensive colonic involvement accounted for approximately half of all cases. 14

Patient disposition and ET from the study after visit at week 14 (W14), at week 54 (W54), and at week 80 (W80). In Poland, patients with no response to treatment were discontinued from the NDP. Reasons for ET were as follows: ET1 – no response to treatment (nine patients), ET2 – loss of response (23 patients), discontinuation of treatment because of planning for pregnancy (one patient), patient resignation (one patient), severe course of pneumonia due to flu (one patient), mistake in visit scheduling (one patient), and bladder tumor (one patient), ET3 – loss of response.
Selected baseline characteristics of the patients.

Values are shown as medians (IQR), unless stated otherwise. Baseline clinical characteristics of the study group were described previously. 14
BMI, body mass index; IQR, interquartile range.
Effectiveness outcomes
At 54-week follow-up, clinical response with vedolizumab was achieved in 62% of patients (n = 62/100) versus 83% (n = 83/100) at week 14 (Table 2, Figure 2(a)). Within subgroups, the percentage of responders was similar in biologic-naïve patients (65.5%, n = 36/55) compared with those who had previous biologic exposure (57.8%, n = 26/45). Over half of the patients who had previously failed to anti-TNF-α treatment achieved response to therapy with vedolizumab (52%, n = 13/25). Maintenance of clinical response from week 14 to week 54 was observed in 75% of patients (n = 62/83).
Clinical response and remission rates of treatment with vedolizumab at weeks 14 and 54 and response durability at 26 weeks after treatment discontinuation.
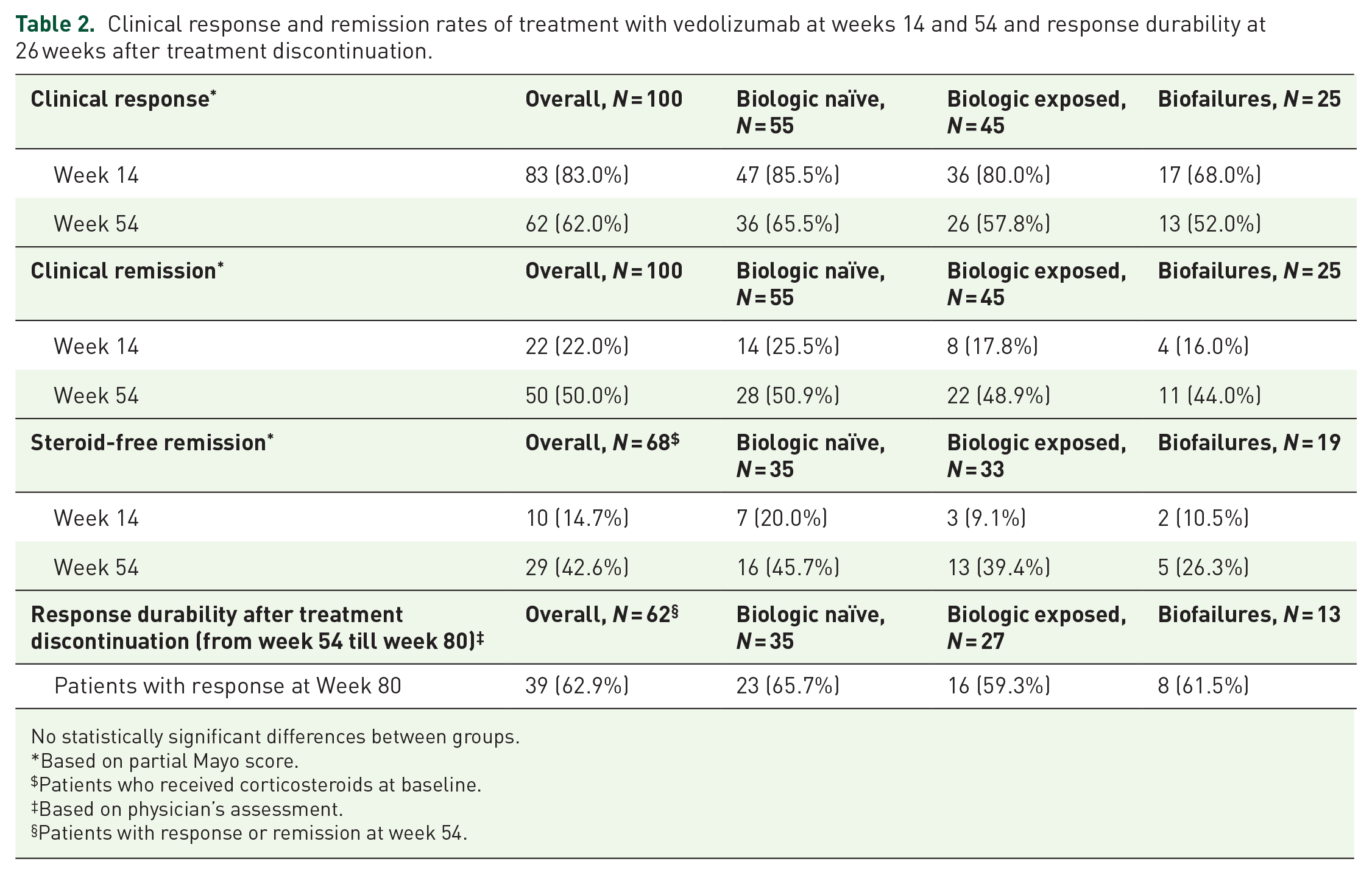
No statistically significant differences between groups.
