
Abstract
Background and Aims:
Single-operator cholangioscopy-assisted electrohydraulic lithotripsy (SOC-EHL) is effective and safe in difficult choledocholithiasis. The optimal timing of SOC-EHL use, however, in refractory stones has not been elucidated. The following aims to determine the most cost-effective timing of SOC-EHL introduction in the management of choledocholithiasis.
Methods:
A cost-effectiveness model was developed assessing three strategies with a progressively delayed introduction of SOC-EHL. Probability estimates of patient pathways were obtained from a systematic review. The unit of effectiveness is complete ductal clearance without need for surgery. Cost is expressed in 2018 US dollars and stem from outpatient US databases.
Results:
The three strategies achieved comparable ductal clearance rates ranging from 97.3% to 99.7%. The least expensive strategy is to perform SOC-EHL during the first endoscopic retrograde cholangiography pancreatography (ERCP) (SOC-1: 18,506$). The strategy of postponing the use of SOC-EHL to the third ERCP (SOC-3) is more expensive (US$18,895) but is 2% more effective. (0.9967). SOC-EHL during the second ERCP in the model (SOC-2) is the least cost-effective. Sensitivity analyses show altered conclusions according to the cost of SOC-EHL, effectiveness of conventional ERCP, and altered willingness-to-pay (WTP) thresholds with early SOC-1 being the most optimal approach below a WTP cut-off of US$20,295.
Conclusions:
Early utilization of SOC-EHL (SOC-1) in difficult choledocholithiasis may be the least costly strategy with an effectiveness approximating those achieved with a delayed approach where one or more conventional ERCP(s) are reattempted prior to SOC-EHL introduction.
Keywords
Introduction
Endoscopic retrograde cholangiography pancreatography (ERCP) is the standard of care in the management of choledocholithiasis. Different techniques have been developed including balloon sphincteroplasty, mechanical lithotripsy, and stent insertion for stone dissolution. 1 Overall, ductal clearance rates with traditional ERCP range from 87% to 100%.2–5 Difficult bile duct stones, however, often require multiple ERCP sessions, increasing the risk for procedure-related adverse events, patient inconvenience, and cost. Single-operator cholangioscopy with electrohydraulic lithotripsy (SOC-EHL) has recently gained widespread adoption in the management of difficult stones with the advent of improved cholangioscopy technology and high clinical success. 6 Several expert societies have advocated for the use of SOC-EHL with failure of conventional ERCP.7,8 In addition, compared with mechanical lithotripsy, SOC-EHL appears to be cost-effective. 9
Nevertheless, due to the high up-front cost of SOC-EHL, most institutions have adopted a step-up approach to difficult stones starting with traditional ERCP and only proceeding to SOC-EHL following multiple failed ERCP. This strategy is largely based on data supporting the role of plastic stent insertion and stone dissolution with high rates of ductal clearance on repeat ERCPs. 10 The optimal timing of SOC-EHL introduction in the management algorithm remains unclear. A delayed approach allows for the possibility of clearing the stones without the need for SOC-EHL. This option, however, is likely associated with more procedures and patient inconvenience, with the potential for higher cumulative rates of adverse events and its associated costs. Early introduction of SOC-EHL, on the other hand, may be accompanied with fewer procedures and greater patient satisfaction, but its adoption is often limited due to the greater up-front costs. We thus aimed to determine the most cost-effective timing of SOC-EHL utilization in the endoscopic management of difficult common bile duct stones.
