
Abstract
Diverticulosis and diverticulitis are leading indications for colorectal surgery in Western countries. Abdominal pain, functional disorders, and low health-related quality of life (HRQoL) can limit the outcome of abdominal surgery even in the absence of complications. Therefore, we aimed to review current evidence on postoperative long-term outcomes including HRQoL, functional disorders, abdominal pain, and patients’ satisfaction after diverticular surgery for diverticulosis/diverticulitis. We performed a PubMed database search (inception: 17 December 2020). Identified publications were screened and outcome parameters extracted. In summary, HRQoL increased after diverticular surgery in 9 out of 10 longitudinal cohort studies. Similarly, patients’ satisfaction with treatment and their choice to undergo surgery was commonly reported as high or very good, as reported in eight studies. In a randomized control trial and retrospective cohort, elective diverticular surgery was superior to conservative treatment regarding HRQoL. In cross-sectional analyses, chronic abdominal pain and functional disorders including defaecation disorders or diarrhoea/obstipation were found in a relevant fraction of patients. Incontinence ranged from 5% to 25% with insufficient data for comparison before and after surgery. However, functional disorders did not result in decreased HRQoL in most studies, and no increase in functional disorders was observed after elective diverticular surgery in longitudinal analyses. We conclude that HRQoL among operated patients with diverticular disease improved in most studies after surgery. Functional disorders and postoperative abdominal pain can be present after elective diverticular surgery; however, no increase in functional disorders was observed in longitudinal studies. Functional disorders after diverticular surgery need to be carefully discussed with the patient before surgery and a careful clinical assessment before surgery including incontinence scoring should be considered.
Introduction
Colon diverticulosis and diverticulitis are common diseases affecting patients in developed countries and remain a frequent indication for colorectal surgery. 1 Only 5% of the population younger than 40 years are affected by diverticular disease, whereas this number rises to up to 65% among individuals older than 65 years.2,3 The number of patients treated for diverticulitis has been increasing in the last decades in parallel with increasing age in Western populations. 4
Most patients with diverticulosis remain asymptomatic and only a subset of about 10–20% of patients will develop symptoms of diverticulitis, such as left-sided abdominal pain, fever, chills or altered stool frequency. 5 Although diverticulitis has an increased risk of recurrence, complicated courses after recovery from an uncomplicated episode are rare and do not seem to be influenced by younger age or two or more previous episodes. 6 However, chronic symptoms were found to persist in 5–22% of patients despite uneventful surgical resection. Thus, recommendations for elective surgical treatment of diverticulitis have been shifting from a strict scheme based on the number of previous attacks to a more personalized patient-based approach, considering multiple parameters, such as burden of disease, patient preference, ongoing symptoms and predicted health-related quality of life (HRQoL) after surgery.4,6,7
When balancing the risks and benefits of elective diverticular surgery, considerations regarding long-term outcomes are crucial. Therefore, the aim of this literature review was to summarize available evidence on postoperative HRQoL, functional disorders and pain after diverticular surgery for diverticulitis or symptomatic diverticulosis.
Methods
We screened PubMed from inception to 16 December 2020 in any language using the following search strategy: (((diverticulosis) OR (diverticulitis)) AND (surgery) AND ((pain) OR (patient satisfaction) OR (quality of life)) AND (colon)) (Appendix 1 Figure 2). The inclusion criteria were (1) a clinical study or case series with patients treated surgically due to diverticulosis or diverticulitis, (2) a follow-up after surgery of at least 3 months and (3) endpoints including one or more of the following: abdominal pain, functional abdominal problems, HRQoL and/or patient satisfaction after surgery. Exclusion criteria were (1) article in another language than English or German and (2) case reports or systematic reviews/meta-analyses (however with inclusion of individual studies).
Extracted parameters included study size, centricity, average age, gender proportion, duration of follow-up, numbers lost to follow-up, diagnostic procedures, and the specific indication for surgery among included patients. Furthermore, outcome parameters describing the outcome of the studies, that is, adverse and favourable outcomes and the respective assessment tools, were recorded.
