
Abstract
Background:
Patients with Crohn’s disease (CD) are at increased risk of co-occurring immune-mediated inflammatory diseases (IMIDs). As discrepancy exists regarding the phenotypic presentation of CD among patients with such co-occurring IMIDs, we aimed to conduct a systematic review with meta-analysis characterizing the phenotype of CD among this subgroup of patients.
Methods:
PubMed, Embase, and Scopus were searched from their earliest records to October 2019 for studies reporting the behavior and localization of CD according to the Vienna or Montreal Classifications and CD-related surgery in patients with co-occurring IMIDs. These studies were the subject of a random effect meta-analysis.
Results:
After reviewing 24,413 studies, we identified a total of 23 studies comprising 1572 and 35,043 CD patients with and without co-occurring IMIDs, respectively, that fulfilled our inclusion criteria. Overall, patients with co-occurring IMIDs were more likely to have upper gastrointestinal inflammation than were patients without co-occurring IMIDs [relative risk (RR) = 1.49 (95% confidence interval (CI) 1.09–2.04), p = 0.01, I2 = 7%]. In addition, presence of primary sclerosing cholangitis (PSC) was associated with a lower occurrence of ileal affection [RR = 0.44 (95% CI 0.24–0.81), p < 0.01, I2 = 32%], increased occurrence of colonic affection [RR = 1.78 (95% CI 1.33–2.38), p < 0.01, I2 = 32%] and an increased likelihood of non-stricturing and non-penetrating behavior [RR = 1.43 (95% CI 0.97–2.11), p = 0.07, I2 = 86%]. The latter reached significance when cumulating different IMIDs [RR = 1.30 (95% CI 1.09–1.55), p < 0.01, I2 = 88%]. CD patients with PSC also underwent fewer CD-related surgeries [RR = 0.55 (95% CI 0.34–0.88), p = 0.01, I2 = 0%], irrespective of CD location or behavior.
Conclusion:
This study emphasizes that CD patients with co-existing PSC are likely to have a unique inflammatory distribution primarily confined to the colon, while patients with IMIDs in general have higher likelihood of affection of upper gastrointestinal tract and a non-stricturing and non-penetrating behavior. As such a phenotype of CD is typically associated with a milder disease course; future studies are needed to confirm these results.
Keywords
Introduction
Inflammatory bowel disease (IBD) consists of ulcerative colitis (UC) and Crohn’s disease (CD), which are immune-mediated inflammatory diseases (IMIDs) with a multifactorial etiology. Both UC and CD commonly cluster with other IMIDs.1–3 These IMIDs have similarities regarding immunological disruptions, as well as genetic and environmental risk factors with UC and CD. In addition, these co-occurring IMIDs might have courses that run in parallel with, or independently of, the course of IBD. 4 The existing literature has focused on describing the localization and behavior of UC in relation to co-occurring primary sclerosing cholangitis (PSC), showing that these patients experience milder disease activity but a higher risk of pancolitis, backwash ileitis, rectal sparing, colorectal cancer and mortality. Thus, UC-PSC has been acknowledged as a unique subtype of UC. 5 Unlike with UC, the existing literature has not described the disease characteristics of CD in the presence of other IMIDs in depth. 6 However, we found in a recent meta-analysis that patients with CD and PSC have a remarkably lower risk of IBD-related surgeries and an increased risk of malignancies. 7 Therefore, the aim of this systematic review was to investigate the disease localization and behavior of CD with and without co-occurring PSC and other IMIDs. In addition, we investigated the association between CD-related surgery, disease phenotype of CD and presence of IMIDs.
Materials and methods
The protocol of this systematic review was registered in the International Prospective Register of Systematic Reviews prior to its initiation (CRD42020166247). The review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analyses and the Cochrane handbook.8,9
Search strategy
The electronic databases PubMed, Embase and Scopus were searched by two authors, MA and MZ, from their earliest records to October 2019 for studies reporting the disease localization or behavior of CD in the presence of IMIDs. Supplemental File 1 provides the search strategy. The keywords used were ‘IMIDs’ (not specified further), ‘autoimmune disease’ (not specified further), ‘Diabetes type 1’, ‘asthma’, ‘Grave’s disease’, ‘spondyloarthropathy’, ‘spondyloarthropathies’, ‘ankylosing spondylitis’, ‘iridocyclitis’, ‘uveitis’, ‘rheumatoid arthritis’, ‘polymyalgia rheumatica’, ‘psoriasis’, ‘psoriatic arthritis’, ‘primary sclerosing cholangitis’, ‘celiac disease’, ‘pyoderma gangrenosum’, ‘pernicious anemia’, ‘autoimmune hepatitis’, ‘sarcoidosis’, ‘giant cell arteritis’, ‘primary biliary cholangitis’, ‘primary biliary cirrhosis’, ‘Hashimoto’s thyroiditis’, ‘episcleritis’ and ‘Sjogren’s syndrome.’
