
Abstract
Background:
Coronavirus disease 2019 (COVID-19) has triggered a global public health crisis. Proton pump inhibitors (PPIs) are one of the most commonly prescribed drugs. However, the effect of PPIs on the clinical outcomes of COVID-19 patients remains unclear.
Methods:
All COVID-19 patients admitted to the Wuhan Huoshenshan Hospital from February 2020 to April 2020 were retrospectively collected. Patients were divided into PPIs and non-PPIs groups. Logistic regression analyses were performed to explore the effects of PPIs on the outcomes of COVID-19 patients, including transfer to intensive care unit, mechanical ventilation, and death. Subgroup analyses were performed according to the presence of upper gastrointestinal symptoms potentially associated with acid and the routes, types, median total dosage, and duration of PPIs. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Results:
Of the 3024 COVID-19 patients included, 694 and 2330 were in PPIs and non-PPIs groups, respectively. Univariate logistic regression analysis showed that PPIs significantly increased the risk of reaching the composite endpoint in COVID-19 patients (OR = 10.23, 95% CI = 6.90–15.16, p < 0.001). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, PPIs were independently associated with an increased risk of reaching the composite endpoint (OR = 7.00, 95% CI = 4.57–10.71, p < 0.001). This association remained significant in patients with upper gastrointestinal symptoms and those who received an intravenous omeprazole alone, but not those who received oral lansoprazole or rabeprazole alone. It was not influenced by dosage or duration of PPIs.
Conclusion:
The use of intravenous PPIs alone during hospitalization may be associated with worse clinical outcome in COVID-19 patients.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has triggered a global public health crisis. 1 From the COVID-19 outbreak at the end of 2019 to 13 April 2022, the World Health Organization has reported a total of 497,960,492 confirmed cases and 6,181,850 deaths. 2 Among the COVID-19 patients, fever and respiratory symptoms are the most common clinical presentations. 3 In addition, SARS-CoV-2 can cause gastrointestinal symptoms, including anorexia, nausea, vomiting, and diarrhea.4–6 Proton pump inhibitors (PPIs) are usually considered for the management of gastrointestinal symptoms and prevention of stress ulcers in COVID-19 patients, especially those who have received hormones.7,8 However, gastric acid can prevent microorganisms from reaching the gastrointestinal tract by inactivating the source of infection ingested. 9 Thus, PPIs inhibit gastric acid secretion and then lead to gastric acid deficiency, which may increase the risk of SARS-CoV-2 infection. 10 On the other hand, the use of PPIs can cause adverse effects, including acute interstitial nephritis, gastrointestinal infections, and respiratory infections, which may increase the risk of death in patients with COVID-19.11,12 Until now, the benefits and risks of PPIs in COVID-19 patients remain unclear. This retrospective study attempted to explore the effects of PPIs on the clinical outcomes of COVID-19 patients.
Methods
The reporting of this study conforms to the STROBE statement. 13
Study design
This retrospective study was approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command and performed in accordance with the Declaration of Helsinki. The ethical approval number was Y (2021) 059. Due to the nature of this retrospective observational study without any additional interventions, the patients’ informed consents were waived. All patients’ details have been de-identified. We collected the data of 3041 COVID-19 patients consecutively admitted to the Wuhan Huoshenshan Hospital from February 2020 to April 2020.14–17 Among them, 17 patients were excluded, because the severity of COVID-19 at admission was not clearly defined. Age, sex, and presence of malignancy were not limited.
By reviewing electronic medical records, only PPIs, but not H2 receptor antagonists, were acid suppression drugs used in the Wuhan Huoshenshan Hospital. Based on the use of PPIs during hospitalization, eligible patients were divided into PPIs group and non-PPIs group. The routes, types, total dosage, and duration of PPIs were recorded.
The following data were collected from medical records: demographics (i.e. age and sex), COVID-19 severity at admission, comorbidities (i.e. diabetes, hypertension, cardiovascular diseases, chronic kidney diseases, and malignancy), clinical characteristics, and laboratory tests (i.e. total bilirubin, international normalized ratio, albumin, C-reactive protein, procalcitonin, interleukin-6, and white blood cell). The outcomes of interest included transfer to the intensive care unit (ICU), mechanical ventilation, or death.
