
Abstract
Background:
In France, the colorectal cancer organised screening programme uses the faecal immunological test. A positive test ⩾30 μg Hb/g of stool leads to a colonoscopy for identification of potential colorectal lesions. Cut-off values vary from 20 to 47 μg Hb/g of stool in Western countries. We herein question this threshold’s relevance in a French population and perform a retrospective observational study using the Parisian database between 1 April 2015 and 31 December 2018.
Methods:
Rates of participation, numbers of positive faecal immunological test (FIT), detection rates and positive predictive values for advanced adenomas and/or colorectal cancer were determined. Mean positivity values for colorectal lesions were calculated.
Results:
In our population, there were 4.1% positive tests and 67.6% colonoscopy results available with final reports. Positive predictive value for advanced adenomas and colorectal cancer were 30% [95% confidence interval (CI) 29.8–30.3] and 7.4% (95% CI 7.35–7.52), respectively. The mean positivity value for all positive tests in our population was 101.7 µg Hb/g of stool (95% CI 85–118.3). There were 1136 normal colonoscopies (21.4%) with a mean positivity value of 88.6 μg Hb/g of stool. Following a negative test in a first screening campaign, 40.8% of patients in our population performed a second test with a positivity rate of 1.3% and with the encounter of 81 colorectal cancers. The risk of having a positive test during the second screening campaign and finding advanced colorectal lesions significantly increased (all p < 0.001) when comparing negative FIT results ranging between 15 and 29 μg Hb/g of stool to 0 and 14 μg Hb/g of stool from the previous campaign.
Conclusion:
Using the current positivity threshold, some patients were considered negative with a delay in colorectal cancer diagnosis, suggesting the threshold could be lowered. Also, the mean positivity value for normal colonoscopies was high, raising the question of upper gastrointestinal bleeding.
Introduction
In France, colorectal cancer (CRC) is a public health issue with an incidence of more than 40000 cases in 2015 (www.e-cancer.fr). It benefits from an organised nationwide screening programme to identify asymptomatic individuals with advanced adenomas (AAs) and/or early cancer. It addresses a population aged from 50- to 74-years old who receive an invitation for the test every 2 years. In France, it is based on a two-step strategy: first the use of a stool test and then, if positive, the performance of a colonoscopy. The quantitative faecal immunological test (FIT; OC sensor®) has been used since April 2015, replacing the guaiac-based Hemoccult®. Guaiac-based tests such as Hemoccult® have been criticised for their fairly low sensitivity and their lack of specificity for human haemoglobulin (Hb). 1 Indeed, they could also detect traces of animal blood after ingestion, which led to false-positive results. The cumulative risk of false positive with guaiac-based tests after 10 years of CRC screening was 23%. 2 The OC sensor® is now the recommended screening test in France, supported by trials demonstrating its effectiveness in CRC prevention and because of its specificity for the human blood.3–5
The actual French recommended threshold of positivity for the OC sensor® is 30 µg Hb/g of stool. Various studies have tried to identify the optimal cut-off value for the test. FIT being a quantitative test, its value should be proportional to the bleeding intensity which could be the consequence of an advanced colorectal lesion. In Lee et al.’s 6 meta-analysis, varying the cut-off value influenced the performance characteristics of FIT. This work suggested that a 20 μg Hb/g of stool threshold had the best combination of sensitivity and specificity for CRC compared with values ranging from 20 μg Hb/g to 50 μg Hb/g of stool, or greater. 6 In a European simulation modeling analysis with the OC-Sensor®, different cut-off strategies ranging from 10 μg Hb/g to 150 μg Hb/g of stool were compared and a cut-off value of 50 μg Hb/g was the most efficient and cost-effective strategy, assuming a specificity of 95.8%. 7 In the meantime, in a Korean study, there was no significant difference in advanced neoplasia detection using a threshold of 20 μg Hb/g versus 10 μg Hb/g of stool (28.9% versus 30.8%). 8 Based on these studies, the US task force recommends a cut-off value of 20 μg Hb/g of stool. 3 Finally, in Toes-Zoutendijk et al.’s 9 work, the initial threshold chosen in The Netherlands was 15 µg Hb/g of stool, but to reach the intended balance of harms and benefits recommended by the Dutch Health Council, the threshold value was raised to 47 µg Hb/g of stool in the second part of the study. With this new threshold the false-positive rate lowered from 5% to 2.6% but the number of positive tests also decreased (from 7.8% to 6.3%) leading to less colorectal lesions identified. 9
To sum up, FIT positivity thresholds vary between countries because of differences in health programmes and finding the optimal cut-off value is a challenge. Based on the CRC screening programme database for Paris, we herein evaluate the efficacy of the 30 µg Hb/g of stool threshold.