In addition, a manual search of abstracts from the ECCO congress (European Crohn’s and Colitis Organization), UEG Week (United European Gastroenterology) and DDW (Digestive Diseases Week) between 2015 and 2019 was also conducted to obtain potential, near-future publications. The search results were exported to Mendeley and de-duplicated prior to screening. Reference lists of the relevant reviews were also screened for eligibility.
Inclusion criteria
All original studies in the English language reporting the outcome of CD localization or behavior according to the Montreal or Vienna Classifications in the presence of IMIDs were eligible for inclusion in this study. Moreover, final inclusion of studies required a clinically verified diagnosis of CD according to international criteria.10,11
We excluded studies of only UC patients, reviews, case reports, editorials and studies in languages other than English. If a study presented insufficient data, the corresponding author was asked to provide the missing data and the study was included if these data were provided.
Selection process
The selection process is presented in Figure 1. First, two of the study authors, MA and MZ, independently screened all search results based on titles and abstracts and removed irrelevant studies. Subsequently, MA and MZ independently assessed the full texts of the remaining studies for possible inclusion; any disagreements were solved by joint review.
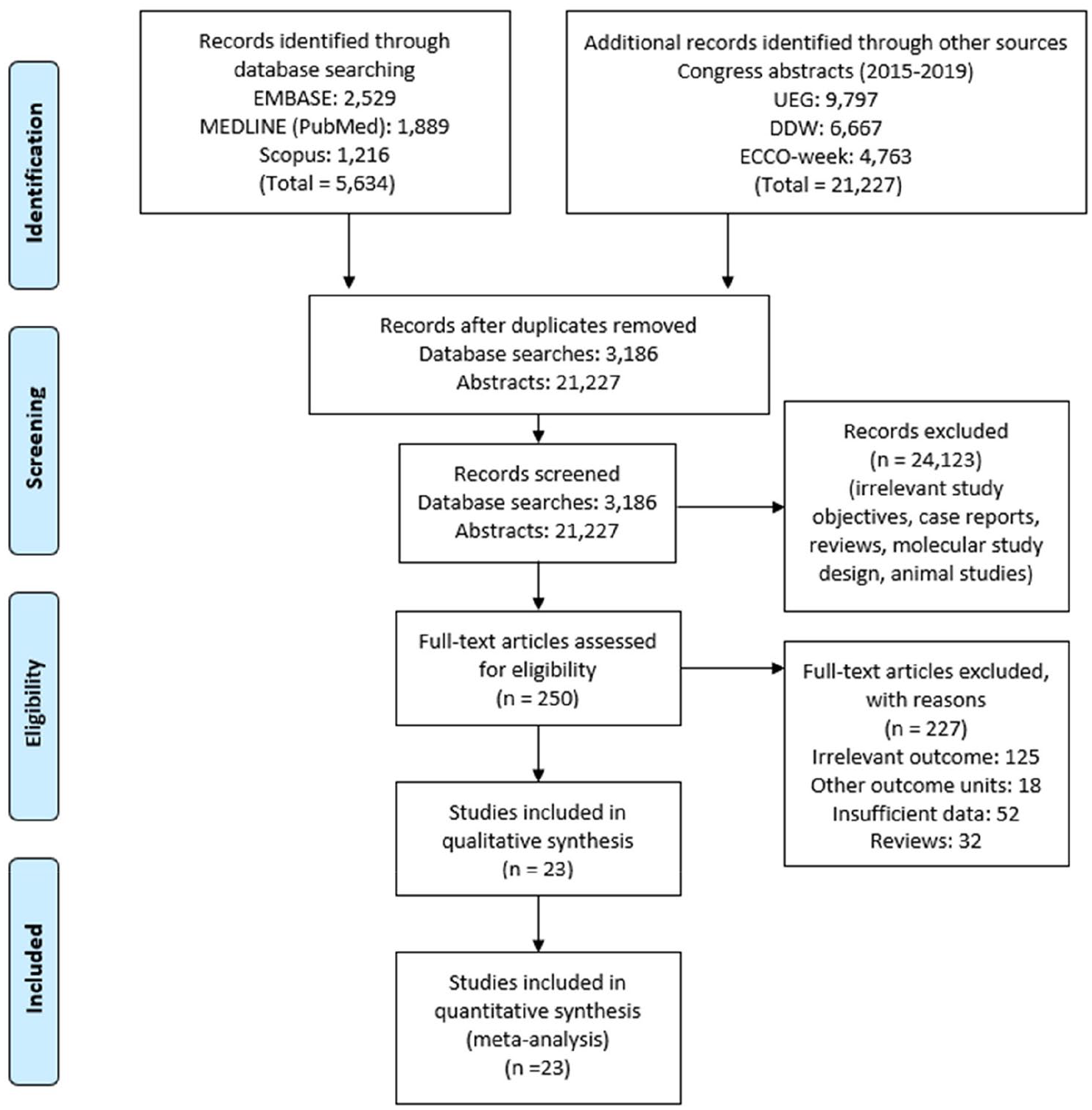
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram of the literature search.