Definitions
The severity of COVID-19 patients was classified into mild, moderate, severe, and critical based on the New Coronavirus Pneumonia Prevention and Control Program published by the National Health Commission of China (Provisional, 7th Edition Revision). 18 Mild cases were defined as the clinical symptoms were mild without pneumonia on imaging. Moderate cases were defined as the patients presented with fever with respiratory symptoms and pneumonia on imaging. Severe cases would be defined, if any of the following conditions was met: (1) shortness of breath, respiration rate ⩾30 times/min; (2) resting oxygen saturation ⩽93%; or (3) arterial partial pressure of oxygen/fraction of inspiration oxygen ⩽300 mmHg. Critical cases would be defined, if any of the following conditions was met: (1) respiratory failure requiring mechanical ventilation; (2) shock; or (3) other organ failure requiring ICU monitoring.
Upper gastrointestinal symptoms potentially associated with acid were defined as nausea, vomiting, abdominal distention, abdominal pain, heartburn, regurgitation, hematochezia, and melena.
The composite endpoint was defined as transfer to ICU, requirement of mechanical ventilation, and/or death.
Statistical analyses
All statistical analyses were performed by the statistical software IBM SPSS version 20.0 (IBM Corp, Armonk, NY, USA). Continuous variables were expressed by mean ± standard deviation (SD) and median (range). Categorical variables were expressed by frequency and percentage. Nonparametric Mann–Whitney U test and chi-square test were used for continuous and categorical variables to compare the differences between PPIs and non-PPIs groups, respectively. Univariate and multivariate logistic regression analyses were performed to explore the effects of PPIs on the clinical outcome of COVID-19 patients. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Subgroup analyses were performed according to the presence of upper gastrointestinal symptoms potentially associated with acid and the routes, types, median total dosage, and duration of PPIs. A two-tailed p < 0.05 was considered statistically significant.
Results
Patient characteristics
Overall, 3024 COVID-19 patients were included in our study. Baseline characteristics of patients are shown in Table 1. The median age was 60 years (range: 11.00–100.00), and majority (50.86%, 1538/3024) were men. The most common comorbidity was hypertension (17.60%, 532/3024), followed by diabetes (14.40%, 434/3024), cardiovascular diseases (8.90%, 268/3024), malignancy (2.50%, 77/3024), and chronic kidney diseases (1.70%, 50/3024). Of them, 13.00% (393/3024) were considered to have upper gastrointestinal symptoms potentially associated with acid, including abdominal distention (5.90%, 177/3024), followed by nausea/vomiting (4.40%, 132/3024), heartburn/regurgitation (2.30%, 69/3024), abdominal pain (2.12%, 64/3024), and hematochezia/melena (1.80%, 55/3024). At admission, 26.12% (790/3024) and 1.55% (47/3024) of patients had severe and critical COVID-19, respectively.
Differences between PPIs and non-PPIs groups.

COVID-19, coronavirus disease 2019; CRP, C-reactive protein; INR, international normalized ratio; PPIs, proton pump inhibitors; Pts, patients; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
Overall analyses
Overall, 22.95% (694/3024) of COVID-19 patients were prescribed with PPIs during their hospitalizations. Univariate logistic regression analysis showed that PPIs significantly increased the risk of reaching the composite endpoint in patients with COVID-19 (OR = 10.23, 95% CI = 6.90–15.16, p < 0.001). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, PPIs remained an independent risk factor of reaching the composite endpoint (OR = 7.00, 95% CI = 4.57–10.71, p < 0.001) (Figure 1).
