
Abstract
Background:
Small bowel enteropathy (SBE) is a complication of nonsteroidal anti-inflammatory drug (NSAID) therapy occurring in 71% of NSAID users. We aimed to analyse the efficacy and safety of medications to prevent and treat NSAID-induced SBE in randomized controlled trials (RCTs).
Methods:
This review was registered on PROSPERO (CRD42021223371). We systematically searched four databases until 20 October for comparing mucoprotective (MP), antibiotic and probiotic treatments to placebo, proton-pump inhibitors (PPIs) or histamine-2 (H2) receptor antagonists in NSAID-associated small intestinal injuries. The main outcomes were mucosal integrity, mucosal breaks after treatment, mucosal injury improvement and complete healing of mucosal breaks. Meta-analytical calculations for weighted mean differences (WMDs) and odds ratios (ORs) were performed with the random-effects model and interpreted with 95% confidence intervals (CIs).
Results:
A total of 18 RCTs were included in the quantitative synthesis. MP medications administered preventively reduced the number of mucosal erosions (WMD = −1.24, CI: −2.15 to −0.34) and lead to a significantly lower chance of developing mucosal breaks after treatment (OR = 0.38, CI: 0.16–0.93). MP therapy was associated with a higher rate of complete healing of mucosal breaks (OR = 5.39, CI: 2.79–10.42). In the qualitative synthesis, there were tendencies for a lower increase in the mean number of mucosal breaks and reddened lesions with prophylactic and a higher decrease in mucosal breaks with therapeutic MP drug administration.
Conclusion:
MP treatment administered with NSAIDs can prevent and reduce small intestinal mucosal lesions.
Introduction
Nonsteroidal anti-inflammatory drugs (NSAIDs) are among the most frequently prescribed drugs worldwide.1,2 As capsule endoscopy (CE) became more available in the past two decades, small bowel enteropathy (SBE) started to get much more attention among NSAID users. While the incidence of upper gastrointestinal (GI) events decrease, an increasing trend in lower GI events was observed among these patients. 3 Manifestations of SBE are nonspecific, with various signs and symptoms, including abdominal discomfort, diarrhoea and constipation, and consequences like iron-deficiency anaemia or protein loss. Moreover, life-threatening ulcer complications, bleeding and perforation can also appear in this population. 4
The pathogenetic mechanisms of NSAID-induced small bowel injuries are still not fully elucidated. It is known that NSAIDs going through enterohepatic recirculation are more potent to induce mucosal lesions. Inhibition of prostaglandin synthesis, direct damage to the intestinal epithelial cells, increased intestinal permeability and altered gut microbiota are associated with these medications.5,6 A recent study demonstrated that NSAID-triggered inflammatory signals can activate the NLRP3 inflammasome. 7 This protein plays a crucial role in SBE, as it affects gut homeostasis by modulating the interactions between the innate immune system, intestinal epithelium and microbiota. 6
Discontinuation of NSAIDs should be the first step in SBE treatment, but it can aggravate patients’ comorbidities that they take these drugs for. Serious cardiovascular events had a higher chance in patients who stopped aspirin, although those who continued were more likely to have melena or hematochezia. 8 To prevent gastroduodenal injuries, acid secretion suppressing therapy is commonly prescribed for NSAID consumers. However, previous randomized controlled trials (RCTs) have already demonstrated that proton-pump inhibitors (PPIs) and histamine-2 (H2) receptor antagonists cannot protect the mucosa of the small intestine compared with mucoprotective (MP) drugs, such as irsogladine, rebamipide or geranylgeranylacetone (GGA).9–12
As small intestinal injuries were described in 71% of NSAID users, prevention and treatment of SBE are crucial to prevent relevant complications. 13 One meta-analysis has already shown the rebamipide’s protective impact in NSAID-induced SBE compared with placebo. 14 However, a study on rats proved the superiority of irsogladine compared with rebamipide or GGA. 15 A recent systematic review also showed the beneficial effect of different probiotics on the small bowel. 16 However, the existing data on this topic have not been systematically reviewed and meta-analysed to show the specific medical treatments’ effect. We aimed to comprehensively assess the impact of MP and other medications on NSAID-induced SBE.
