
Abstract
Background:
Colonic neuroendocrine carcinomas (co-NECs) are heterogeneous and aggressive, especially with regard to metastasis. Whether co-NECs on the right and left sides of the colon have different characteristics from colon adenocarcinoma is unknown.
Methods:
The co-NEC patients were selected from the 2010–2017 Surveillance, Epidemiology, and End Results Program (SEER) database. The right and left sides of the colon were separated by the splenic flexure. Coarsened exact matching (CEM) was performed to adjust for relevant factors before regression models were constructed.
Results:
A total of 669 pathologically diagnosed co-NEC patients with sufficient baseline data were identified from the SEER database. A total of 80.72% of the patients had co-NEC that originated from the right side of the colon, and their mean overall survival (mOS) was similar to that of the patients with left-sided co-NECs (right versus left: 22.30 m versus 22.55 m). A total of 44.84% of the patients were diagnosed with liver metastasis (46.68% right side versus 37.98% left side). In patients with liver metastasis, those with right-sided co-NECs had better survival than those with left-sided co-NECs (mOS right versus left: 15.37 m versus 9.62 m; adjusted hazard ratio (HR) = 0.69, 95% confidence interval (CI): 0.49–0.98, p = 0.035). To further investigate the survival benefits of primary site resection, we separated the patients who had liver metastasis according to the primary site and performed CEM to balance the groups (no patients underwent liver metastasis resection or intervention). The results suggested that primary surgery could benefit patients with both left- and right-sided co-NECs (adjusted HR = 0.50, 95% CI: 0.33–0.77, p = 0.001 on the right side; HR = 0.38, 95% CI: 0.16–0.89, p = 0.026 on the left side).
Conclusions:
Co-NECs frequently originate on the right side and commonly develop liver metastasis. Right-sided co-NECs are associated with better survival than left-sided co-NECs after liver metastasis has occurred. Primary site resection is associated with prolonged survival in co-NEC patients with liver metastasis, regardless of the side from which the co-NEC has originated.
Introduction
The incidence of colonic neuroendocrine neoplasms has been reported to be 0.2 cases per 100,000 population per year, 1 and most cases are aggressive neuroendocrine carcinomas, 2 which have an even worse prognosis than adenocarcinomas. 3 More than 50% of patients have metastatic disease at the time of diagnosis and a median survival duration of less than 1 year.4,5 Whether primary site resection can benefit patients with colonic neuroendocrine carcinoma (co-NEC) with distant metastases is still controversial.6,7
Recently, an increasing number of studies have reported differences in clinical, pathobiological, and molecular characteristics between left-sided and right-sided colon cancer, which contribute to the development of precise treatments for colon adenocarcinoma. 8 However, the differences in the clinical and pathological differences between left-sided and right-sided co-NECs have not been well described, and much of the available data have been generated by single-institution studies with small patient populations. 9
The aim of this study was to present the clinical characteristics of left-sided and right-sided co-NECs and further discuss the value of primary site resection in co-NEC patients with metastases using data from the Surveillance, Epidemiology, and End Results Program (SEER) database, which is an authoritative data source and allows us to draw a convincing conclusion. We report for the first time the significant clinical and survival differences between patients with left-sided and right-sided co-NECs with liver metastases and describe the survival benefits of primary resection in this patient population.
Materials and methods
Data collection and patient selection
The patients were pathologically diagnosed with co-NECs and selected from the 2010–2017 SEER database, 10 which includes all patients with cancer diagnosed in 18 geographic regions in America. We used the SEER*Stat 8.3.8 program to identify individuals in the SEER database as follows: ICD-O-3 codes 8013, 8150-8156, and 8246-8248 and site codes C18.0–C18.9. Cases of rectal NECs were excluded from this study because of the reported heterogeneity between co-NECs and rectal NECs. 11 We defined tumors proximal to the splenic flexure as right-sided tumors and tumors distal to the splenic flexure as left-sided tumors. 12 Information on the resection of metastases was obtained from ‘Rxsummsurgothregdis2003’. 10 Patients who did not undergo the resection of metastases were included in the survival analysis. The final follow-up of patients in the SEER database occurred in November 2019.
We excluded patients who met the following criteria: (1) patients whose survival data or follow-up data were incomplete; (2) patients diagnosed with more than one primary tumor; (3) patients who died due to non-neoplastic disease; and (4) patients with incomplete surgical information.