Methods
Model design
A decision tree was used to model the clinical successes and failures of three different strategies in managing patients with difficult biliary stones with ERCP and SOC-EHL. This type of analysis was chosen to ascertain simultaneously the effectiveness and costs of competing strategies. Difficult biliary stones are defined as choledocholithiasis with failure of complete ductal clearance using conventional ERCP methods including sphincterotomy with balloon or basket stone extraction with or without sphincteroplasty and mechanical lithotripsy. As such, every patient included in the model is presumed to have failed ductal clearance with an initial, elective ERCP. The numbering of ERCPs in our decision tree, therefore, does not include this initial failed procedure. The model thus outlines three possible strategies of EHL-SOC (SOC-1, SOC-2, SOC-3). The first strategy (SOC-1) introduces SOC-EHL immediately at the first ERCP. The second option (SOC-2) introduces SOC-EHL at the second ERCP for incomplete ductal clearance. The final option (SOC-3) introduces SOC-EHL during the third ERCP for persistent choledocholithiasis. A plastic biliary stent is presumed to be inserted with each failed procedure. For all three strategies, if ductal clearance is not achieved following SOC-EHL, a second SOC-EHL session is subsequently carried out. Surgery is considered as a final option if ductal clearance is not achieved after two ERCP with SOC-EHL. Patients are followed for adverse events following each endoscopic session over a 6-month time horizon. Death is not considered in the model due to the extremely low rates of mortality attributable to choledocholithiasis without cholangitis. The software TreeAge Suite 2018 (Williamstown, MA, USA) 11 was used for construction of the model (Figure 1) and for the cost-effectiveness analysis.

Structure of the model.
Probability and cost assumptions
Probabilities for failure and complications at each step were obtained from a systematic review of literature from January 1980 to December 2018 using MEDLINE, EMBASE, and ISI Web of knowledge. The selection of articles utilized a highly sensitive search strategy to identify citations with a combination of MeSH headings adapted to each database and text words related to (1) cholangioscopy or lithotripsy, (2) Spyglass®, electrohydraulic lithotripsy. Recursive searches and cross-referencing were also carried out using a “similar articles” function; furthermore, hand searches of articles were also performed. All fully reported published studies were included. For costs, a third-party perspective was adopted including only direct costs. Our model was designed to be representative of the national costs in the American health care system. Physician fees were provided by the Centers for Medicare and Medicaid services. 12 These fees are national averages according to types of visits and medical specialties in the United States. Equipment costs for SOC-EHL were provided by the Endoscopy purchasing department of a US hospital 13 for Spyglass® (Boston Scientific Inc., Marlborough, MA, USA 14 ). Costs for the cholangioscopy and lithotripsy generators were amortized over their anticipated lifespan and determined as an individual cost per use (which is added to the single use of the rest of the equipment). The lifespan of both the cholangioscopy and lithotripsy generators were estimated to be 5 years, as per the manufacturer, with an estimated 50 cases/year. The cost of the generator per use was therefore calculated by dividing the total cost of the generator by 250 cases (50 cases/year × 5 years). Stent prices and facility fees for ERCP were obtained from Boston Scientific Inc. (Marlborough, MA, USA). 14 The cost of surgery and adverse events with their respective hospitalization costs and lengths of stay were computed using weighted national data from the American National Inpatient Sample (NIS) 15 which gathers more than 7 million discharges collected from almost 5,000 hospitals in 47 American states. The NIS has been extensively used in previous cost-effectiveness analyses16–19 and its weighted methodology ensures that it is representative of the national health care costs from all types of insurances in the United States. The cost of surgery was based on the adult inpatient records registered under ICD-10 codes: K80.42 calculus of bile duct with acute cholecystitis without obstruction, K80.44 calculus of bile duct with chronic cholecystitis without obstruction, and K80.50 calculus of bile duct without cholangitis or cholecystitis without obstruction. Adverse event costs were ascertained from adult hospitalizations recorded in the NIS that included K83.0 cholangitis, K92.2 gastrointestinal hemorrhage, unspecified, and K85.9 acute pancreatitis, unspecified. The weights associated with each of these three codes varied according to the probability estimates obtained from the literature review.
The US consumer price index for medical care services from the Bureau of Labor Statistics 20 was used, when necessary, to express all costs in 2018 US$.
Cost-effectiveness analysis
The unit of effectiveness was defined as complete ductal clearance without the need for surgery over the 6-month time horizon. The total cumulative representative costs were computed for each path in the tree, thus each terminal node computes the average individual total cost per patient treated at the end of the 6-month time horizon. Results are reported as cost, effectiveness, cost-effectiveness ratio, net monetary benefit, and incremental cost-effectiveness ratios. The willingness-to-pay (WTP) was fixed a priori at US$50,00016–18,21 with a posteriori sensitivity analysis to assess how varying this threshold altered the results.