Materials and methods
Our systematic review and meta-analysis is reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2009 Statement. 17 We performed this study following the Cochrane Handbook’s recommendations for Systematic Reviews of Interventions, Version 6.1.0. 18 The review protocol was registered in advance on PROSPERO under registration number CRD42021223371 (see https://www.crd.york.ac.uk/prospero).
Systematic search and eligibility criteria
A systematic literature search was performed in four major medical databases: MEDLINE (via PubMed), Cochrane Library (CENTRAL), Embase and Scopus from inception to 20 October 2020. The query, including different types of NSAIDs, enteropathy-related terms and the word ‘random*’ (see Supplementary Material), was applied to all fields in the search engines, except for Scopus, where we used it in the title–abstract–keyword sections. There were no language or other restrictions imposed.
We included RCTs reporting on patients with NSAID-induced SBE diagnosed with CE before and after receiving treatment. Based on the presence or absence of the SBE in study participants at the trials’ initiation, we formed two population-intervention-control-outcome (PICO) frameworks. The main differences between the two PICOs were in the study population and the primary outcome.
P – Articles discussing (PI.) adult patients who did not have NSAID-induced SBE and started the NSAID therapy on the first day of the trial were included in the prevention group. In the treatment group (PII.), we accepted studies that discussed chronic NSAID users (>18 years old) diagnosed with SBE.
I – For both groups as intervention (I), we accepted any treatment that could prevent the formation or reduce the number of small intestinal lesions.
C – When the study population received PPIs or H2-receptor antagonist, we accepted only the placebo (C1) as a comparator. If PPI or H2-receptor antagonist was not applied along with the NSAID treatment, we allowed PPIs (C2) or H2-receptor antagonist (C3) as comparators.
O – Primary outcomes for the prevention group were mucosal integrity (OI.I.1.) and mucosal breaks after treatment (OI.I.2.); primary outcomes for the treatment group were mucosal injury improvement (OI.II.1.) and complete healing of mucosal breaks (OI.II.2.). Details of the primary outcomes are enclosed in the Supplementary Material. Our secondary outcomes for both groups were the following: change in faecal calprotectin level, haemoglobin level, small bowel transit time, Lewis score and adverse events (OII.).
All articles and abstracts without full text were eligible that contained at least one of our outcomes. In the case of mucosal integrity and injury improvement, we selected only those studies that provided sufficient data on the number of lesions before and after treatment, both in the intervention and control groups. Outcomes reported only in one or two RCTs and articles using non-MP agents as intervention were included only in the systematic review. There was no overlap between the studies. We did not find additional RCTs after checking and comparing the reference list of the included articles.
Study selection and data collection
We used a reference management software for the yielded articles’ selection (EndNote X9, Clarivate Analytics, Philadelphia, PA, USA). After duplicate removal, publications were screened separately by two independent authors (B.T., E.B.) for the title, abstract and full text. Cohen’s kappa coefficient (κ) was calculated after each step to measure interrater reliability. 19 In case of any disagreement, consensus was reached by a third investigator’s arbitration (Sz.V.).
Two authors (B.T., E.B.) independently extracted the relevant data into a predefined Excel spreadsheet (Office 365, Microsoft, Redmond, WA, USA). The following data were collected from each eligible article: first author, Digital Object Identifier (DOI), year of publication, study type (full text or conference abstract), study location, time period, number of centres included in the study, study design, demographic data (sample sizes, age, percentage of participating males), details of the received treatments and data regarding our dichotomous (presence of event in the intervention and control groups, and the number of participants in each group) and categorical outcomes (change in the outcome in the intervention and control groups, before and after treatment) for statistical analysis. A third reviewer (B.E.) resolved the discrepancies between the two authors.
When the outcome definitions about mucosal injuries in the articles did not meet the prespecified definitions (see Supplementary Material), we renamed the respective outcome when it was possible. Authors of eligible articles were also contacted for additional outcome data.
Quality assessment and quality of evidence
Quality assessment was performed with the revised tool for assessing the risk of bias (RoB 2) by the Cochrane Collaboration. 20 We followed the recommendation of the ‘Grades of Recommendation, Assessment, Development, and Evaluation (GRADE)’ workgroup to evaluate the quality of evidence. 21 Summary of Findings table and the additional tables were prepared with the GRADEPro Guideline Development Tool. 22 Two reviewers assessed the risk of bias and quality of the outcomes separately (B.T., L.F.). Disagreements between the assessors were resolved by discussion and the involvement of a third reviewer (Sz.V.).
