
Abstract
Background:
Transmural healing (TH) is being increasingly recognized for reflecting deep remission in Crohn’s disease (CD). The long-term clinical significance of achieving TH is still not fully known. We aimed to evaluate TH as a predictor of long-term positive outcomes using intestinal ultrasonography (US), with comparison with the established endpoint mucosal healing (MH).
Methods:
CD patients were consecutively recruited from September 2015 to August 2018 at a single tertiary hospital. All patients were evaluated at baseline and followed up at 6 months prospectively with a guideline-based treatment regimen. Achieving TH/MH or not was evaluated by US/colonoscopy at the first follow-up. Long-term outcomes including steroid-free clinical remission (CR), drug escalation, hospitalization, and surgery, were recorded after at least another 12 months.
Results:
We identified 77 patients with a median age of 30 years (range, 12–73 years). Twenty-five (32%) patients achieved TH, and 31 (40%) patients achieved MH. TH and MH were poorly correlated (Cohen’s κ = 0.387; p < 0.05). Univariate analysis showed that both MH and TH were associated with better long-term outcomes. In multivariate analysis, TH was an independent predictor of steroid-free CR [odds ratio (OR), 52.6; p < 0.001], drug escalation (OR, 0.1; p = 0.002), and hospitalization (OR, 0.05; p = 0.005), while MH was an independent predictor of drug escalation (OR, 0.3; p = 0.05). Smoking habit was the only predictor of surgery (OR, 6.6; p = 0.02).
Conclusion:
TH is an independent predictor of more favorable long-term outcomes than MH, suggesting that TH could become the potential treatment endpoint in CD.
Plain language summary
The therapeutic endpoints of Crohn’s disease keep evolving. The long-term clinical significance of achieving transmural healing is not fully discovered.
Transmural healing is an independent predictor of more favorable long-term outcomes than mucosal healing.
Transmural healing could become the potential treatment endpoint in Crohn’s disease.
Introduction
Crohn’s disease (CD) is a condition of chronic, relapsing bowel inflammation that can severely damage bowel structures and cause complications, greatly compromising patients’ quality of life and shortening their lifespans. 1 Because persistent inflammation correlates with disease progression and surgery rates,2,3 the treatment regimen aims to eliminate bowel inflammation.
Mucosal healing (MH), as assessed by ileocolonoscopy, is the gold-standard criterion for inflammation resolution and has been widely used for years as the endpoint of CD treatment. 4 Multiple systematic reviews and meta-analyses have demonstrated that it is a strong predictor of long-term steroid-free clinical remission (CR), as well as low rates of hospitalization and surgery.5–8 However, researchers have continuously questioned whether MH can reveal the entirety of inflammation, since (1) CD is characterized by transmural inflammation from the mucosa to the serosa, meaning that active intramural inflammation can exist concurrently with endoscopically demonstrated MH; 9 and (2) ileocolonoscopy cannot evaluate the condition of the small intestine except for the terminal ileum. Therefore, in recent years, transmural healing (TH) has been proposed as a potential new treatment endpoint in CD.10–12
Generally, the definition of TH is: the normalization (⩽3 mm) of bowel wall thickness (BWT), with the normalization of stratification, no hypervascularization, and the resolution of mesenteric inflammatory fat.13,14 Cross-sectional diagnostic modalities, such as ultrasonography (US), computed-tomography enterography (CTE), and magnetic-resonance enterography (MRE), are commonly used tools to detect TH. Among them, US is a non-radiative, non-invasive, and cost-effective method with high sensitivity in detecting bowel lesions by evaluating thickened bowel walls, ulcers, and both intramural and extramural abscesses. 15 Preliminary studies have shown that TH is associated with lower rates of drug escalation, CD-related hospitalizations, and surgeries, despite heterogeneous study design and inconsistent TH definitions.11,16,17 It is still not known whether TH or MH is the better prognostic indicator of long-term outcomes. Therefore, our study aimed to determine TH’s ability to predict long-term outcomes in the presence of MH and other related factors.
Methods
Patients and study design
This was a prospective, longitudinal cohort study at a single tertiary hospital in China. We enrolled CD patients who had been consecutively hospitalized from September 2015 to August 2018 following inclusion criteria: (1) confirmed diagnosis of CD, based on European Crohn’s and Colitis Organization (ECCO) guidelines (second consensus for patients diagnosing before January 2017, and third consensus for patients diagnosing after);18,19 (2) no use of CD-related steroids, immunosuppressants, or biologics for at least 6 months prior, and about to initiate a new course of CD-related medication therapy; and (3) follow-up with intestinal US along with routine evaluations at 6-month intervals for at least 18 months (three follow-ups) from study onset. Exclusion criteria were as follows: (1) pregnancy; severe systemic comorbidities; or other bowel comorbidities such as malignant intestinal tumors, Behçet’s disease, or intestinal tuberculosis; (2) incomplete colonoscopy examination.