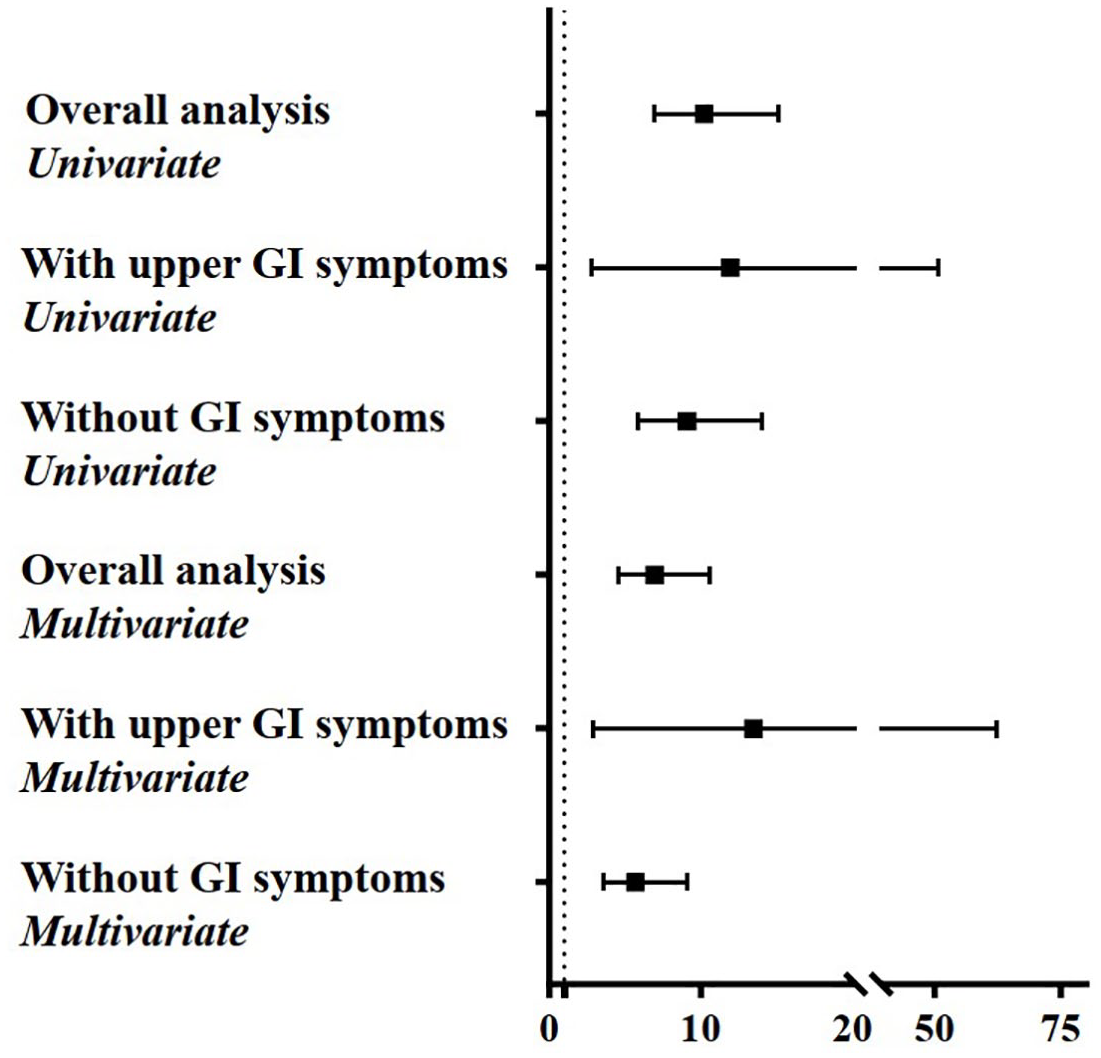
Forest plots showing the major results of univariate and multivariate analyses regarding the association between PPIs use and the outcomes of COVID-19 patients.
Subgroup analyses according to the presence of upper gastrointestinal symptoms potentially associated with acid
Univariate logistic regression analysis showed that PPIs significantly increased the risk of reaching the composite endpoint in COVID-19 patients with upper gastrointestinal symptoms potentially associated with acid (OR = 11.95, 95% CI = 2.81–50.83, p < 0.001) and those without any gastrointestinal symptom (OR = 9.09, 95% CI = 5.87–14.08, p < 0.001). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, PPIs remained an independent risk factor of reaching the composite endpoint in COVID-19 patients with upper gastrointestinal symptoms potentially associated with acid (OR = 14.74, 95% CI = 3.17–68.60, p < 0.001) and those without any gastrointestinal symptom (OR = 5.51, 95% CI = 3.43–8.84, p < 0.001) (Figure 1).