Data synthesis and analysis
The minimum number of RCTs was three for performing a meta-analytical calculation on an outcome. We collected incidences from the treatment and control groups and calculated pooled odds ratios (ORs) with a 95% confidence interval (CI) in the case of categorical outcomes (mucosal breaks after treatment and complete healing of mucosal breaks). For continuous outcomes (mucosal integrity, mucosal injury improvement, faecal calprotectin level, small bowel transit time and haemoglobin level), a weighted mean difference (WMD) with a 95% CI was calculated from the mean differences between the pre- and posttreatment means. Where the means and standard deviations were not available, we used medians, minimum, maximum, first quartile and the third quartile to estimate them, using the method of Wan and colleagues. 23 When the p value for the mean difference was not published, we estimated the t value based on a two-sample t test; however, that considered that the outcomes before and after the intervention are not in pairs.
All analyses were performed in Comprehensive Meta-Analysis (Version 3) statistical software (Biostat, Inc., Englewood, NJ, USA). A p value of less than 0.05 was considered to be statistically significant. We used the random effect model by DerSimonian and Laird in the quantitative synthesis. 24 Heterogeneity was tested with I² and χ² tests. Q test less than 0.1 was interpreted as indicating significant heterogeneity. Sensitivity analysis was carried out in the case of one outcome (small bowel transit time). Trial Sequential Analyses (TSAs 0.9.5.10. Beta, Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet, Copenhagen, Denmark) were also performed to quantify the statistical reliability and estimate the optimal information size. Publication bias could not be interpreted by visual inspection of the Funnel plots, and Egger’s test could not be performed as the number of the studies for each outcome was less than 10.
We intended to perform subgroup analyses based on the type of medication. However, because of the insufficient number of articles, our subgroups (PGIAs – prostaglandin increasing agents) included interventions with a common mechanism: the elevation of the serum and small intestinal prostaglandin level.
Protocol deviation
We did not find data regarding mucosal bleeding sites, faecal occult blood test and severity of mucosal injuries. However, we included three additional outcomes: mucosal breaks after treatment, small bowel transit time and Lewis score. Statistical analysis was performed with Comprehensive Meta-Analysis software, mucosal integrity and mucosal injury improvement were considered continuous outcomes and subgroup analyses with PGIAs were performed.
Results
Systematic search and selection
Our systematic search provided a total of 3341 duplicate-free records. After title, abstract and full-text selection, we identified 26 RCTs9–12,25–47 for our qualitative synthesis. We included 12 articles on the prevention9,11,12,26–29,35,38,40,42,46 and 6 articles on the treatment31,32,39,44,45,47 of NSAID-induced SBE in the quantitative synthesis. We selected one conference abstract where relevant information was reported 39 and included an additional RCT 35 as we identified the full text of a conference abstract from our comprehensive search. The summary of the selection process is shown in Figure 1.

PRISMA flow diagram of the screening and selection process.
Main characteristics of the included studies
Characteristics of the identified RCTs for the systematic review and meta-analytical part of our article are detailed in Table 1 and Supplemental Table S2.
Main characteristics of the included studies.

Bif195, Bifidobacterium breve Bif195; CFUs, colony forming units; ESH, egualen sodium hydrate; GGA, geranylgeranylacetone; LC, Lactobacillus casei, LG, Lactobacillus gasseri; N/A, data not available; NSAID, nonsteroidal anti-inflammatory drug; RCTs, randomized controlled trials.
Cross-over study design, washout period of 2 weeks.
Cross-over study design, washout period of 4 weeks.
Multiple centres.
Conference abstract.
Age in median.