Based on partial Mayo score.
Patients who received corticosteroids at baseline.
Based on physician’s assessment.
Patients with response or remission at week 54.
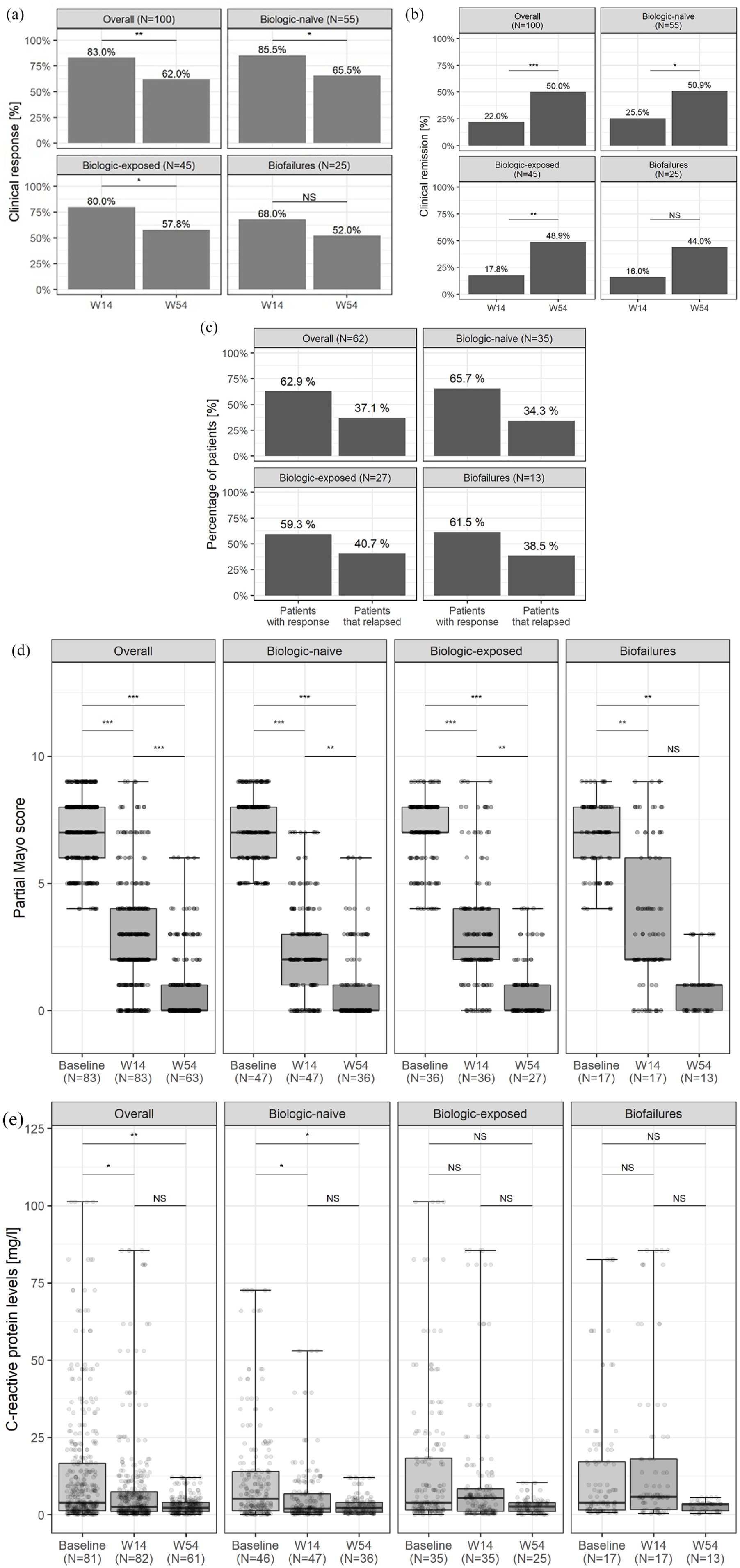
Clinical effectiveness of vedolizumab in therapy for UC. (a) Clinical response at weeks 14 and 54 (based on partial Mayo score). (b) Clinical remission at weeks 14 and 54 (based on partial Mayo score). (c) Percentage of patients with response and relapse at week 80 (based on physician’s assessment). (d) Partial Mayo score at weeks 0, 14, and 54 (only responders). (e) CRP levels at weeks 0, 14, and 54 (only responders).
Half of the patients (50%, n = 50/100) were in clinical remission at week 54 (Table 2, Figure 2(b)). In 42.6% of patients who received corticosteroids at baseline (n = 29/68), steroid-free remission was observed at week 54 (Table 2).
In all, 62 patients who maintained clinical response up to week 54 were followed-up after treatment cessation for another 26 weeks, until week 80. According to physician’s assessment, the relapse rate in this period was 37% (n = 23/62), while response durability after treatment discontinuation was observed in 63% of patients (n = 39/62) (Table 2, Figure 2(c)).