HRQoL estimates daily quality of life according to a subjective evaluation by the patient regarding several aspects of his/her health (e.g. physical or mental limitations, energy level, mood) related to the underlying disease. 8 Several scores have been derived to quantify HRQoL in gastrointestinal diseases. The Gastrointestinal Quality of Life Index (GIQLI) is a widely used disease-specific questionnaire for gastrointestinal, physical and psychological symptoms. 9 Other HRQoL scores include disease-specific questionnaires such as the Fecal Incontinence Quality of Life Scale (FIQoL), 10 the Cleveland Global Quality of Life (CGQL) 11 and Padova Inflammatory Bowel Disease Quality of Life (PIBDQL) 12 for inflammatory bowel disease, and rather general HRQol scores, that is, the Medical Outcomes Survey Short Form 36 (SF-36), 13 EuroQoL 5-D score, 14 and the visual analogue scale (VAS) score for general quality of life.
This literature review summarizes evidence from currently available studies, which had been approved by their respective institutional review boards. Therefore, an additional institutional review for this project was not necessary.
Results
Primary PubMed search identified 620 records (Appendix 1 Figure 1). Three additional publications were retrieved from the list of references of other publications. Out of 623 publications, 583 were excluded after screening of the abstract. From the remaining 40 studies, 17 were excluded after full-text assessment. The remaining 23 publications were included in the final literature review (Appendix 1 Figure 1, Table 1).
General characteristics.
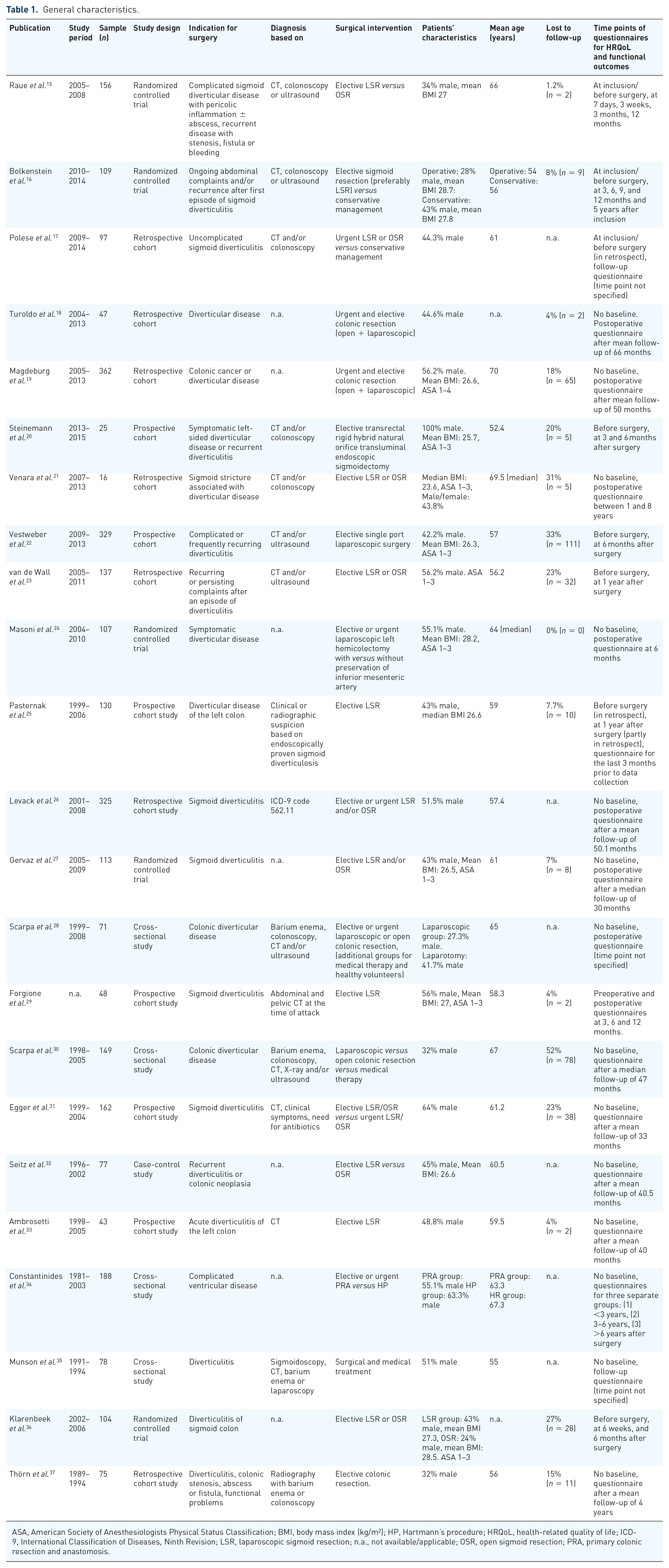
ASA, American Society of Anesthesiologists Physical Status Classification; BMI, body mass index (kg/m2); HP, Hartmann’s procedure; HRQoL, health-related quality of life; ICD-9, International Classification of Diseases, Ninth Revision; LSR, laparoscopic sigmoid resection; n.a., not available/applicable; OSR, open sigmoid resection; PRA, primary colonic resection and anastomosis.