Quantitative synthesis
Efficacy of MP drugs in the prevention of NSAID-induced SBE
Mucosal integrity
Out of all the outcomes regarding mucosal integrity (see Supplemental Table S3), only mucosal erosion had enough data published for meta-analysis (see Figure 2; see Supplemental Table S1). Five RCTs9,11,12,26,40 (with a total of 146 subjects) showed a 60% lower increase in the mean number of mucosal erosions when treated preventively with MP drugs (WMD = −1.24, CI: −2.15 to −0.34; I2 = 92.0%, p < 0.001). Subgroup analysis confirmed the beneficial effect of PGIAs. The increase in the mean number of mucosal erosions was 38% lower in the intervention group (WMD = −1.15, CI: −2.17 to −0.12; I2 = 92.1%, p < 0.001).

Forest plot representing that preventive mucoprotective agents are associated with fewer mucosal erosions compared with control.
Mucosal breaks after treatment
The risk of developing mucosal breaks was reduced after treatment with all MP drugs pooled (OR = 0.38, CI: 0.16–0.93; I2 = 47.9%, p = 0.088), but not in the PGIA subgroup (OR = 0.35, CI: 0.12–1.04; I2 = 42.5%, p = 0.157) (see Figure 3).9,27,28,35,38,46
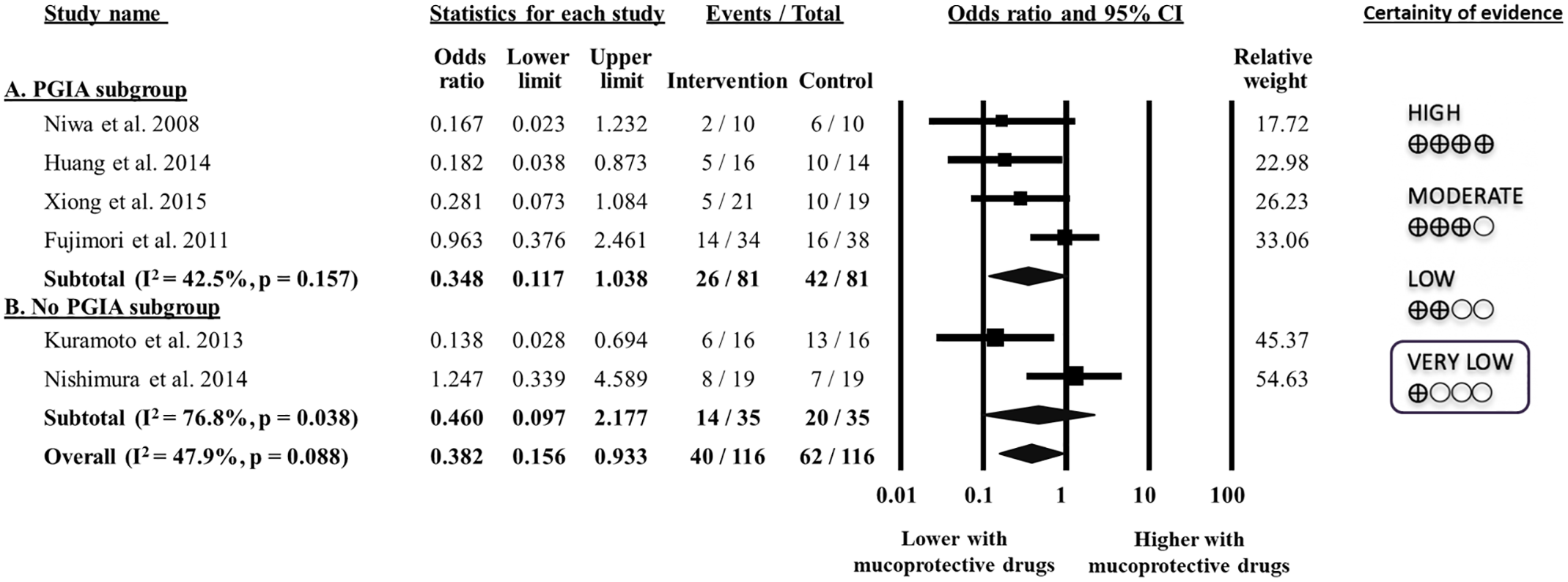
Forest plot of studies representing that preventive treatment with mucoprotective agents is associated with a reduced risk of mucosal breaks after treatment compared with control, but not for the PGIA subgroup.