Sensitivity analysis
Deterministic sensitivity analysis was performed on all 50 variables of the model. The value of each parameter was varied inside its respective prefixed ranges, whereas other input variables remained unchanged. Probabilistic sensitivity analysis explored further but simultaneously the impact of variability across all model parameters. One hundred thousand simulations generated by the model using different values of variables were run as part of the Monte-Carlo analysis and are summarized with a cost-effectiveness acceptability curve and scatterplot graph. The reporting of our results is in accordance with the standards put forth in the Consolidated Health Economic Evaluation Reporting Standards Statements. 22 Ethics approval or consent was not required given the use of prior public cost data with no patient identifiers.
Results
The systematic review yielded 1870 articles (PRISMA diagram, Figure 2). After abstract screening, 59 articles were included that addressed the management of patients with difficult bile duct stones having failed prior ERCP. A total of 24 articles were used in the analysis with data abstracted from their full text.10,23–45

PRISMA flow diagram.
Tables 1 and 2 list the cost and probability input variables entered in the model, with their respective ranges. Cost variables are associated with β-distributions and probabilities with γ-distributions. All three strategies cost approximately US$20,000 per treatment (Table 3). The three strategies achieved clinically comparable effectiveness rates ranging from 97.3% to 99.7%. The least expensive strategy is to perform SOC-EHL during the first ERCP (SOC-1: 18,506$). The strategy of postponing the use of SOC-EHL at the third ERCP (SOC-3) is more expensive (US$18,895) but presents the highest measure of effectiveness (0.9967) among the three options. The strategy of introducing SOC-EHL during the second ERCP in the model (SOC-2) was the most costly and was economically dominated by SOC-3.
Length of stay and cost data used in the model.

All costs are expressed in 2018US$. Length of stay is in days.
ERCP, endoscopic retrograde cholangio-pancreatography; SOC-EHL, single-operator cholangioscopy-assisted electrohydraulic lithotripsy.
Probabilities used in the model.

All costs are expressed in 2018US$.
ERCP, endoscopic retrograde cholangio-pancreatography; SOC-EHL, single-operator cholangioscopy-assisted electrohydraulic lithotripsy.
CEA report.
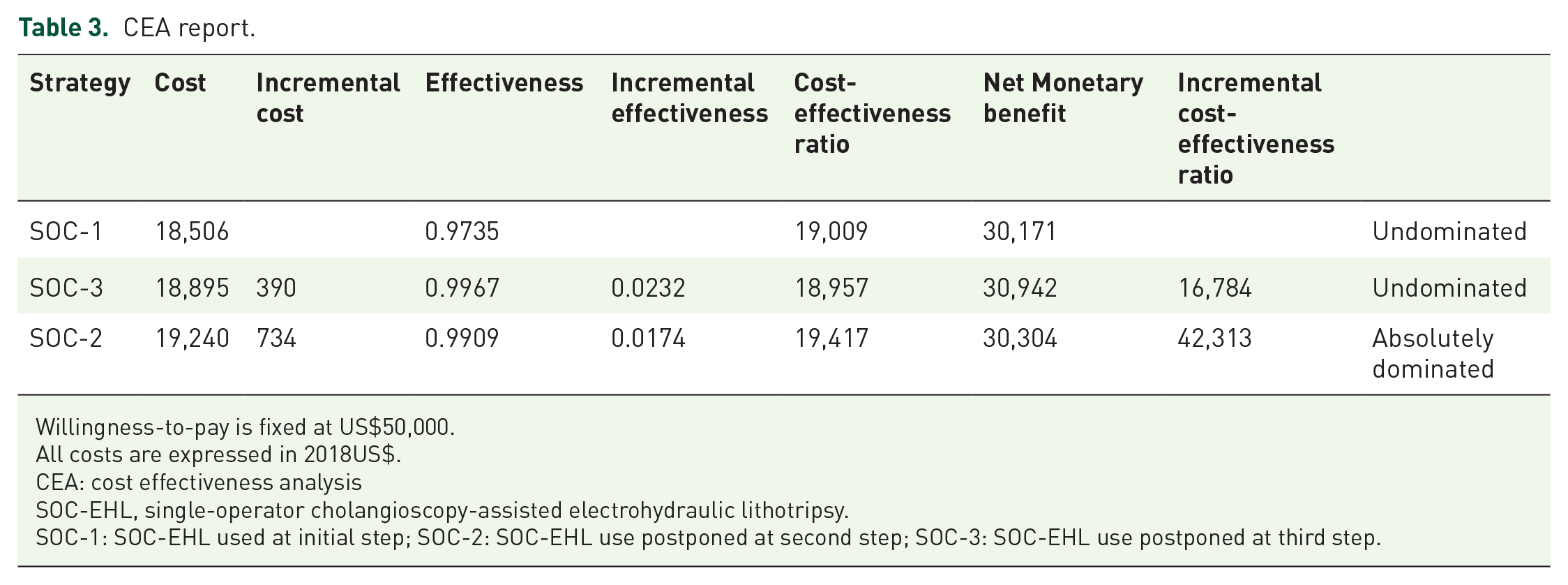
Willingness-to-pay is fixed at US$50,000.
