
Abstract
Background:
Benzodiazepines (BZDs) and analgesics are widely used for conscious sedation during endoscopic ultrasound (EUS) or endoscopic retrograde cholangiopancreatography (ERCP). However, endoscopic procedures are sometimes discontinued because of BZD-induced disinhibitory reactions such as excessive movement. We evaluated the usefulness of dexmedetomidine (DEX) for BZD-induced disinhibition in ERCP.
Methods:
Between February 2018 and August 2019, 22 patients who underwent EUS or ERCP were enrolled. All patients showed BZD-induced excessive movement at the first examination (BZD group) and received DEX at the second examination (DEX group). The initial DEX dose was 6 μg/kg/h for a 10-min loading, followed by 0.4 μg/kg/h during the procedure. BZDs and analgesics were administered before scope insertion. An additional sedative was administered to achieve a Ramsay sedation scale (RSS) of 4–5. Sedative effect, procedure completion rate, and changes in circulatory and respiratory dynamics were evaluated.
Results:
Mean RSS scores were significantly higher (p < 0.001) in the DEX (5.1 ± 0.5) compared with the BZD (4.0 ± 0.5) group. The movement score (p < 0.001) and number of additional sedatives required (p < 0.01) were lower in the DEX group. The procedure completion rate was significantly higher in the DEX (95.5%) compared with the BZD group (63.6%; p < 0.05). Significant differences in the frequency of hypotension (p = 1.00), bradycardia (p = 0.22), and respiratory depression (p = 0.68) were not noted between groups.
Conclusions:
The addition of DEX to BZD therapy yielded better sedative efficacy, lower excessive movement, a reduction in BZDs used, and a higher procedure complete rate. DEX may be used as an alternative method for BZD-induced inhibition during ERCP.
Keywords
Introduction
Gastrointestinal endoscopy alone is uncomfortable and sometimes painful for many patients. Endoscopy under conscious sedation not only reduces pain, but may also be associated with the completion of the procedure as well as improved treatment results.1,2 In particular, the scopes used for endoscopic ultrasound (EUS) or endoscopic retrograde cholangiopancreatography (ERCP) are thicker, and require deeper sedation than for gastrointestinal endoscopy.3,4 In addition, since ERCP includes drainage, stent placement, and stone extraction, meaning it is more invasive than other endoscopic procedures, the burden on patients is quite heavy. Deeper sedation and fewer body movements are necessary in order for patients to undergo stable treatment. However, increasing the amount of sedatives can cause airway obstruction, as well as respiratory and circulatory depression associated with deep sedation. 2
Therefore, benzodiazepines (BZDs; e.g. diazepam, midazolam) and analgesics are often used for conscious sedation during EUS or ERCP. 5 Combination therapy with analgesics is known to synergize sedative effects, and allows a reduction in the amount of sedative used and frequency of adverse events. 5 However, BZDs sometimes cause paradoxical reactions such as disinhibition (e.g. excessive movement), 6 making it difficult to continue the endoscopic procedure. Yet reports that review the incidence of BZD-induced disinhibition during endoscopic procedures and their frequency are lacking.
Dexmedetomidine (DEX) is a short-acting selective alpha-2 adrenoceptor agonist, with both sedative and analgesic effects, used for conscious sedation in intensive care units and treatment under local anesthesia.7,8 Since DEX can also be used in nonintubation procedures, it is reported to be useful for endoscopic procedures.9,10 Recent studies have shown the efficacy of DEX in comparison with midazolam during ERCP.11–13 Because the administration method is somewhat complicated, DEX is not used for all cases during EUS or ERCP, and it is currently undecided what kind of case it should be used for. In addition, reports on the effect of DEX on patients with BZD-induced disinhibition are unknown.
The study aimed to evaluate the usefulness of DEX combined with BZDs in patients who had difficulty in continuing ERCP due to BZD-induced disinhibition during the procedure.
Patients and methods
Study population
The analysis included patients who underwent EUS or ERCP at Sapporo Medical University Hospital between February 2018 and August 2019. Patients who showed excessive movement due to disinhibition induced by BZDs at the first examination (EUS or ERCP) were included in the BZD group. Of these patients, those who received a combination of DEX and BZDs at the second examination (ERCP in all cases) were included in the DEX group. Written informed consent was obtained from all patients before ERCP. This was a retrospective, single-center study that conformed to the ethics standards of the Declaration of Helsinki and was approved by the Institutional Review Board of Sapporo Medical University (approval No. 312-1092).