Mucosal breaks
Three articles27,28,35 including 140 participants showed a 82% lower increase in the number of the mucosal breaks in the PGIA subgroup (WMD = −9.67, CI: −11.67 to −7.67; I2 = 16.3%, p = 0.274), but not with all MP drugs (WMD = −4.96, CI: −14.14 to 4.22; I2 = 98.2%, p < 0.001) (see Supplemental Figure S1).
Reddened lesions
In total, 141 patients from three RCTs9,27,35 had CE to visualize reddened lesions. However, the number of these lesions did not show a significantly lower increase when treated preventively with MP treatment (WMD = −2.96, CI: −7.01 to 1.17; I2 = 99.7%, p < 0.001) (see Supplemental Figure S2).
Faecal calprotectin level
Pooled WMDs from five RCTs9,11,12,29,35 (149 subjects) did not show difference in the faecal calprotectin level (WMD = −5 mg/l, CI: −17 to 8; I2 = 91.4%, p < 0.001) (see Supplemental Figure S3). However, the PGIA subgroup including only two articles showed a significantly lower elevation with 83% in the faecal calprotectin level when MP drugs were administered (WMD = −11 mg/l, CI: −19 to −3; I2 = 92.6%, p < 0.001) compared with the control group.
Small bowel transit time
Five studies11,12,26,38,42 provided data regarding this outcome, including a total of 130 participants (see Supplemental Figure S4). Treatment with PGIAs could not reduce the small bowel transit time significantly; however, it was 64% longer compared with the control group (WMD = −16 min, CI: −38 to 5; I2 = 77.0%, p = 0.002). A sensitivity analysis (leave-one-out method) identified an influential study 11 that changed the results; without it, the small bowel transit was slower by 70% in the intervention group (WMD = −27 min, CI: −40 to −13).
Efficacy of MP drugs in the treatment of NSAID-induced SBE
Mucosal injury improvement
There were sufficient data only for mucosal breaks to allow meta-analytical calculation. The other outcomes are systematically detailed in Supplemental Table S4. Five studies31,32,39,44,45 analysing 236 patients did not show significant difference between the two groups (WMD = −3.70, CI: −11.05 to 3.63; I2 = 98.9, p < 0.001) (see Supplemental Figure S5). However, by the end of the treatment the change in the mean number of mucosal breaks was 79% lower in the intervention group. On the other hand, the change was 83% lower for the subgroup receiving PGIA agents, but the difference was not significant as well (WMD = −4.58 number, CI = −12.80 to 3.64; I2 = 99.2%, p < 0.001).
Complete healing of mucosal breaks
Four RCTs31,32,44,47 assessed this outcome. Among 285 participants, 56 in the intervention group (out of 148) and 15 in the control group (out of 137) reached this event. Pooled analysis demonstrated that MP drugs lead to a significantly higher chance of complete healing of mucosal breaks (OR = 5.39, CI: 2.79–10.42; I2 = 0.0%, p = 0.839) (see Figure 4).

Forest plot of studies representing that treatment with mucoprotective agents is associated with a higher chance for complete healing of mucosal breaks compared with control.
Haemoglobin level
A total of 272 patients from four RCTs31,32,44,47 provided data regarding the haemoglobin level. There was no difference between the ones treated with PGIA and the ones receiving placebo (WMD = 0.46 g/dl, CI: −0.03 to 0.96; I2 = 70.4%, p = 0.017) (see Supplemental Figure S6).
Qualitative synthesis
Adverse events
In the prevention group, four RCTs reported adverse events.9,10,33,46 Only those patients who experienced adverse reactions received Bifidobacterium breve Bif195; 33 however, there was no significant difference between the intervention (8 subjects out of 38) and control groups (14 subjects out of 37) (see Supplemental Table S5). Four studies37,38,41,42 using GGA, rifaximin and rebamipide assessed serious adverse reactions, and there was none reported (see Supplemental Table S6).
In the treatment group from five RCTs,25,30,32,44,47 side effects were noted in two,32,47 when misoprostol was the intervention. A total of 35 participants out of 92 (38.04%) reported adverse events and 2 subjects out of 92 (2.17%) reported serious adverse events. There were no significant differences between the intervention and control groups regarding adverse and serious adverse reactions (35/92 versus 33/94 and 2/92 versus 1/94, respectively). Participants reported no side effects with Lactobacillus casei, irsogladine and rebamipide, and investigators did not observe serious side effects when patients received Lactobacillus gasseri or rebamipide (see Supplemental Tables S7 and S8).