Subgroup analyses according to the routes of PPIs
Only a single route of PPIs administration was analyzed to avoid the bias caused by multiple routes of PPIs concomitantly given. PPIs were given via an oral route (77.38%, 537/694) or an intravenous (11.82%, 82/694) route alone. Univariate logistic regression analysis showed that intravenous PPIs alone group had a significantly higher risk of reaching the composite endpoint as compared to non-PPIs group (OR = 70.26, 95% CI = 40.77–121.08, p < 0.001) and oral PPIs alone group (OR = 27.09, 95% CI = 14.65–50.11, p < 0.001), and that oral PPIs alone group had a significantly higher risk of reaching the composite endpoint as compared to non-PPIs group (OR = 2.59, 95% CI = 1.50–4.48, p < 0.001). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, intravenous PPIs alone group still had a significantly higher risk of reaching the composite endpoint as compared to non-PPIs group (OR = 26.01, 95% CI = 14.11–47.95, p < 0.001) and oral PPIs alone group (OR = 13.77, 95% CI = 6.94–27.33, p < 0.001), and oral PPIs alone group still had a significantly higher risk of reaching the composite endpoint as compared to non-PPIs group (OR = 1.95, 95% CI = 1.09–3.48, p = 0.024) (Figure 2).

Forest plots showing the major results of univariate and multivariate analyses regarding the association between routes of PPIs and the outcomes of COVID-19 patients.
Subgroup analyses according to the types of PPIs
Only a single type of PPIs was analyzed to avoid the bias caused by multiple types of PPIs concomitantly given. Omeprazole, lansoprazole, or rabeprazole monotherapy was used in 82, 456, or 66 patients, respectively. Notably, among them, omeprazole was given only via an intravenous route; by comparison, lansoprazole and rabeprazole were given only via an oral route. Univariate logistic regression analysis showed that the use of omeprazole (OR = 70.26, 95% CI = 40.77–121.08, p < 0.001) or lansoprazole (OR = 2.32, 95% CI = 1.28–4.21, p = 0.006) alone, but not that of rabeprazole alone (OR = 3.03, 95% CI = 0.91–10.12, p = 0.071), significantly increased the risk of reaching the composite endpoint as compared to non-PPIs. After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, the use of omeprazole alone (OR = 26.01, 95% CI = 14.11–47.95, p < 0.001), but not lansoprazole alone (OR = 1.72, 95% CI = 0.92–3.21, p = 0.091), remained an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 3).

Forest plots showing the major results of univariate and multivariate analyses regarding the association between types of PPIs and the outcomes of COVID-19 patients.
Subgroup analyses according to the median total dosage of PPIs every patient
Only a single type of PPIs was analyzed to avoid the bias caused by multiple types of PPIs concomitantly given. The median total dosage of omeprazole was 320 mg (range: 40.00–3120.00) for every patient during hospitalization. Of the 82 patients receiving omeprazole alone, 35 and 47 received omeprazole at a dosage of >320 and ⩽320 mg, respectively. Univariate logistic regression analysis showed that omeprazole >320 mg (OR = 60.18, 95% CI = 28.71–126.15, p < 0.001) and ⩽320 mg (OR = 78.89, 95% CI = 40.67–153.04, p < 0.001) significantly increased the risk of reaching the composite endpoint as compared to non-PPIs, but the risk of reaching the composite endpoint was not significantly different between omeprazole >320 and ⩽320 mg groups (OR = 0.76, 95% CI = 0.32–1.84, p = 0.545). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, omeprazole >320 mg (OR = 21.62, 95% CI = 9.45–49.49, p < 0.001) and ⩽320 mg (OR = 25.97, 95% CI = 12.36–54.55, p < 0.001) remained an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 4).