System and monitoring
At our institution, conscious sedation was administered by a single sedation physician (nonanesthesiologist) in addition to the investigator. Patient characteristics, including age, sex, height, and body weight, were measured before ERCP. Oxygen was administered (2 l/min) using a nasal cannula before the administration of sedation. Blood pressure, heart rate, and percutaneous arterial oxygen saturation (SpO2) were measured by monitor before the administration of sedation and monitored every 5 min during the procedure.
DEX group
The initial dose of DEX (Precedex Syringe; Maruishi Pharmaceutical Co., Ltd, Osaka, Japan) was 6 μg/kg/h for a 10-min loading, followed by 0.4 μg/kg/h continued by intravenous administration during the procedure. Blood pressure, heart rate, and SpO2 were measured very 2 min during loading. After 10 min, this was switched to monitoring every 5 min. Diazepam (5–10 mg; Maruishi Pharmaceutical Co., Ltd, Osaka, Japan) and 35 mg meperidine (Takeda Pharmaceutical Co., Ltd, Osaka, Japan) were intravenously injected before insertion of the scope. When conscious sedation was shallow, an additional dose of 5 mg diazepam was intravenously administered to achieve a Ramsay sedation scale 14 (RSS) of 4–5. Meperidine (35 mg) was intravenously administered when analgesia was insufficient.
BZD group
Diazepam (5–10 mg; Maruishi Pharmaceutical Co., Ltd) or 2.5–5 mg midazolam (Maruishi Pharmaceutical Co., Ltd) as a sedative, and 35 mg meperidine (Takeda Pharmaceutical Co., Ltd) were intravenously injected before insertion of the scope. When conscious sedation was shallow, an additional dose of 5 mg diazepam or 2.5 mg midazolam was intravenously administered to achieve an RSS of 4–5. Meperidine (35 mg) was intravenously administered when analgesia was insufficient.
Variables
The primary outcome was a sedation level according to RSS. Secondary outcomes were movement score, completion rate of the procedure, the number of additional sedatives, and adverse events. Movement scores 15 were defined as shown in Table 1. Blood pressure, heart rate, and SpO2 were measured continuously during sedation; presedation and minimum values were assessed. Adverse events were as follows: hypotension with a systolic blood pressure <90 mmHg, bradycardia with a heart rate <50 beats per min (bpm), and respiratory depression with SpO2 <90%.
Movement scores.

Statistical analysis
The Wilcoxon signed-rank test was used for continuous variables. A chi-square test, Fisher’s exact test or McNemar’s test was used to compare categorical variables. An analysis of changes in blood pressure, heart rate, and SpO2 was performed using Friedman’s test. A two-sided p value of <0.05 was considered statistically significant. All statistical analyses were performed using EZR software (Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Results
Patient characteristics
From February 2018 to August 2019, a total of 373 patients underwent EUS or ERCP; 22 (5.9%) of these who had BZD-induced disinhibition were included in this study. The median age was 71 years (range 21–86 years), with 17 males and 5 females. Eight patients were alcoholics, and two patients regularly used sleeping pills. At a prior examination, ERCP was performed on 16 patients and EUS on 6 patients. All patients underwent ERCP at a second examination. Patient characteristics are shown in Table 2.
Patient characteristics.
Data are expressed as median (range) or N (%); BMI, body mass index; ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound.
Procedure characteristics
Statistically significant differences (p = 0.58) in the procedure time between DEX and BZD groups (mean [±SD] 51 ± 29 versus 47 ± 22) were not noted. Procedure details for the DEX group were as follows: biliary drainage in 15 patients, intraductal ultrasonography (IDUS) in 3 patients, fluoroscopic biopsy in 10 patients, stone extraction in 3 patients, and peroral cholangioscopy (POCS) in 10 patients. Procedure details for the BZD group were: biliary drainage in 13 patients, IDUS in 5 patients, fluoroscopic biopsy in 4 patients, and EUS in 6 patients. The rates of fluoroscopic biopsies (p = 0.04) and POCS (p < 0.001) performed were significantly greater in the DEX group compared with the BZD group (Table 3). Both Fluoroscopic biopsies and POCS were difficult to perform due to BZDs-induced disinhibition in the BZD group. Six patients in the BZD group were attempted to perform POCS, but they were unable to do it. The completion rate for procedures was significantly higher in the DEX group (95.5%) compared with the BZD group (63.6%; p < 0.05; Figure 1). The endoscopy procedure was discontinued for eight patients (36.4%) of the BZD group due to excessive movement. Procedure characteristics are shown in Table 3.
Comparison of procedures between the two groups.

BZD, benzodiazepine; DEX, dexmedetomidine; EUS, endoscopic ultrasonography; IDUS, intraductal ultrasonography; POCS, peroral cholangioscopy.