Data extraction and outcomes
One author, MA, extracted the data and repeated the data extraction. The following data were extracted, per the Cochrane Consumers and Communication Review Group’s template: 12 author name, study title, publication year, study design, geographical region, number of patients, age at onset of CD, proportion of females, proportion of smokers, IMID subtype and CD-related disease localization and behavior, namely L1 to L4 and B1 to B3. Due to different study designs, L4 represented both isolated and non-isolated upper gastrointestinal affection. Surgery rates among patients were also extracted.
Definitions
IMIDs were defined as diseases in which either autoimmune, autoinflammatory or inflammatory mechanisms play a vital role in the pathophysiology. Population-based studies were defined as studies that included all CD patients within a well-defined geographical area.
Historically, features of CD were described in the Vienna Classification System, which considered age of onset, disease location and disease behavior as the predominant phenotypic elements. 13 Primarily in order to compensate for rigid categorization in terms of inability to describe upper gastrointestinal disease along with more distal disease and difficulty categorizing perianal disease, the Vienna Classification got revised to the Montreal Classification System.13,14 Accordingly, the main update is that the newer system takes perianal disease to consideration as a feature to be added to the non-stricturing and non-penetrating (B1), stricturing (B2) or penetrating (B3) behavior of CD, while upper gastrointestinal involvement (L4) is considered a modifier of ileal (L1), colonic (L2) or ileocolonic (L3) involvement.
Quality assessments
Quality assessment of the studies was conducted by two authors (MA and MZ) independently, using the Newcastle–Ottawa Scale (NOS), which is based on a total of eight factors across three domains: selection, comparability and outcome/exposure. 15 To our knowledge, NOS has not been externally validated, but is among the most frequently used quality assessment tools for non-randomized studies. In addition, it is used by The Cochrane Collaboration. 9
A high-quality study was defined as having a score of 7–9, while moderate- and low-quality studies were defined as having scores of 4–6 and 0–3, respectively. Publication bias was assessed using Egger’s regression test using RStudio version 1.2.1335 and illustrated via funnel plots in Review Manager (RevMan) version 5.3.
Statistical analysis
The extracted data were analyzed using RevMan version 5.3. Meta-analysis of the pooled proportions of L1–L4 and B1–B3 among patients with CD, with and without co-occurring IMIDs, was conducted using DerSimonian and Laird’s random-effect model in accordance with Cochrane recommendations. The results were expressed as risk ratios (RRs) with 95% confidence intervals (95% CIs). A p-value smaller than 0.05 was considered significant. In addition, subgroup analyses and meta-regressions were also performed in RStudio version 1.2.1335 and visualized in bubble plots weighting the studies by their variance and heterogeneity. Heterogeneity was assessed by squared inconsistency (I2) statistics and, as per the Cochrane recommendations, an I2 higher than 75% indicated a substantial between-study variance, while an I2 lower than 25% indicated low heterogeneity. Subgroup-analyses were conducted of the type of co-occurring IMIDs and type of study design, while meta-regressions were conducted to assess the effect measures in relation to the proportion of females, age at onset of CD and the proportion of smokers. Subgroup-analysis was conducted whenever an IMID was investigated in at least two publications. The risk of CD-related surgery among patients with co-occurring IMIDs was also assessed in relation to the disease localization and behavior of CD and the aforementioned variables.
Results
Patients and study characteristics
The systematic search (presented in Figure 1) yielded a total of 5634 studies and 23,197 congress abstracts. After removing duplicates, irrelevant studies and studies not fulfilling the eligibility criteria, 23 studies were ultimately included in this meta-analysis, including nine retrospective case–control studies, seven prospective cohort studies, six retrospective cohort studies and one population-based cohort study.16–38 A total of 1572 CD patients with IMIDs and 35,043 CD patients without IMIDs were included. Among the IMIDs, CD behavior and localization was most extensively investigated in relation to PSC in a total of eight studies.16,19–21,32,36–38 The remaining studies investigating CD patients with co-occurring ankylosing spondylitis and sacroiliitis,17,18,22 autoimmune pancreatitis, 23 axial spondyloarthropathy, 24 celiac disease,25,27 erythema nodosum,29,35 multiple sclerosis, 31 psoriasis 34 and uveitis 28 were pooled in the group ‘IMIDs other than PSC’.
An overview of the data extraction including sample sizes, study designs, type of IMID and proportion of phenotypes is presented in Table 1. A summary of the results of the meta-analysis stratified according to each IMID is presented in Table 2. The statistical analysis, including all forest and funnel plots, is provided in Supplemental File 2.
Characteristics of the 23 studies fulfilling the inclusion criteria.