Median partial Mayo score in responders (n = 62) at week 54 reached 0, decreasing from 7 at baseline (n = 83) (Figure 2(d)). The median CRP concentration was generally similar to that obtained at week 14 and it was about 2.2 mg/L (Figure 2(e)).
At week 54, improvements were observed in all Mayo score subscales compared to weeks 0 and 14 in responders (p < 0.001 for each subscale) (Figure 3). More than two-thirds of patients (71%, n = 44/62) had normal stool frequency versus 0% at baseline (n = 0/62) and 30.6% at week 14 (n = 19/62) (Figure 3(a)). Almost 90% of patients (n = 55/62) noted no rectal bleeding versus 1.6% at baseline (n = 1/62) and 74.2% at week 14 (n = 46/62) (Figure 3(b)). The physician observed no disease activity in almost 75% of patients at week 54 (n = 46/62) versus 0% at baseline (n = 0/62) and 21% at week 14 (n = 13/62) (Figure 3(c)). The results for the subgroups (biologic-naïve, biologic-exposed, and biofailure patients) are shown in supplemental Figures S2–S4. Change from baseline for rectal bleeding and stool frequency in the responders and in subgroups is shown in Figure 4.

Effect of maintenance therapy with vedolizumab on disease activity in responders: (a) stool frequency, (b) rectal bleeding, and (c) physician’s rating of disease activity, at weeks 0, 14, and 54.