Data are expressed as mean (SD) or N.
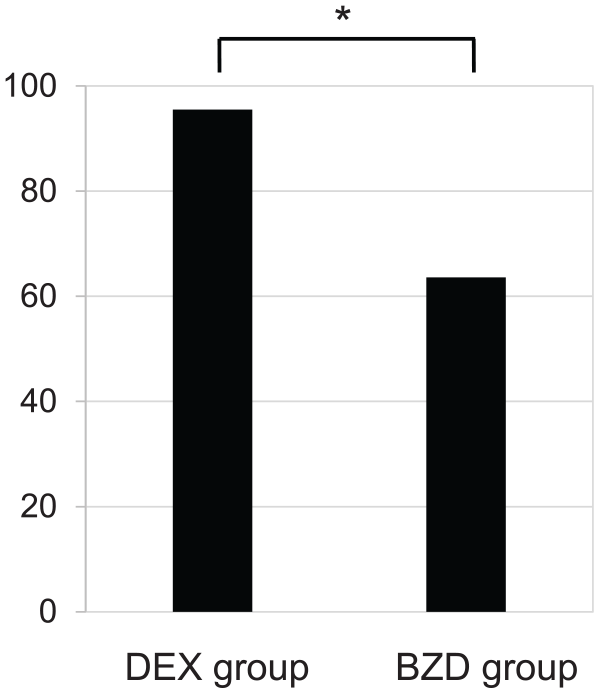
Comparison of the two groups for completion rates of procedures.
Evaluation of sedation
The RSS score for the DEX group was significantly higher compared with that of the BZD group during the procedure [mean (±SD) 5.1 ± 0.5 versus 4.0 ± 0.5, p < 0.001; Figure 2a]. The maximum movement score for the DEX group was significantly lower than that of the BZD group [mean (±SD) 1.7 ± 0.8 versus 3.2 ± 0.7, p < 0.001; Figure 2b]. The number of additional sedatives taken was also significantly lower in the DEX group [mean (±SD) 2.6 ± 2.1 versus 5.3 ± 2.4, p < 0.01; Figure 2c]. In the BZD group, diazepam was administered to 18 patients, midazolam was administered to 4 patients. Significant differences in the RSS score [mean (±SD) 4.1 ± 0.5 versus 3.8 ± 0.4, p = 0.19], the maximum movement score [mean (±SD) 3.2 ± 0.7 versus 3.3 ± 0.8, p = 0.84], the number of additional sedatives [mean (±SD) 5.4 ± 2.6 versus 4.8 ± 1.5, p = 0.65] and the completion rate for procedures (66.7% versus 50% p = 0.60) between diazepam and midazolam were not observed in the BZD group.

Comparison of Ramsay sedation scale (a), movement score (b), and additional sedative (c) between the two groups.
Adverse events
The mean lowest systolic blood pressure was 103 mmHg in the DEX group, and 101 mmHg in the BZD group. The systolic blood pressure after sedation was significantly decreased in both groups (p < 0.001 for the DEX group, p < 0.001 for the BZD group; Figure 3a). The mean lowest heart rate was 56 beats/min in the DEX group, and 73 beats/min in the BZD group. The heart rate was significantly decreased in both groups (p < 0.05 in the DEX group, p < 0.01 in the BZD group; Figure 3b). The mean lowest SpO2 was 96% in the DEX group, and 93% in the BZD group. SpO2 was significantly decreased in both groups (p < 0.001 in the DEX group, p < 0.001 in the BZD group; Figure 3c). Significant differences in the frequency of hypotension (p = 1.00), bradycardia (p = 0.22), and respiratory depression (p = 0.68) between the two groups were not observed (Table 4). In the DEX group, one patient had severe hypotension (systolic blood pressure <60 mmHg), and subsequently discontinued DEX treatment. In the BZD group, one patient had hypotension and bradycardia (heart rate <30bpm), and was administered flumazenil, catecholamine, and atropine.

Comparison of systolic blood pressure (a), heart rate (b), and SpO2 (c) after sedation in both groups.
Adverse circulatory and respiratory events.

bpm, beats per min; BZD, benzodiazepine; DEX, dexmedetomidine; SpO2, percutaneous arterial oxygen saturation.
Hypotension: systolic blood pressure <80 mmHg, Bradycardia: heart rate <50bpm.
Respiratory depression: SpO2 <90%.