HRQoL and patients’ satisfaction
Out of 23 studies, 20 provided postoperative HRQoL measurements after diverticular resection (Table 2),15–30,32,34,36,37 10 thereof with an additional preoperative questionnaire.15–18,20,22,23,25,29,36 and 2 with a conservatively treated control group.16,17 Among them, HRQoL was recorded in 11 studies after elective surgery.15,16,20–23,25,27,29,32,36
Outcome data.

BIQ, Body Image Questionnaires; BSFS, Bristol Stool Form Scale; CGQL, Cleveland Global Quality of Life; DDSS, diverticular disease symptom score; DV-QoL, Diverticulitis quality of life questionnaire; EORTC-QLQ-C30 v3, European Organisation for Research and Treatment of Cancer Quality-of-life Questionnaire Core 30, 3rd version; EQ5D, EuroQoL 5-D score; FiQoL, Faecal Incontinence QoL Scale; FISI, Faecal Incontinence Severity Index; GIQLI, Gastro-intestinal quality of life Index; HP, Hartmann’s procedure; HRQoL, health-related quality of life; IMA, inferior mesenteric artery; LSR, laparoscopic sigmoid resection; MBFI, Memorial Bowel Function Index; n.a., not applicable/available; OSR, open sigmoid resection; PIBDQL, Padova Inflammatory Bowel Disease Quality of Life; PRA, primary colonic resection and anastomosis; SD, standard deviation; SF-36, Medical Outcomes Survey Short Form 36; VAS, visual analogue scale; ↑, overall improvement in HRQoL after diverticular surgery; ↔, no change in HRQoL after diverticular surgery; ↓, deterioration in HRQoL after diverticular surgery; ?, insufficient information for longitudinal assessment of HRQoL after diverticular surgery.
In most of these studies, HRQoL increased after surgical treatment.15–18,22,23,25,29,36
Some studies deserve special mention. The randomized controlled study with the longest follow-up of 5 years included 108 surgically versus conservatively treated patients suffering from recurrent diverticulitis and/or ongoing symptoms related to diverticulosis. 16 Five years after randomization, GIQLI was significantly higher in the surgical than in the conservative group with a significant improvement from baseline in both groups. However, improved GIQLI scores in the conservative group might be overestimated owing to a relevant cross-over rate to surgery of 46%.
Consistently, data from an Italian retrospective cohort among 97 patients with uncomplicated sigmoid diverticulitis indicate a significantly increased HRQoL after surgical treatment (time points not specified) compared to their conservatively treated peers. 17
HRQoL also increased in two randomized controlled trials upon laparoscopic or open sigmoid resection (the level of statistical significance was not assessed in one study 15 ). In one study, no differences between laparoscopic and open resection were noted, 15 in the other, differences were no longer significant after 6 months. 36
However, a relevant fraction with low overall HRQoL after diverticular surgery was noted in two retrospective,19,26 one prospective 20 and one cross-sectional study, 28 but most of these studies did not have a reference HRQoL at baseline.