Methodology
A retrospective observational study was performed. The data were extracted from the computerised CRCDC-IDF (dépistage des cancers Ile de France) registry in Paris. We evaluated the population of patients who performed a FIT between 1 April 2015 and 31 December 2018 in Paris, France.
Description of the Paris CRC screening programme
The CRC screening programme in Paris was previously described with the results of the first months of screening with FIT in Paris. 10 It is centrally managed by the CRCDC-IDF office which invited the eligible population: asymptomatic adults aged 50–74 years’ old, attached to the Parisian health insurance and not enrolled in an individual CRC screening.
Invitations for participation to the CRC screening programme were sent by mail from the CRCDC-IDF office. Individuals were invited to consult their general practitioner (GP) who distributed the OC Sensor® freely. The invitation was sent every 2 years. If patients did not respond, a first reminder was sent after 90 days. A second reminder could be sent after 120 days if there was still no answer. After invitation, patients could be excluded for medical reasons (death, individual screening programme, etc.), change in address of residence or performance of a recent colonoscopy (in the past 5 years). Analysis was then performed on one sample of stool after participants returned it by mail in a prepaid envelope. When the first test was negative, patients received a new invitation 2 years later. If the test was positive, they were advised to perform a colonoscopy for detection and/or treatment of potential colorectal lesions and addressed to a gastroenterologist (GI). Participants whose sample was not assessable (outdated test, error in filling out the form, etc.) were sent a new test. Individuals who did not respond to the invitations after reminders were labelled as non-responders.
Colonoscopy was the standard diagnostic and/or therapeutic exam after a positive test. Some patients could also be referred for a virtual colonoscopy by their GI. When the colonoscopy was performed, the CRCDC-IDF office recovered colonoscopy and pathology reports when possible. If colonoscopy reports could not be recovered, patients’ results were not registered in the Parisian screening database.
Outcomes and statistical analyses
Data were collected to assess results with FIT in our population. The study was observational with only descriptive data. Regarding FIT, we evaluated participation and positivity rates. Also, we evaluated the colonoscopy participation rate but also detection rates and positive predictive values (PPVs) for colorectal lesions. Finally, we calculated the mean value of positivity for each encountered lesion.
The FIT participation rate was defined as the number of persons performing the test (one stool sample) divided by the number of persons invited by the CRCDC-IDF minus the excluded population. The positivity rate was defined by the number of patients with a result at or above 30 µg Hb/g of stool divided by the number of participants with an assessable test. The participation rate for colonoscopy was defined by the number of patients performing a colonoscopy exam with available reports divided by the number of patients with a positive FIT.
Colonoscopies were considered complete when the caecum was reached. Colonoscopies were considered normal when no colorectal lesions were described in the report. Colorectal lesions described in our work were benign lesions (haemorrhoids and diverticula), inflammatory bowel disease (IBD), polyps (hyperplasic and adenomas) and CRC. Polyps with a risk of transformation, or AAs, were defined as adenomas with size of 10 mm and/or larger, and/or with histology showing villous component and/or high-grade dysplasia. Serrated polyps were not described in our work because not registered in the Parisian database.
The detection rate was defined as the proportion of individuals with colorectal lesions detected during a colonoscopy per 1000 screened individuals with an assessable FIT. PPVs were calculated as the number of patients with colorectal lesions divided by the number of patients who underwent a colonoscopy with available pathology reports. The false-positive rate was defined as the number of patients with a normal colonoscopy divided by the number of patients with a positive test. For each type of encountered lesion, the mean value of positivity was defined as the sum of all test values divided by the number of tests. For our main results we will also show 95% confidence intervals (95% CI).
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics
The Ethical Review Committee for publications of the Cochin University Hospital (CLEP) has examined the research and found it conformed to generally accepted scientific principles and research ethical standards and in conformity with the laws and regulations of the country in which the research experiment was performed. The need for informed patient consent was waived by the ethical committee due to the retrospective nature of the study. CLEP decision no. AAA-2019-08004.