We collected enrolled patients’ demographic information, clinical courses of disease, past and family histories, Crohn’s Disease Activity Index (CDAI), laboratory tests, cross-sectional imaging data, colonoscopy results, and pathological findings at baseline. In accordance with ECCO guidelines, different medications at different doses were prescribed based on disease status, medication history, and personal willingness. At each follow-up evaluation, we required patients to undergo a thorough assessment involving CDAI, serum C-reactive protein (CRP) levels, the simple endoscopic score for CD (SES-CD), and the US with/without other tests (i.e. CTE and MRE) as a standard regime. 20 The time between US and colonoscopy had to be within 2 weeks. MH and TH were evaluated at the first follow-up evaluation (6 months from baseline), and further follow-ups for at least 12 months were tracked to assess the long-term outcomes. The general principle of medication adjustment is: if patients presented with clinical remission and an obvious recovery under endoscopy and/or by radiological methods at 6 months, a continuance of the original therapy was usually suggested to wait for MH/TH. If patients presented with no clinical remission, or no improvements by endoscopy/CTE/US, a dose escalation, switch or swap of medication might be suggested as determined by a comprehensive clinical, endoscopic, and radiological evaluation, plus the consideration of side effects and economic conditions.
The Institutional Review Board (IRB) of Peking Union Medical College Hospital (Beijing, China) has reviewed the protocol of this manuscript and determined that this study is exempt from full IRB review and informed consent.
Colonoscopic evaluation and MH
Experienced gastroenterologists performed colonoscopies in accordance with standardized procedures. A gastroenterologist with more than 10 years of experience in inflammatory bowel disease treatment who was blinded to radiological information interpreted the colonoscopic images at the 6-month follow-up. MH was defined as no ulcerations in any bowel segment (SES-CD 0–2) at follow-up endoscopy in patients who had ulcerations present on baseline ileocolonoscopic images, on the premise that the colonoscope must reach the terminal ileal area. 6 For patients with L4 diseases, both upper endoscopy and ileocolonoscopy were applied to assess MH following the same criteria.
US evaluation and TH
One radiologist with more than 10 years of experience in intestinal imaging performed intestinal US studies using a Philips iU22 machine (Philips Healthcare, Bothell, WA, USA) with convex (C5-2) and linear (L9-3) transducers, following the European Federation of Societies for Ultrasound in Medicine and Biology guidelines. 21 Patients fasted for at least 8 h before US examination. The average body mass index of enrolled patients was 20.5 kg/m2; therefore, US image quality was good for all patients. The colon was scanned consecutively, with BWT measured at the ileocecal area, ascending colon, transverse colon, descending colon, and sigmoid colon continuously with a 2 cm distance. The small intestine was examined throughout the abdomen to look for diseased sections. BWT was measured at the left-upper, left-lower, right-upper, and right-lower quadrants of the small intestine, the pelvic intestine, and the terminal ileum. BWT ⩾3 mm was considered abnormal. At least two BWT measurements were undertaken for each bowel section. When the abnormal bowel section was identified, the radiologist further assessed features such as maximum BWT, bowel wall structure, vascularity, and complications (fistulas, strictures, or abscesses) at the diseased location.
TH was defined as BWT ⩽3 mm in any place, with the normalization of stratification, no hypervascularization, the resolution of mesenteric inflammatory fat, and no signs of active inflammation (abscesses or fistulas).13,14 Images and videos from baseline and the 6-month follow-up evaluation were reviewed by two radiologists, both with more than 10 years of experience in intestinal imaging; each of them was unaware of clinical, laboratory, endoscopic, and other radiological findings, as well as of the other radiologist’s opinion. If a difference of opinion occurred, a third radiologist with more than 15 years of experience in intestinal imaging would be referred to make a final diagnosis.