Postoperative functional disorders
Fifteen studies reported persistent or new postoperative functional symptoms in the absence of any physical correlate such as inflammation or stenosis15,17,18,24,26,28 (Table 2). Thereof, seven studies provided longitudinal analyses with pre- and postoperative symptoms.20,23,28,29,31,33,35 Furthermore, functional disorders after elective diverticular surgery were recorded in seven studies.15,20,23,29,32,33,37
The most frequently reported functional complaints were defaecation disorders in six studies such as abnormal defaecation, faecal incontinence, difficult or incomplete evacuation, or nocturnal defaecation.18–20,23,24,26 Thereof, two studies provided longitudinal comparisons with a positive impact of both elective laparoscopic and open sigmoid resection on abnormal defaecation in 77.1% in the retrospective cohort study by van de Wall et al., 23 while the prospective cohort study by Steinemann et al. 20 assessing the impact of elective transrectal rigid hybrid natural orifice transluminal endoscopic sigmoidectomy showed no significant improvement in nocturnal defaecation, difficult or incomplete evacuation. The four remaining studies only provided cross-sectional data; new or persistent defaecation disorders were reported among a fourth 18 to a half 24 of the study populations.
The most severe post-surgical defaecation disorder is faecal incontinence. Different measures for incontinence were applied and incontinence rates ranged from 5.4% involuntary stool loss once a week to 11.4% once a month, 19 10%, 24 or 24.8% 26 in other studies. Only in the prospective cohort study by Steinemann et al., 20 St. Marks incontinence score was repeatedly assessed preoperatively and at 6 and 12 months and no significant dynamics upon surgery was observed. Furthermore, faecal urgency was a common postoperative finding among 4.25% of patients in the retrospective cohort study by Turoldo et al., 18 while Magdeburg et al. 19 reported urgency in 3.4% of patients more than once a week and in 12.5% more than once a month. Fragmented or incomplete evacuation was reported in three studies ranging in frequency between 17%, 18 20.8% 26 and 36.4%. 24
Diarrhoea and constipation are equally common after diverticular surgery with rates of diarrhoea ranging from 4% 18 to 23.3% 31 and constipation from 10.4% 32 to 43% 30 of the study populations, respectively. Alternating diarrhoea and constipation was found in 32.7%. 24 Bloating and flatulence were also a common symptom in 14.3% 32 to 30% 30 of patients.
Seven longitudinal studies on functional outcomes after diverticular surgery are available.20,23,28,29,31,33,35 Of these studies, three prospective20,29,33 and one retrospective cohort study 23 focus on elective diverticular surgery.20,23,29,33 Overall, theses longitudinal studies showed an improved or at least unchanged rate of functional disorders. Improvements in defaecation symptoms were found in 77.1% in a retrospective cohort of patients undergoing elective laparoscopic or open sigmoid resection due to ongoing complaints after a first episode of conservatively treated diverticulitis. 23 In a prospective cohort study after elective laparoscopic sigmoid resection (LSR) by Ambrosetti et al., 33 satisfaction with bowel movements improved in 56%, remained unchanged in 37% and worsened in 7%.
However, functional outcomes did not change in two studies. In the prospective cohort study by Steinemann et al. 20 which used an innovative surgical-endoscopic hybrid approach, no postoperative change in stool consistency, nocturnal defaecation, stool evacuation and incontinence was reported, as compared to preoperative symptoms. Similarly, in another prospective cohort study observing patients after LSR due to sigmoid diverticulitis, no difference in stool frequency was noted. 29
Despite a relevant proportion of functional disorders after surgery, most studies reported a good postoperative HRQoL15–18,22,23,25,29,36 and patients’ satisfaction18,21,25,31,33,37 even in the presence of these gastrointestinal symptoms.