Prevention group
Mucosal integrity
Five articles assessing this outcome presented a lower increase in the mean number of mucosal injuries, 35 breaks, 41 ulcers11,12 and erosions 34 when treated with the specific intervention. Only one RCT 40 found a higher increase in the number of mucosal injuries.
Lewis score
Umegaki and colleagues 11 administered GGA as a preventive treatment and revealed a decrease in the mean Lewis score of patients (WMD = −90, CI: −105.7 to −74.5).
All the above-listed information is detailed in Supplemental Table S3.
Mucosal breaks after treatment
Scarpignato and colleagues 41 administered rifaximin as an intervention to 24 study participants and placebo as a comparator to 17 subjects. In the intervention group, only 6 patients developed mucosal breaks at the end of the treatment; meanwhile, mucosal breaks were evaluated in 13 patients in the control group.
Treatment group
Mucosal injury improvement
All the included five RCTs25,30,31,45,47 demonstrated a decrease in the mean number of mucosal injuries, 30 breaks, 25 ulcers and erosions,31,47 and reddened lesions25,31,45 for the participants in the intervention group.
Haemoglobin level
Treatment with Lactobacillus casei led to an increase in the haemoglobin level compared with no intervention. 25
Lewis score
Two articles reported this outcome,25,45 assessing a decrease in the Lewis score after using Lactobacillus casei 25 and polaprezinc 45 as an intervention.
Data regarding the outcomes mentioned above are detailed in Supplemental Table S4.
Risk of bias assessment
The result of the assessment of the risk of bias of the included studies in the meta-analysis (Supplemental Figures S7–S15) and systematic review (Supplemental Figures S16–S21) is detailed in the Supplementary Material. One of the included studies was at high risk of bias, as it was available only as a conference abstract. 39 In 11 articles, the bias regarding randomization process domain was at ‘some concerns’.6,11,34,35,37–42,46 Measurement of the outcome, missing outcome data and deviation from the intended intervention domains were at the lowest risk of bias in all the articles.
Trial sequential analysis
TSA was performed for all the outcomes included in our quantitative synthesis (see Supplemental Figures S22–S30). For mucosal erosions and complete healing of mucosal breaks, the cumulative Z-curve crossed the monitoring boundary. This means that additional trials are not necessary for these two outcomes, as the required optimal sample size was reached in the included RCTs. The futility boundary was reached only in the case of complete healing of mucosal breaks suggesting that the addition of more RCTs is unlikely to show any effect on the outcome.
Quality of evidence
Six outcomes regarding prevention and three about the treatment of SBE were included in our Summary of Findings (see Supplemental Tables S9 and S10). The quality of evidence was moderate for the complete healing of mucosal breaks (treatment group); however, it was very low for the other quantitative synthesis outcomes. The quality of evidence for the systematic review is detailed in Supplemental Tables S11 to S13.
Discussion
This systematic review and meta-analysis evaluated the prophylactic and therapeutic effects of specific interventions in NSAID-induced SBE. Our findings provided evidence that patients without SBE who received MP treatment had fewer mucosal erosions. Those who had PGIA as intervention had fewer mucosal breaks and erosions at the end of the study (very low certainty). Furthermore, preventive treatment with MP drugs led to a lower chance for the appearance of mucosal breaks after NSAID treatment and a lower faecal calprotectin level when treated with PGIA (very low certainty). We also demonstrated that the odds for complete healing of mucosal breaks was higher in subjects with SBE who received MP drugs as treatment (moderate certainty).
Moreover, based on the TSA, further studies are not necessary for this outcome, as they are not likely to change our findings. There were clear tendencies of less increased mucosal breaks, reddened lesions and small bowel transit time in the prevention group, and decreased number of mucosal breaks and increased haemoglobin level in the treatment group, favouring the intervention (very low certainty). However, based on the TSA, larger sample sizes are required to see the intervention’s effect on these outcomes.