Results
Through the organised screening programme 754154 invitation letters were sent to eligible individuals (women and men), representing 26% of the overall Parisian population (Figure 1). From it, 534073 (78.8%) individuals received a second invitation. Some 32845 patients (4.3%) were excluded, mainly due to the knowledge of a colonoscopy performed in the 5 previous years or of pre-existing digestive diseases. A total of 192565 tests were performed, resulting in a FIT participation rate of 25.5%. Tests were positive in 7937 (4.1%) participants, including 3733 positive tests in women and 4204 in men. About 36% of participants with a positive test were aged between 50- and 59-years old. A total of 9.9% of tests were not assessable.

Flow chart of the CRC screening programme in the Parisian population, between 1 April 2015 and 31 December 2018 in Paris.
For the 7937 positive tests, 5949 individuals (74.9%) performed a colonoscopy but only 5367 individuals (67.6%) had a full final report (with histology when needed), including 53 incomplete colonoscopies. Therefore, a total of 5314 colonoscopies were considered for the final analysis, including 69 virtual exams. Seventeen patients refused a colonoscopy after a positive test.
Mean time to colonoscopy after a positive test was 81.3 days. A total of 412 GIs performed these exams with a mean of 12 (1–180) colonoscopies by a physician. The majority of colonoscopies were performed in private practice (>75%).
Detection rates, PPV values
In patients with a positive test and available results, 1136 participants had a normal colonoscopy (21.4%). The false-positive rate was 14.3%. A total of 4178 colorectal lesions were encountered including 905 adenomas [PPV = 17.0% (95% CI 16.9–17.2)], 1595 AAs [PPV = 30.0% (95% CI 29.8–30.3)] and 395 CRC [PPV = 7.4% (95% CI 7.35–7.52); Table 1].
Mean values of positivity for colorectal lesions encountered with positive FIT in the studied population between 1 April 2015 and 31 December 2018 in Paris.
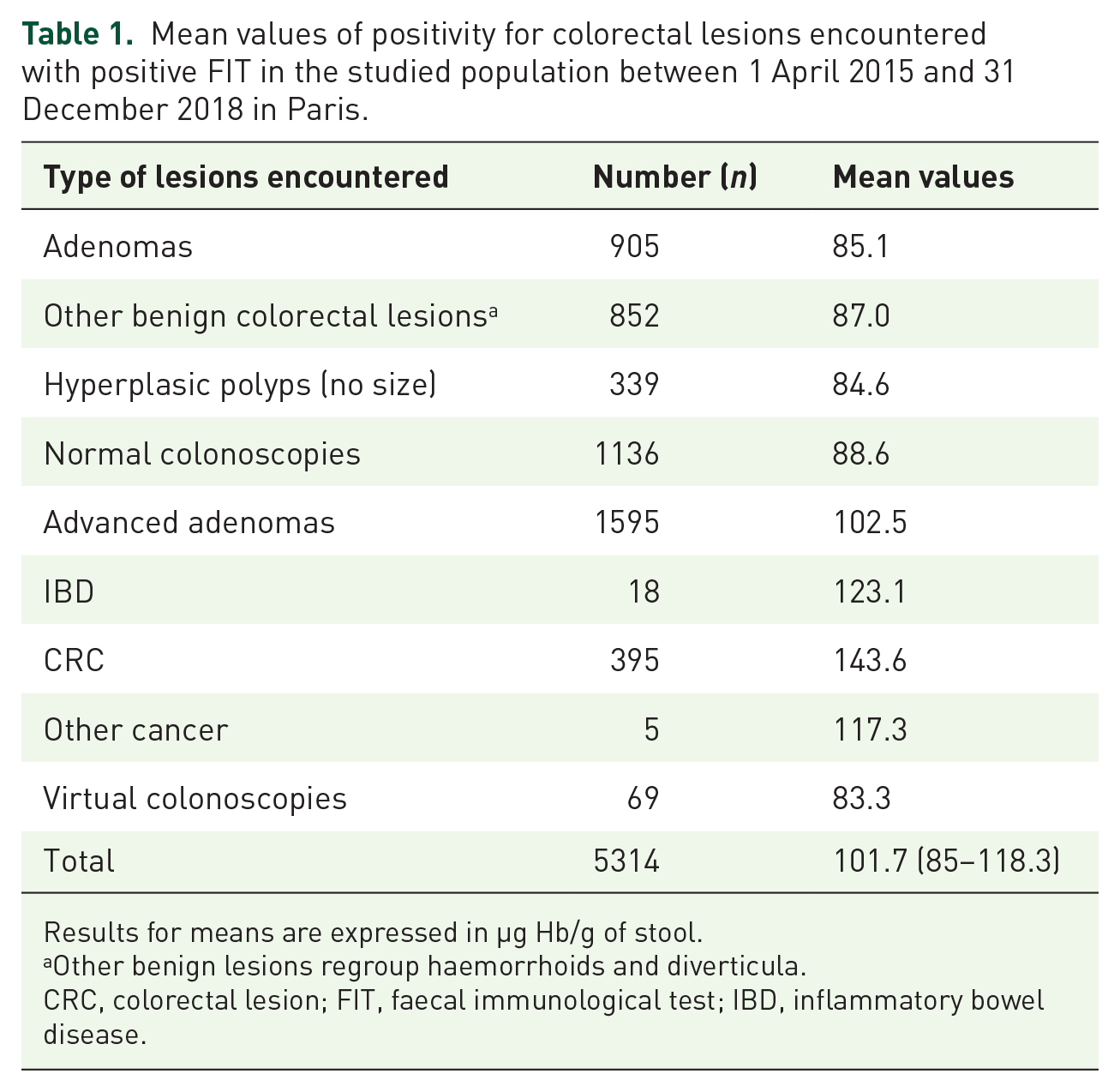
Results for means are expressed in µg Hb/g of stool.
Other benign lesions regroup haemorrhoids and diverticula.
CRC, colorectal lesion; FIT, faecal immunological test; IBD, inflammatory bowel disease.
Detection rates in our population for AAs and CRC were 8.3 and 2.1 for 1000 individuals, respectively.
Positivity values