Postoperative abdominal pain
Eleven studies assessed postoperative pain during follow-up.15–18,22,23,30–33,35,36 Four studies assessed the dynamics of abdominal pain pre- and postoperatively.17,18,23,33 Eight studies reported on postoperative pain only after elective diverticular surgery.15,16,22,23,27,32,33,36
Decreased abdominal pain after surgery was reported in a randomized controlled trial 16 and two longitudinal studies.18,23 Bolkenstein et al. 16 found a significant decrease in VAS pain levels from baseline in both surgically and conservatively treated patients with ongoing complaints after a first episode or recurrent diverticulitis; however, reduction in pain levels was significantly greater in operated patients compared to their conservatively treated counterparts even 5 years after baseline (p = 0.01). In the retrospective cohort study by van de Wall including 137 patients after elective laparoscopic and open sigmoid resection for diverticular disease, 87.5% experienced decreased abdominal pain after operation. 23 Consistently, the retrospective cohort study by Turoldo et al. 18 reported a significant reduction in abdominal pain among 47 patients after both urgent and elective colonic resection (p = 0.02).
However, the retrospective cohort study by Polese et al. 17 did not find a significant change in pain levels before and after urgent laparoscopic or open sigmoid resection. Other studies reported persistent abdominal pain in 18% 32 and 43%, 30 respectively, or persistent (mostly painful) symptoms in overall 25%. 31 New abdominal pain after surgery was reported in 9.3% in the prospective cohort study by Ambrosetti et al. 33
Patient satisfaction
Patient satisfaction was addressed in six studies. The majority of patients (78–96%) considered surgical results and the functional outcome after surgery to be very good or good;18,21,25,27,31,33,37 90–95% of patients would be willing to undergo the surgery again.18,21,33 In one study, assessment of satisfaction was limited to the cosmetic results which were higher after laparoscopic surgery (97%) than after open surgery (63%). 32
Discussion
Overall, this review summarized evidence from 23 original publications regarding postoperative HRQoL, functional gastrointestinal disorders, and abdominal pain.
Most studies agreed upon a good or even increased HRQoL15–18,22,23,25,29,36 and high patients’ satisfaction regarding the operation.18,21,25,31,33,37 However, literature on functional outcomes and postoperative pain after diverticular surgery is still not sufficient to draw a clear conclusion, especially due to the scarcity of longitudinal assessments and preoperative objective measurements. Nevertheless, a relevant number of studies indicate the possibility of new or persistent abdominal pain,15–18,22,23,30–33,35,36 and a few studies reported unchanged or decreased HRQoL19,20,26,30 even after successful and uncomplicated abdominal surgery. Although functional disorders were commonly reported in almost every forth postoperative patient in cross-sectional analyses,15,17,18,24,26,28–37 there was no evidence for a functional deterioration before and after elective diverticular surgery in longitudinal studies.
These results have to be interpreted cautiously in the light of highly heterogeneous study designs, quality, patients’ selection, operation techniques and length of follow-up. For instance, the outcome measurement tools were not standardized and validated in a relevant subset of studies.31,33,35,37 Therefore, direct comparisons are not meaningful, and a meta-analysis would be potentially misleading.
Various explanations regarding the inconsistent results of the impact of diverticular surgery on HRQoL are conceivable. Obviously, HRQoL, postoperative functional disorders and abdominal pain are very subjective parameters, which may be influenced by a recall bias when recorded retrospectively and may vary according to the setting of urgent and elective interventions as well as the surgical approach for diverticular disease. Furthermore, postoperative complications and related surgical re-interventions may provoke persistent functional disorders and abdominal pain and therefore reduced HRQoL. The current review summarizes the most frequent postoperative complications (Table 2); however, no study stratified for operated patients with and without complications after diverticular surgery in regard to postoperative HRQoL, functional disorders, and abdominal pain, which emphasizes the need for future research in this field.