Discussion
Benzodiazepines, such as diazepam and midazolam, are often used for conscious sedation in anticipation of anxiolytic, sedative, and hypnotic effects during endoscopic procedures. However, cases exist in which a paradoxical response, such as excessive movement, multivalency, and aggression, has been described. 16 The outcome of ERCP is sometimes affected by the patient being in a prone position. If a patient is likely to feel pain during ERCP, deeper sedation is required than for gastrointestinal endoscopy. However, the repeated use of benzodiazepines increases the risk of a paradoxical response, sometimes making it difficult to complete the procedure. More recently in prior studies, propofol has been widely used for sedation in endoscopic procedures. Kiriyama and colleagues 16 described how propofol has advantages with regard to the strength of sedation and speed of waking. However, propofol increases the dose-dependent frequency of respiratory depression, 17 and must be used carefully when for general use.
DEX exerts its effect through the alpha-2 receptor present in the locus ceruleus. Since the alpha-2 receptor is involved in sedation, analgesia, anxiety, and sympathetic nerve blockade, DEX shows a wide range of pharmacological actions, including sedation, analgesia, and anxiolytic activity. In addition, DEX has little affinity for gamma-aminobutyric receptors, characterized by almost no respiratory depression. However, sympathetic blockade may cause hypotension or bradycardia.18,19 The usefulness of DEX sedation has been reported in endoscopic submucosal dissection, but is considered controversial in ERCP. 20 Mazanikov and colleagues 21 reported that DEX alone is insufficient during ERCP. Lee and colleagues 12 described how combined DEX and midazolam maintains a good sedation level, and shows fewer adverse events. The utility of a combined regimen of DEX and midazolam during ERCP has been shown in previous studies.12,20 However, to our knowledge, reports examining the effectiveness of DEX combined with BZD-induced disinhibition as a paradoxical response have not been described.
In this study, sedative effects were evaluated by RSS, movement score, and the number of additional sedatives given. In particular, the combined use of DEX led to high-quality sedation and fewer excessive movements, resulting in an increase in the completion rate of the procedure (95.5% versus 63.6%). Only one patient in the DEX group had their endoscopic procedure discontinued due to excessive movement. For this patient, being in a prone position was likely the cause of movement; they subsequently underwent an endoscopic procedure when in a lateral position at the next examination. The addictive nature of BZDs for patients when used as sleeping pills and being an alcoholic can be cited as risk factors that cause paradoxical reactions.22,23 Alcoholic patients (36.4%) and those addicted to sleeping pills (13.6%) were included in our study, but better sedation was obtained when combined with DEX. In the BZD group, significant differences in the RSS score, the maximum movement score, the number of additional sedatives, and the completion rate for procedures between diazepam and midazolam were not observed. In our study, midazolam has no additional contribution over diazepam in producing the disinhibition.
However, effects on circulatory dynamics are known to be a side effect of DEX.24,25 In this study, the systolic blood pressure after sedation was significantly low in both groups. The heart rate, however, was significantly lower after sedation for patients in the DEX group only. In addition, in the DEX group, only one patient showed severe hypotension (systolic blood pressure <60 mmHg), leading to the discontinuation of DEX treatment. This patient presented with intravascular dehydration at the time of hospitalization and this was thought to be the cause of the hypotension. The SpO2 was significantly decreased in both groups. For the DEX group, this decrease in SpO2 may have been because multiple additional doses of BZD were required.
Several hypotheses exist to explain the mechanism of BZD-induced disinhibition: These include gamma-aminobutyric acid (GABA) agonism, 26 a central anticholinergic effect, 27 the involvement of the serotonin system, 28 the activation of the dopamine nervous system, 29 and an association with genetic factors. 30 DEX has a different mechanism of action from BZDs and does not act on GABA receptors. However, the mechanism of how DEX reduces the BZD-induced disinhibition has not been clarified. Dey and colleagues 31 reported that DEX reduced the stress response and suppressed myoclonus in comparison with midazolam. DEX may provide a better sedative effect by decreasing the incidence of myoclonus. Reports showing the usefulness, for BZD-induced disinhibition, of combination DEX therapy are lacking. Because DEX shows sedative, analgesic, and anti-anxiety effects stronger, it is possible to reduce pain in a patient during the endoscopic procedure, as well as reduce delirium and anxiety compared with using conventional sedatives.
However, the present study had several limitations: (a) it was a retrospective, single-center study; (b) it used a small number of patients; (c) it may have had a patient selection bias; and (d) the use of sedatives in the BZD group was inconsistent, with the amount of sedative used not able to be compared between the two groups. We hope that a well-designed prospective study in the future can resolve these problems.
Conclusion
DEX provided a high-quality sedative effect, induced lower excessive movement in patients, and led to a higher completion rate for ERCP procedures with BZD-induced disinhibition. Combination treatment with DEX may be an alternative method for cases in which continuing an endoscopic examination such as ERCP is difficult.