Some enrolled patients also underwent CTE, which we performed using a 16-slice MDCT scanner (GE Light Speed Pro; GE Healthcare, Chicago, IL, USA). A bowel cleanse was performed beforehand. Patients ingested 1500 ml mannitol followed by 500 ml water over 60 min prior to the examination for bowel extension. Next, they were scanned during the enteric phase (peak small-bowel enhancement) 50 s after intravenous injection of iodinated contrast agent. Multi-planar images were reconstructed at a high spatial resolution (slice thickness, 3 mm).
TH in these patients was evaluated by one experienced radiologist specializing in CT abdominal imaging and blinded to clinical, laboratory, endoscopic, and other radiological findings. On CTE, TH was defined as a reduction in lesion length to 0 cm and a score <1 (four point scale) for all other parameters (decreased enhancement or length of disease, no worsening of parameters of active inflammation – dilated vasa recta/comb sign, perienteric inflammation (edema, phlegmon, or abscess), or fistula. 22
Long-term outcomes
The positive outcome was steroid-free CR, which, in accordance with ECCO guidelines, we defined as CDAI <150 without the use of systemic steroids or budesonide at any evaluation during follow-up.18,19 The three negative outcomes included drug escalation, hospitalization, and surgery. Drug escalation was defined as a swap of original drugs to a higher class or an increase of either dosage or interval. Corticosteroid usage during the follow-up period was also considered as drug escalation. The treatment regimen was in accordance with ECCO guidelines based on clinical symptoms and colonoscopic manifestations. 23 Hospitalization was defined as any CD-related admission, with causes including disease relapse, complication, and drug side effects, except for surgery. Surgery was defined as any CD-related intestinal procedure except for perianal procedures.
Statistics
We performed statistical analysis using SPSS software version 23 (IBM Corp., Armonk, NY, USA). Descriptive statistics were reported as number (percent) for categorical variables, or median (range) for continuous variables. Cohen’s kappa (κ) coefficient was calculated for agreement estimation among CR, MH, and TH; κ-value was defined as poor (<0.20), fair (0.20–0.40), moderate (0.40–0.60), good (0.60–0.80), or very good (0.80–1.00). We estimated the cumulative probability of long-term outcomes using Kaplan–Meier (KM) survival curves. The log-rank test was used to compare difference between groups. Binary logistic-regression analyses were performed to find the independent predictors of long-term outcomes. In multivariate analyses, we assessed patient characteristics such as sex, age, smoking habit, previous bowel surgery, and previous use of anti-tumor necrosis factor (anti-TNF) agents; disease characteristics such as location, behavior, and perianal disease; therapy regimens including 5-ASA, thiopurines, anti-TNF agents, thalidomide, combination therapy; whether the regimen started with prednisone, or whether dosage was increased during treatment; and TH and MH. Factors with p < 0.1 were included. An experienced biomedical statistician reviewed the statistical methods used in this study.
Results
Patient information
We identified a total of 104 consecutive patients at our medical center who met the inclusion criteria during the study period. Of them, 18 decided to discontinue US as their follow-up imaging modality, and nine patients were lost to follow-up. Ultimately, 77 patients were analyzed; 70% were male, and the median age was 30 years (range, 12–73 years). Median disease duration was 81 months (range, 14–420 months). All patients were in the active phase at baseline, with the median CDAI of 358 (range, 151–440). The mean SES-CD was 24 (range, 7–50). Baseline characteristics of enrolled patients are listed in Table 1.
Baseline characteristics of enrolled CD patients.