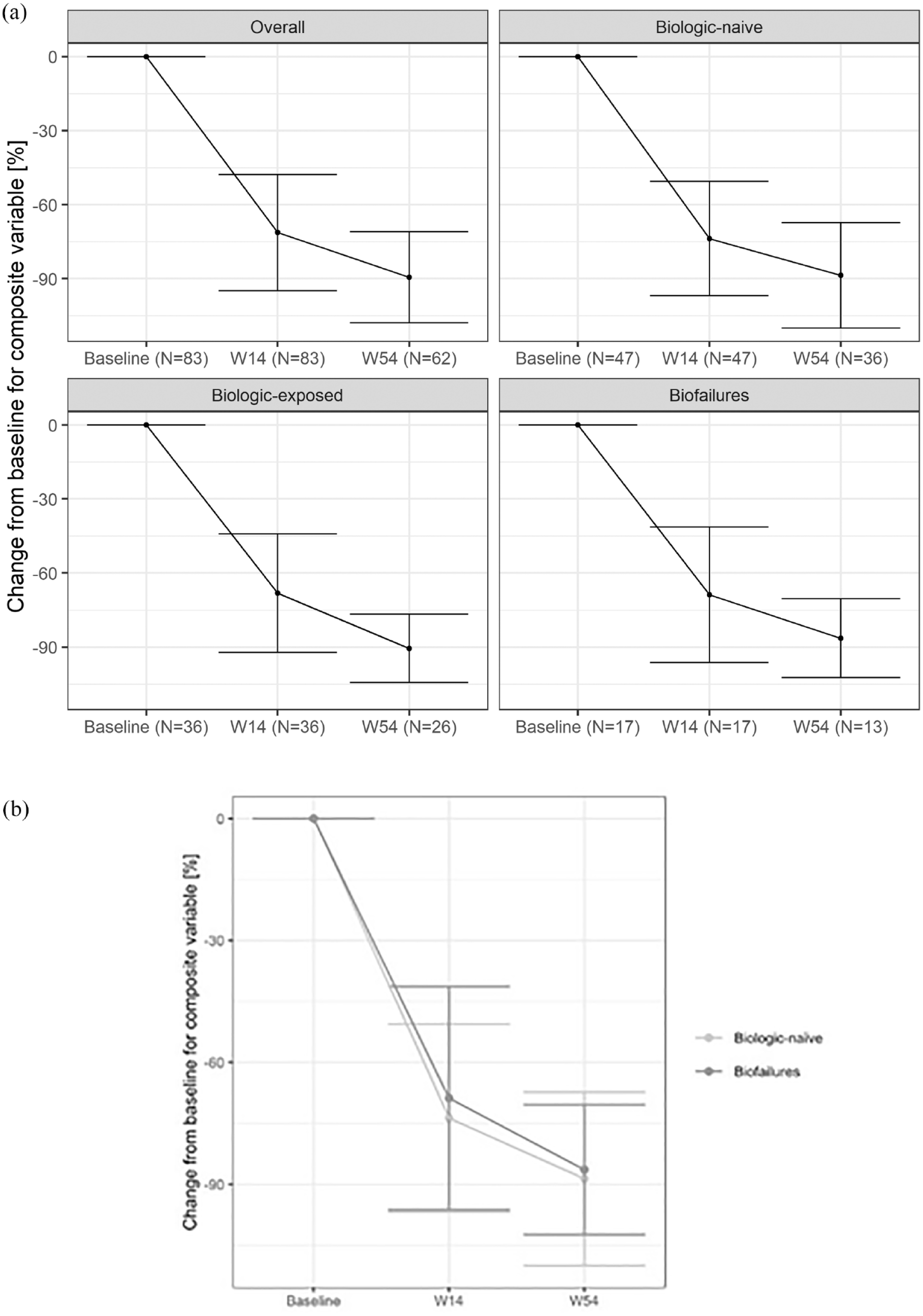
Change from baseline for composite variable (rectal bleeding and stool frequency) in responders. (a) Overall and in subgroups. (b) Biologic-naïve versus biofailure patients; no statistically significant differences between groups.