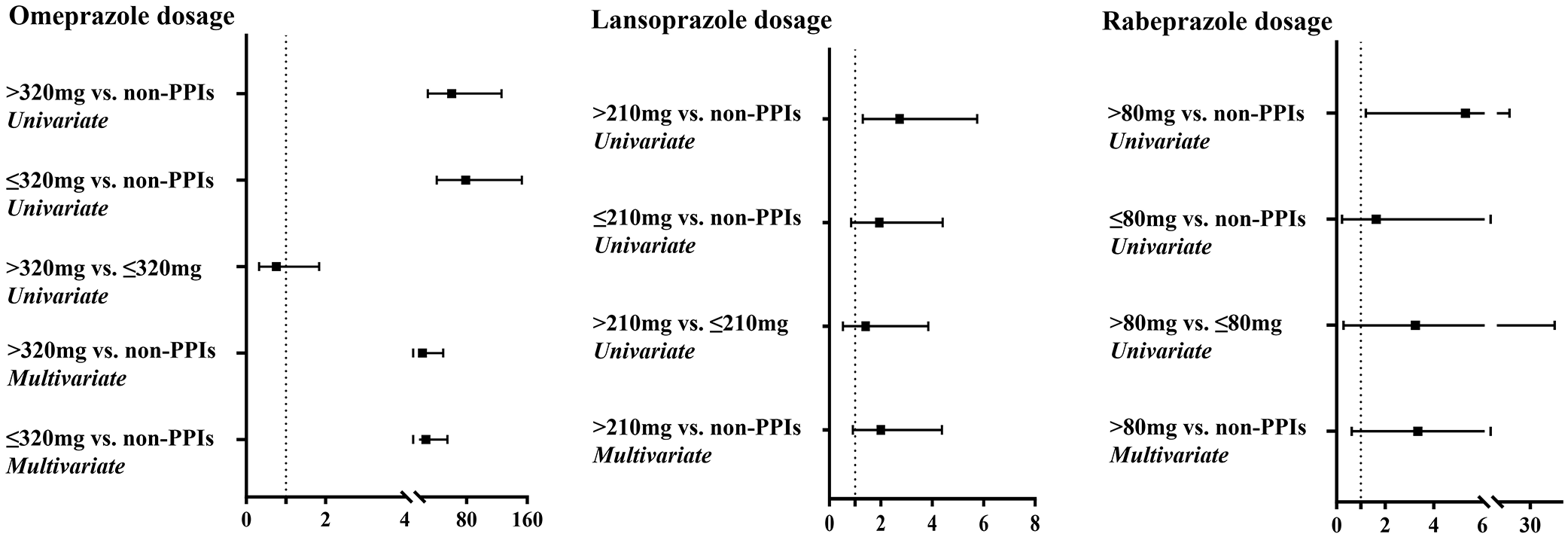
Forest plots showing the major results of univariate and multivariate analyses regarding the association between dosage of PPIs and the outcomes of COVID-19 patients.
The median total dosage of lansoprazole was 210 mg (range: 10.00–8190.00) for every patient during hospitalization. Of the 456 patients receiving lansoprazole alone, 219 and 237 received lansoprazole at a dosage of >210 and ⩽210 mg, respectively. Univariate logistic regression analysis showed that lansoprazole >210 mg (OR = 2.73, 95% CI = 1.30–5.75, p = 0.008), but not lansoprazole ⩽210 mg (OR = 1.94, 95% CI = 0.85–4.41, p = 0.114), significantly increased the risk of reaching the composite endpoint as compared to non-PPIs. However, the risk of reaching the composite endpoint was not significantly different between lansoprazole >210 and ⩽210 mg groups (OR = 1.41, 95% CI = 0.52–3.85, p = 0.505). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, lansoprazole >210 mg (OR = 1.16, 95% CI = 0.40–3.33, p = 0.787) was not an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 4).
The median total dosage of rabeprazole was 80 mg (range: 10.00–410.00) for every patient during hospitalization. Of the 66 patients receiving rabeprazole alone, 26 and 40 received rabeprazole at a dosage of rabeprazole >80 and ⩽80 mg, respectively. Univariate logistic regression analysis showed that rabeprazole >80 mg (OR = 5.31, 95% CI = 1.21–23.32, p = 0.027), but not rabeprazole ⩽80 mg (OR = 1.63, 95% CI = 0.22–12.22, p = 0.632), significantly increased the risk of reaching the composite endpoint as compared to non-PPIs. However, the risk of reaching the composite endpoint was not significantly different between rabeprazole >80 and ⩽80 mg groups (OR = 3.25, 95% CI = 0.28–37.80, p = 0.346). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, rabeprazole >80 mg (OR = 3.35, 95% CI = 0.61–18.53, p = 0.162) was not an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 4).