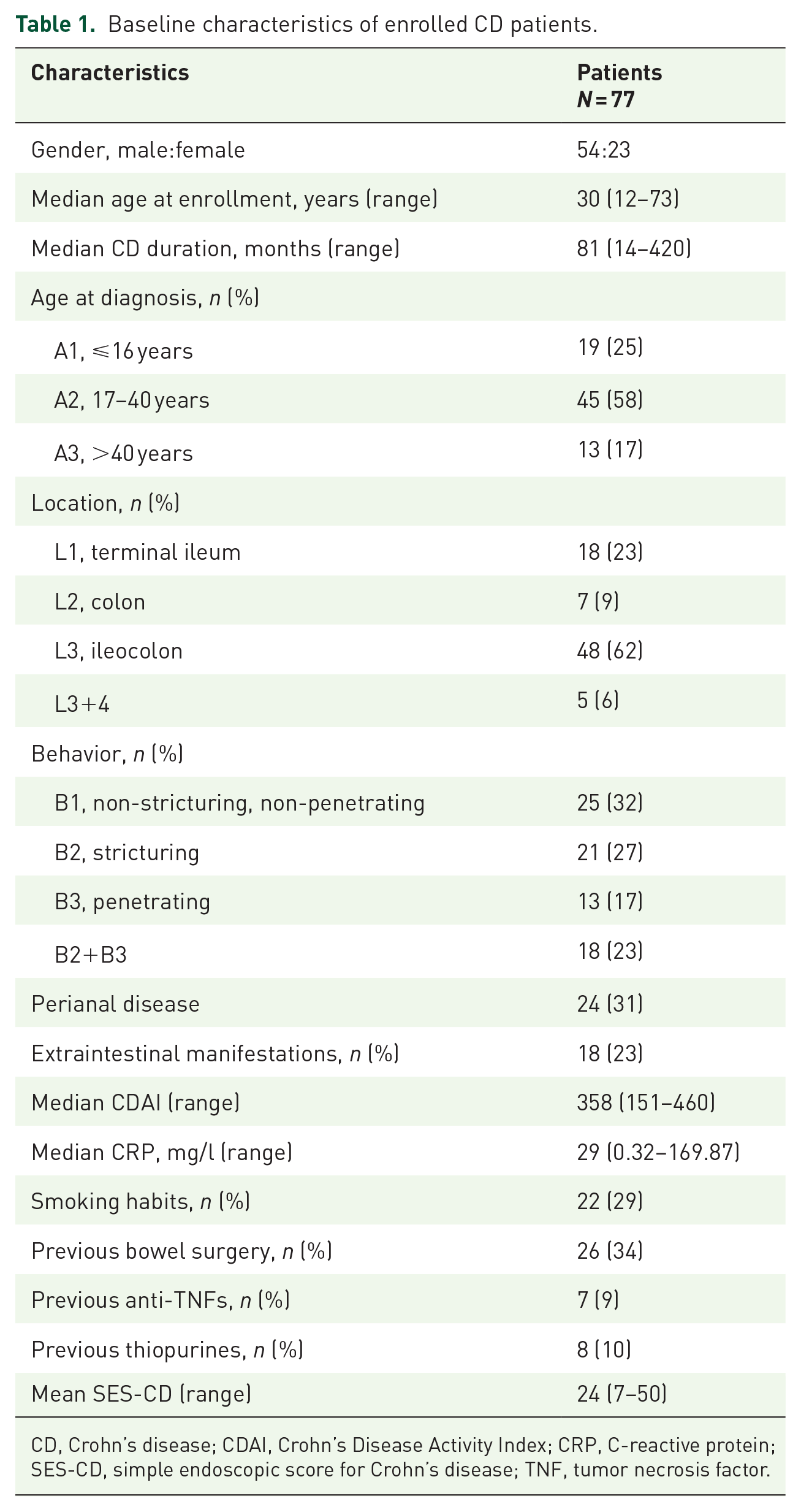
CD, Crohn’s disease; CDAI, Crohn’s Disease Activity Index; CRP, C-reactive protein; SES-CD, simple endoscopic score for Crohn’s disease; TNF, tumor necrosis factor.
Medication used in enrolled patients and the MH/TH rates in different treatment groups are listed in Supplemental material Table 1 online. Thiopurines were the most common (33/77, 43%), followed by anti-TNF agents (14/77, 18%) and 5-ASA agents (14/77, 18%). Seven percent of patients were treated with combination therapy (anti-TNF agents + thiopurines), 38/77 (49%) of patients started treatment with prednisone. Patients with anti-TNF agents achieved higher TH/MH rates than with most other drugs; however, no statistically significant differences were found between any groups.
US characteristics of enrolled patients at baseline and the 6-month follow-up evaluation are listed in Supplemental Table 2. The most commonly involved site was the ileocecal area (61/77, 79%); the most frequent complication was fistulas (23/77, 30%). After 6-month treatment, the BWT, bowel wall structure, and vascularity of the former involved sites were significantly recovered.
Evaluation of treatment response
We performed comprehensive follow-ups after 6 months of treatment, including clinical, laboratory, sonographic, and endoscopic examinations. Colonoscopy results showed that 31/77 (40%) patients achieved MH; US results showed that 25/77 (32%) achieved TH. TH and MH were poorly correlated (Cohen’s κ = 0.387; p < 0.05). Eight patients achieved TH but not MH; and 14 patients achieved MH but not TH. There were 35/77 (45%) enrolled patients who also underwent CTE at their 6-month evaluations. Results of the two imaging techniques had a high level of agreement [Cohen’s κ = 0.793; p < 0.001; total agreement rate = 97% (34/35)]. Comparable US, CTE, and colonoscopic images of one representative patient are presented in Figure 1. TH correlated poorly with CR (Cohen’s κ = 0.157; p < 0.05) and poorly with normal CRP levels (Cohen’s κ = 0.230; p < 0.05).