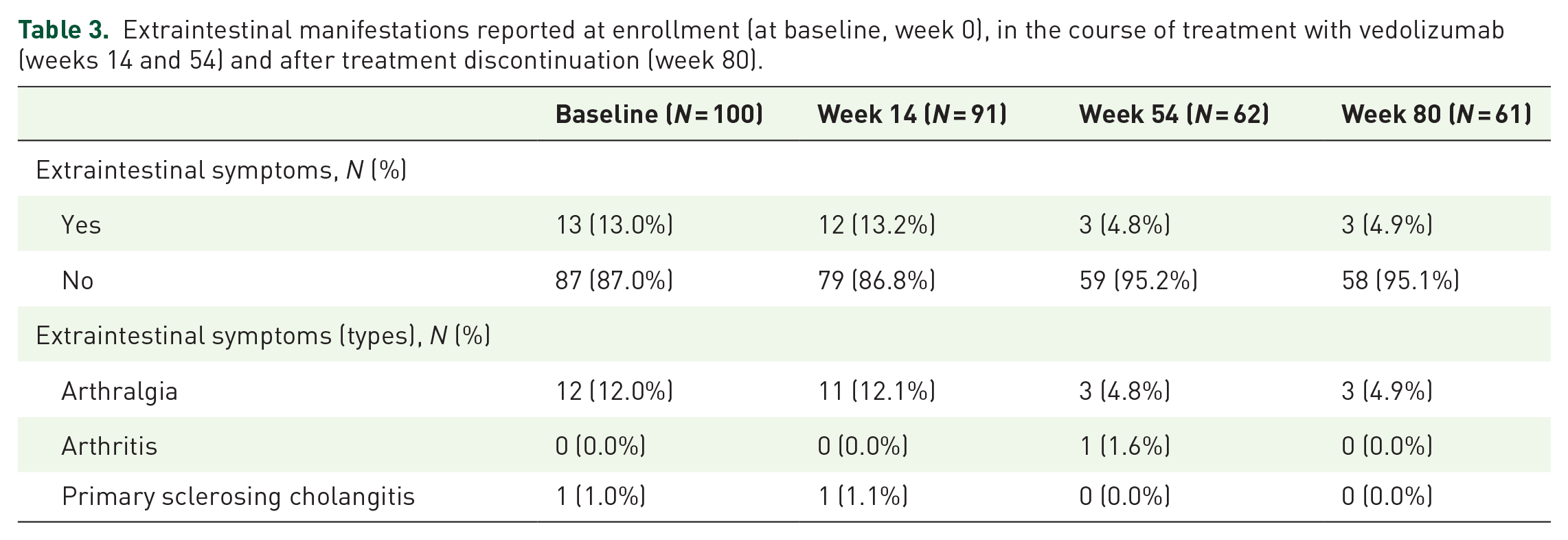
More than twofold reduction in the presence of extraintestinal manifestations of UC throughout the therapy with vedolizumab was observed (13% at baseline and at week 14 versus less than 5% at weeks 54 and 80) (Table 3). The most frequently reported extraintestinal symptom was arthralgia (n = 11 at week 14 versus n = 3 at week 54).
Extraintestinal manifestations reported at enrollment (at baseline, week 0), in the course of treatment with vedolizumab (weeks 14 and 54) and after treatment discontinuation (week 80).
Predictors of response and remission
A total of 100 patients were included in the logistic regression analysis for response and remission at week 54. In the multivariate analysis, decrease in the number of liquid stools and rectal bleeding of at least 50% at week 14 [11.05, 95% confidence interval (CI): 3.2–44.41; p < 0.001] and endoscopic response at week 14 (5.44, 95% CI: 1.52–20.94; p < 0.05) were associated with an increased odds of clinical response at week 54 (Figure 5(a)). Endoscopic response was defined as decrease of at least 1 point in mucosal appearance at endoscopy at week 14 (in comparison to baseline value). In terms of clinical remission, time from diagnosis ranging 2–5 years (6.75, 95% CI: 1.16–52.09; p < 0.05), decreased stool frequency in Mayo subscore by 1 point (0.23, 95% CI: 0.07–0.59; p < 0.01), and non-concomitant corticosteroids at baseline and at week 14 (0.28, 95% CI: 0.08–0.86; p < 0.05) were predictive factors for clinical remission at week 54 (Figure 5(b)).

Multivariate model for (a) clinical response at week 54. (b) Clinical remission at week 54. (c) Response durability after treatment discontinuation at week 80. PRO2 = number of liquid stools = 0 and rectal bleeding = 0 at week 54; PMS = partial Mayo score < 3 and no subscale > 1 at week 54.
In total, 62 patients with response for treatment at week 54 were included in the multivariate analysis for week 80. Partial Mayo score < 3 with no subscale score > 1 at week 54 was identified as a predictive factor of response durability at 26 weeks after discontinuation of 54-week vedolizumab therapy (37.84, 95% CI: 3.69–1082.24; p < 0.01) (Figure 5(c)).