L1–L4 and B1–B3 are disease localization and behavior of Crohn’s disease according to the Montreal Classification.
CD, Crohn’s disease; IMID, immune-mediated inflammatory disease.
Summary of results from the meta-analysis.

L1–L4 and B1–B3 are disease localization and behavior of Crohn’s disease according to the Montreal Classification.
AS, ankylosing spondylitis; EN, erythema nodosum; IMID, immune-mediated inflammatory disease; PSC, primary sclerosing cholangitis. Bold values indicate statistical significance.
Description of the quality of studies
The mean Newcastle–Ottawa Scale score was 7.6, including 21 high-quality studies and two studies of moderate quality. Supplemental File 3 summarizes the quality assessment using the Newcastle–Ottawa Scale.
CD localization among patients with and without co-occurring IMIDs
All the included studies described the CD localization in presence and absence of other IMIDs. Overall, the distribution of disease location with regard to L1 [RR = 0.86 (95% CI 0.73–1.02), p = 0.09, I2 = 54%; Supplemental Figure 1(a)], L2 [RR = 1.16 (95% CI 0.95–1.41), p = 0.14, I2 = 72%; Supplemental Figure 2(a)] and L3 [RR = 1.03 (95% CI 0.94–1.12), p = 0.54, I2 = 9%; Supplemental Figure 3(a)] was found to be comparable in CD patients with and without co-occurring IMIDs. However, L4 was more frequent in patients with co-occurring IMIDs [RR = 1.49 (95% CI 1.09–2.04), p = 0.01, I2 = 7%; Supplemental Figure 4(a)].
Risk stratification for specific IMIDs revealed that CD patients with concurrent PSC had a distinct inflammatory distribution, with a lower occurrence of L1 [RR = 0.44 (95% CI 0.24–0.81), p < 0.01, I2 = 32%; Supplemental Figure 1(a)] and a higher occurrence of L2 [RR = 1.78 (95% CI 1.33–2.38), p < 0.01, I2 = 32%] in comparison with patients without PSC. Such a lower occurrence of L1 was not observed among patients with ankylosing spondylitis [RR = 1.16 (95% CI 0.95–1.42), p = 0.14, I2 = 0%] or celiac disease [Supplemental Figure 1(a)]. Likewise, the increased occurrence of L2 among patients with PSC was not found among patients with other IMIDs; in contrast, patients with ankylosing spondylitis showed a trend toward a lower occurrence of colonic disease [RR = 0.75 (95% CI 0.56–1.00), p = 0.05, I2 = 0%] (Figure 2). Aiming to address the high heterogeneity observed in the distribution of L2, we conducted subgroup analysis stratifying the study design, but this did not explain the heterogeneity [Supplemental Figure 2(b)]. Instead, at least part of the heterogeneity seems to be related to the types of IMID (Figure 2).
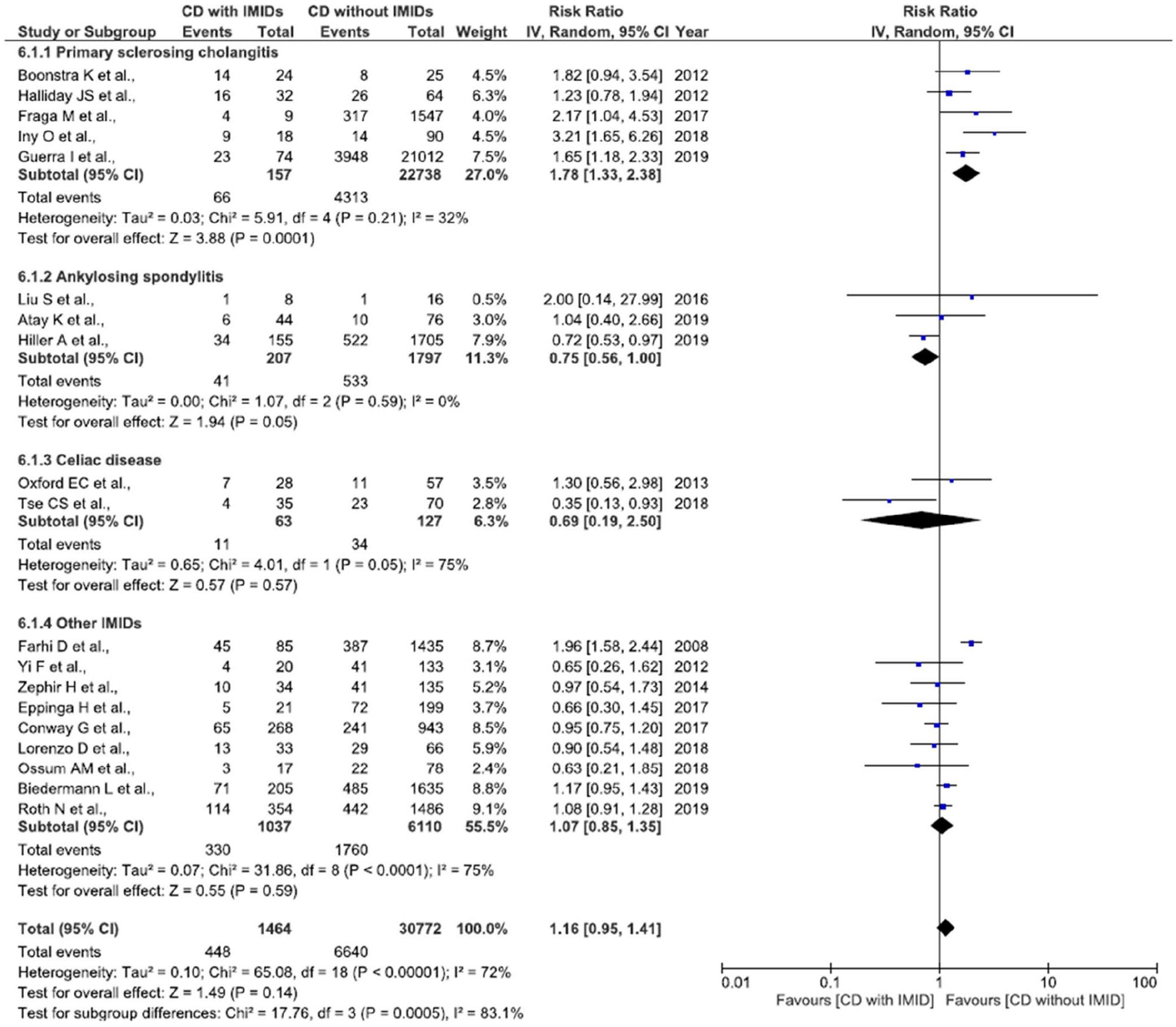