Comparable ultrasonography (US), computed-tomography enterography (CTE), and colonoscopic images in evaluation of transmural and mucosal healing.
Prediction of long-term outcomes
We followed up with enrolled patients for at least another 12 months after TH/MH evaluations to record their long-term outcomes. The average follow-up time was 19 months (range, 12–42 months). The full versions of univariant and multivariant analyses are presented in Supplemental Tables 3–6.
Steroid-free CR
During the follow-up period, 30/77 (39%) patients achieved sustained steroid-free CR. KM survival analysis demonstrated a significantly higher cumulative probability of steroid-free CR among patients with MH than those without (log-rank p = 0.003). Similarly, a significantly higher cumulative probability of steroid-free CR was demonstrated among patients with TH than those without [log-rank p < 0.001; Figure 2(a)]. In logistic-regression analysis, smoking habit [odds ratio (OR), 0.1; 95% confidence interval (CI), 0.02–0.90; p = 0.04] and TH (OR, 52.6; 95% CI, 10.1–250; p < 0.001) were independent predictors of steroid-free CR (Table 2).
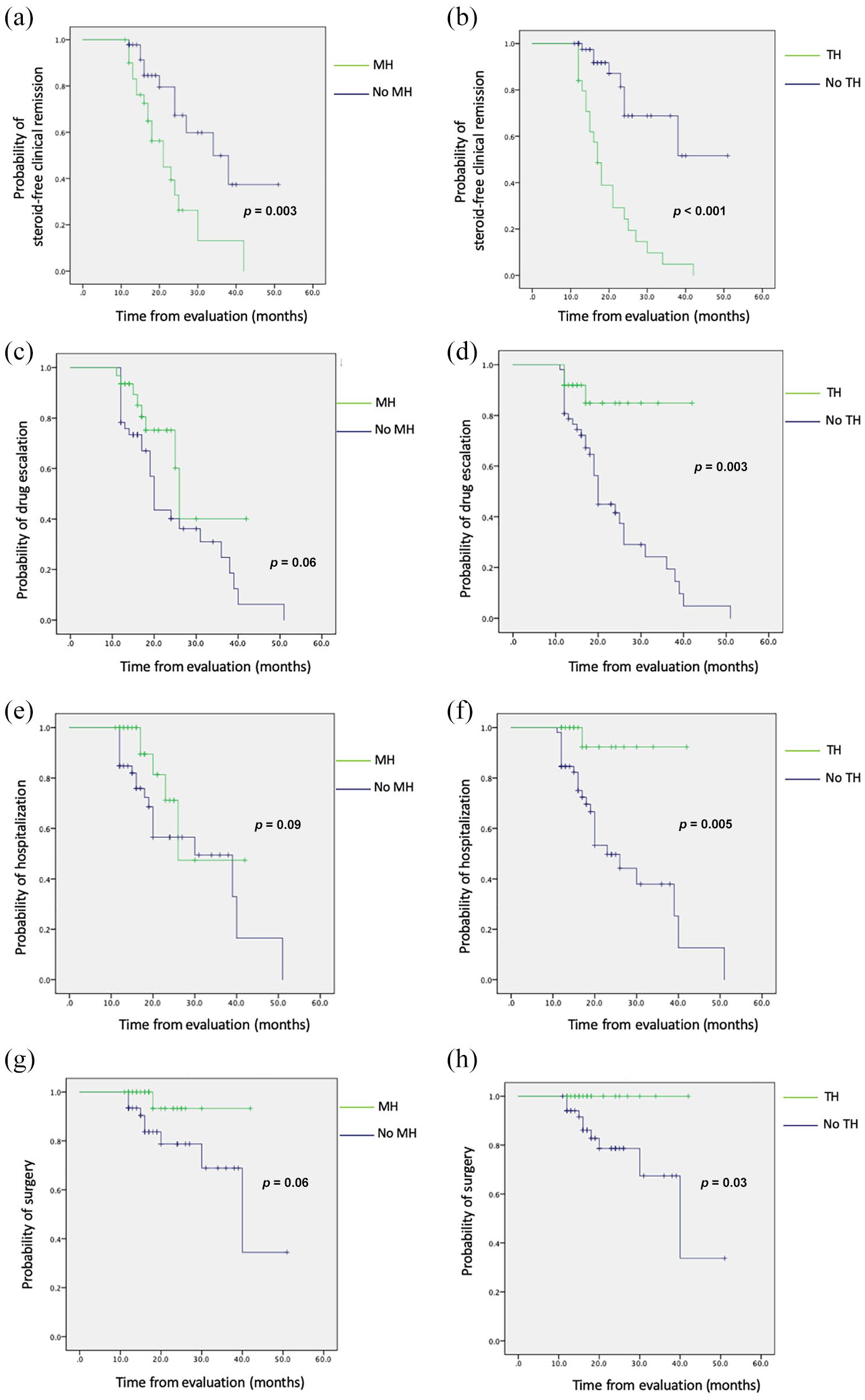
Cumulative survival rates with long-term outcomes of mucosal healing (MH) and transmural healing (TH). (a) and (b) Steroid-free clinical remission. (c) and (d) Drug escalation. (e) and (f) Crohn’s disease (CD)-related hospitalization. (g) and (h) CD-related surgery.