Treatment patterns
Overall, dosing interval shortening due to lessening response to the treatment was necessary in 12.9% of responders (n = 8/62) at week 54. In the group of week-14 responders, the number of patients without concomitant corticosteroids increased almost 2.5-fold from week 0 (32.5%, n = 27/83) to week 14 (80.7%, n = 67/83), finally reaching 90.3% (n = 56/62) at week 54 (Table 4). The reduced need for concomitant corticosteroids was even more pronounced in the subgroup of biologic-naïve patients (Tables S1–S3). At week 54, two biologic-naïve patients were on concomitant corticosteroids (5.6%, n = 2/36) versus three patients in the biofailure subgroup (23.1%, n = 3/13). The median daily prednisone dose equivalent in the responders dropped by half, from 20 mg at week 0 to 10 mg at week 54. A similar decline was observed in the biologic-naïve, biologic-exposed, and biofailure subgroups (Tables S1–S3).
Concomitant non-biological treatment in responders at weeks 0, 14, and 54.

Dose as prednisone equivalent.
Adverse events
A total of 12 patients (12%, n = 12/100) experienced AEs during 54 weeks of vedolizumab treatment (Table 5). The majority of the reported AEs belonged to the MedDRA system organ class of infections and infestations (eight cases). The treating physician considered the following severe AEs (SAEs) to be related to vedolizumab therapy: anaphylactic reaction and neutropenia in one patient and drug hypersensitivity in another patient, respectively. The rate of SAEs related to vedolizumab treatment was 3.63 per 100 patient-years.
AEs summary in patients with UC treated with vedolizumab using MedDRA 23.0 terminology.

The association with treatment was deemed by the treating physician.
AEs, adverse events; UC, ulcerative colitis.
Discussion
This study showed that maintenance therapy with vedolizumab for UC provided clinical benefit in a Polish real-world cohort. At week 54, two-thirds of patients responded to treatment, half of the patients attained clinical remission, and more than 40% of patients were in steroid-free remission. At week 80, 37% of patients who maintained clinical response at week 54 relapsed after treatment discontinuation. To the best of our knowledge, this is the first report that described real-world effectiveness of vedolizumab for UC and durability of response after treatment discontinuation not only for Poland but also for regions of Eastern Europe.
Due to the observational nature of our study, only the procedures consistent with standard clinical practice within the NDP were performed. At the time of conducting the POLONEZ study, treatment of UC with vedolizumab in Poland was limited to 54 weeks within the NDP. Therefore, at week 80, only data relating to response durability after treatment discontinuation based on physician’s assessment could have been collected.
The clinical response and remission rates at week 54 observed in our study were slightly higher than in randomized clinical trials. In the pivotal GEMINI 1 trial, clinical remission after maintenance treatment was achieved in 44.8% of patients at week 52. 10 According to the systematic reviews of the available real-world experience studies with vedolizumab, which were published in 2018, clinical response rates at week 52 were at the level of 48% (two studies, CI was not calculated) and 52% (16 studies, 95% CI: 37–65%), while clinical remission was achieved in 39% (two studies, CI was not calculated) and in 42% of patients (corticosteroid-free clinical remission assessed in nine studies, 95% CI: 31–53%).22,23 In the more recent long-term real-world studies, the observed clinical response rate was 49% in a Swedish cohort 24 and 45% in an Israeli cohort. 25 In the abovementioned cohort studies, clinical remission rates were 47% and 33%, respectively.24,25 Furthermore, a Scottish cohort observed an endoscopic remission rate of 57.4%. 26 A similarly high proportion of UC patients from Australia and United Kingdom achieved clinical remission after 12 months of treatment (60%). 27 In the Italian cohort, only 25% of patients with UC achieved a clinical response and 20% achieved clinical remission at week 52; however, the study population was small (n = 22). 28 A high percentage of biologic-naïve patients in our cohort could have affected the observed overall results. As the study of Macaluso et al. showed, clinical response rates in biologic-naïve patients reached 73.8% after 52 weeks of treatment, 29 which is even a higher outcome than in our biologic-naïve subgroup (65.5%). A similar trend was described in another study, where 76.7% of anti-TNF-naïve patients were in clinical response at the last follow-up (42.5 weeks, IQR: 30–52 weeks). 30 Although the reduced effectiveness of vedolizumab in biologic-exposed patients, especially biofailure individuals, was often reported,26–28,31–34 in a Polish real-world cohort, no statistically significant differences between subgroups were demonstrated, similarly as in the Swedish study. 24 The authors of the study conducted on Danish patients concluded that vedolizumab was effective in achieving and restoring long-term clinical remission in patients with treatment-refractory UC (34% of patients at week 52). 34