Statistical analysis
Coarsened exact matching (CEM) was performed to adjust for relevant factors before regression models were constructed. 13 The patients’ demographic data and tumor characteristics were summarized using descriptive statistics. Univariate analyses were performed using the χ2 test or Student’s t-test. Patients were separated into treatment groups, and survival in these groups was compared between patients with right-sided and left-sided co-NECs using multivariate analysis. All statistical analyses were performed using Intercooled Stata 12.0 (Stata Corporation, College Station, TX, USA). The results were considered statistically significant at a two-sided p < 0.05. The specific selection procedure is presented in Figure 1(a).
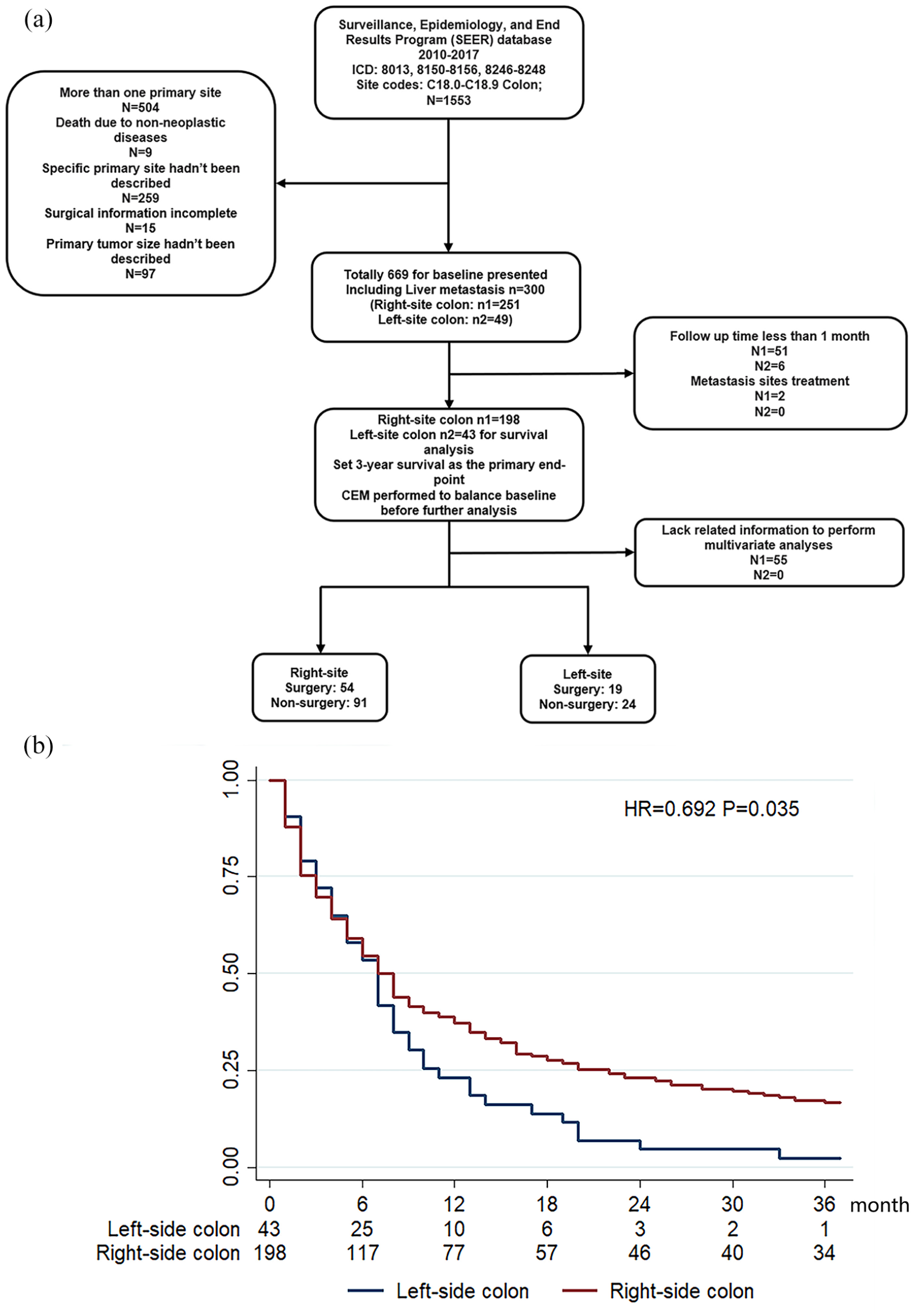
Flow chart of patient selection and survival differences between right-sided and left-sided co-NECs. (a) Flow chart of patient selection. (b) Survival differences between right-sided and left-sided co-NECs.