All costs are expressed in 2018US$.
CEA: cost effectiveness analysis
SOC-EHL, single-operator cholangioscopy-assisted electrohydraulic lithotripsy.
SOC-1: SOC-EHL used at initial step; SOC-2: SOC-EHL use postponed at second step; SOC-3: SOC-EHL use postponed at third step.
The deterministic sensitivity analysis is shown in Figure 3 and Table 4 and demonstrates that if the cost of SOC-EHL decreases below US$1,732, SOC-1 becomes optimal (the most acceptable strategy with a fixed WTP of US$50,000). The cost-effectiveness acceptability curve generated by the probabilistic sensitivity analysis (Figure 4) shows that SOC-2 is always dominated by SOC-3. The strategy or choice when comparing SOC-1 with SOC-3 varies depending on the threshold value adopted for the WTP. SOC-3 is chosen in 65% of these simulations (inside plausible scenarios) versus 35% for SOC-1 at the base-case analysis WTP value of US$50,000. The scatterplot comparing SOC-1 with SOC-3 shows the dispersion of the Monte-Carlo simulations of SOC-1 cases compared with SOC-3 (Figure 5 included in appendix). When the WTP threshold drops below US$20,295, SOC-1 becomes the approach most often chosen.

Tornado diagram: incremental cost-effectiveness ratio (SOC-1 versus SOC-3).
Relevant values highlighted by the one-way sensitivity analysis.

SOC-1 is both less effective and less expensive but with an ICER below the willingness-to-pay (whereas SOC-3 exceeds the willingness-to-pay).
ERCP, endoscopic retrograde cholangio-pancreatography; SOC-EHL, single-operator cholangioscopy-assisted electrohydraulic lithotripsy (Spyglass®, Boston Scientific Inc., Marlborough, MA, USA). 15
Willingness-to-pay is fixed at US$50,000.
SOC-1: SOC-EHL used at initial step; SOC-2: SOC-EHL use postponed at second step; SOC-3: SOC-EHL use postponed at third step.