Forest plot for the risk of colonic affection (L2) in patients with Crohn’s disease and co-occurring immune-mediated inflammatory diseases (IMIDs) as compared with patients without IMIDs.
For the purpose of investigating the association between colonic involvement of CD and the presence of PSC, we pooled the L2 and L3 results and found that patients with co-occurring PSC were more likely to suffer from colonic disease as compared with patients without PSC [RR = 1.33 (95% CI 1.21–1.45), p < 0.01, I2 = 0%]. In fact, there was a trend toward a higher likelihood of colonic involvement of CD among patients with any IMID [RR = 1.10 (95% CI 1.00–1.21), p = 0.05, I2 = 79%], including celiac disease (Table 2). However, there was a trend toward less colonic affection among patients with ankylosing spondylitis [Supplemental Figure 5(a)]. The high heterogeneity was not explained by study design but partly by stratification of IMIDs [Supplemental Figure 5(a) and (b)].
Possible modulators of CD localization in the presence of co-occurring IMIDs were also investigated in meta-regressions but neither age at diagnosis of CD (p = 0.16), gender (p = 0.31), nor smoking status (p = 0.07) was associated with CD localization in patients with IMIDs. However, age at CD diagnosis was significantly associated with L1 among patients without IMIDs (p < 0.01), and being female was significantly associated with the occurrence of L4 (p = 0.01). In addition, smoking was significantly associated with L1 (p = 0.04) and L4 (p < 0.01). All meta-regressions are summarized in Supplemental File 4, but could not be stratified according to specific types of IMIDs.
We found no evidence of publication bias as funnel plot and the Egger’s regression test was conducted for each disease localization (Supplemental Files 1c–5c).
CD behavior among patients with and without co-occurring IMIDs
The behavior of CD in relation to co-occurring IMIDs was investigated in 18 studies comprising a total of 847 and 28,601 patients with and without co-occurring IMIDs, respectively.16,17,19,21–25,27,29–35,37,38
Non-stricturing and non-penetrating disease (B1) was significantly more frequent among patients with co-occurring IMIDs than among patients without IMIDs [RR = 1.30 (95% CI 1.09–1.55), p < 0.01, I2 = 88%], which was primarily driven by PSC [RR = 1.43 (95% CI 0.97–2.11), p = 0.07, I2 = 86%] rather than ankylosing spondylitis, celiac disease or erythema nodosum in the subgroup analysis (Figure 3). The high heterogeneity was found to be driven by case–control studies and this subgroup demonstrated significance regarding distribution of B1 [Supplemental Figure 6(b)].