Results
Basic characteristics of co-NEC patients
In total, 669 pathologically diagnosed co-NEC patients with sufficient baseline data were identified from the SEER database (Table 1). A total of 80.72% of the co-NECs originated from the right side of the colon, and the mean overall survival (mOS) was similar between the two groups when all stages were considered (right versus left: 22.30 m versus 22.55 m). Patients with right-sided co-NECs had an older mean age at diagnosis than patients with left-sided co-NECs (right versus left: 64.05 years old versus 60.12 years old; p = 0.010). A higher proportion of the patients with right-sided co-NECs developed distant metastasis (right versus left: 45.74% versus 39.53%). In total, 44.84% of the co-NEC patients were diagnosed with liver metastasis, and the liver was the most common metastatic site, regardless of whether the co-NEC originated from the right or left side (right versus left: 46.68% versus 37.98%). The pattern of metastasis was similar between right-sided and left-sided co-NECs (p = 0.72, Table 1).
Demographic and clinical characteristics of all colon NEC patients.
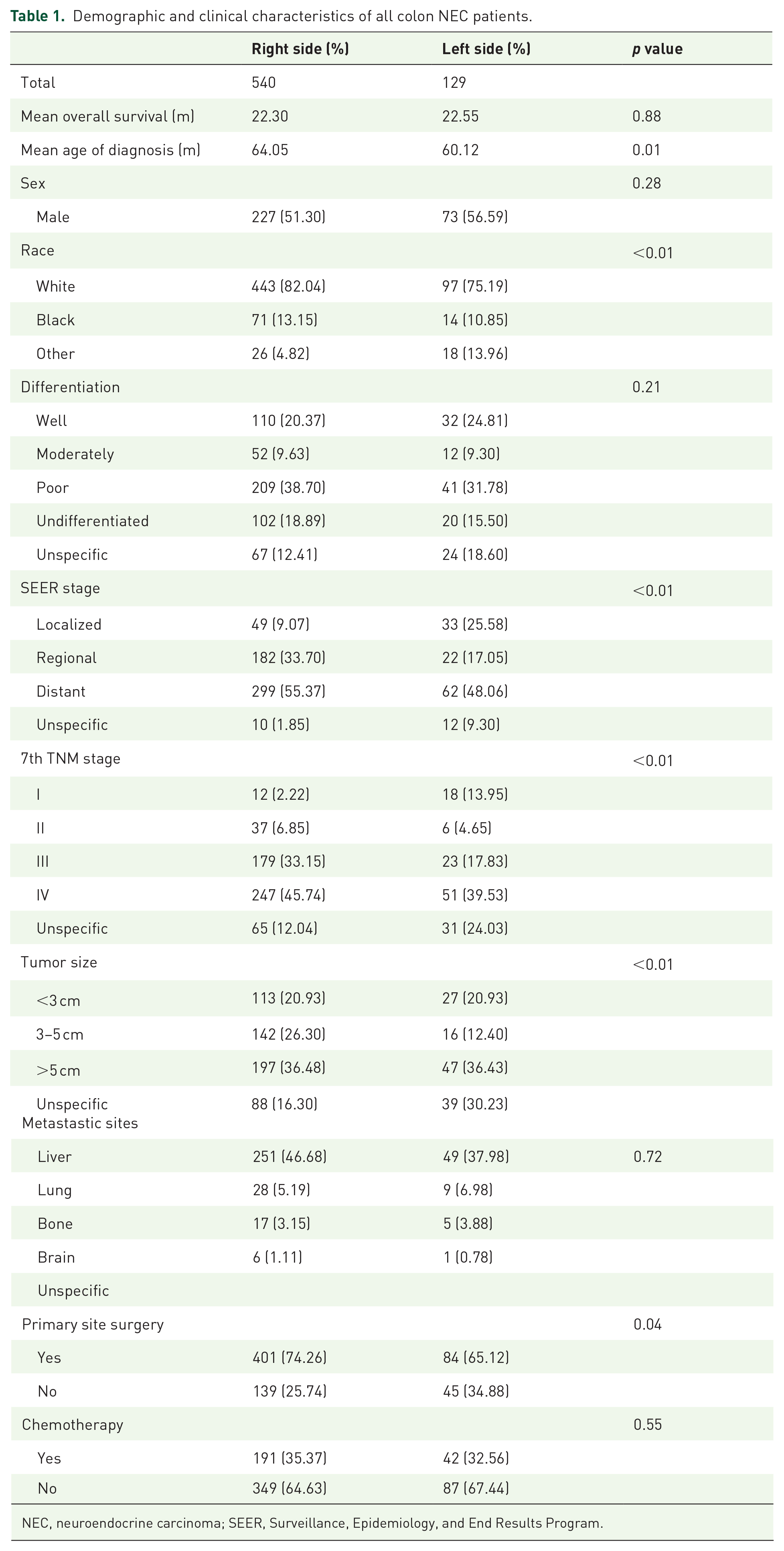
NEC, neuroendocrine carcinoma; SEER, Surveillance, Epidemiology, and End Results Program.