The mean value of all positive tests in our population was 101.7 µg Hb/g of stool (95% CI 85–118.3 µg Hb/g).
We also calculated mean values for each type of encountered lesions during colonoscopies (Table 1). The mean value for patients with a normal colonoscopy was 88.6 µg Hb/g of stool. The mean value for patients with hyperplasic polyps and adenomas were 84.6 and 85.1 µg Hb/g of stool, respectively. The mean value for patients with AA and CRC were 102.5 and 143.6 µg Hb/g of stool, respectively.
Regarding the 1966 patients with a test result between 30 and 49 µg Hb/g of stool in our final analysed population, there were 481 normal colonoscopies, 499 AAs and 59 CRC. Therefore, the rate of normal colonoscopies in this subgroup was 24.5%, and PPV for AAs and CRC were 25.4% (95% CI 24.9–25.9) and 2.9% (95% CI 2.7–3.0) respectively.
Regarding the 1401 patients with a test result ⩾150 µg Hb/g of stool, there were 244 normal colonoscopies, 466 AAs and 222 CRC. Therefore, the rate of normal coloscopies in this subgroup was 17.4%, and PPV for AAs and CRC were 33.3 (95% CI 32.4–34.1) and 15.9% (95% CI 15.4–16.3) respectively.
CRC localisation
Regarding the 395 CRCs found in our population, 90 were localised in the right colon (22.8%) and 293 in the left colon (74.2%). Information on tumour site was missing for 12 patients (3.0%).
After a first negative test
We also analysed FIT results for individuals who participated in two consecutive screening campaigns between 1 April 2015 and 31 December 2018. We evaluated the cohort population who performed a second FIT during the second campaign (F2) after a first negative test during the previous campaign (F1), without including new participants. Results are shown in Table 2 and Table 3. A total of 180436 tests were negative during F1. About 41% of participants from F1 performed a second test during the next campaign, with 59% lost to follow up for unknown reasons. A total of 2373 tests were positive during F2 for the population who did the two consecutive screenings (1.3%), resulting in 1549 colonoscopies performed (65.3%) and the detection of 335 AAs and 81 CRC. PPVs ranged from 19.3% to 40.4% and from 4.1% to 15.9% for AA and CRC, respectively, during F2.
FIT results during a second campaign after a first negative test, performed between the 1 April 2015 and 31 December 2018: participation rates and positivity rates.