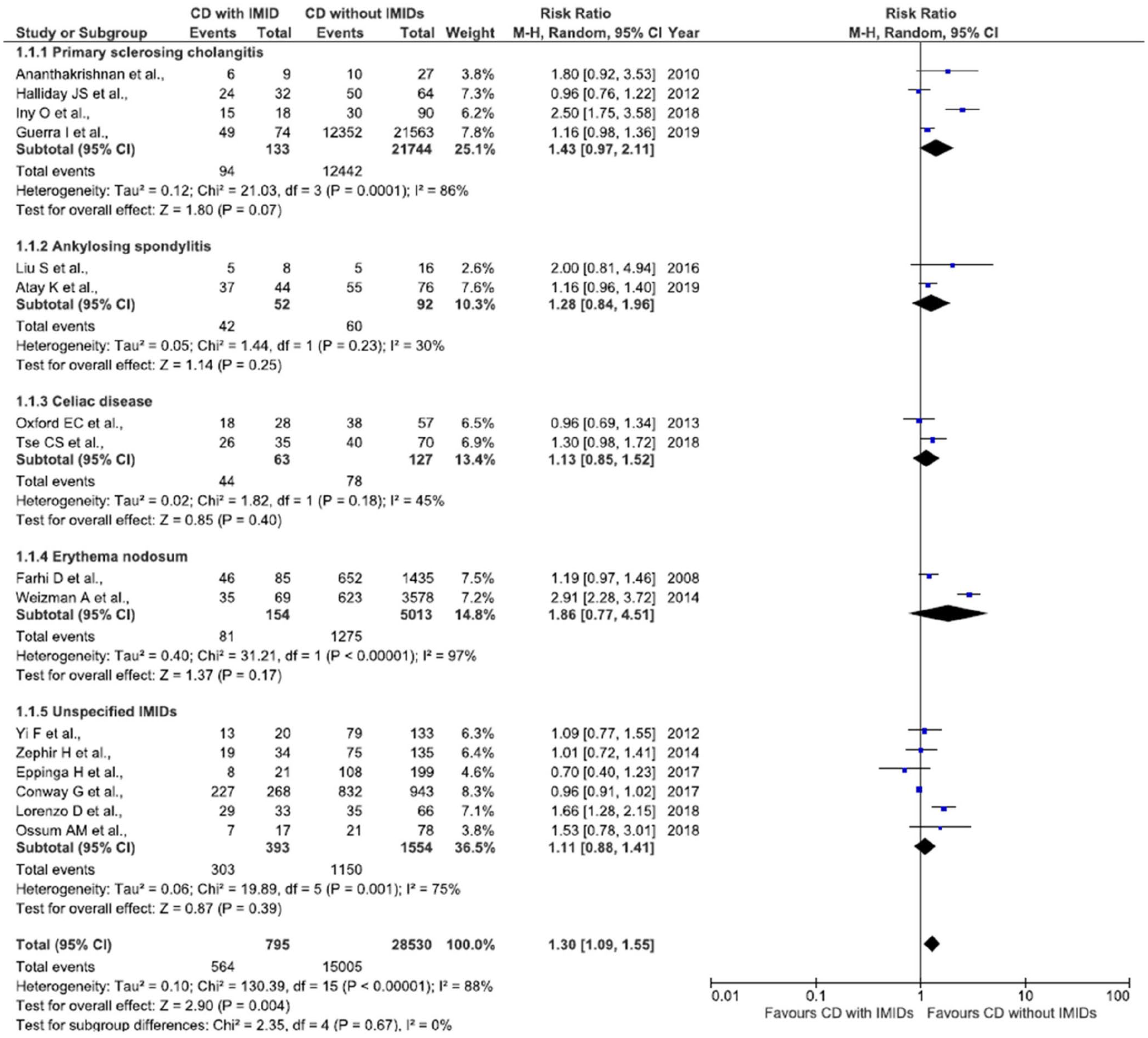
Forest plot for the probability of a non-stricturing disease in patients with Crohn’s disease and co-occurring immune-mediated inflammatory diseases.
In contrast to B1, the co-existence of PSC, ankylosing spondylitis, celiac disease, or erythema nodosum along with CD was not associated with an increased risk of stricturing disease [Supplemental Figure 7(a)] or penetrating disease [Supplemental Figure 8(a) and Table 2].
For the purpose of investigating the risk of complicated disease, we pooled B2 and B3 and found that patients with co-occurring IMIDs had a trend towards less complicated disease behavior [RR = 0.79 (95% CI 0.61–1.02), p = 0.07, I2 = 88%; Supplemental Figure 9(a)]. This was numerically attributed to PSC [RR = 0.63 (95% CI 0.39–1.00), p = 0.05, I2 = 52%] and celiac disease [RR = 0.61 (95% CI 0.37–1.03), p = 0.07, I2 = 0%] but not erythema nodosum. The high heterogeneity was addressed in subgroup analysis according to study design, finding that this was related to case–control studies, while cohort studies showed a low degree of heterogeneity and a significantly reduced risk of complicated CD in presence of IMIDs [RR = 0.90 (95% CI 0.82–0.98), p = 0.02; Supplemental Figure 9(b)].