Survival differences in co-NEC patients with liver metastasis
From among the co-NEC patients with liver metastasis, we selected the patients who underwent primary site resection and performed a survival analysis stratified by primary site (right side of the colon versus left side of the colon). None of the co-NEC patients with liver metastasis underwent resection or other interventions of the metastases. The right-sided co-NEC patients had better survival than the left-sided co-NEC patients (mOS right versus left: 15.37 m versus 9.62 m; adjusted HR = 0.692, 95% confidence interval (CI): 0.492–0.975, p = 0.035) (Table 2, Figure 1(b)). The right-sided co-NEC patients still had an older mean age at diagnosis (right versus left: 60.59 years old versus 55.18 years old; p = 0.015). Most primary tumor sizes were larger than 3 cm (right versus left: 83.22% versus 89.28%, except unspecified tumor sizes). We observed that the proportions of patients who underwent surgical resection of the primary co-NEC differed based on the side (right versus left: 61.62% versus 44.19%, p = 0.04). To further investigate the potential factors affecting the survival of co-NEC patients with liver metastasis identify more favorable treatment strategies, we separated the patients with liver metastasis according to the location of the primary site and performed the following analysis.
Demographic and clinical characteristics of patients with liver metastasis.

Association of primary site resection with prolonged survival in co-NEC patients with liver metastasis
To evaluate whether primary site resection benefited co-NEC patients with liver metastasis, we performed multivariate analyses. We matched co-NEC patients with liver metastases who did and did not undergo primary site resection with CEM to balance the factors (Tables 3 and 4). None of the patients underwent resection or other interventions at the site of liver metastases. Among the right-sided co-NEC patients, before CEM, male patients (HR = 1.49, 95% CI: 1.09–2.06, p = 0.013) had a higher risk of mortality than female patients, and primary site resection benefited the patients (HR = 0.55, 95% CI: 0.37–0.82, p = 0.003). After CEM, primary site resection was still associated with prolonged survival (adjusted HR = 0.50, 95% CI: 0.33–0.77, p = 0.001). The baseline characteristics of left-side colon were balanced, enabling the multivariate analyses to be performed. The results suggested that primary surgery also benefited left-sided co-NEC patients (adjusted HR = 0.38, 95% CI: 0.16–0.89, p = 0.026) (Table 4, Figure 2).
Baseline of both side colon separating according to the primary site surgery.

CEM, coarsened exact matching.
Multivariate analyses of overall survival.

CEM, coarsened exact matching; CI, confidence interval; HR, hazard ratio.

Survival benefits of primary tumor resection right-sided and left-sided co-NECs. (a) Right-sided co-NEC survival. (b) Left-sided co-NEC survival.
Discussion
The high heterogeneity of neuroendocrine neoplasms, not only in terms of the primary site but also the metastatic pattern, has been widely recognized.14–16 Whether the distinct embryologic origins of the right and left colon contribute to the differences in characteristics and affect the choice of treatment for co-NECs needs more attention. In this study, we present for the first time an overview of the clinical differences between right-sided and left-sided co-NECs and discuss the difference in survival between patients with left-sided and right-sided co-NECs with liver metastasis. We found that in this patient population, patients with right-sided co-NECs had better survival than those with left-sided co-NECs, although the former were diagnosed at an older age. The survival of co-NEC patients is quite different from that of colon adenocarcinoma patients. Helvaci Kaan and colleagues recently reported the differences between right-sided and left-sided colon cancer in a 1725-patient cohort. The conclusion was that right-sided colon adenocarcinoma was more common, diagnosed at an older age, and was associated with worse survival than left-sided colon adenocarcinoma. 17 The older age and higher rate of diagnosis of right-side colon may be due to the lack of symptoms in the proximal colon, which is also common in NEC and adenocarcinoma, 18 while the differences in survival suggests that the pathological and molecular differences between the two sides play essential roles. 19 The choices of systematic treatment for metastatic colon adenocarcinoma were divided based on primary site in the large retrospective study CALGB/SWOG 80405. 20 A review of the clinical and survival differences in big data is urgently needed to inspire further pathological and molecular studies on co-NECs, which may differ substantially from adenocarcinoma and warrants further investigation.