Multivariate analysis for long-term outcomes.
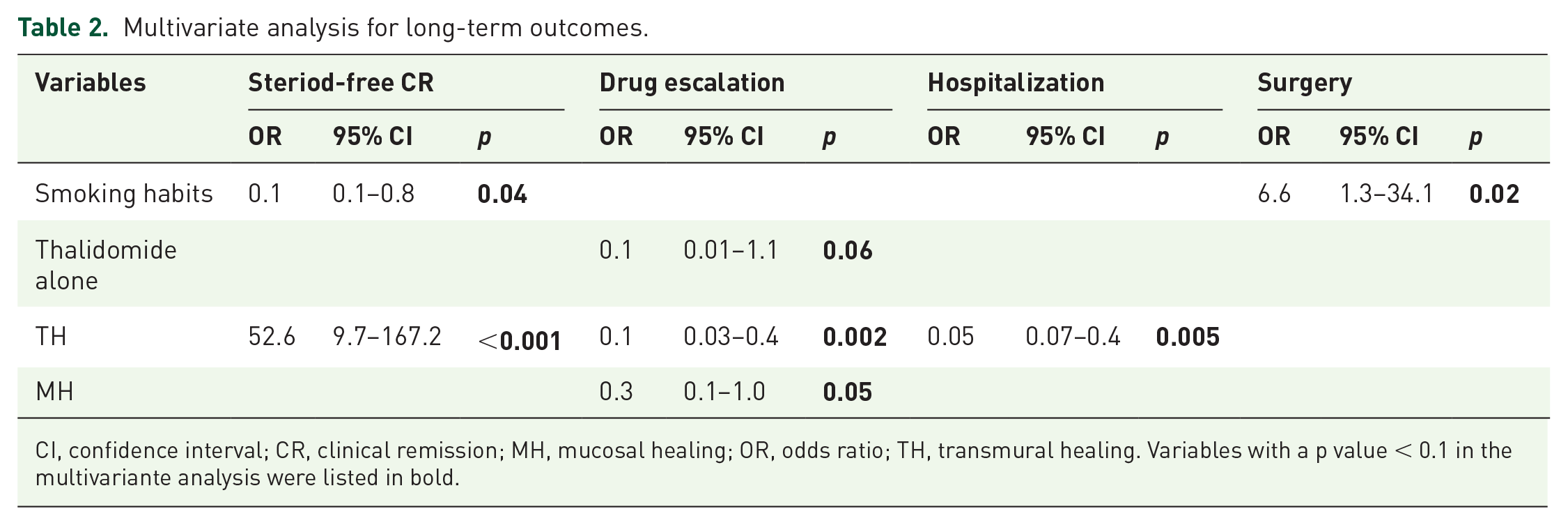
CI, confidence interval; CR, clinical remission; MH, mucosal healing; OR, odds ratio; TH, transmural healing. Variables with a p value < 0.1 in the multivariante analysis were listed in bold.
Drug escalation
During follow-up, 37/77 (48%) patients underwent drug escalation. KM survival analysis showed that patients with MH had a longer time to drug escalation than those without (log-rank p = 0.06); the same was true of patients with TH versus those without [log-rank p = 0.003; Figure 2(b)]. In logistic-regression analysis, use of thalidomide (OR, 0.1; 95% CI; 0.01–1.1, p = 0.06), TH (OR, 0.1; 95% CI, 0.03–0.40; p = 0.002), and MH (OR, 0.3; 95% CI, 0.1–1.0; p = 0.05) were independent predictors of drug escalation (Table 2).