Subgroup analyses according to the total duration of PPIs every patient
Only a single type of PPIs was analyzed to avoid the bias caused by multiple types of PPIs concomitantly given. The median duration of omeprazole was 5 days (range: 1.00–39.00) for every patient during hospitalization. Of the 82 patients receiving omeprazole alone, 41 and 41 received omeprazole for a duration of >5 and ⩽5 days, respectively. Univariate logistic regression analysis showed that omeprazole >5 days (OR = 55.03, 95% CI = 27.42–110.44, p < 0.001) and ⩽5 days (OR = 89.96, 95% CI = 44.53–181.73, p < 0.001) significantly increased the risk of reaching the composite endpoint as compared to non-PPIs, but the risk of reaching the composite endpoint was not significantly different between omeprazole >5 and ⩽5 days groups (OR = 0.64, 95% CI = 0.27–1.54, p = 0.321). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, either omeprazole >5 days (OR = 19.32, 95% CI = 8.91–41.88, p < 0.001) or ⩽5 days (OR = 29.85, 95% CI = 13.52–65.88, p < 0.001) remained an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 5).

Forest plots showing the major results of univariate and multivariate analyses regarding the association between duration of PPIs and the outcomes of COVID-19 patients.
The median duration of lansoprazole was 9 days (range: 1.00–47.00) for every patient during hospitalization. Of the 456 patients receiving lansoprazole alone, 209 and 247 received lansoprazole for a duration of >9 and ⩽9 days, respectively. Univariate logistic regression analysis showed that lansoprazole >9 days (OR = 2.87, 95% CI = 1.36–6.04, p = 0.006), but not lansoprazole ⩽9 days (OR = 1.86, 95% CI = 0.82–4.22, p = 0.139), significantly increased the risk of reaching the composite endpoint as compared to non-PPIs. However, the risk of reaching the composite endpoint was not significantly different between lansoprazole >9 and ⩽9 days groups (OR = 1.54, 95% CI = 0.57–4.22, p = 0.398). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, lansoprazole >9 days (OR = 1.94, 95% CI = 0.89–4.25, p = 0.096) was not an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 5).
The median duration of rabeprazole was 7 days (range: 1.00–27.00) for every patient during hospitalization. Of the 66 patients receiving rabeprazole alone, 24 and 42 received rabeprazole for a duration of rabeprazole >7 and ⩽7 days, respectively. Univariate logistic regression analysis showed that rabeprazole >7 days (OR = 5.79, 95% CI = 1.31–25.56, p = 0.020), but not rabeprazole ⩽7 days (OR = 1.55, 95% CI = 0.21–11.61, p = 0.667), significantly increased the risk of reaching the composite endpoint as compared to non-PPIs. However, the risk of reaching the composite endpoint was not significantly different between rabeprazole >7 and ⩽7 days groups (OR = 3.73, 95% CI = 0.32–43.44, p = 0.294). After adjusting for age, sex, comorbidities, other medications, and severe/critical COVID-19, rabeprazole >7 days (OR = 4.47, 95% CI = 0.99–20.24, p = 0.052) was not an independent risk factor of reaching the composite endpoint as compared to non-PPIs (Figure 5).
Discussion
The finding of our overall analysis showed that the use of PPIs significantly increased the risk of reaching composite endpoint in COVID-19 patients and that such an adverse effect remained statistically significant even after adjusting for major confounding factors, which are consistent with the findings from a previous meta-analysis. 19 Additionally, major findings from our subgroup analyses included the following: (1) PPIs significantly increased the risk of reaching the composite endpoint in COVID-19 patients with upper gastrointestinal symptoms potentially associated with acid and those without gastrointestinal symptoms; (2) an intravenous route of PPIs, but not oral route of PPIs, significantly increased the risk of reaching the composite endpoint in COVID-19 patients; (3) as compared to non-PPIs, the use of omeprazole alone, regardless of its dosage and duration, significantly increased the risk of reaching the composite endpoint; and (4) as compared to non-PPIs, the use of oral lansoprazole or rabeprazole alone could not independently increase the risk of reaching the composite endpoint in COVID-19 patients.