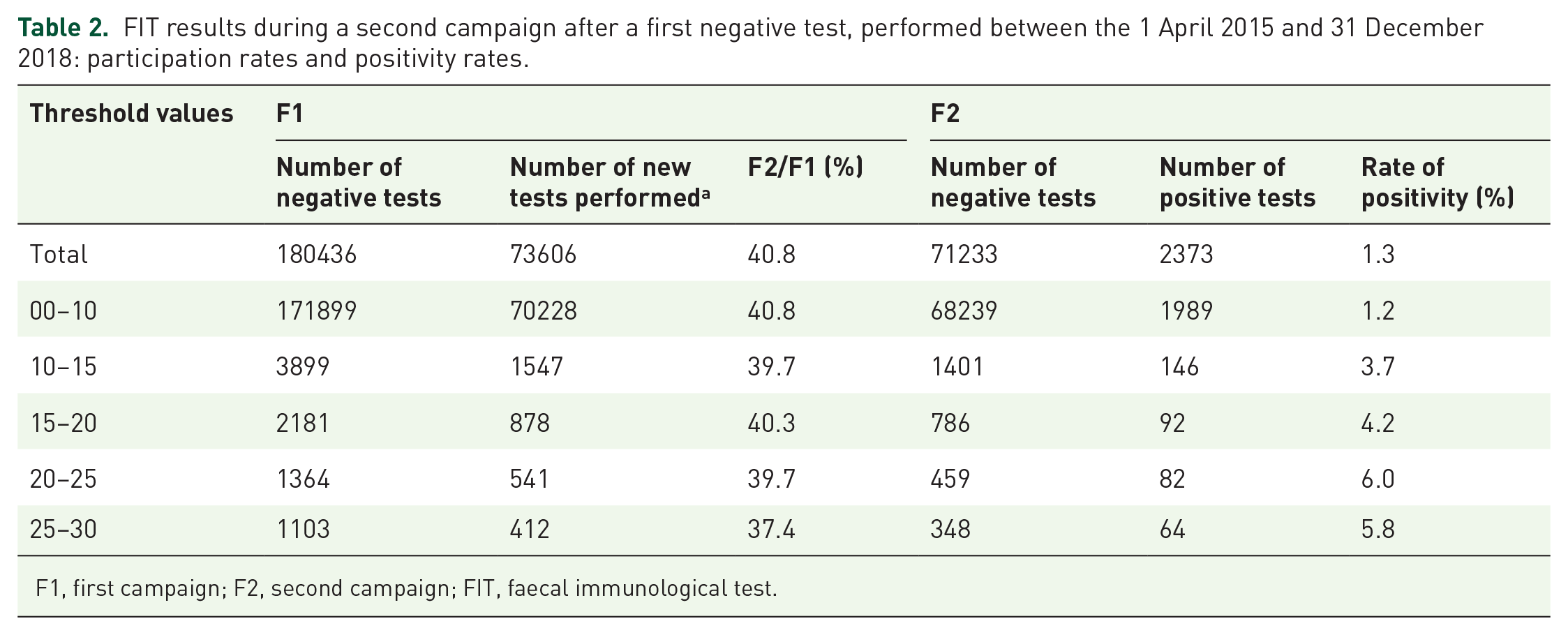
F1, first campaign; F2, second campaign; FIT, faecal immunological test.
FIT results during a second campaign after a first negative test, performed between the 1 April 2015 and 31 December 2018: type of lesions encountered and mean FIT values during the second campaign, F2.

Results for means are expressed in µg Hb/g of stool. F1 and F2 are the first and second screening campaigns, respectively. The percentage of colorectal lesions was calculated as the number of lesions divided by the number of positive tests, PPVs were calculated as described in the methodology section.
Number of new tests performed was calculated after removing non-assessable tests.
AA, advanced adenoma; CRC, colorectal cancer; FIT, faecal immunological test; PPV, positive predictive value.
The risk of having a positive test during F2 increased by 9.9% (p < 0.001) when comparing FIT results ranging between 15 µg Hb/g and 29 µg Hb/g, and 0 µg Hb/g and 14 µg Hb/g during F1. The risk of finding advance colorectal lesions such as AA and CRC during F2 increased by 15% and 8.6%, respectively (both p < 0.001), when comparing negative FIT results ranging from 15 µg Hb/g and 29 µg Hb/g to 0 µg Hb/g and 14 µg Hb/g from F1.