Hospitalization
During follow-up, 24/77 (31%) patients were hospitalized. Time to hospitalization was longer for patients with MH than those without (log-rank p = 0.09), and the same was true for patients with TH versus those without [log-rank p = 0.005; Figure 2(c)]. In logistic-regression analysis, TH (OR, 0.05; 95% CI, 0.07–0.4; p = 0.005) was the only independent predictor of drug escalation (Table 2).
Surgery
During follow-up, 11/77 (14%) patients underwent surgery. KM survival analysis showed that patients with MH had a longer time to surgery than those without (log-rank p = 0.06), and the same was true of patients with TH versus those without [log-rank p = 0.03; Figure 2(d)]. In a logistic regression analysis, smoking (OR, 6.6; 95% CI, 1.3–34.1; p = 0.02) was the only independent predictor of surgery (Table 2).
Discussion
The goal of CD treatment has been constantly changing throughout the years, from simple symptom remission to long-term maintenance of symptom remission, to complete pathological healing and disease cure. Consequently, the treatment endpoint has also kept evolving. 24 MH has long been considered the gold-standard treatment endpoint, but its limitations are obvious as well, including the inability to indicate the transmural pathological features of CD, poor access to the small intestine, and contraindication for patients with stenosis or perforation. In a meta-analysis by Reinink et al., 8 MH predicted lower rates of surgeries and hospitalizations and higher rates of CR, but relative-risk values were just within 0.34–1.84. In addition, complete MH is not significantly different from partial healing in predicting surgeries and hospitalizations, which indicates that MH might represent only partial bowel healing. In short, it seems that MH is not the perfect indicator of complete pathological-healing status.
Cross-sectional modalities such as US and MRE have also been used as important tools for disease evaluation. Their advantage is to provide a more comprehensive evaluation of all layers of the bowel wall, which fit the pathological behavior of CD. 25 Consequently, recently, TH was proposed to be assessed as a measure of the remission depth in addition to the classical therapeutic targets – clinical remission and MH. 26 Recent studies have shown the benefits of attaining TH in long-term outcomes, although the definition of TH varies.27,28 Deepak et al. 22 and Zorzi et al. 28 evaluated TH based on radiological manifestations in CTE/MRE/small-intestine contrast US solely and showed that TH is associated with low risks of hospitalization, surgery, and need for steroids. However, as their multivariate analysis did not include MH, neither team was able to determine the relationship between MH and TH or which was better at predicting long-term outcomes. Several studies have considered TH a combination of radiological TH plus MH, which has a strong association with good clinical outcomes.11,17,29 Although the correlation between endoscopic and transmural findings has been well investigated in the setting of postoperative CD recurrence, a minority of patients with mild mucosal disease can show TH at US. 30 In addition, for patients who cannot undergo colonoscopy, it is still unknown whether radiological TH can be a reliable treatment endpoint. For these reasons, we believe it is necessary to explore the predictive value of radiological TH as a separate factor along with MH.
In our study, we assessed MH and TH by colonoscopy and US/CTE independently. Results showed a good correlation between US and CTE in identifying TH, whereas TH had a poor agreement with MH. This might be explained by the healing process of CD not being uniform; for example, mucosal ulcers can disappear ahead of transmural inflammation in some cases, whereas in other cases the reverse happens. Both TH and MH are associated with a lower presence of negative outcomes and a higher cumulative probability of long-term remission. In our multivariate analysis, TH was associated with long-term CR, drug escalation, and hospitalization, while MH was associated only with drug escalation. Although MH was associated with all three outcomes in univariate analysis, it seems that TH was a more powerful predictor and might have interacted with MH. The practical significance of this result was that TH should be considered a more important indicator for a good prognosis than MH and should be favored when TH and MH are inconsistent.
Our study showed that neither TH nor MH was associated with surgery, even though both TH and MH were associated with surgery rate in univariate analysis. In other studies, TH was proven to be associated with lower rates of surgery, although the definition and methodology of TH were different from our study.11,17 Our results might have been due to the strong association between smoking and surgery, or to the relatively small sample size.