Almost half of co-NECs develop distant metastasis, and the liver was the most common site observed in our study, which agrees with previous reports.15,21 The value of primary site and metastasis site resection in distant metastasis patients has not been confirmed or reached an agreement. The primary site resection of co-NECs with and without metastases is still controversial9,18 and the decision regarding resection is made on an individual basis. 22 The small sample sizes and use of data from single institutions are the main limitations preventing the conclusions of previous studies from being convincing.23,24 Recently, a study stated that patients from the National Cancer Database (NCDB) with high-grade neuroendocrine carcinomas of the colon and rectum who underwent chemotherapy and surgical resection of the primary tumor had better overall survival than those managed without resection. 4 This study had a larger sample size and recommended primary resection, although the substantial heterogeneity among right-sided colonic, left-sided colonic, and rectal primary sites was neglected. Our study included only co-NEC patients from the SEER database, 10 which is an authoritative data source and with a large population of patients from multiple institutions, to identify the clinical characteristics of and differences in left-sided and right-sided co-NECs. We focused on the most controversial aspect, namely, whether patients with metastatic disease benefit from primary site resection and a shift in the treatment pattern, by balancing demographics (including age, sex, race, and tumor size) with CEM to avoid potential bias. 25 Therefore, the finding that co-NEC patients with liver metastasis benefit from primary resection can be used as a foundation for more clinical research in the future. The management of liver metastasis is a hotspot in colon cancer research, and successful management has been reported to prolong the survival and improve the quality of life of colon adenocarcinoma patients.26,27 The indications for liver metastasis site resection and interventional therapy need to be carefully evaluated in colon adenocarcinoma. 28 Recently, some reports suggested that liver metastasis site resection could also benefit co-NEC patients.29–31 More attempts to improve co-NEC patient survival and quality of life were encouraged. Unfortunately, no patients underwent liver metastasis site resection or other interventions in our study, and whether patients with right-sided and left-sided co-NECs gain equal benefits from the management of liver metastasis is worth considering in future research. Before we performed CEM adjusting factors to indicate the benefits of primary surgery, we found that male patients with right-sided NECs had higher risk of death than female patients (HR = 1.49, 95% CI: 1.09–2.06, p = 0.013). Sex has been reported as the independent risk factor in many kinds of cancer due to the life style, level of hormone, and so on. 32 Also, some studies reported male sex could be a risk factor in colorectal neuroendocrine tumors (NETs) and NECs.33,34 But whether the sex could be an independent risk factor in NECs or specific sub-types of NECs is still unclear and worth to be further investigated.
There are still some limitations that need to be considered when interpreting our results. This study was a retrospective review, and the SEER database does not have details of the surgeries (e.g. acute operations/ruptured tumors, microvascular invasion, and lymphatic vessel invasion) that could affect the therapeutic effect and patient prognosis. In addition, the details of the systemic chemotherapy administered to patients were unclear, so we could not further investigate the specific benefits of chemotherapy.
Based on the above, we advocate for the performance of a study to investigate the differences in molecular characteristics and therapeutic responses between left-sided and right-sided co-NECs and additional prospective studies to identify better treatment strategies, especially with regard to the surgical resection of the primary site.
Conclusions
Co-NECs frequently originate from the right side and commonly develop liver metastasis. Right-sided co-NECs with liver metastases are associated with better survival than left-sided co-NECs. Primary site resection in co-NEC patients with liver metastasis is associated with better survival, although additional clinical research is needed. We advocate for the performance of more studies focusing on the differences in molecular characteristics and therapeutic responses between left-sided and right-sided co-NECs.
Footnotes
Acknowledgements
Wen Cai, Weiting Ge and Jiawei Zhang contributed equally to this work.
Author contributions
WC and WG acquired data. WC, WG, and JZ prepared figures, and drafted and revised the manuscript. HH and JM designed and supervised the study. All authors uphold the integrity of the work, approved the manuscript in its entirety, and are accountable for all aspects of the work.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (32070630 & 81372348), the National Natural Science Foundation of Zhejiang Province (LQ19H160024), the Scientific Research Fund of Zhejiang Provincial Education Department of China (Y202045589), and National Key R&D Program of China (2016YFC1302803).
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
The code used are available from the corresponding author on reasonable request.