Previous animal studies revealed the protective impact on the small bowel of all the interventions included in this quantitative synthesis (rebamipide, irsogladine, misoprostol, GGA or teprenone, egualen sodium hydrate, and isinglass or muscovite).4,15,48–50 Although the mechanisms of action are different, our findings and the results of the individual studies included in the qualitative synthesis have also shown the beneficial effect of these medications. Rebamipide, GGA, misoprostol, isinglass and ecabet sodium could be included in our PGIA subgroup based on their mechanism of action. They elevate the prostaglandin levels in the serum and small intestinal mucosa, resulting in an increased mucosal blood flow, enhanced mucus and bicarbonate secretion, thus promoting mucosal defence.4,5,48,51 Animal studies on ecabet sodium’s effect on the small bowel were not found, but it shares common mechanisms in the gastric mucosa with rebamipide. It was assumed to act similarly in the small intestine, too. 40
Previous clinical and animal studies showed that co-administration of PPIs with NSAIDs is harmful to the small bowel mucosa.52,53 These treatments were given to most of our study participants to prevent gastroduodenal lesions. It is essential to highlight that PPIs or H2-receptor antagonists’ potentially damaging impact remained unnoticeable in our review. Based on our results, MP treatments could prevent and improve small intestinal mucosal injury formation when acid suppressants were administered, additionally to NSAID therapy. In four of the included RCTs, the control group received acid suppressants instead of placebo.9,11,12,39 All four RCTs confirmed the interventions’ superiority which may be driven by anti-acid medications’ detrimental effects. In addition, when we assessed the interventions’ effect in studies without acid secretion inhibiting drugs as a placebo, we also saw its benefit.10,34,46
All medications, besides ecabet sodium, 40 included in the meta-analysis also showed a favourable impact on mucosal integrity and injury improvement in the qualitative analysis. Polaprezinc treatment, with its anti-inflammatory effect and intercellular tight-junction protection, could also reduce the number of reddened lesions and the Lewis score. 45
Regarding antibiotic and probiotic treatment in SBE, our findings confirmed their benefits as published in a recent systematic review. 16 Gram-negative bacteria dominance in the small intestine can increase ulcer formation risk during NSAID treatment. 5 Moreover, a previous study demonstrated PPIs’ harmful consequences on the small bowel with its use resulting in dysbiosis. 53 Rifaximin can increase the barrier function of the epithelium besides acting against Gram-negative bacteria. 16 We found that it also helped to prevent the formation of mucosal breaks. 41 Regarding Lactobacillus casei, we assumed that it could improve mucosal injury and decrease Lewis score, as it has an anti-inflammatory effect on the mucosa. 25 Also, Lactobacilli are well known to inhibit Gram-negative bacterial overgrowth by lowering the pH through lactic acid production. 54
Of all the interventions, only Bifidobacterium breve Bif195 and misoprostol were reported to cause side effects. Treatment with misoprostol induced two serious adverse reactions in 92 patients, which must be considered regarding NSAID-induced SBE treatment. However, it is important to highlight that there were no significant differences between the intervention and control groups regarding these outcomes.
Strengths and limitations
To the best of our knowledge, our work is the first meta-analysis and systematic review assessing MP drugs’ effect on NSAID-induced SBE. We used a rigorous methodology, the study process is transparent and the data collection was precise and detailed.
However, our study has limitations. RCTs included in our analysis used different NSAIDs, interventions and controls with different dosages and in some cases, the whole population received PPIs or H2-receptor antagonists. In these articles, the sample sizes were small, the follow-up periods were short and different, and certain RCTs had crossover design. Most of the studies were conducted in Asia. Participants were approximately two decades younger in the RCTs on prevention than the participants of RCTs on the treatment of SBE. Males were predominant in both groups. The means of the number of lesions were converted from medians which affect the WMDs. Moderate risk of bias and high heterogeneity within the studies included in our meta-analysis is also a limitation of this article. Publication bias could not be adequately assessed because of the low number (<10) of articles for the outcomes.
Implications for research
We could see the beneficial effect of every intervention in our review; however, further RCTs are needed with the same intervention, same dosage, longer follow-up period and larger sample sizes to decide which drug is the most effective.
The effect of the included interventions compared with PPIs or H2-receptor antagonists should also be assessed on the gastroduodenal mucosa. In case of the superiority of MP drugs, secretion inhibitors could be replaced with them because the MP treatment would affect the small intestine as well. We also propose cost-effectiveness analyses studies, as none of the included RCTs assessed the price of treatments, and it is a crucial factor of decision making.