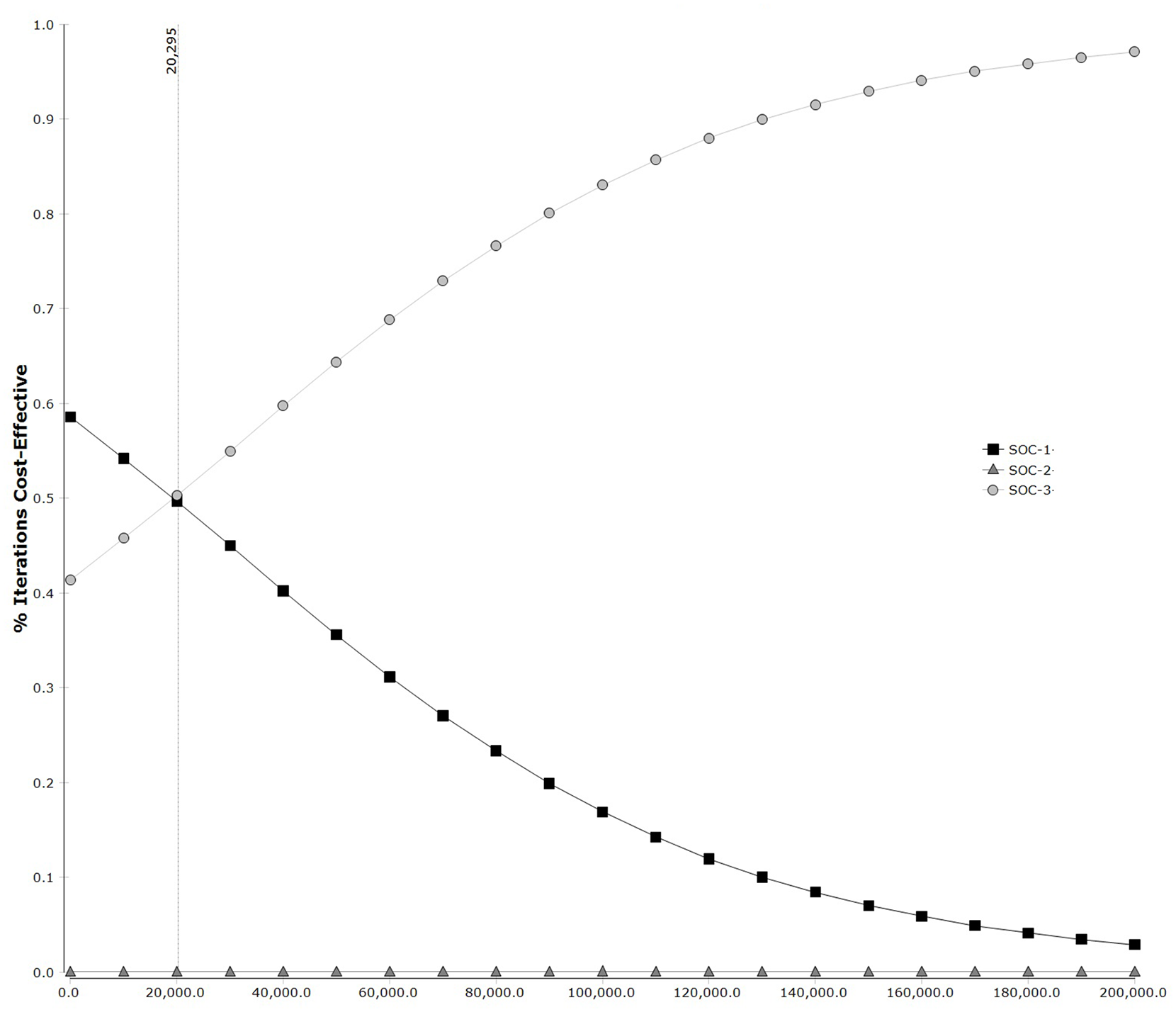
Cost-effectiveness acceptability curve.
Discussion
SOC-EHL is a major advancement in the technique of ERCP. Its ease of use and well-established effectiveness have made it a popular modality in the management of patients with difficult bile duct stones. 7 Although shown to be cost-effective and advocated by expert societies in the management of difficult stones, most centers will defer the use of SOC-EHL until at least one or two failures with conventional ERCP given the high up-front cost of SOC-EHL, extensive experience with mechanical lithotripsy, and high ductal clearance rates with repeated ERCP following stent-induced stone dissolution. Using the Belgium health care model, Deprez et al. 9 have recently demonstrated that SOC-EHL is cost-effective when compared with traditional ERCP with mechanical lithotripsy. The optimal timing of SOC-EHL introduction in the algorithm of endoscopic difficult stone management, however, has not been elucidated, and guidelines remain equivocal or silent in addressing this important aspect.7,46 To our knowledge, the current analysis is the first to specifically study the timing of SOC-EHL in the endoscopic management of difficult stones based on considerations of cost-effectiveness. Our results show that early use of SOC-EHL (SOC-1) is the least expensive strategy with an ICER of US$16,784 (i.e. per additional successfully treated patient) while delaying SOC-EHL to the third procedure after two failed ERCP (SOC-3) is the most effective. Interestingly, delaying SOC-EHL to the second ERCP (SOC-2 approach) was dominated, making it the least cost-effective strategy as it is comparatively not cheap enough for the additional effectiveness it achieves when compared with SOC-3.