We used intestinal US to assess TH. The value of this imaging modality in diagnosing and assessing intestinal complications in CD patients has been proven,31,32 but only a few studies report on its value in evaluating TH and predicting long-term outcomes. Ripollés et al. 12 showed that US manifestations at 12 weeks of treatment can predict clinical outcomes at 52 weeks. Orlando et al. 33 found that the strain ratio of US elasticity imaging at 14 weeks was correlated with clinical outcomes at 52 weeks. Our study further validated the usefulness of US for TH evaluation over a longer follow-up time and also compared the predictive role of TH with that of MH. While MRE might be the more mainstream cross-sectional imaging technique in Europe and North America, intestinal US is more popular in developing countries, as it is more cost-effective and comfortable than MRE. Therefore, this study is of great importance for the clinical application of US for CD patients in these countries.
We evaluated MH/TH at 6 months after therapy initiation, which is a relatively early time-point. In previous studies, MH/TH was evaluated at 3/6/12/24 months of treatment, and all studies found the association between MH/TH and long-term outcomes, suggesting that the evaluation time might not be a decisive factor. 5 Furthermore, the early response to therapy is also an important sign that may reflect the long-term outcomes, as supported by several studies.12,33 That we chose to evaluate MH/TH at 6 months is because it is the time-point of the first follow-up, which is critically important for estimating therapeutic response and adjusting treatment strategies if necessary. However, we acknowledge that the evaluation at 6 months might underestimate the MH/TH rate in some patients.
Another difference between our study and previous ones is that we enrolled consecutive patients with various drug regimens, not only with anti-TNFs or thiopurines. Therefore, our results reflected a more general spectrum of treatment responses in clinical practice. In our study, patients with anti-TNF agents achieved higher TH/MH rates than most other drugs, but with no statistically significant differences, which is probably due to the small sample size. Thalidomide therapy was found to have a negative correlation to drug escalation. Thalidomide has been proved effective in children and adult patients with refractory active CD. 34 ECCO/European Society for Paediatric Gastroenterology Hepatology and Nutrition guidelines recommended using thalidomide in anti-TNF agent responders who do not tolerate or lost response to biologic anti-TNF agents. 35 In this study, we used thalidomide as the second-line medication for adult patients with refractory CD who were dependent/resistant or intolerant to corticosteroids and/or immunomodulators or biologics, or a substitute of anti-TNF agents when adult patients cannot afford them. As to its efficacy, several studies presented an MH rate ranging from 28.1% to 50.0%.36,37 Our MH rate of thalidomide fell within this range.
Furthermore, although CD in children appears to be more aggressive than in adults, there was no difference regarding the age group and positive long-term outcomes in the presence of TH in our study. The results imply that achievement of TH should be attempted in patients of any age group through therapeutic efforts.
There were several limitations to our study as well. First, original US data were acquired by only one radiologist, which could have introduced potential bias in machine settings and image saving. Second, we did not look at the evaluation results lesion by lesion, due to hard backtracking on endoscopic and US images in every lesion. Third, we did not discuss the differences of TH/MH rates between CD subgroups, such as age subgroups, therapeutic subgroups, et cetera, as limited by the sample size. Since the sample size was relatively small compared with previous studies, future large-sampled research is required to further validate our results.
In conclusion, our findings showed that TH was a good predictor of favorable long-term CD outcomes in the presence of MH, suggesting that TH has the potential to become the new treatment endpoint in CD.
Supplemental Material
sj-docx-1-tag-10.1177_17562848211016259 – Supplemental material for Comparison of transmural healing and mucosal healing as predictors of positive long-term outcomes in Crohn’s disease
Supplemental material, sj-docx-1-tag-10.1177_17562848211016259 for Comparison of transmural healing and mucosal healing as predictors of positive long-term outcomes in Crohn’s disease by Li Ma, Wenbo Li, Nan Zhuang, Hong Yang, Wei Liu, Weixun Zhou, Yuxin Jiang, Jianchu Li, Qingli Zhu and Jiaming Qian in Therapeutic Advances in Gastroenterology
Footnotes
Author contributions
Conception and design: Qingli Zhu, Li Ma, Wenbo Li, Jiaming Qian. Administrative support: Yuxin Jiang, Jianchu Li. Provision of study materials or patients: Li Ma, Nan Zhuang, Wenbo Li, Wei Liu, Hong Yang, Weixun Zhou. Collection and assembly of data: Li Ma, Wenbo Li. Data analysis and interpretation: Li Ma, Wenbo Li, Nan Zhuang. Manuscript writing: all authors. Final approval of manuscript: all authors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Sciences Foundation of China (grant number 81971640) and CAMS Innovation Fund for Medical Sciences (grant number 2017-I2M-1-006).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.