In our study, 28% of all patients (n = 28/100) discontinued vedolizumab after week 14 during maintenance therapy and the main reason was loss of response (secondary non-response, n = 23/28) to vedolizumab treatment. This percentage was similar to that of other studies, where the discontinuation rate after 3-month therapy varied between 18%, 23.5%, and 26% of UC patients.24,25,35
To the best of our knowledge, although there are numerous reports of patient persistence on vedolizumab therapy, 36 there is only little data about response durability after treatment discontinuation in UC patients. In the retrospective study of Martin et al., 37 two-thirds of patients with inflammatory bowel diseases, who achieved clinical remission after therapy with vedolizumab, experienced relapse within the first year after drug discontinuation. Re-treatment with vedolizumab resulted in steroid-free remission in 70% of patients at week 14. 37 In our study, the therapeutic effect was maintained up to 6 months after the end of treatment with vedolizumab in 63% of patients who responded to treatment at week 54, while 37% of patients relapsed. Our results indicate the validity of chronic vedolizumab therapy. However, discontinuation of treatment can be considered after 1 year, in case of some circumstances (e.g. the patient’s decision, mild side effects, but troublesome for the patient, fear of the pregnant woman of continuing the therapy), but only in patients with a high clinical response and predictors of the durability of the therapeutic effect (according to our analysis: partial Mayo score < 3 with no subscale score > 1 at week 54). Our study is probably the first to address such data, important from a practical point of view.
Multivariate analysis of patients with UC conducted in our study showed that decrease in the number of liquid stools and rectal bleeding score of at least 50% at week 14 and endoscopic response at week 14 were predictors of clinical response at week 54. Time from diagnosis spanning 2–5 years, decreased stool frequency in Mayo subscore by 1 point, and non-concomitant corticosteroids at baseline and at week 14 were associated with an increased odds of clinical remission at week 54. Allegretti et al. aimed to identify the predictors of long-term clinical response or remission in UC patients with the initial response to vedolizumab. However, no such predictors were identified, although the need for hospitalization demonstrated a trend toward decreased odds of response or remission. 38 In turn, according to Amiot et al., patients who exhibited a clinical response at week 6 were more likely to be in steroid-free clinical remission at week 54. 39 Another report indicated that prior exposure to TNF-α antagonists was associated with a reduced probability of achieving clinical remission, mucosal healing, and endoscopic improvement. 26 Stallmach et al. found more predictive factors for clinical remission: apart from remission at week 14 and no prior anti-TNF treatment, also the use of steroids less than 25% of the time within the last 6 months, lower CRP at week 14 as compared to baseline, and lower fecal calprotectin at week 14. 33 According to a machine learning algorithm using laboratory data proposed by Waljee et al., the five strongest baseline predictors of corticosteroid-free endoscopic remission at week 52 were as follows: fecal calprotectin, albumin, neutrophils, white blood cell count, and absolute lymphocyte count. Prior use of anti-TNF therapy as well as use of immunomodulators or corticosteroids at baseline was notably weak baseline predictors of this outcome. 40 Along with the effectiveness and safety of new drugs used in inflammatory bowel disease, current research focuses on identification of predictive markers of response to each of them. Also, for vedolizumab, clinical, biochemical, molecular, microbiota, and genetic markers are being studied in this respect.41–45 Identification and selection of therapy that is optimal in each case would prevent patients from receiving unnecessary treatments that fail and limit incurred costs related to the therapy. Therefore, identification of easily available drug response predictors is of utmost importance and should be one of the goals for future studies.
Our analysis showed that 90.3% of all patients who reached week 54 were without corticosteroids. This result was consistent with the reports by Kopylov et al. (86.2% at week 52), 25 Stallmach et al. (83% at week 54), 33 and White et al. (85% at week 52), 46 which similarly observed a significant decrease in concomitant corticosteroid use compared with baseline. Steroid-free clinical remission at week 54 was the primary endpoint in the study conducted by Amiot et al. (40.5% of all patients) 39 and a secondary endpoint of the pivotal GEMINI-1 trial (41.8% of patients who continued to receive vedolizumab every 8 weeks and 44.8% of patients who continued to receive vedolizumab every 4 weeks), 10 which is similar to our study (47% of all patients).