Discussion
Regarding CRC screening with FIT in a French studied population between 1 April 2015 and 31 December 2018, the participation rate for FIT was 25.5% and the false-positive rate was 14.3%. The mean value of positive FIT with normal colonoscopies was 101.7 µg Hb/g of stool (95% CI 85–118.3 µg). This work collected data from a large population, and results of detection rates and PPV for advanced colorectal lesions were in line with that expected in FIT in this population. 10 Similar to the results for the first 18 months of CRC screening with FIT in Paris, participation rates are still low with many patients lost to follow up, so there is still room for improvement. 10
We found that the mean value for all positive tests with a normal colonoscopy (88.6 µg Hb/g of stool) was higher than means for adenomas and hyperplasic polyps, which is not what is expected with a quantitative test. Also, 17.4% of colonoscopies were considered normal for a cut-off value of 150 g Hb/g of stool, with a similar percentage of CRC also detected in this same population. To our knowledge, this has never been described before. The level of faecal Hb in stool varies according to age and sex. 11 FIT analysis requires a stable Hb molecule for a reliable result, so there have been concerns regarding the performance of FIT during warm seasons, with variable results.12–14 To date, there are no sufficient data to forbid the performance of the test during warm seasons and we do not think this explains our results. One hypothesis could be that patients are bleeding from an upper gastrointestinal lesion. Faecal occult blood test are said to be more efficient at the detection of specific colorectal bleeding: the positivity of a guaiac-based test is generally proportional to the quantity of faecal haem, which in turn is related to the size and location of the bleeding lesion; immunochemical tests are considered incapable of detecting small quantities of blood from the upper gastrointestinal tract. 15 Nevertheless, various studies have evaluated the need for a gastroscopy in case of a positive guaiac-based test and a negative colonoscopy: results are contradictory but showed that some advanced gastric lesions were revealed with a positive test.15–18 Another explanation for our results could be the consequence of missed colorectal lesions due to variations in GI colonoscopy performance and in the quality of colonoscopy reports. This raises the question of dedicated French GIs for CRC screening colonoscopies with a defined experience and a standard number of colonoscopies performed each year, as it is done in the United Kingdom and The Netherlands.9,19
Regarding our results, there were 1.3% of patients with a positive test during a second screening campaign after a first negative FIT, but with many patients lost to follow up. Indeed, CCR screening is not mandatory in France and only 40.8% of patients in our population repeated a second test. Therefore, this positivity rate was probably underestimated. Eighty-one CRCs were diagnosed with the second test but tumour–node–metastasis (TNM) staging was not available in the database. Because of small sample sizes, we compared our results during the second campaign for negative values ranging from 15 µg Hb/g and 29 µg Hb/g to 0 µg Hb/g and 14 µg Hb/g from the first FIT: with an increasing negative FIT value, there was also a significant increase of the FIT positivity rate, as well as the number of advance colorectal lesions found during the second screening (all p < 0.001). As highlighted in Toes-Zoutendijk et al.’s 9 work, if the 47 µg Hb/g of stool cut-off level had been applied in the first part of their study, this would have led to failure to detect 14.5% CRC and 31.3% AAs because of a decrease in the number of positive tests. Lowering the cut-off level of positivity leads to a risk of performing more negative colonoscopies and reducing specificity with the detection of more benign colorectal lesions. As mentioned before, various researchers have tried to find the optimal threshold for sensitivity and specificity. Nevertheless, there is still a risk of interval cancer that seems partly related to the cut-off value. In a Scottish study, with a threshold of 80 µg Hb/g of stool, the percentage of interval CRC was 51%. 20 In an Italian study, with a threshold of 20 µg Hb/g of stool the percentage of interval CRC was 31%. 21 Finally, Buron et al. 22 have also shown that the probability of testing positive in consecutive screens and being diagnosed with advanced neoplasia rose with increasing values of negative FIT, which is in line with our results.
Overall, choosing the optimal cut-off value is a challenge and mainly a matter of economics and health-system management. Although samples were small, with missing data due to lack of participation, our results suggest that the French cut-off level could be lowered because of the risk of missed CRC, and with previous studies also showing that advanced colorectal lesions can be found with low levels of FIT positivity. Additionally, serrated polyps were not considered in our work, as mentioned in the methodology section, and this could also have impacted our results. Indeed, serrated polyps can also lead to CRC, and we think they should be reported in the French CRC screening database. Further studies on larger populations should confirm whether the actual French positivity threshold should be lowered, with the obvious risk of an excessive performance of colonoscopies and a higher number of false positives. Also, the reporting of serrated adenomas in the French screening programme should be established and might impact future results. Finally, the reason for such high values of FIT in patients with normal colonoscopies should be investigated: is FIT really specific for colorectal bleeding, or should we look for upper gastrointestinal lesions?