There are several potential explanations for the impact of PPIs on the outcomes of COVID-19 patients (Figure 6). First, the main function of gastric acid is to inactivate the ingested microorganisms to prevent them reaching the intestine. 20 PPIs inhibit gastric acid secretion by blocking gastric H+K+-ATPase. 21 Thus, the protective effect of gastric acid can be impaired, leading to intestinal bacterial overgrowth and changing the composition of gut microbiome, 22 which causes gastrointestinal infections and increases the risk of death in COVID-19 patients.23–25 Second, PPIs increased the risk of secondary infections in patients with COVID-19. Furthermore, as compared to those without, COVID-19 patients with secondary infections had a significantly higher proportion of developing acute respiratory distress syndrome (ARDS). 26 ARDS, a common complication of COVID-19, can lead to a mortality of 45%. 27 Third, patients with cardiovascular diseases often take clopidogrel. PPIs compete with hepatic cytochrome P450 2C19 isoenzymes to inhibit the activation of clopidogrel, promote thrombosis, and aggravate the progression of cardiovascular diseases.28–30 Thus, cardiac damage may be aggravated by the use of PPIs in COVID-19 patients. Fourth, PPIs and their metabolites are deposited as circulating immune complexes in renal tubules and renal interstitium, which may induce immune response and cause acute interstitial nephritis.31,32 Thus, renal damage may be aggravated by the use of PPIs in COVID-19 patients. Fifth, elimination of gastric acid barrier by PPIs leads to small intestinal bacterial overgrowth. Bacteria cross the intestinal lumen and enter the mesenteric lymph nodes, causing bacterial translocation and then spontaneous bacterial peritonitis.33,34 Additionally, excessive growth of intestinal flora and bacterial translocation caused by PPIs may promote the progression of hepatic encephalopathy.35–37 Thus, the risk of liver disease-related complications may be increased by the use of PPIs in COVID-19 patients.
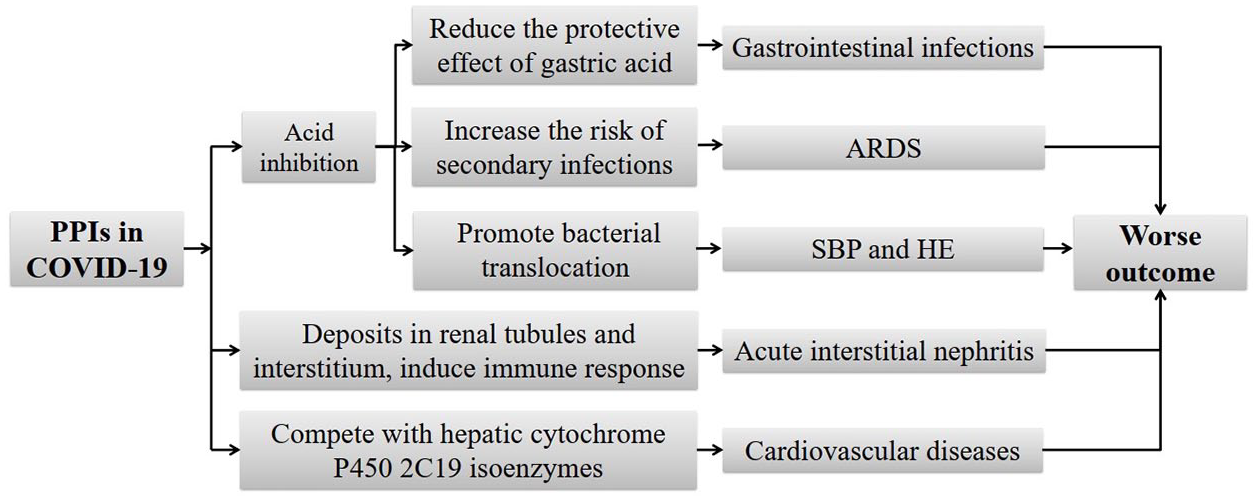
Potential mechanisms regarding the impact of PPIs on the outcomes of COVID-19 patients.