Implications for practice
In the current practices, administration of PPIs or H2-receptor antagonists alongside NSAIDs prevents gastroduodenal injuries. However, based on the literature and our present results, they cannot prevent SBE. We suggest that all patients taking NSAIDs should receive MP medication in addition to acid suppressant treatment.
Conclusion
In summary, we demonstrated that additional MP treatment to NSAIDs prevents small intestinal injuries and reduces the number of mucosal lesions. Also, we summarized the evidence which supports the administration of these drugs alongside the currently used acid-suppressing agents such as PPIs and H2-receptor antagonists.
Supplemental Material
sj-docx-1-tag-10.1177_17562848211038772 – Supplemental material for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-tag-10.1177_17562848211038772 for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials by Brigitta Teutsch, Eszter Boros, Szilárd Váncsa, Alex Váradi, Levente Frim, Szabolcs Kiss, Fanni Dembrovszky, Zsuzsanna Helyes, Sarlós Patrícia, Hegyi Péter and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-zip-1-tag-10.1177_17562848211038772 – Supplemental material for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-zip-1-tag-10.1177_17562848211038772 for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials by Brigitta Teutsch, Eszter Boros, Szilárd Váncsa, Alex Váradi, Levente Frim, Szabolcs Kiss, Fanni Dembrovszky, Zsuzsanna Helyes, Sarlós Patrícia, Hegyi Péter and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-zip-2-tag-10.1177_17562848211038772 – Supplemental material for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-zip-2-tag-10.1177_17562848211038772 for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials by Brigitta Teutsch, Eszter Boros, Szilárd Váncsa, Alex Váradi, Levente Frim, Szabolcs Kiss, Fanni Dembrovszky, Zsuzsanna Helyes, Sarlós Patrícia, Hegyi Péterand Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-zip-3-tag-10.1177_17562848211038772 – Supplemental material for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-zip-3-tag-10.1177_17562848211038772 for Mucoprotective drugs can prevent and treat nonsteroidal anti-inflammatory drug-induced small bowel enteropathy: a systematic review and meta-analysis of randomized controlled trials by Brigitta Teutsch, Eszter Boros, Szilárd Váncsa, Alex Váradi, Levente Frim, Szabolcs Kiss, Fanni Dembrovszky, Zsuzsanna Helyes, Sarlós Patrícia, Hegyi Péter and Bálint Erőss in Therapeutic Advances in Gastroenterology
Footnotes
Brigitta Teutsch helped in conceptualization, project administration, data curation and writing original draft. Eszter Boros helped in conceptualization, data curation and visualization. Szilárd Váncsa contributed to conceptualization, data curation and methodology. Alex Váradi helped in conceptualization and formal analysis. Levente Frim helped in conceptualization and data curation. Szabolcs Kiss contributed to conceptualization, methodology and validation. Fanni Dembrovszky contributed to conceptualization and validation. Zsuzsanna Helyes and Patrícia Sarlós contributed to conceptualization and writing – review and editing. Péter Hegyi helped in conceptualization, funding acquisition and writing – review and editing. Bálint Erőss contributed to conceptualization, methodology, supervision and writing original draft. All authors provided critical conceptual input and approved the final version of the article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Economic Development and Innovation Operational Programme Grant (GINOP-2.3.2-15-2016-00048 – STAY ALIVE; GINOP-2.3.4-15-2020-00010 – Competence Center for Health Data Analysis, Data Utilization and Smart Device and Technology Development at the University of Pécs) and by a Human Resources Development Operational Programme Grant (EFOP-3.6.1.-16-2016-00004 – Comprehensive Development for Implementing Smart Specialization Strategies at the University of Pécs), both supported by the European Union. Furthermore funding was provided by the ÚNKP20-3, a New National Excellence Programme of the Ministry for Innovation and Technology from the source of the National Research Development and Innovation Fund (to Sz.V.) and by the National Research, Development and Innovation Office (grant FK132834 to P.S.). The project was co-financed by the European Social Fund. Sponsors had no scientific role in our study. They were not involved in the study selection, data collection, analysis, interpretation and manuscript preparation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.