When comparing SOC-1 with SOC-3, there is no clear-cut dominant strategy. SOC-1 is less costly while SOC-3 is 2% more effective. This small difference in effectiveness is explained by two more attempts at stone extraction prior to SOC-EHL. As clinicians, it is important to realize that the 2% increase in success rate does not account for a patient’s quality of life, which was not measured in our model due to a paucity of data on the topic and the short time horizon of the medical condition, as has been discussed previously. 42 Causes of altered quality of life can include recurrent visits for invasive instrumentation and persistence of an obstructive stone with its associated complications, such as cholangitis. Had QALYs been used as unit of effectiveness, this would likely have increased the cost-effectiveness of SOC-1 due to the need for fewer re-interventions.
Nevertheless, the most cost-effective strategy in our analysis between SOC-1 and SOC-3 largely depends on the cost of the SOC-EHL equipment and WTP threshold adopted by a decision taker. Although the cost of cholangioscopy in our base-case analysis was set at 2,450$, which is representative of the current US market, dropping SOC-EHL costs below US$1,732 make SOC-1 the optimal strategy for the pre-set WTP of US$50,000. In terms of WTP, although there is no single accepted WTP threshold,47–49 a US$50,000 cut-off was used in our base-case analysis similarly to prior endoscopic cost-effectiveness studies addressing acute disease processes.16–18,21 In probabilistic sensitivity analysis, a lower WTP threshold of US$20,000 favors the SOC-1 approach, whereas greater thresholds favor the increased effectiveness yet at an increased cost attributable to the repeated attempts strategy (SOC-3). Overall, it appears that early SOC-1 is the preferred strategy in clinical practice, given that it is the least costly while being associated with the fewest procedures with a minimal decrease in effectiveness when compared with delaying SOC-EHL to the third ERCP (SOC-3). Our results will hopefully assist budget managers and clinicians in adopting a cost-effective approach to this clinical problem, keeping in mind current cost restraints in the dispensation of medical care.
One limitation of our study is the lack of controlled data, putting the model assumptions at risk for overestimation of clinical success and under-reporting of associated complications among included studies. Extensive sensitivity analyses were performed in an effort to minimize the effects of these shortcomings. As aforementioned, quality of life data were not used for our analysis due to a lack of data on the topic. Additionally, we did not consider laser lithotripsy of bile duct stones, because of its rarer adoption in North American endoscopy units. However, the extensive variations of costs of SOC-EHL equipment in our sensitivity analysis likely account for the effectiveness and cost ranges of laser lithotripsy.
In conclusion, this cost-effective analysis shows that early introduction of SOC-EHL is the least expensive strategy with a surgery-free stone clearance that clinically approximates its later introduction following repeated conventional ERCP attempts. Sensitivity analyses characterized the variability of our conclusions based on alterations in cost and probability assumptions. Decision makers will need to individualize their choices based on local resources and expertise. Data from high-quality prospective randomized trials are ideally needed to confirm these findings.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848211031388 – Supplemental material for Early cholangioscopy-assisted electrohydraulic lithotripsy in difficult biliary stones is cost-effective
Supplemental material, sj-pdf-1-tag-10.1177_17562848211031388 for Early cholangioscopy-assisted electrohydraulic lithotripsy in difficult biliary stones is cost-effective by Saad Alrajhi, Alan Barkun, Viviane Adam, Kashi Callichurn, Myriam Martel, Olaya Brewer, Mouen A. Khashab, Nauzer Forbes, Majid A. Almadi and Yen-I Chen in Therapeutic Advances in Gastroenterology
Footnotes
Conflict of interest statement
Alan Barkun is a consultant for Pendopharm Inc., Boston Scientific Inc., Olympus Inc., Cook Inc., and ATGen Inc.
Mouen Khashab is a consultant for Boston Scientific, Olympus, and Medtronic.
Nauzer Forbes is a consultant for Boston Scientific and has received speaking fees and research funding from Pentax.
Yen-I Chen is a consultant for Boston Scientific.
No disclosures for the remaining authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.