Meta-regressions were also conducted to investigate possible modulators of CD behavior. While age at CD diagnosis (p = 0.09) and gender (p = 0.12) had no influence on the behavior of CD in the presence of IMIDs, ongoing or former smoking was positively associated with the risk of stricturing disease (p = 0.02), although this was not the case for patients without co-occurring IMIDs (p = 0.36). On the other hand, among patients without co-occurring IMIDs, being female was associated with a lower risk of complicated disease behavior (B2 and B3) (p < 0.01). All meta-regressions are summarized in Supplemental File 4.
While Egger’s regression test proved negative for patients without co-occurring IMIDs, the regression test regarding data of patients with co-occurring IMIDs were significant (p < 0.05), indicating presence of publication bias.
Risk of IBD-related surgery in relation to CD behavior, localization and the presence of IMIDs
Finally, we investigated the possible association between IBD-related surgery and CD localization and behavior among patients with and without co-occurring IMIDs.
A total of 12 studies comprising 833 and 1682 CD patients with and without co-occurring IMIDs, respectively, were included in the meta-regressions.18,21–23,25,26,28,30–32,36,38 We investigated whether CD localization and behavior associated with the presence of PSC could explain the lower risk of IBD-related surgery. 7 As shown in Table 3 and Figure 4, colonic disease (L2 and L3) does seem to affect the risk of surgery; however, this modulation was also observed in patients without co-occurring IMIDs (p < 0.01), indicating that the association between PSC and risk of CD-related surgery might be unrelated to the localization and behavior of CD. The behavior of CD was also not associated with the risk of CD-related surgery (Table 3). These analyses could not be stratified according to specific IMIDs.
Meta-regression analysis for the risk of CD-related surgeries.

L1–L4 and B1–B3 are disease localization and behavior of Crohn’s disease according to the Montreal Classification.
CD, Crohn’s disease; IMID, immune-mediated inflammatory disease; PSC, primary sclerosing cholangitis.

Bubble plot illustrating the meta-regression of the association between colonic Crohn’s disease (CD) in patients with and without co-occurring immune-mediated inflammatory diseases and their risk of CD-related surgeries.
Discussion
To our knowledge, this is the first systematic review investigating the localization and behavior of CD in relation to co-occurring IMIDs. We found that CD patients with co-occurring IMIDs had a significantly increased affection of the upper gastrointestinal tract, while patients with co-occurring PSC had a lower occurrence of ileal disease and a higher occurrence of colonic affection. In contrast, patients with ankylosing spondylitis showed a trend towards a lower involvement of CD. In addition, we found that patients with PSC showed a trend towards increased inflammatory behavior B1. The findings might indicate that CD patients with co-occurring IMIDs, specifically PSC, constitute a distinct subgroup of CD with a milder phenotype. Interestingly, a milder phenotype of IBD in the presence of PSC is already acknowledged to exist among patients with UC and it has been proposed that PSC colitis might represent a separate and milder disease entity. 5 We recently showed that the presence of IMIDs increases the risk of IBD-related surgery and the present findings underline the importance of future prospective studies for evaluating whether the risk of surgery is due to altered disease activity or rather to changes in clinicians’ perception of the right treatment strategy. 7
The relationship between the liver and the gut has been recognized for more than 50 years and it has been shown that the course of UC worsens after liver transplantation due to PSC and that the risk of a recurrence of PSC negatively correlates with colectomy rates.39–41 This indicates a pathophysiological connection between the gut and the liver. However, the pathophysiological mechanisms driving the association between IBD and PSC are still unknown. A recent and comprehensive review 42 of this topic summarizes three hypotheses aiming to explain the association between IBD and PSC. First, ‘leaky gut’ 43 and ‘gut lymphocyte homing’ 44 refer to a translocation of bacteria, secondly T-cells and memory cells from an inflamed gut into the portal circulation, causing biliary inflammation. The third hypothesis focuses on an antigenic overlap between the colon and the biliary system that causes inflammation, including MAdCAM-1 and CCL25, which promote the migration of α4β7-positive T-cells into the liver. 45 However, this pathway does not fully explain the distribution of inflammation in CD, nor the fact that vedolizumab, which acts as an antibody against the α4β7 integrin, is safe in patients with co-occurring IBD and PSC but does not seem to have an impact on the hepatic inflammation.46–48
Nonetheless, increasing evidence has now established that PSC is in fact a multifactorial disease. Genome-wide associations have revealed that the macrophage stimulating 1 (MST 1) gene is central in the pathogenesis of both CD 49 and PSC. 50 However, its role in inducing the biliary inflammation which characterizes PSC has yet to be defined. Among environmental factors, vitamin D has well-known immunological properties and more than half of patients with CD and PSC have a vitamin D deficiency.51,52 As the microbiota, which is disrupted in patients with both CD and PSC, is responsible for the metabolism of different bile acids, and these in turn regulate activation of the vitamin D receptor, it could be that this disruption results in a defective regulation of vitamin D functions. In addition, smoking is a known risk factor for a more progressive CD, 53 while no such association exists between CD and PSC. 54 If fewer patients with CD and co-occurring PSC are smokers, this could partially explain the milder phenotype of CD found in patients with co-occurring IMIDs.