Several systematic literature reviews and international guidelines6,7 concluded that elective diverticular surgery should not be routinely performed in every patient after the second episode of diverticulitis. There is a broad consensus on a lower risk for recurrent diverticulitis or other complications of diverticulosis after surgery with a diverticulitis recurrence rate of 4.2% after elective LSR for diverticulitis. 38 However, surgery should be indicated after a careful and thorough individualized patient selection since previous episodes of uncomplicated diverticulitis were not found to predict recurrence, severity of future attacks, and need for emergency operations. 39
Another factor is the presence of irritable bowel syndrome (IBS) in patients undergoing diverticular surgery which could be one of the reasons for reduced postoperative HRQoL, persistent or increasing functional symptoms, and abdominal pain. This is relevant since the prevalence of IBS is estimated to be as high as 17% among patients with diverticular disease. 40 Therefore, screening, early recognition and adequate treatment of preoperative IBS are warranted before the evaluation of elective diverticular surgery.
Conversely, Cohen et al. 41 stated that patients with diverticulitis could be at risk for subsequent development of de novo IBS and other functional disorders and proposed the term post-diverticulitis IBS for this disorder. Furthermore, Jung et al. 42 reported a significantly increased likelihood for colonic diverticulosis in patients with IBS. These associations of IBS and colonic diverticular disease might be due to a shared etiopathogenesis of both conditions. Therefore, similar to post-infectious IBS, an attack of diverticulitis could trigger functional bowel disorders and post-diverticulitis IBS might be a variant of post-inflammatory IBS. Post-diverticulitis IBS might be responsible for functional disorders after surgery for diverticular disease in some cases.
Especially for elective diverticular surgery, predictors for a favourable postoperative outcome regarding HRQoL, functional disorders and abdominal pain guiding this decision process are needed. Predictors for favourable postoperative outcomes and high patients’ satisfaction were male sex, 26 absence of preoperative IBS, 33 length of the resected colon, 33 elective setting of the operation, multiple previous episodes of diverticulitis and low preoperative HRQoL.25,29 Preoperative screening could be expanded using the validated irritable bowel severity scoring system by Francis et al. 43 to identify the presence of IBS before surgery. Furthermore, factors predisposing for IBS such as the gastrointestinal symptom-related anxiety and depression, a high Visceral Sensitivity Index, 44 and high scores in the Hospital Anxiety and Depression Scale 45 could be identified preoperatively. These factors might also be relevant as predictors for functional problems after diverticular surgery. However, such a strategy would need confirmation in larger prospective observational studies or dedicated randomized clinical trials.
Irrespective of positive results in most studies, a minority of patients remained with low/reduced HRQoL, persistent symptoms, new symptoms, abdominal pain and/ or low satisfaction with therapy. These unfavourable results can be a significant burden for patients and physicians. Strategies to reduce the rates of unfavourable outcomes including patient selection would be desirable and efficient strategies to support affected patients are needed. The least physicians can do now is to communicate the possibility of unfavourable outcomes clearly and transparently to patients before surgery.
Strength of the current review includes the large number of affected studies with overall 2948 patients. Limitations include the heterogeneous study design of most identified studies, precluding a quantitative summary or a meta-analysis. Furthermore, most studies have an observational (noninterventional) study design and large randomized controlled trials with preoperative assessment of risk factors, and long-term outcomes regarding abdominal function, pain and HRQoL assessed by validated and standardized tools would be desirable.
Conclusion
The decision for elective diverticular surgery is complex. In recent years, surgical guidelines evolved from a strict recommendation for surgery after the second attack of diverticulitis to a more individualized approach. Current literature points to an improved HRQoL in most patients upon short- and long-term follow-up for up to 5 years. However, data on functional outcomes are controversial; while cross-sectional analyses found functional disorders after diverticular surgery in a relevant proportion of patients, functional disorders did not deteriorate in four longitudinal studies after elective diverticular surgery. Thus, careful preoperative clinical assessment regarding functional impairments including IBS and incontinence scoring should be considered. Finally, the indication for elective diverticular surgery should be discussed carefully with the patient, especially when preoperative IBS and predictors thereof are present.
Footnotes
Appendix 1
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Misselwitz reports grants from MSD; personal fees from MSD, Vifor and Takeda, outside the submitted work. Dr Segna reports travelling fees from AbbVie, Vifor and Gilead and a research grant from the Novartis Foundation for Medical-Biological Research unrelated to this project. The other authors have nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.