Remission of arthralgia, a frequent extraintestinal manifestation in UC patients, treated with vedolizumab, has been reported previously.39,47 Our results confirmed the substantial reduction in arthralgia symptoms after 1 year of treatment. Sustained resolution of extraintestinal manifestations was considered to be associated with clinical remission in UC. 48
The literature on AEs occurring during maintenance therapy with vedolizumab varies widely. The percentage of AEs reported in different studies ranged from 6% to 60%.22,32,33,39,49 Loftus et al. noted that treatment-related SAEs were observed in 4.1% UC patients versus 2% in our study. 50 In general, the most frequently reported AEs were infections, mainly of the gastrointestinal tract (i.e. Clostridioides difficile) and the upper respiratory tract.22,28,32,39,49
Our study has several limitations. First, vedolizumab was administered in the scope of the NDP, which is a national reimbursement program authorized by the Polish Ministry of Health. NDP defines the inclusion and exclusion criteria for biologics in Poland as well as all required and reimbursed tests and examinations to monitor treatment effectiveness and safety. Therefore, our non-interventional study could not change diagnostic or monitoring procedures applied to the patients. As a consequence, all medical procedures were carried out according to the NDP guidelines that did not include obligatory endoscopic evaluation at the end of maintenance therapy. As a result, mucosal healing, a treatment target in UC according to STRIDE recommendations6,51 was assessed in a small number of patients who completed 54 weeks of vedolizumab treatment. Therefore, the effectiveness assessment could only be done based on the partial Mayo score. Furthermore, a relatively small sample size was included. However, the group of 100 consecutive patients with UC enrolled into this study from multiple centers represents one of the largest real-world cohorts observed prospectively for the effectiveness of vedolizumab in induction and maintenance therapies in a real-world setting. Moreover, the low number of non-responders to vedolizumab could have impacted the results of the analysis of predictors of treatment response. It is worth mentioning that all patients recruited to our study were treated with vedolizumab in the scope of NDP, which required the clinical data to be fully and systematically collected.
Conclusions
Results of our study support the effectiveness and favorable safety profile of vedolizumab used as a maintenance therapy for UC patients, with more than 60% of patients responding to the 54-week treatment and 50% of patients with clinical remission. However, the relapse rate within 26 weeks after treatment discontinuation was high (37% of patients). The outcomes obtained from a Polish real-world cohort, characterized by a severe UC disease activity and a relatively low percentage of patients who previously failed anti-TNF treatment, complement the data of clinical trials and other real-world studies in relation to a larger patient population and daily clinical practice.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231151295 – Supplemental material for Real-world outcomes of 54-week vedolizumab therapy and response durability after treatment discontinuation in ulcerative colitis: results from a multicenter prospective POLONEZ study
Supplemental material, sj-docx-1-tag-10.1177_17562848231151295 for Real-world outcomes of 54-week vedolizumab therapy and response durability after treatment discontinuation in ulcerative colitis: results from a multicenter prospective POLONEZ study by Piotr Eder, Maria Kłopocka, Halina Cichoż-Lach, Renata Talar-Wojnarowska, Maria Kopertowska-Majchrzak, Agata Michalak, Rafał Filip, Katarzyna Waszak, Kamila Stawczyk-Eder, Maria Janiak, Krzysztof Skrobot, Ariel Liebert, Hubert Zatorski, Anna Solarska-Półchłopek, Michał Krogulecki, Anna Pękała, Elżbieta Poniewierka, Izabela Smoła, Aleksandra Kaczka, Krzysztof Wojciechowski, Szymon Drygała and Edyta Zagórowicz in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors are grateful to the following persons for their contribution to data collection, analysis, assistance with statistical analysis, critical review of the article, and medical writing support: (1) National Cancer Institute: Monika Cichaczewska; (2) Święcicki University Hospital: Agnieszka Dobrowolska, MD, PhD, Anna Królewska; (3) Biostat: Edyta Klemba, Marian Płaszczyca, PhD, Barbara Gorzawska, Anna Zabielska; (4) Proper Medical Writing sp. z o.o.: Maria Kołtowska-Häggström, MD, PhD, Anna Jesionek, PhD, Ewa Marczuk, funded by Takeda Pharma sp. z o.o.; and (5) Takeda: Fiona Brägger, PhD, Marlies Neuhold, MD.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.