In this systematic review we also found a lower risk of CD-related surgeries and ileal involvement among patients with co-occurring PSC. The exact reasons for this have yet to be explained but might be secondary to a milder inflammatory burden that also characterizes patients with ulcerative colitis with co-occurring PSC. We aimed to explore whether less ileal affection could explain the lower proportion of surgeries, but this was not the case in patients with PSC (p = 0.65) or IMIDs other than PSC (p = 0.90).
This study has some limitations. First, we were unable to describe the course of CD in relation to the severity of PSC. A recent study compared CD patients with co-occurring PSC requiring liver transplantation with patients with a milder phenotype of PSC and found that they did not differ in terms of disease activity nor risk of colectomy. 55 Similar findings were reported among patients with UC and PSC. 39 Second, we described the association between localization and behavior of CD and the presence of co-occurring IMIDs irrespective of the type of IMID and its incidence in patients with CD, and this might have introduced bias because of the underreporting of specific IMIDs. In addition, pooling data for different IMIDs might have increased the heterogeneity in our pooled results; however, this heterogeneity might also be ascribed to patient-related (e.g. ethnicity and age groups) and study-related (e.g. study design and exclusion of studies in languages other than English) factors, which themselves also are considered limitations. However, we aimed to take these factors into consideration following current guidelines on this topic as we conducted subgroup analysis based on study design and conducted meta-regression of gender, smoking status and age at diagnosis of CD. We have not investigated perianal CD among patients with co-occurring IMIDs as this has already been reviewed. 7 Finally, there is a potential risk of misclassifying UC as colonic CD, as PSC appears more frequently in UC. 56 Unfortunately some of the studies included in this review did not state explicitly that the diagnosis of CD was based on biopsies and, hence, clearly distinguishable from UC.
In conclusion, this systematic review and meta-analysis shows that the presence of IMIDs affects disease localization and behavior in CD patients, and that this is especially the case for PSC, which was shown to be associated with a colonic phenotype of CD, while IMIDs in general were associated with upper gastrointestinal involvement and a non-stricturing and non-penetrating behavior. These results underline the importance of recognizing IMIDs, especially PSC, for their prognostic value among patients with CD, and not only among those with UC. This may impact clinical practice with increased awareness of upper gastrointestinal affection among patients with CD and IMIDs. Future studies in a prospective setting are needed to confirm and elaborate on these findings.
Supplemental Material
sj-docx-1-tag-10.1177_17562848211004839 – Supplemental material for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease
Supplemental material, sj-docx-1-tag-10.1177_17562848211004839 for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease by Mohamed Attauabi, Mirabella Zhao, Flemming Bendtsen and Johan Burisch in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848211004839 – Supplemental material for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease
Supplemental material, sj-docx-2-tag-10.1177_17562848211004839 for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease by Mohamed Attauabi, Mirabella Zhao, Flemming Bendtsen and Johan Burisch in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-3-tag-10.1177_17562848211004839 – Supplemental material for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease
Supplemental material, sj-docx-3-tag-10.1177_17562848211004839 for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease by Mohamed Attauabi, Mirabella Zhao, Flemming Bendtsen and Johan Burisch in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-4-tag-10.1177_17562848211004839 – Supplemental material for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease
Supplemental material, sj-docx-4-tag-10.1177_17562848211004839 for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease by Mohamed Attauabi, Mirabella Zhao, Flemming Bendtsen and Johan Burisch in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-5-tag-10.1177_17562848211004839 – Supplemental material for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease
Supplemental material, sj-docx-5-tag-10.1177_17562848211004839 for Systematic review and meta-analysis: the impact of co-occurring immune-mediated inflammatory diseases on the disease localization and behavior of Crohn’s disease by Mohamed Attauabi, Mirabella Zhao, Flemming Bendtsen and Johan Burisch in Therapeutic Advances in Gastroenterology
Footnotes
Author contributions
MA: study concept design, search strategy design and execution, data extraction, analysis and interpretation of data, drafting of manuscript, critical revision of manuscript.
MZ: study concept design, search strategy design and execution, critical revision of manuscript.
FB and JB: study concept design, search strategy design, critical revision of manuscript, supervision.
All authors approved the final version of the manuscript, including the authorship list.
Conflict of interest statement
MA: none
MZ: travel fees from Takeda Pharma A/S.
FB: grants from Ferring and Tillotts. None of these pertain to the research submitted here.
JB: personal fees from AbbVie, Janssen-Cilag, Celgene, MSD, Samsung Bioepis, and Pfizer; grants and personal fees from Takeda and Tillots Pharma; grants from Novo Nordisk. None of these pertain to the research submitted here.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.