There are two potential explanations for the findings that an intravenous route of PPIs, rather than oral route of PPIs, had a worse outcome in COVID-19 patients. First, during the process of an intravenous infusion, the particles enter the human body through the liquid, thereby causing vascular embolism and allergic reactions, which may increase the risk of death in COVID-19 patients. 38 Second, an intravenous route requires insertion of a cannula, in which skin bacteria, such as Staphylococcus epidermidis, can enter into the circulatory system through the cannula site, and then cause systemic bacteremia, which may be lethal in COVID-19 patients.39,40 Notably, such a finding could also be used to explain why omeprazole alone, but not lansoprazole or rabeprazole alone, was an independent prognostic factor in COVID-19 patients. In the present study, omeprazole is given by an intravenous route alone; in contrast, lansoprazole or rabeprazole is given by an oral route alone.
Our study features are as follows. First, in this large cohort from China, we collected the data of COVID-19 patients who were consecutively admitted to the Wuhan Huoshenshan Hospital during a 2-month period. In this setting, the treatment strategy is nearly similar, which may reduce the bias of treatment selection. Second, we carefully reviewed the medical records of each patient, and obtained PPIs information more accurately; by comparison, in previous studies, 41 PPIs data came from self-reports that might cause recall bias. Third, we performed subgroup analyses to further explore whether the use of PPIs would affect the outcomes in COVID-19 patients with and without gastrointestinal symptoms. In addition, we performed subgroup analyses according to the routes, types, dosage, and duration of PPIs; by comparison, previous studies did not conduct such analyses. Fourth, we performed multivariate analyses to identify the independent effect of PPIs on the patients’ outcomes by adjusting for major confounding factors, including age, sex, comorbidities, other medications, and severe/critical COVID-19.
Several limitations are as follows. First, our study mainly collected the information during hospitalization. It was unclear about whether COVID-19 patients had previously used PPIs or other acid-inhibiting drugs. Second, lansoprazole and rabeprazole were given orally alone, so we cannot explore the effect of an intravenous lansoprazole or rabeprazole on the outcomes of COVID-19 patients. Similarly, omeprazole was given intravenously alone, so we cannot explore the effect of oral omeprazole on the outcomes of COVID-19 patients. Other types of PPIs or acid suppression drugs were not used in our patients, so their effects could not be further analyzed in our study. Third, endoscopy was not available, and PPIs were often prescribed at the discretion of the physicians’ decisions according to each patient’s individual condition. The indications of PPIs were not clear. Fourth, the mechanisms about how PPIs lead to a worse outcome in COVID-19 patients have not been explored yet.
In conclusion, the use of PPIs during hospitalization may be associated with a worse outcome among patients with COVID-19. Notably, an intravenous omeprazole alone, regardless of dosage and duration, can lead to a worse outcome of COVID-19 patients. But such a poor outcome has not been observed in COVID-19 patients receiving oral lansoprazole or rabeprazole alone. Therefore, intravenous PPIs should be prescribed with caution in COVID-19 patients. High-quality studies are needed to provide more solid evidence to further verify the association of PPIs with COVID-19.
Supplemental Material
sj-doc-1-tag-10.1177_17562848221104365 – Supplemental material for Impact of proton pump inhibitors on the in-hospital outcome of COVID-19 patients: a retrospective study
Supplemental material, sj-doc-1-tag-10.1177_17562848221104365 for Impact of proton pump inhibitors on the in-hospital outcome of COVID-19 patients: a retrospective study by Haijuan Yao, Hongyu Li, Zhuang Ma, Yanyan Wu, Yufu Tang, Hao Meng, Hao Yu, Chengfei Peng, Yue Teng, Quanyu Zhang, Tianyi Zhu, Haitao Zhao, Guiyang Chu, Zhenhua Tong, Lu Liu, Hui Lu and Xingshun Qi in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We are indebted to all of the medical staffs who volunteered to participate in the treatment of COVID-19 patients at the Wuhan Huoshenshan Hospital. We would like to appreciate our study team for collecting the data of COVID-19 patients, including Yang An, Ruirui Feng, Li Luo, Yiyan Zhang, and Hongxin Chen, who have not been listed as the co-authors of the current paper.
Authors’ Note
The abstract of the paper has been presented by two major authors as a poster at the 21st Congress of Gastroenterology China (CGC), which was published in 2021 in the Journal of Digestive Diseases (doi: 10.1111/1751-2980.13053).
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.